
Abstract
Background
The Bougainville Crisis (1988–1997) was the largest armed conflict in the Pacific since WW-II. Despite this, there has been no assessment of the Mental Health and Psychosocial (MHPS) impact of the war. The aim of this paper is to summarize the available data regarding the longer-term MHPS impact of the Bougainville Crisis.
Methods
A literature review and a sequence of consultations in Bougainville were conducted to identify the MHPS impact of the Bougainville Crisis and the capacity within Bougainville to address these issues.
Results
The Bougainville Crisis resulted in violence-related deaths; the displacement of more than half of the population; widespread human rights abuses; far-reaching societal impacts including undermining of the traditional authority of elders and women and damage to cultural values and relationships; property damage; and significant impacts on education and the economy. Conflict-related experiences continue to impact on mental health in the form of trauma-related symptoms, anger, complicated grief, alcohol and substance abuse, domestic violence including sexual assault, excessive alcohol use and a lack of engagement in purposeful activities. Other impacts include an increase in other forms of gender-based violence (including sexual assault), population displacement, and adverse trans-generational effects on children exposed to disturbed parental behaviours attributable to conflict exposure. In spite of the evident needs, there is limited capacity within Bougainville to address these pressing MHPS issues.
Conclusions
The Bougainville Crisis has had a significant MHPS impact at multiple levels in the society. There is a strong interest within Bougainville to draw on external expertise to build local capacity to address MHPS issues. Preliminary recommendations are made to assist the process of building the capacity in Bougainville to address MHPS needs.
Similar content being viewed by others

Background
The Bougainville Crisis refers to a civil war that occurred between 1988 and 1997 in the North Solomons Province of Papua New Guinea (PNG), now known as the Autonomous Region of Bougainville. The war, which was the largest armed conflict in the Pacific since WW-II [1–3] was accompanied by widespread human rights abuses and resulted in a significant number of combat and civilian deaths, the displacement (mostly internal) of more than half of the population, and far-reaching social, economic and educational impacts on the society as a whole. Despite the gravity of the upheaval, no thorough assessment has been made of the MHPS impact of the war on the community as a whole.
In October 2009, the first author (DT) was invited by a Bougainville political leader and senior Catholic Nun to engage with local agencies and government on how to address the medium-term MHPS effects of the war. The first author undertook a series of visits and consultations and an extensive literature review on the MHPS impact of the war. The data presented here represents a distillation of first-hand experiences gained during successive visits together with evidence gleaned from existing records and documents. Based on these sources, we review briefly the history of the conflict pertaining to the MHPS impact of the war, and our direct observations from community consultations to reflect on the level of local interest in addressing MHPS issues and the capacity within Bougainville to mount an effective response. We conclude by making preliminary recommendations aimed at assisting in building the capacity in Bougainville to address MHPS needs. In undertaking this task, our explicit intention is to avoid the language of blame in relation to the causes or consequences of the conflict.
Brief history of the Bougainville Crisis
We provide only a synopsis of the origins and course of the Bougainville Crisis. The complex mix of ethnic, cultural and economic issues that motivated the conflict has been considered elsewhere [5–7]. In November, 1988, landowners with a range of longstanding grievances associated with the operation of the Panguna mine in central Bougainville, damaged mine property, interrupting production and subsequently resulting in its closure in May 1989 [3, 4, 6]. The mine had provided 45 % of PNG’s export income and 12 % of PNG’s gross domestic product [7]. Armed conflict was triggered in December 1988, when the PNG Police mobile squads and later the Police Defence Force (April 1989) were deployed to the area to facilitate the re-opening of the mine [8]. The police tactics used were regarded as harsh by the indigenous people, igniting longstanding secessionist sentiments in Bougainville [6, 9] which in turn garnered broader support for the protest group who subsequently formed the Bougainville Republican Army (BRA), leading to the initially localized conflict spreading across the province [2].
Failure of PNG police to halt the BRA and growing criticism about its handling of the situation compelled the PNG government to accept a ceasefire in March 1990 [10]. Subsequently, all PNG forces and services were withdrawn from Bougainville [5, 10]. In May 1990, the PNG government imposed a total sea and air blockade on Bougainville, preventing the transportation of all goods into the territory including medical supplies [5, 6]. In the absence of PNG Forces, undisciplined factions of the BRA targeted specific groups within Bougainville (the wealthy, well-educated, senior government officers and those suspected of co-operating with the PNG government), resulting in an escalating internecine conflict fuelled by pre-existing feuds and land disputes, in some instances, resulting in frankly criminal acts [3, 4, 6, 8].
In response to a request by Bougainville leaders concerned about the ongoing violence, in September 1990, the PNG Defence Force returned to the administrative centre, Buka Island, to restore and maintain the security and safety of villagers [5]. In July, 1992, the newly elected PNG government took a more assertive position to re-establish control of other parts of Bougainville [8]. In the period 1992–1993, the Bougainville Resistance Forces (BRF) formed in opposition to the BRA, aligning with and supported by the PNG Defence Force [4, 8]. It has been argued that the BRF “bore the brunt of the fighting” on the PNG government side [2]. Armed conflict continued through to the commencement of the peace process in July 1997, and conflict, deaths and injuries continued [6] until February 1999, when the cease-fire agreement was signed, followed in April 2001 by the adoption of the comprehensive Bougainville Peace Agreement [4, 8]. The agreement established Bougainville as an autonomous region within PNG, embodying a commitment to holding a referendum on independence for the territory at some point between 2015 and 2020 [11].
Methods
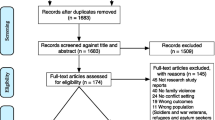
We applied two approaches to assess the longer-term MHPS impact of the Bougainville. First, a review of the literature was conducted to identify the conflict-related events that were likely to have impacted on the longer-term MHPS of the Bougainville population. DT searched key databases including MEDLINE, EBSCO Psychology and Behavioural Sciences Collection, PsycINFO, SocINDEX, PsycARTICLES and internet search engines (Google, Yahoo) using the following terms: Bougainville, Bougainville Crisis, Bougainville war AND psychology, psychiatry, mental health, trauma and impact. While no systematic investigations of the MHPS impact of the war were found, various reports documented events that occurred during the war that, according to past research and knowledge from similarly conflict-affected countries were deemed likely to have had a MHPS impact. Reports referred to herein were compiled by official investigators, academics and others who we judged had applied investigative rigour and impartiality to their assessments. Credibility was judged by the identification of sources, accurate specification of dates and locations, and adequacy of the detail given, for example, in identifying the key groups involved (BRA, PNG, BRF). Reports that were based primarily on opinion or appeared to be advocating for a particular side in the conflict were excluded.
Second, during three successive field visits (2009, 2011, 2013), DT made a detailed inquiry into the extent of exposure of the population to conflict-related events, community perceptions regarding current MHPS issues, the level of interest amongst a wide range of stakeholders to address MHPS issues, and the capacity within Bougainville to address these needs. During the 2013 field visit, the Bougainville Mental Health Steering Committee, comprised of local stakeholders, was established to pursue preliminary steps to building capacity in Bougainville in order to address MHPS issues. Subsequently, in 2014, DT, DS and PB were contracted by Counterpart International (an international not for profit organization) with support from USAID to work with the Bougainville Mental Health Steering Committee (including BM, LG, EB) to develop a strategic framework to address MHPS issues. Table 1 provides an overview of the community consultation activities conducted during the three field trips (2009, 2011, 2013) and the joint consultation (2014).
Results
Findings: literature review
Table 2 provides a summary of the events that occurred during the war identified by the literature review and likely to contribute to ongoing MHPS issues. Estimates of the number of war deaths vary considerably, but a figure of between 15,000 and 20,000 appears to be most widely accepted in Bougainville. Most deaths involved civilians. Other events relevant to MHPS were the displacement of more than half of Bougainville’s population; the perpetration of wide-scale human rights abuses; undermining of the traditional authority of elders and women, cultural values and relationships; property damage; and major disruptions to education and the economy. Participants engaged in the series of consultations during field visits affirmed the importance and widespread nature of the conflict-related events listed in Table 2. The consensus view, however, was that the data gleaned from the literature review underestimated the scale and gravity of the events that occurred during war and their likely contribution to ongoing MHPS issues [14].
Findings: community perceptions of ongoing MHPS issues and the need to address these issues
Table 3 summarizes community perceptions regarding current MHPS issues among specific groups and across the broader community that were consistently identified across a sequence of consultations (2009, 2011, 2013, 2014) and, where available, from research and existing documentation. Absence of epidemiological data, with the exception of information regarding domestic violence and sexual assault [27, 28], limits the extent to which the prevalence of the problems identified in Table 3 can be specified. Nevertheless, in personal communication with DT, Mr. Beleh (local politician) and Sr. Garasu (Catholic Nun) reported that they had identified 232 ex-combatants as manifesting one or more MHPS problems arising from the conflict in one of Bougainville’s 33 political constituencies. Those who were children/adolescents during the war (the lost generation) were reported as having limited education, a lack of engagement in traditional values and activities and displaying aberrant behaviours all of which contribute to their marginalization in the community. Many of this group experienced events during the war likely to have been traumatic [14, 24] and while the numbers who continue to be impacted by these experiences is yet to be determined, an expatriate Marist Brother teacher/counsellor noted that most of 50 male students he taught had been involved in combat and appeared to be suffering from symptoms of post-traumatic stress [24]. Various reports, largely based on community perceptions, have highlighted the detrimental effects of the conflict on subsequent risk of substance abuse [14, 23, 29, 30]. Gender-based violence including sexual violence is considered a significant issue in Bougainville [27, 28] and thought to continue at a higher rate compared to that prior to the war. The number of people missing presumed to have died during the war is unknown, but the inability to conduct customary burial ceremonies was reported as resulting in complicated grief for the surviving relatives and as having broader impacts including land title and use issues [14]. Meetings with senior police personnel highlighted the difficulties the police force experience in carrying out their duties amongst a community impacted by the war and its aftermath [14] and by some officers who continue to be impacted by their personal war experiences. People continue to be displaced since the war and family separation, separation from traditional land, insecure living circumstances and the strain on host communities/families were reported as continuing impacts [14]. Finally, our informants reported a trans-generational impact on those born after the war through their exposure to a range of trauma-related aberrant behaviours displayed by parents and within the community at large.
Collectively, the MHPS identified were described as having a broad impact on the social fabric of Bougainville society and, indirectly, on economic recovery. Across the sequence of consultations (2009, 2011, 2013, 2014) there was a broad consensus concerning the priority need to address MHPS issues to reduce the distress experienced by individuals and the burden of associated disturbed behaviours on families, community, health services, the police, the judiciary and educational institutions. The overarching view of our informants was that addressing MHPS issues, particularly trauma related aberrant behaviours had the potential to: assist in healing relationships damaged during and since the conflict; support efforts to maintain and enhance the peace process; and encourage the re-engagement of those affected in purposeful and productive family, community and economic activity. It was recognized that, in addition to the need for MHPS services, traditional reconciliation ceremonies in which perpetrator(s) compensate victims, might play a complementary role in achieving healing for sides of the conflict.
Findings: current resources to address MHPS issues
While a range of government, non-government (secular, faith-based, voluntary) services, agencies and groups are confronted by MHPS issues in their daily work, only a few agencies are specifically focused on assisting persons with these problems. Two such agencies are the Nazareth Centre, which provides refuge for women and other survivors of family violence, youth who have substance abuse issues and treatment for former combatants; and the Leitana Nehan Women’s Development Agency who provide counselling and referral related to gender based violence, trauma-related awareness raising programs and training for community based organizations.
In addition to the limited number of trained staff to address MHPS issues across Bougainville, there are minimal resources to attend to people with severe mental disorders including those with psychotic disorders (schizophrenia, bipolar disorder, and other psychotic disorders), neuropsychiatric conditions/brain disorders, severe mood disorders and chronic traumatic stress disorders that are typically found in low-income, post-conflict settings [32–34]. Yet at the time of writing, there is only one mental health nurse for the total Bougainville population of 254,000 persons. Patients referred to the national hospital are assessed and treated by the mental health nurse supported by hospital physicians, noting that the hospital is distant from and difficult to access from many areas of Bougainville. The only options for care for the more severely disturbed patients referred to the hospital are short-term accommodation in a centre designed principally to provide refuge for women experiencing domestic violence; being held in police cells with criminal offenders; or being transported by air (with medical and police escort) to the national capital, Port Moresby, for specialist treatment. The inadequacies of the system add credence to observer reports that the mentally ill are at risk of neglect (and in some cases abuse) throughout Bougainville.
This brief overview indicates that while key individuals and agencies have worked valiantly over many years to address MHPS issues, it is evident that the capacity within Bougainville to address these issues is severely limited relative to the demand and this has been noted in a number of reports [14, 23]. The issues identified during the consultations constraining the capacity in Bougainville to address current MHPS issues are in Table 4.
On the positive side, important facilitating factors were made evident during the consultations regarding the potential to address MHPS issues, as outlined in Table 5. A clear recognition of the need to address MHPS was identified throughout the consultation process as was a strong interest in building Bougainville’s capacity to address these needs and the Government’s interest in developing the necessary supportive policy and legislative framework.
Discussion
It is widely accepted within Bougainville that the Crisis left in its wake a range of MHPS issues that require urgent attention. Specific groups have been identified as at high risk of MHPS problems but research in similar situations would suggest a broader community impact. There has also been no assessment of the numbers or needs of those who have severe mental disorders in Bougainville, nor the needs of their families. Although it has been generally assumed that 2 % of any population have a severe mental disorder, findings from a comparable population (Timor-Leste) have found a figure closer to 3 % [33]. In other post-conflict low resource countries up to a third of exposed persons have been found to experience broadly defined traumatic stress reactions [35], and those directly exposed to the more severe traumas of mass conflict (including torture, other forms of human rights abuses, combat, exposure to murder, gender-based violence) have an increased risk of experiencing a range of disorders and reactions including complex PTSD, prolonged grief, explosive anger, somatoform disorders, drug and alcohol problems and psychotic-like reactions (often presenting as culturally specific reactions) [36, 37]. The majority of the Bougainville population has directly experienced war or its aftermath including ongoing violence, stress, and/or physical and economic disruption. Informants in our consultations (2009, 2011, 2013, 2014), supported by relevant research/reports highlighted the following as significant current mental health issues: substance abuse [14, 23, 29]; gender based violence including sexual assault [14, 27, 28]; displacement-related stressors [14]; complicated grief and land title/use issues for relatives who are unable to perform customary burial rituals for missing persons thought to have died during the war [14]. Adverse trans-generational effects amongst those born after the war exposed to a range of trauma-related aberrant behaviours in parents and the society at large was also reported by informants. The widespread erosion of the social and cultural fabric of the society has had negative impacts at a population level, adding to a context of psychosocial vulnerability and hence, risk of mental disorder. At the societal level, undermining of the economy, the capacity of conflict-affected persons to use existing resources and constraints in the institutional framework to address these issues have severely limited the capacity of Bougainville to attend effectively to the broad psychosocial needs of the population as well as to specific mental health and traumatic stress problems experienced by a substantial minority.
Limitations
There is a lack of systematic and comprehensive data concerning MHPS needs in Bougainville [14]. The data cited in this paper therefore can only provide indicators of need based on broad observations and estimates. The consultation process undertaken did not include the collection of demographic information and it is therefore unclear to what extent the views of the informants is representative of the population. Further, while informants consistently reported that gender based violence, including sexual assault, and substance abuse have continued at a higher rate compared to that prior to the war, there are no pre-war data to allow comparison. There may also be an attributional bias within Bougainville (as in other conflict-affected settings) in assigning responsibility for most current MHPS to the direct or indirect impacts of the war.
Recommendations
A sequence of consultations (2009, 2011, 2013, 2014) identified that mental and psychosocial problems are a priority in Bougainville, and that there is broad support amongst politicians, senior public servants, service providers and the general community to build Bougainville’s capacity to address these issues. There appears to be a consensus that addressing MHPS issues would reduce the distress experienced by individuals with MHPS problems and the burden experienced by families and others caring for them. Further, unresolved trauma has been associated with a range of aberrant behaviours (e.g. violence including gender based violence and sexual assault, substance abuse) impacting the community at large, as well as a range of specific services (e.g. police, health) and, more broadly, economic activity [14, 23, 24]. It is anticipated that the provision of appropriate treatment and support for those affected will have broad community benefits, including contributing to the ongoing peace process [14].
The following recommendations, developed in close collaboration with the Bougainville Mental Health Steering Committee, have been submitted to the Autonomous Bougainville Government for review [12]. (1) To conduct systematic research regarding MHPS needs, current practice in caring for the mentally ill, and service provider capacity. (2) To use the resulting data to develop a comprehensive mental health model for Bougainville. The model would include three service levels (village-based, community level health service and hospital based mental health service) dependent on an assessment of need and response to treatment, and a referral system between the various levels of service. It could include community based psychosocial support and psychotherapy approaches for PTSD, depression, and anxiety that have been found to be effective in other low resource environments (e.g. [38–40]). The service delivery model would incorporate the building of institutional and worker capacity with strategies and ongoing resources to ensure sustainability and the mainstreaming of mental health services as an essential component of overall health service development. (3) To similarly develop and test strategies to raise awareness and advocacy to highlight mental health within the broad community with the aim of improving knowledge of and support for those with mental health issues and their families. (4) To develop an overarching mental health policy, based on these findings and available literature, with the aim to provide sustained and accessible services to the Bougainville population.
Conclusion
Although systematic data are lacking, existing information suggests that the majority of people in Bougainville have been significantly affected by the trauma, stress and disruptions resulting from the war. There is an immediate need and a strong interest within Bougainville for assistance to build local capacity to address MHPS issues. This situation warrants assertive and immediate action in relation to the more precise delineation of the mental health status of the Bougainville people and development of comprehensive services to address the multiple needs of the population.
References
Alpers P, Twyford C. Small arms in the Pacific. Geneva: Small Arms Survey; 2003. http://www.smallarmssurvey.org/fileadmin/docs/B-Occasional-papers/SAS-OP08-Pacific.pdf. Accessed 18 Feb 2016.
Boege V. Peacebuilding and state formation in post-conflict Bougainville. Peace Review J Soc Justice. 2016;2009(21):29–37. doi:10.1080/10402650802690037 (Accessed 18 Feb 2016).
Claxton K. Bougainville 1988–1998: five searches for security in the North Solomons Province of Papua New Guinea. Canberra: Strategic and Defence Studies Centre, Research School of Pacific and Asian Studies, Australian National University, Canberra; 1998. http://ips.cap.anu.edu.au/sites/default/files/130%20Bougainville%201988-98%20%20Five%20Searches%20for%20Security%20in%20the%20North%20Solomons%20Province%20of%20Papua%20New%20Guinea.%20Canberra%20Papers%20on%20Strategy%20and%20Defence%20No.%20130%20Karl%20Claxton%20209p_073152750X.pdf. Accessed 18 Feb 2016.
Braithwaite J, Charlesworth H, Reddy P, Dunn L. Reconciliation and architectures of commitment: sequencing of peace in Bougainville. Canberra: ANU E Press; 2010. http://press.anu.edu.au?p=57571. Accessed 4 July 2015.
Oliver D. Black Islanders: A personal perspective of Bougainville 1937–1991. Melbourne: Hyland House; 1991.
Regan AJ. Current developments in the Pacific: causes and course of the Bougainville conflict. J Pacific Hist. 2016;1998(33):269–85. doi:10.1080/00223349808572878 (Accessed 18 Feb).
Carruters DS. Some implications for Papua New Guinea of the closure of the Bougainville copper mine. In: May RJ, Spriggs M, editors. The Bougainville Crisis. Bathurst: Crawford House Press; 1990. p. 38–44.
Regan A. Light Interventions: lessons from Bougainville. Washington: Institute of Peace; 2010.
Reddy P. Reconciliation in Bougainville: civil war, peacekeeping and restorative justice. Contemporary Justice Review: Issues in Criminal, Restorative and Social Justice. 2016;2008(11):117–30. doi:10.1080/10282580802057744 (Accessed 18 Feb).
Amnesty International. Papua New Guinea: under the barrel of a gun—Bougainville 1991–1993; 1993. https://www.amnesty.org/en/documents/asa34/005/1993/en/. Accessed 4 July 2015.
Bougainville Peace Agreement. 2001. http://www.usip.org/sites/default/files/file/resources/collections/peace_agreements/bougain_20010830.pdf. Accessed 18 February 2016.
Tierney D, Silove D, Bolton P. Strategic mental health framework to address mental health and psychosocial issues in the Autonomous Region of Bougainville. 2015.
United Nations. Papua New Guinea common country assessment. 2001. http://www.asia-pacific.undp.org/content/damrbap/docs/programme-documents/cca/PG-CCA-2001. Accessed 4 July 2015.
United Nations. Universal periodic review on Papua New Guinea: Bougainville civil society stakeholder report to OHCHR. 2011. https://archive.org/details/UPRAROB2011ShadowReport. Accessed 4 July 2015.
Havini M. A compilation of human rights abuses against the people of Bougainville 1989–1995. New South Wales: Bougainville Freedom Movement; 1995.
Joint Standing Committee on Foreign Affairs, Defence and Trade. Bougainville: The Peace Process and Beyond. 1999. http://www.aph.gov.au/parliamentary_business/committees/house_of_representatives_committees?url=jfadt/bougainville/bvrepindx.htm. Accessed 4 July 2015.
Garasu L. The role of women promoting peace and reconciliation. In: Carl A, Garasu L, editors. Accord: Weaving consensus—the Papua New Guinea-Bougainville Peace Process. London: Conciliation Resources; 2002. p. 28–31. http://www.c-r.org/resources/weaving-consensus-papua-new-guinea-bougainville-peace-process. Accessed 4 July 2015.
Amnesty International. Bougainville: the forgotten human rights tragedy. 1997. https://www.amnesty.org/en/documents/asa34/001/1997/en/. Accessed 4 July 2015.
Havini M. A compilation of human rights abuses against the people of Bougainville 1989–1996: vol. 2. New South Wales: Bougainville Freedom Movement; 1996.
United Nations. Report of the Special Rapporteur on extrajudicial, summary or arbitrary executions. Economic and Social Council Commission on Human Rights. 1996. http://www1.umn.edu/humanrts/commission/country52/4-add2.htm Accessed 4 July 2015.
Braithwaite J. Rape, shame and pride. J Scandinavian Stud Criminology Crime Prevention. 2015;2006(7):2–16. doi:10.1080/14043850601029059 (Accessed 4 July 2015).
Nash J. Factors relating to infrequent domestic violence among the Nagovisi. Pacific Stud. 1990;13(3):127–40.
Howley P. Breaking spears and mending hearts: peacemakers and restorative justice in Bougainville. NSW: Federation Press; 2002.
Howley P. Restorative justice in Bougainville. Development Bulletin. 2000; 53: 23–5. https://crawford.anu.edu.au/rmap/devnet/dev-bulletin.php. Accessed 4 July 2015.
Thompson H. The economic causes and consequences of the Bougainville crisis. Res Policy. 1991;17:69–85. doi:10.1016/0301-4207(91)90027-S.
Scales I, Craemer R, Thappa I. Market chain in development: Australia’s roads, wharves and agricultural projects in post-conflict Bougainville. Australian Agency for International Development; 2008. http://www.ausaid.gov.au/publications/pdf/Bvlle_market_chain_report_Feb08.pdf?bcsi_scan_D4A612CF62FE9576=0&bcsi_scan_filename=Bvlle_market_chain_report_Feb08.pdf. Accessed 5 Feb 2015.
Fulu E, Jewkes R, Roselli T, Garcia-Moreno C. Prevalence of and factors associated with male perpetration of intimate partner violence: findings from the UN multi-country Cross-sectional Study on Men and Violence in Asia and the Pacific. Lancet Global Health. 2013;1(4):e187–207. doi:10.1016/S2214-109X(13)70074-3.
Jewkes R, Fulu E, Roselli T, Garcia-Moreno C. Prevalence of and factors associated with non-partner rape perpetration: findings from the UN multi-country Cross-sectional Study on Men and Violence in Asia and the Pacific. Lancet Global Health. 2013;1(4):08–218. doi:10.1016/S2214-109X(13)70069-X.
National HIV/AIDS Support Project. Situational analysis for strategic planning at a district level, Bougainville Province, social mapping project. National Aids Council of Papua New Guinea, Port Moresby; 2004. http://staging.nacs.org.pg/resources/documents/Bougainville_Report.pdf. Accessed 9 Feb 2011.
United Nations. Convention on the elimination of all forms of discrimination against women. 2009. https://archive.org/details/PNGCEDAWReportMay09. Accessed 18 Feb 2016.
https://www.icrc.org/en/document/papua-new-guinea-bougainville-government-adopts-missing-persons-policy. Accessed 18 Feb 2016.
Silove D, Ekblad S, Mollica R. The rights of the severely mentally ill in post-conflict societies. Lancet. 2016;2000(355):1548–9. doi:10.1016/S0140-6736(00)02177-2.
Silove D, Manicavasagar V, Baker K, Mausiri M, Soares M, de Carvalho F, Soares A, Fonseca Amiral Z. Indices of social risk among first attenders of an emergency mental health service in post-conflict East Timor: an exploratory investigation. Aust N Z J Psychiatry. 2004;38:929–32. doi:10.1080/j.1440-1614.2004.01483.x.
Silove D, Bateman CR, Brooks RT, Fonseca CA, Steel Z, Rodger J, Soosay I, Fox G, Patel V, Bauman A. Estimating clinically relevant mental disorders in a rural and an urban setting in postconflict Timor Leste. Arch Gen Psychiatry. 2008;65:1205–12. doi:10.1001/archpsyc.65.10.1205.
Steel Z, Chey T, Silove D, Marnane C, Bryant RA, van Ommeren M. Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: a systematic review and meta-analysis. JAMA. 2009;302:537–49. doi:10.1001/jama.2009.1132.
Rees S, Silove D. Sakit Hati: a state of chronic mental distress related to resentment and anger amongst West Papuan refugees exposed to persecution. Soc Sci Med. 2011;73:103–10. doi:10.1016/j.socscimed.2011.05.004.
Silove D, Ivancic L, Rees S, Bateman-Steel C, Steel Z. Clustering of symptoms of mental disorder in the medium-term following conflict: an epidemiological study in Timor-Leste. Psychiatry Res. 2014;219:341–6. doi:10.1016/j.psychres.2014.05.043.
Bolton P, Bass JK, Zangana G, Kamal T, Murray S, Kaysen D, Lejuez CW, Lindgren K, Pagoto S, Murray LK, Van Wyk S, Ahmed A, Mohammad Amin NM, Rosenblum M. A randomized controlled trial of mental health interventions for survivors of systematic violence in Kurdistan, Northern Iraq. BMC Psychiatry. 2014;14:360. doi:10.1186/s12888-014-0360-2.
Bolton P, Bass J, Neugebauer R, Clougherty K, Verdeli H, Ndogoni L, Wickramaratne P, Weissman M. Results of a Clinical Trial of a Group Intervention for Depression in Rural Uganda. JAMA. 2003;289:3117–24. doi:10.1001/jama.289.23.3117.
Weiss WM, Murray LK, Zangana GA, Mahmooth Z, Kaysen D, Dorsey S, Lindgren K, Gross A, Murray SM, Bass JK, Bolton P. Community-based mental health treatments for survivors of torture and militant attacks in Southern Iraq: a randomized control trial. BMC Psychiatry. 2015;15:249. doi:10.1186/s12888-015-0622-7.
Authors’ contributions
All authors participated in the consultation process undertaken to determine mental health needs in Bougainville. DT conducted a review of the literature and wrote a draft of this paper which was revised significantly following reviews by DS and PB. All authors read and approved the final manuscript.
Acknowledgements
We would like to thank the many people consulted in Bougainville and the following for their encouragement, advice and feedback about earlier drafts of this paper: Dr. Clement Malau, former Secretary, Health Department, Papua New Guinea; Dr. Peter Cook, Clinical Psychologist, Essendon, Victoria, Australia; and Professor Henry Jackson, Department of Psychology, Melbourne University, Victoria, Australia. We also appreciate the helpful comments made by an anonymous reviewer about an earlier draft of this paper.
Competing interests
The authors declare that they have no competing interests.
Funding
Funding for the 2014 Consultancy was provided by Counterpart International as part of a 2-year Women Peace Building Initiatives project in Bougainville supported by USAID. The program aims to address the issues of gender empowerment, civil society capacity building, post-conflict recovery, policy development and advocacy.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Tierney, D., Bolton, P., Matanu, B. et al. The mental health and psychosocial impact of the Bougainville Crisis: a synthesis of available information. Int J Ment Health Syst 10, 18 (2016). https://doi.org/10.1186/s13033-016-0054-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13033-016-0054-x