
Abstract
Sexual violence and intimate partner violence are exacerbated by armed conflict and other humanitarian crises. This narrative systematic review of evidence for interventions to reduce risk and incidence of sexual and intimate partner violence in conflict, post-conflict and other humanitarian crises, updates and expands our review published in 2013. A search of ten bibliographic databases for publications from January 2011 to May 2020 used database specific key words for sexual/intimate partner violence and conflict/humanitarian crisis. The 18 papers, describing 16 studies were undertaken in conflict/post-conflict settings in 12 countries. Six intervention types were reported: i) personnel; ii) community mobilisation; iii) social norms; iv) economic empowerment; v) empowerment; and vi) survivor responses, with the most common being economic empowerment (n = 7) and gendered social norms interventions (n = 6). Combined interventions were reported in nine papers. Four studies identified non-significant reductions in incidence of sexual/ intimate partner violence, showing an evident positive trend; all four evaluated gendered social norms or economic empowerment singly or in combination. Evidence for improved mental health outcomes was found for some economic empowerment, social norms and survivor interventions. Some evidence of reduced risk of sexual violence and intimate partner violence was identified for all intervention types. Qualitative studies suggest that experiences of social connection are important for women who participate in programming to address sexual and intimate partner violence. Interventions with multiple strategies appear to hold merit. Achieving and demonstrating reduced sexual and intimate partner violence remains challenging in this context. Future research should continue to explore how social norms interventions can be most effectively delivered, including the impact of including mixed and same sex groups. Work is needed with local partners to ensure programs are contextually adapted.
Similar content being viewed by others


Introduction
Gender-based violence, prevalent during peace, is exacerbated in armed conflict and other humanitarian crises [1,2,3,4]. This review focuses specifically on sexual violence and intimate partner violence, two most prevalent forms of gender-based violence. Sexual violence is defined as “any sexual act, attempt to obtain a sexual act, unwanted sexual comments or advances, or acts to traffic, or otherwise directed against a person’s sexuality, using coercion, by any person, regardless of their relationship to the victim, in any setting, including, but not limited to, home and work” [5] (p. 149). Intimate partner violence refers to “a pattern of behaviour by a current or former partner causing physical, sexual or psychological harm, such as physical aggression, sexual coercion, psychological abuse and/or controlling behaviours.”[6] (p. vii).
Available estimates for prevalence of sexual violence among women in humanitarian emergencies range from 21 to 53% [7,8,9] and for intimate partner violence 12–80%, [10,11,12,13,14] although prevalence in this context are considered to be under-reported. [15,16,17] Forms of sexual violence are perpetrated by armed actors, aid workers, peacekeepers, intimate partners, family and community members. Sexual violence and intimate partner violence can result in serious long term physical and mental health effects [18, 19], including adverse pregnancy outcomes, maternal mortality, and sexually transmitted infections, as well as heightened risk of stigma, isolation, stress, reduced ability to negotiate sex, forced pregnancy, and unsafe sexual practices [7, 10,11,12, 20,21,22,23].
Factors exacerbating sexual violence and intimate partner violence in crises include: exposure to armed conflict; increased availability of weapons; perceived threats to masculinity; increased substance abuse; human rights abuses; extreme poverty; loss of livelihoods; disrupted family and community protection structures; traumatic stress; loss of legal and protective mechanisms; disability; pre-existing intimate partner violence; transactional sex, and lost access to basic resources [1, 9,10,11, 20, 21, 23,24,25,26,27,28,29,30].
Background
This systematic review updates and expands one published in 2013 on evidence for interventions to reduce incidence and risk of sexual violence in contexts of conflict, post-conflict and other humanitarian crises [31, 32]. That review found some evidence of decreased sexual violence in association with firewood distribution and from programming to reduce sexual exploitation by peacekeepers. Apparent increased risk occurred through lack of protection, stigma and retaliation associated with interventions. Significant barriers were identified which prevented women seeking help after sexual violence, although multiple component interventions and sensitive community engagement appeared to contribute to positive outcomes [31].
Documentation of intimate partner violence in humanitarian contexts has shown that it is as, or more, prevalent than sexual violence [15] which has led to the increased recognition of the need to address intimate partner violence and other forms of gender-based violence in these settings. Furthermore, the call to address the social and economic drivers of gender-based violence in emergencies have expanded the focus beyond survivor response to also include primary prevention [16]. Initiatives driving this work include the ‘IASC Guidelines for Integrating Gender-Based Violence Interventions in Humanitarian Action’ outlining actions for mitigating risk of and preventing gender-based violence [33], as well as the What Works? Research consortium-seeking evidence on preventing violence against women and girls, including in conflict and humanitarian crises. Further appraisal of the evidence has occurred through systematic reviews of programming for gender-based violence in refugee settings [4, 34] and of psychosocial support interventions in conflict zones [24, 35]. Post-settlement programs are not included, given the different context in which these are provided and accordingly, scope is restricted to low and middle income countries. This review examines trends in prevention and reduction of risk of sexual violence and intimate partner violence across conflict, post–conflict and other humanitarian settings, a current gap in the literature.
Methodology
This review sought to answer the question: What is the evidence of the impact of programmes/interventions to reduce risk and incidence of intimate partner violence and sexual violence in conflict and post-conflict states and other humanitarian crises in low and middle income countries? While recognising that other forms of gender-based violence are prevalent, given the wide scope of this review we excluded interventions which address: trafficking and female genital mutilation; directed towards children, apart from those related to preventing early, child and forced marriage, or where these are part of interventions aimed at intimate partner violence and sexual violence. This review recognises men may be affected by sexual violence especially during conflict, however focused on abuse directed towards women, given higher risk and prevalence for women [6, 13, 15]. The review is registered with PROSPERO, CRD42020186405.
Conceptual framework
Our approach built on the conceptual framework applied in the 2013 review, updated based on advice from the WHO and an expert panel convened by the WHO. Drawing on an ecological approach, interventions were conceptualized as operating at the level of individual, family, community or society [36] (Table 1) recognising that multi-strategy programs which span different levels are increasingly delivered in humanitarian contexts.
Reducing incidence of sexual violence and intimate partner violence is a long-term outcome, which is difficult to achieve and measure accurately in any context, but particularly in crisis settings. Reduced risk is a key intermediate outcome. A non-exhaustive list of indicators adapted from Violence Against Women and Girls: A Compendium of Monitoring and Evaluation Indicators (Bloom 2010) used in the 2013 review, was updated to reflect inclusion of intimate partner violence and to incorporate elements of the RESPECT Women framework which reflects current approaches to gender based violence prevention [37] (Additional file 1). Inclusion and exclusion criteria (Table 2) were determined with advice from the expert panel. We included interventions delivered to refugee/migrant women in Greece, although it is not a LMIC, given the large number of refugee arrivals directly to this country.
Searches
Searches were conducted in May 2020 on the following databases: CINAHL; Cochrane Library; EMBASE; GlobalHealth; Johanna Briggs Institute EBP; Proquest; PTSDPubs; PSYCInfo; Pubmed Central; Scopus. Search terms for “sexual violence” or “intimate partner violence” and “conflict” or “post-conflict” or “humanitarian crisis” and their synonyms were used to search key terms/subject, title and abstract. The search of the PsycINFO database is reported in Fig. 1 as an example of the approach used. Grey literature was hand-searched via: Institutional Repository for Information Sharing, Google Advance and Campbell Collaboration database using the same search terms.

Sample search strategy (Psycinfo)
Screening and quality review
The title and abstracts, and then full-text were screened by pairs of team members independently. Divergent results were resolved by the team as a whole. The Johanna Briggs Institute (JBI) Quality Appraisal Checklists (http://joannabriggs-webdev.org/research/critical-appraisal-tools.html were applied to assess quality of papers, selected as these tools allow for diverse study types to be assessed. These tools assess the methodological quality including the risk of bias which may be present in research design and analysis. Team members in pairs double assessed individual studies, (LK, CM, DRG, CTA) with one team member (JS) reviewing the overall results. Quality was not used to exclude studies.
Data extraction and analysis
Using a standardized template, data were extracted and coded by two team members on: country of intervention; strategy type; intervention; target population; duration and intensity of intervention; study design and participants; organization type; context; reported outcomes and unintended consequences. Studies were also rated for decrease/increase or no change to risk or incidence of sexual violence/intimate partner violence. Data were analysed as a team using narrative synthesis [38], involving close reading of each text and consideration of each strategy type against the review questions: evidence for i) reduced incidence of sexual violence/intimate partner violence; ii) reduced risk of sexual violence/intimate partner violence as a result of interventions, including identification of new indicators as agreed by the team; and iii) impacts of secondary prevention interventions on survivors’ wellbeing. Qualitative findings were used to amplify and contextualize results from quantitative studies.
Results
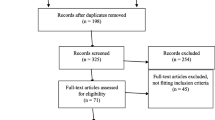
The search strategy yielded 4794 records reduced to 2898 after de-duplication. Screening for title and abstract yielded 90 titles, reduced to 18 papers following full text review (Fig. 2). Only one inclusion was identified through the grey literature search [39].

Search strategy and filtering
Studies identified
Eighteen articles were included in the review, reporting results from 16 separate studies, summarised in Table 3. Articles by Gupta, Falb et al. [40], Falb, Annan et al. [41] and Annan, Falb et al. [42] all reported on a single intervention addressing economic empowerment and social norms as denoted by * in Table 3. Interventions were conducted in 12 countries, with the greatest number (n = 5) occurring in the Democratic Republic of Congo (DRC). Nine studies were conducted in post-conflict, five in conflict and two in combined conflict and post-conflict settings. All humanitarian crises were in scope, however no studies which met the inclusion criteria were identified from disaster or epidemic settings. Seven of the 16 included studies targeted intimate partner violence, seven targeted both sexual violence and intimate partner violence, while two addressed sexual violence only.
Of the 16 possible intervention types identified in the conceptual framework, (Table 1) evidence was found for six: i) personnel; ii) community mobilisation; iii) social norms; iv) economic empowerment; v) empowerment and; vi) survivor responses. Almost half (n = 7) of the 16 studies combined two intervention types. Duration and intensity of the intervention is indicated in Table 3 for all studies where this was reported. As reported in papers, ten of the interventions were delivered by international non-government organizations (NGOs). Three were delivered jointly by international and local NGOs [42,43,44,45]. Two interventions were implemented by local NGOs alone [46, 47] and one by a state agency [48]. Data were not available for most studies on length of implementation prior to measuring outcomes, with nine run specifically as trials.
Table 4 summarises the evidence for reduced risk and changed incidence of intimate partner violence and/or sexual violence as well as the key impacts of the interventions. Four studies identified reductions in incidence of intimate partner violence [40, 46, 49, 50] and one of sexual and intimate partner violence [51], though none reached statistical significance. One showed reduced intimate partner violence only among a sub-set of women with moderate baseline food insecurity [52]. These six studies evaluated social norms [50, 51], or economic empowerment interventions [46] or both combined [40, 49, 52]. Some evidence of a reduction in factors associated with risk of sexual violence/intimate partner violence was identified in all studies against the identified list of indicators, to which we added five further indicators during the analysis. These were: household poverty reduced; increased economic autonomy for women; changed norms supporting women’s equality; changed norms on unacceptability of gender-based violence in men. In addition, strong evidence was present for projects that focused on economic empowerment [46] and economic empowerment plus social norms [42] for improved mental health outcomes.
Study quality
The JBI quality of evidence assessment was completed for 17 of the 18 papers using tools for: i) randomised control trials (RCTs); ii) qualitative studies and; iii) cohort studies. Lack of a quality tool for case studies precluded an assessment of Bacon et al. As applied in another recent review [53], we converted scores to ratings, identifying ten studies as: Good (84–100%); six studies as Fair (50–84%); and one study as Poor (< 50%). Studies with higher quality scores tended to be cluster RCTs and RCTs while qualitative studies and mixed method studies scored lower. RCTs predominantly displayed true randomization, similar groups at baseline, reliable outcome measures consistently measured across control and intervention groups, but blinded assignment was not in most cases possible due to the nature of the interventions. Qualitative studies tended to be weaker on congruity between philosophical perspective and methodology and addressing the influence of the researcher. Overall the quality of included studies was assessed to be Fair to Good.
Synthesis of findings
The following section synthesizes the studies by intervention type explored by level in the ecological framework from societal to individual level, as reported in Tables 3 and 4. Combined interventions are grouped according to the intervention type that appears to be the primary one.
Personnel
One study was identified at the societal level of intervention. Liberia’s gender sensitive police reform, aimed at increasing the proportion of female officers to 20% alongside creation of a specialist police unit for sexual violence and intimate partner violence, reported as a case study [48]. Successful recruitment occurred, however limited worker capacity building and training, and officer attrition reduced impact. Prosecution cases typically stalled in court, with a weak justice system reported to reduce effectiveness. A quality score is not available for this study, due to lack of suitable tools for case studies.
Community mobilization
At the community level of intervention, one paper reported on community mobilisation as a standalone intervention [45]. The intervention involved community members creating films on gender rights and respectful relationships and screening them to local audiences, to prompt dialogue. A total of 150 films were viewed by a reported 25,000 community members across the five countries (Table 3). Seventy-six interviews and 18 focus groups conducted with community members suggested positive responses to the messaging contained in the videos, with local production in local language by community members being one of the mechanisms of impact. Reported changes by participants included increased reporting of gender-based violence and community leaders taking action on forced marriage. Overall quality of the study was poor with conclusions not clearly linked to the analysis.
Community mobilisation featured as an element of two survivor response studies reported by Hossain et al. [39] and Lilleston et al. [54], further reported below. Lilleston et al.’s qualitative study, suggested that the community mobilisation element resulted in increased awareness of women’s rights among the community. Hossain et al. reported that refugee community workers engaged in activities including forums and discussions with community leaders. In neither study was community mobilisation among the interventions for which outcomes were reported, with both instead focussing on worker and service user experiences of individual interventions. Although community mobilisation is widely implemented as a stand-alone or combined intervention, there are a lack of studies evaluating its impact, perhaps reflecting the challenges and cost of comprehensively measuring impacts.
Social norms
Interventions aiming to change gendered social norms were explored in three cluster RCTs addressing intimate partner violence in post-conflict settings in Côte d’Ivoire, Somalia and the DRC [44, 50, 51]. All interventions involved facilitated group discussions designed to challenge community member beliefs about gendered social norms, creating expectations for gender equitable attitudes and behaviours. Trained community members delivered approximately 16 weekly sessions of discussion (duration not reported) [44, 50, 51]. The Côte d’Ivoire intervention [51] was adapted as the Engaging Men through Accountable Practice (EMAP) programme in the DRC [50]. Both provided discussion groups to men only and though both found some changes to social norms, challenges included ensuring sufficient attendance to achieve program goals. The Communities Care study in Somalia advanced social norms research, first by collaborating with community members to identify relevant norms and then testing a tool for systematically measuring social norms [44]. Delivered to mixed/single sex groups, no data were provided on attendance.
The three studies had fair [50] to good study quality [44, 51]. Lower than anticipated sample sizes limited analysis for both the Côte d’Ivoire and Somalian studies [44, 51], with only one demonstrating reductions in women’s reported physical and sexual intimate partner violence (non-significant) [51]. Overall these interventions showed promising evidence of positive changes in social norms, demonstrated through reported outcomes such as increased male involvement in household tasks, reduced male intention to perpetrate violence, and increased belief in women’s right to refuse sex, though in other respects changes regarding consent were weaker.
Economic empowerment
At the individual level of intervention, one RCT and a qualitative study evaluated economic empowerment, and a further two RCTs combined economic empowerment with social norms interventions. All involved micro-credit strategies, as opposed to cash transfers. Robust findings were found from all three RCTs that rated at the top end of the quality scale. Both of the economic empowerment only interventions involved livestock asset transfer. Pigs for Peace was offered in the DRC, with 18 month follow up finding reduced experience and perpetration of psychological abuse compared to controls [46]. Only half of the sample were partnered, leading to insufficient power for the intimate partner violence outcomes, and accordingly, non-significant results. However, significant improvement was found on subjective health, PTSD, anxiety symptoms and asset ownership (Table 4). Solidarity Groups, the second economic empowerment only intervention, additionally offered shared farming and group loans [47]. Like the first intervention, eligibility was not restricted to those who had experienced sexual violence/intimate partner violence to avoid stigma. Participants in this qualitative study reported economic and mental health benefits, as well a stronger sense of connection and security from working alongside other women [47].
Economic empowerment via group savings was combined with a gender norms strategy comprising eight gender dialogue groups for women and their partners, in the EA$E intervention in the Cote D’Ivoire [40,41,42]. Evaluated through an RCT comparing group savings alone to group savings with the addition of gender dialogue groups, the intervention messaged non-violence at home, respect and valuing women’s contributions to the household. Follow up 6–8 months post intervention, found economic abuse significantly reduced, but not other forms of intimate partner violence, apart from among couples attending > 75% of sessions. Mental health results from the same study [42] were mixed. Overall, women in the intervention arm were significantly less likely to meet criteria for PTSD, not extended to women experiencing intimate partner violence at baseline, though PTSD scores started from a higher base for this group. A qualitative study reporting experiences of 14 male participants, suggested that mechanisms of change for reduced economic abuse, included increased communication and joint decision making around finances [41].
Green et al. [49] also added a gender norms component to an economic empowerment program, which had previously resulted in increased controlling behaviour by partners. In the second iteration reported in the study, women were invited to include their partner/male relative to attend the training program. Women participants reported small decreases in abuse and control, and overall increases in the quality of their relationships, but less autonomy and influence over household purchases. Gibbs et al. [52] combined a monthly cash stipend with vocational, social empowerment, numeracy and savings training for women in Afghanistan. Women reported less gender inequitable attitudes, decreased food insecurity and greater involvement in household decision-making, but the intervention did not impact on intimate partner violence or depression. A sub-sample of women with baseline moderate food insecurity did however, experience reduced physical intimate partner violence, which the authors suggested may be due to greater impact of livelihood support on this group than on those with severe or nil food insecurity. Low retention may have influenced the impact of combined interventions which relied on men’s participation, with only 46% of both women and men attending 75% of EA$E sessions.
From these studies it is evident that economic empowerment programs, involving micro-credit strategies, with and without social norms strategies, have some potential to reduce abuse, and importantly improve women’s wellbeing in other ways. It is not clear that inclusion of male partners in targeted sessions accompanying economic empowerment programs is sufficient to address potential increases in economic abuse and achieving attendance by males remained elusive.
Empowerment
Two papers from a larger study investigated the efficacy of COMPASS—an empowerment program—to reduce girls’ experiences of violence [55, 56]. Both papers focused on conflict/ post-conflict settings in Ethiopia and the DRC respectively. COMPASS provides safe spaces, life skills and social assets, and mentors, accompanied by parallel caregiver groups. COMPASS in Ethiopia [55] consisted of 30 life skills sessions of 75 to 90 min delivered in in three refugee camps to South Sudanese girls aged 13–19 years. The intervention was complemented by 8 sessions for caregivers aimed at enhancing emotional, parental and support skills (session length not reported). In Ethiopia the focus was primarily on life skills and safe spaces, the later DRC trial enhanced the caregiver intervention [56] also providing to adolescent girls aged between 10 and 14 years 32 life skills sessions of 1–3 h duration, with caregivers in the intervention group receiving 13 sessions, substantially more than in the Ethiopian study. At 12-month follow up neither study demonstrated evidence of reduced girls’ exposure to sexual, physical or emotional violence, or transactional sex. However, in Ethiopia, significant changes were shown for girls in relation to social supports. Significant shifts were also reported in gender attitudes regarding appropriate age of marriage, birth of first child, and schooling. The DRC study found no evidence that adding a caregiver component provided a protective mechanism against sexual violence, but it did appear to increase caregiver affection towards their daughters. Study authors noted the limits to applying “best practice” parenting programs designed for high-income countries. These good quality studies suggest potential for gender norms changes among girls. High attendance by women and girls contrasts with studies involving men in gender norms programming.
Survivor response
Survivor response interventions included provision of care, support and protection to assist women who have experienced sexual violence and/or intimate partner violence, to recover and reduce further exposure to violence. Four studies [39, 43, 54, 57] reported on survivor responses, with two [39, 54] combining community mobilisation as reported above. Interventions focusing on survivor response strategies included a mixed methods study rated good quality on gender-based violence case management by refugee community workers [39], a CRCT rated as fair quality on group-based cognitive processing therapy [43]; a qualitative study rated as good on a mobile gender-based violence service [54]; and a mixed methods study rated as fair on screening for intimate partner violence and referral [57]. Cognitive therapy, case management and the mobile service were all reported to result in improvements in well-being, including mental health. Bass et al. [43] found significantly reduced PTSD, anxiety and depression symptoms for group-based cognitive processing therapy compared to individual support. Increased knowledge of gender-based violence, service availability and acceptability were reported by three studies [39, 54, 57]. Increases in women’s experiences of social support and connectedness were reported in the Lilleston et al. [54] study. Inclusion of community mobilisation [39, 54] appeared to strengthen the impact of survivor interventions. Use of peer refugee community workers- also survivors of gender-based violence, in the Hossain et al. Daadab study [39], improved community awareness of gender-based violence and increased acceptability of the case management service. Overall, the studies observed improved health and well-being for women, as well as increased knowledge of gender-based violence and availability and acceptability of services.
Information about the stage of the emergency in which interventions were delivered, was available for only two studies, respectively conducted in the “recovery” stage in Cote-D’Ivoire [41] and “acute” stage of the emergency in Lebanon [52].
Discussion
This systematic review of evidence for reduced risk and incidence of sexual violence and intimate partner violence from interventions delivered in conflict, post-conflict and other humanitarian crises identified 18 papers reporting on 16 studies, all conducted in conflict/post-conflict settings in 12 countries. Four studies identified reduced incidence of intimate partner violence [40, 46, 49, 52] and one of sexual violence and intimate partner violence [51]. Although none of these studies reached statistical significance, results indicated changes in the desired direction. These studies all evaluated gendered social norms [51], or economic empowerment interventions [46] or both combined [40, 49, 52] providing the strongest evidence of impact in this review.
Some evidence of reduced risk factors for sexual violence/intimate partner violence was identified in all studies and intervention types against our indicators. As reported in Table 4, the most common were: changed norms related to women’s equality (5 studies); increased economic autonomy for women (5 studies) and improved survivor wellbeing/ mental health (4 studies). In addition, good evidence for improved mental health outcomes was found for economic empowerment [46] and economic empowerment plus gendered social norms interventions [42]. It should be noted that each of interventions involved micro-credit strategies, and not cash transfers, which may have different outcomes and mechanisms of impact. Secondary outcomes for reduced risk included reduced PTSD and depression/ anxiety not only for survivor support [43] but also for other types of intervention, including economic empowerment alone [46] and with gender dialogue groups [42], although not in the Gibbs study [52]. Evidence is building for social norms interventions with growing sophistication in conceptualizing and measuring change in social norms. All studies aiming to change social norms had some success, though these varied across norms and between studies and was less evident for norms relating to sexual consent. An unexpected finding was that social norms interventions predominantly focussed at the individual level with few interventions identified which targeted household/ community or societal levels. It is not clear whether this is due to the work not being undertaken or a lack of studies measuring impact. Interventions involving male partners had difficulty in impacting gender norms. Multi-strategy interventions, on the whole yielded stronger results and use of social norms interventions seems well suited to combined strategies, particularly harnessing community mobilisation.
Qualitative studies, though focussing on diverse areas, suggest experiences of social connection are an important outcome for women who participate in programming around gender-based violence [47, 52, 54], which aligns with Herman’s theory that experiences of connection are key to recovery from sexual violence/intimate partner violence [58]. Further, the qualitative studies highlight that women value hearing messaging from peers in their communities [39, 45].
In relation to interventions delivered in conflict vs post-conflict settings—no trend is evident in relation to intervention or study type or outcomes. We identified no studies which met inclusion criteria, undertaken in disasters or epidemics. There was a dearth of studies evaluating community led initiatives, instead most interventions included in this review were delivered by international NGOs. This may reflect a lack of evaluation of such interventions or simply an absence in the peer reviewed literature, signalling at least, the need for local partnerships to ensure adapted or context sensitive interventions that draw further on existing local knowledge.
Over the past ten years, there has been a decrease in studies evaluating survivor responses to sexual violence in conflict and an increase in studies on primary prevention, particularly of intimate partner violence in post-conflict settings, including considerable work with men. Of the 16 studies, six targeted men as participants either exclusively [50, 51]; as a specific focus of a component of the intervention [41, 45, 49]; or as part of interventions targeting community members more broadly [44, 46].
In contrast to our earlier review [31], we found no studies where risk had appeared to increase as a result of interventions. Conversely, it is obvious that in many studies careful attention has been paid to inclusive approaches to delivering interventions in order to: attend to safety and avoid stigmatising/identifying women who have or continue to experience abuse; and to maximising transparency to communities. This contributed to under-powering of studies, a feature of multiple studies in this review—which needs to be recognised as a necessary cost to safe programming and research. Overall, it is clear that while a range of gender-based violence prevention programming is currently being implemented in conflict/post-conflict settings, evidence for the effectiveness of interventions for prevention remains limited. This aligns with two systematic reviews which explored interventions to address gender-based violence specifically in refugee settings [4, 34]. The What Works synthesis brief on evidence to prevent violence against women and girls in conflict and humanitarian crisis also found insufficient evidence to classify any intervention as “effective,” but found positive results from community-based programming focussing on social norms change, and mixed results from economic empowerment interventions [59].
The heterogeneity of interventions, contexts, study types and findings constrained the degree of synthesis possible from this review. However, some overall patterns emerge from our analysis. Firstly, it is clear that demonstrating robust reduction in sexual violence and/or intimate partner violence as a result of interventions may remain elusive in humanitarian settings. A factor in this situation may be the efforts by researchers to undertake transparent and non-stigmatising delivery of interventions and study methods, which have been rightly privileged. Secondly, improvements to mental health, social support and other positive outcomes are clear, even where reduced abuse cannot be established, particularly in relation to social norms and some economic empowerment interventions. Similar outcomes have been found from interventions in non-humanitarian crisis settings, with reduced abuse a harder goal to achieve [60, 61]. Thirdly, programmes addressing structural issues cannot only focus on women, yet have found men challenging to engage. Fourthly, most programming was relatively short term with no follow-up periods longer than two years. These attributes reflect finite resources, however changes to patterns of abuse and gendered social norms are long term outcomes which require longer time frames to accurately measure impact. Fifthly, the studies in this review show a strong emphasis on intimate partner violence or combined intimate partner violence and sexual violence, leaving an ongoing evidence gap in relation to prevention of sexual violence, which remains a challenge in all settings, not just humanitarian contexts. Sexual violence interventions in conflict settings, including non-partner sexual violence appear to have diminished as a focus of research in the past ten years, based on studies identified for this review. The diverse methodologies applied in identified studies are a strength of the field, in particular the use of RCT and CRCTs which provide robust opportunities for comparison, as well as qualitative studies which have capacity for rich insights, to foreground the lived experience of participants receiving interventions, though among studies in this review, these were not always clearly reported. Finally, compared to our earlier review there is a greater volume of interventions targeting structural/ community level change than individual level change. In part, this reflects the strong interest in social norms interventions.
Limitations
Studies that did not explicitly refer to violence/abuse, or to conflict/post-conflict/crisis in the key words, title or abstract may not have been identified. The search also excluded studies with titles, abstracts or full-texts in languages other than English. The disparate interventions allowed for limited synthesis, as did the disparate target groups and study designs. For example among studies without control groups it is not possible to establish if observed changes were due to the intervention. Limited data were available on most changes to risk, and our adopted indicators may have over-rated reductions in risk. There was a lack of findings in relation to the diversity of participants in studies, and as such an intersectional lens to results has not been applied. Lastly, this study focussed only on interventions delivered in low- and middle-income countries, reflecting the unique challenges they face during conflict and other humanitarian crises.
Conclusion
From a policy and practice perspective interventions for changing social norms on gender equality/ acceptability of violence against women, appear to hold promise, including as an adjunct to economic empowerment, although men’s programming for gendered norms needs to address participation rates. It is not yet clear how combining social norms with economic empowerment interventions can best address potential increases in economic abuse and more research is needed on this. The findings also point to the need to work locally with partners to ensure that programs are contextually adapted and privilege community-generated interventions. Methodological strengths of Future research should continue to explore how social norms change interventions can be most effectively delivered, including the impact of having mixed and/or same sex groups. Significant reductions in sexual violence/intimate partner violence incidence is unusual as an outcome from RCTs in all settings, but particularly hard to achieve in humanitarian settings which suggests a need for outcome measures that reflect these realities and recognition that null results are not indicative of no impacts. Other research implications are the need for well-executed qualitative research to understand participants’ experiences of interventions and the mechanisms of change, including from RCTs. This review indicates that significant effort has been directed towards building the evidence base for interventions addressing sexual and intimate partner violence, although with a larger focus on intimate partner violence. While there has been some progress and promising results, there is more work to do to address both sexual violence and intimate partner violence.
Availability of data and materials
The datasets used in the current study are available from the corresponding author on reasonable request.
Abbreviations
- C:
-
Conflict
- DRC:
-
Democratic Republic of Congo
- EE:
-
Economic empowerment
- GBV:
-
Gender-based violence
- IPV:
-
Intimate partner violence
- NGO:
-
Non-government organization
- PC:
-
Post-conflict
- RCT:
-
Randomized control trial
- SV:
-
Sexual violence
- WHO:
-
World Health Organization
References
Aubone A, Hernandez J. Assessing refugee camp characteristics and the occurrence of sexual violence: a preliminary analysis of the Dadaab complex. Refug Surv Q. 2013;32(4):22–40.
Krause U. A Continuum of violence? Linking sexual and gender-based violence during conflict, flight, and encampment. Refug Surv Q. 2015;34(4):1–19.
Muuo S, Muthuri SK, Mutua MK, McAlpine A, Bacchus LJ, Ogego H, et al. Barriers and facilitators to care-seeking among survivors of gender-based violence in the Dadaab refugee complex. Sex Reprod Health Matters. 2020;28(1):1–16.
Tappis H, Freeman J, Glass N, Doocy S. Effectiveness of interventions, programs and strategies for gender-based violence prevention in refugee populations: an integrative review. PLoS Curr. 2016;8:ecurrents.dis.3a465b66f9327676d61eb8120eaa5499.
Jewkes R, Sen P, Garcia-Moreno C. Sexual violence. In: Krug E, Dahlberg L, Mercy J, Zwi A, Lozano R, editors. World Report on Violence and Health. Geneva: World Health Organization; 2002. p. 147–82.
World Health Organization. Responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidelines. Geneva: World Health Organization; 2013.
Vu A, Adam A, Wirtz A, Pham K, Rubenstein L, Glass N, et al. The prevalence of sexual violence among female refugees in complex humanitarian emergencies: a systematic review and meta-analysis. PLoS Curr. 2014;6:ecurrents.dis.835f10778fd80ae031aac12d3b533ca7.
Stark L, Asghar K, Yu G, Bora C, Baysa A, Falb KL. Prevalence and associated risk factors of violence against conflict-affected female adolescents: a multi-country, cross-sectional study. J Glob Health. 2017;7(1):010416.
Cenat JM, Smith K, Morse C, Derivois D. Sexual victimization, PTSD, depression, and social support among women survivors of the 2010 earthquake in Haiti: a moderated moderation model. Psychol Med. 2019;50(15):2587–625.
Chan KL, Zhang Y. Female victimization and intimate partner violence after the May 12, 2008. Sichuan earthquake Violence and victims. 2011;26(3):364–76.
Callands TA, Sipsma HL, Betancourt TS, Hansen NB. Experiences and acceptance of intimate partner violence: associations with sexually transmitted infection symptoms and ability to negotiate sexual safety among young Liberian women. Cult Health Sex. 2013;15(6):680–94.
Gibbs A, Corboz J, Shafiq M, Marofi F, Mecagni A, Mann C, et al. An individually randomized controlled trial to determine the effectiveness of the women for Women International Programme in reducing intimate partner violence and strengthening livelihoods amongst women in Afghanistan: trial design, methods and baseline findings. BMC Public Health. 2018;18(1):164.
Hossain M, Zimmerman C, Kiss L, Kone D, Bakayoko-Topolska M, Manan D, et al. Men’s and women’s experiences of violence and traumatic events in rural Côte d ’Ivoire before, during and after a period of armed conflict. BMJ Open. 2014;4(2):e003644.
Delkhosh M, Merghati Khoei E, Ardalan A, Rahimi Foroushani A, Haravi MB. Prevalence of intimate partner violence and reproductive health outcomes among Afghan refugee women in Iran. Health Care Women Int. 2019;40(2):213–37.
Stark L, Ager A. A systematic review of prevalence studies of gender-based violence in complex emergencies. Trauma Violence Abuse. 2011;12(3):127–34.
García-Moreno C. Responding to sexual violence in conflict. The Lancet. 2014;383(9934):2023–4.
Koos C. Sexual violence in armed conflicts: research progress and remaining gaps. Third World Q. 2017;38(9):1935–51.
García-Moreno C, Jansen H, Ellsberg M, Heise L, Watts C. WHO Multi-country study on women’s health and domestic violence against women : Initial Results on prevalence, health outcomes and women’s responses. Geneva: World Health Organization; 2005.
World Health Organization, London School of Hygiene and Tropical Medicine, South African Medical Resarch Council. Global and regional estimates of violence against women: prevalence and health effects of intimate partner violence and non-partner sexual violence Geneva: World Health Organization; 2013.
Kelly JT, Betancourt TS, Mukwege D, Lipton R, VanRooyen MJ. Experiences of female survivors of sexual violence in eastern Democratic Republic of the Congo: a mixed-methods study. Confl Heal. 2011;5(25):1–8.
Glass N, Ramazani P, Tosha M, Mpanano M, Cinyabuguma M. A Congolese-US participatory action research partnership to rebuild the lives of rape survivors and their families in eastern Democratic Republic of Congo. Glob Public Health. 2012;7(2):184–95.
Amone-P’Olak KE, Ask E, Dokkedahl SB. PTSD, mental illness, and care among survivors of sexual violence in Northern Uganda: findings from the WAYS study. Psychol Trauma Theory Res Pract Policy. 2018;10(3):282–9.
Falb K, Asghar K, Pardo NM, Hategekimana JD, Kakay H, Roth D, et al. Developing an inclusive conceptual model for preventing violence in the home in humanitarian settings: qualitative findings from Myanmar and the Democratic Republic of Congo. J Interpersonal Violence. 2020:1–30.
Tol WA, Stavrou V, Greene MC, Mergenthaler C, van Ommeren M, Garcia-Moreno C. Sexual and gender-based violence in areas of armed conflict: a systematic review of mental health and psychosocial support interventions. Confl Heal. 2013;7(1):16.
Silove DM, Liddell BJ, Rees S, Chey T, Nickerson A, Tam N, et al. Effects of recurrent violence on post-traumatic stress disorder and severe distress in conflict-affected Timor-Leste: a 6-year longitudinal study. Lancet Global Health. 2014;2(5):e293–300.
Rees S, Thorpe R, Tol W, Fonseca M, Silove D. Testing a cycle of family violence model in conflict-affected, low-income countries: a qualitative study from Timor-Leste. Soc Sci Med. 2015;130:284–91.
Cardoso L, Gupta J, Shuman S, Cole H, Kpebo D, Falb K, et al. What factors contribute to intimate partner violence against women in urban, conflict-affected settings? Qualitative findings from Abidjan. Côte d’Ivoire J Urban Health. 2016;93(2):364–78.
Hynes ME, Sterk CE, Hennink M, Patel S, DePadilla L, Yount KM. Exploring gender norms, agency and intimate partner violence among displaced Colombian women: a qualitative assessment. Glob Public Health. 2016;11(1/2):17–33.
Glass N, Kohli A, Surkan P, Remy M, Perrin N. The relationship between parent mental health and intimate partner violence on adolescent behavior, stigma and school attendance in families in rural Democratic Republic of Congo. Glob Ment Health. 2018;5:e20.
Gibbs A, Corboz J, Jewkes R. Factors associated with recent intimate partner violence experience amongst currently married women in Afghanistan and health impacts of IPV: a cross sectional study. BMC Public Health. 2018;18(593).
Spangaro J, Adogu C, Ranmuthugala G, Davies GP, Steinacker L, Zwi A. What evidence exists for initiatives to reduce risk and incidence of sexual violence in armed conflict and other humanitarian crises? A systematic review. PLoS ONE. 2013;8(5):e62600.
Spangaro JA, Adogu C, Zwi AB, Geetha R, Davies GP. Mechanisms underpinning interventions to reduce sexual violence in armed conflict: a realist-informed systematic review. Conflict Health. 2015;9(1):19.
(IASC) ISC. Guidelines for Gender-based Violence Interventions in Humanitarian Settings. Focusing on Prevention of and Response to Sexual Violence in Emergencies. Inter-Agency Standing Committee; 2015.
Asgary R, Emery E, Wong M. Systematic review of prevention and management strategies for the consequences of gender-based violence in refugee settings. Int Health. 2013;5(2):85–91.
Kiss L, Quinlan-Davidson M, Pasquero L, Tejero PO, Hogg C, Theis J, et al. Male and LGBT survivors of sexual violence in conflict situations: a realist review of health interventions in low-and middle-income countries. Confl Heal. 2020;14:1–26.
Heise L. Violence against women: an integrated, ecological framework. Violence against Women. 1998;4(3):262–90.
World Health Organization. RESPECT Women: Preventing Violence Against Women. Geneva: WHO; 2019. Contract No.: (WHO/RHR/18.19).
Mays N, Pope C, Popay J. Systematically reviewing qualitative and quantitative evidence to inform management and policy-making in the health field. J Health Serv Res Policy. 2005;10(1):6–20.
Hossain M, McAlpine A, Muthuri S, Bacchus L, Muuo S, Kohli A, et al. Violence, uncertainty, and resilience among refugee women and community workers: an evaluation of gender-based violence case management services in the Dadaab refugee camps. London: Department for International Development (DFID); 2018.
Gupta J, Falb KL, Lehmann H, Kpebo D, Xuan Z, Hossain M, et al. Gender norms and economic empowerment intervention to reduce intimate partner violence against women in rural Cote d’Ivoire: a randomized controlled pilot study. BMC Int Health Hum Rights. 2013;13(1):46.
Falb KL, Annan J, King E, Hopkins J, Kpebo D, Gupta J. Gender norms, poverty and armed conflict in Côte D’Ivoire: engaging men in women’s social and economic empowerment programming. Health Educ Res. 2014;29(6):1015–27.
Annan J, Falb K, Kpebo D, Hossain M, Gupta J. Reducing PTSD symptoms through a gender norms and economic empowerment intervention to reduce intimate partner violence: a randomized controlled pilot study in Côte D’ivoire. Glob Ment Health. 2017;4:22.
Bass JK, Annan J, McIvor Murray S, Kaysen D, Griffiths S, Cetinoglu T, et al. Controlled trial of psychotherapy for Congolese survivors of sexual violence. N Engl J Med. 2013;368(23):2182–91.
Glass N, Perrin N, Marsh M, Clough A, Desgroppes A, Kaburu F, et al. Effectiveness of the Communities Care programme on change in social norms associated with gender-based violence (GBV) with residents in intervention compared with control districts in Mogadishu, Somalia. BMJ Open. 2019;9(3):e023819.
Gurman TA, Trappler RM, Acosta A, McCray PA, Cooper CM, Goodsmith L. “By seeing with our own eyes, it can remain in our mind”: qualitative evaluation findings suggest the ability of participatory video to reduce gender-based violence in conflict-affected settings. Health Educ Res. 2014;29(4):690–701.
Glass NE, Perrin NA, Kohli A, Campbell JC, Remy MM. Randomised controlled trial of a livestock productive asset transfer programme to improve economic and health outcomes and reduce intimate partner violence in a postconflict setting. BMJ Glob Health. 2017;2(1):1.
Koegler E, Kennedy C, Mrindi J, Bachunguye R, Winch P, Ramazani P, et al. Understanding how Solidarity Groups—a community-based economic and psychosocial support intervention—can affect mental health for survivors of conflict-related sexual violence in Democratic Republic of the Congo. Violence Against Women. 2019;25(3):359–74.
Bacon L. Liberia’s gender-sensitive police reform: improving representation and responsiveness in a post-conflict setting. Int Peacekeeping. 2015;22(4):372–97.
Green EP, Blattman C, Jamison J, Annan J. Women’s entrepreneurship and intimate partner violence: a cluster randomized trial of microenterprise assistance and partner participation in post-conflict Uganda. Soc Sci Med. 2015;133:177–88.
Vaillant J, Koussoube E, Roth D, Pierotti R, Hossain M, Falb KL. Engaging men to transform inequitable gender attitudes and prevent intimate partner violence: a cluster randomised controlled trial in North and South Kivu, Democratic Republic of Congo. BMJ Glob Health. 2020;5(5):e002223.
Hossain M, Zimmerman C, Kiss L, Abramsky T, Kone D, Bakayoko-Topolska M, et al. Working with men to prevent intimate partner violence in a conflict-affected setting: a pilot cluster randomized controlled trial in rural Cote d’Ivoire. BMC Public Health. 2014;14(339):339.
Gibbs A, Corboz J, Chirwa E, Mann C, Karim F, Shafiq M, Mecagni A, Maxwell-Jones C, Noble E, Jewkes R. The impacts of combined social and economic empowerment training on intimate partner violence, depression, gender norms and livelihoods among women: an individually randomised controlled trial and qualitative study in Afghanistan. BMJ Glob Health. 2020;5(3):e001946.
Nordbø E, Andersson C, Nordh H, Raanaas R, Aamodt G. Promoting activity participation and well-being among children and adolescents: a systematic review of neighborhood built-environment determinants. JBI Evid Synthesis. 2020;18(3):k370-458.
Lilleston P, Winograd L, Ahmed S, Salame D, Al Alam D, Stoebenau K, et al. Evaluation of a mobile approach to gender-based violence service delivery among Syrian refugees in Lebanon. Health Policy Plan. 2018;33(7):767–76.
Stark L, Asghar K, Seff I, Yu G, Gessesse TT, Ward L, et al. Preventing violence against refugee adolescent girls: findings from a cluster randomised controlled trial in Ethiopia. BMJ Glob Health. 2018;3(5):e000825.
Stark L, Seff I, Asghar K, Roth D, Bakamore T, MacRae M, et al. Building caregivers’ emotional, parental and social support skills to prevent violence against adolescent girls: findings from a cluster randomised controlled trial in Democratic Republic of Congo. BMJ Glob Health. 2018;3(5):e000824.
Vu A, Wirtz AL, Bundgaard S, Nair A, Luttah G, Ngugi S, et al. Feasibility and acceptability of a universal screening and referral protocol for gender-based violence with women seeking care in health clinics in Dadaab refugee camps in Kenya. Glob Ment Health. 2017;4:e21.
Herman J. Trauma and recovery: the aftermath of violence—from domestic abuse to political terror. New York Harper Collins Publishers; 1992.
Murphy M, Hess T, Casey J, Minchew H. What works to prevent violence against women and girls in conflict and humanitarian crisis: Synthesis Brief Washington D.C. and London: International Rescue Committee and Global Women’s Institute; 2019.
Hegarty K, Valpied J, Taft A, Brown S, Gold L, Gunn J, et al. Two-year follow up of a cluster randomised controlled trial for women experiencing intimate partner violence: effect of screening and family doctor-delivered counselling on quality of life, mental and physical health and abuse exposure. BMJ Open. 2020;10(12):e034295.
Ogbe E, Harmon S, Van den Bergh R, Degomme O. A systematic review of intimate partner violence interventions focused on improving social support and mental health outcomes of survivors. PLoS ONE. 2020;15(6):e0235177.
Acknowledgements
This project was fully funded by the Department of Sexual and Reproductive Health and Research of the WHO. The advice of the Department and of the expert panel convened by the WHO was central to updating the conceptual framework and refinement of the inclusion criteria.
Funding
This study was funded by the Department of Sexual and Reproductive Health and Research (SRH), World Health Organization. The Unit Head of “Addressing the needs of vulnerable populations” in SRH proposed the scope of the study and convened the expert panel. The paper is based on a report provided to the WHO/SRH and incorporates feedback provided.
Author information
Authors and Affiliations
Contributions
CGM proposed the scope of the paper and provided and facilitated expert input. JS, CTA, LK, DRG, and CMcP designed the search strategy, inclusion criteria, contributed to data analysis and drafting of the paper. CTA undertook searches. LK, DRG, CMcP and JS undertook screening DRG and CMcP undertook quality review. JS reviewed overall quality results. Paper drafting was led by CTA. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Indicators for reduced risk and incidence of sexual and intimate partner violence.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Spangaro, J., Toole-Anstey, C., MacPhail, C.L. et al. The impact of interventions to reduce risk and incidence of intimate partner violence and sexual violence in conflict and post-conflict states and other humanitarian crises in low and middle income countries: a systematic review. Confl Health 15, 86 (2021). https://doi.org/10.1186/s13031-021-00417-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13031-021-00417-x