
Abstract
Background
Laryngeal squamous cell carcinoma (LSCC) represents one of the principal tumors of the head and neck. Human papillomavirus (HPV) and Epstein–Barr virus (EBV) are considered risk factors for the development and the clinical prognosis of LSCC. High levels of p16INK4a are suggested as a surrogate marker of HPV or EBV infection in some head and neck tumors but in LSCC is still controversial. Furthermore, pRb expression may be considered an additional biomarker but it has not been clearly defined. This work aimed to compare the expression of pRb and p16INK4a as possible biomarkers in tumor tissues with and without infection by EBV or different genotypes of HPV from patients with LSCC.
Methods
Tumor samples from 103 patients with LSCC were previously investigated for the presence and genotypes of HPV using the INNO-LiPA line probe assay and for the infection of EBV by qPCR. p16 INK4a and pRb expression was assessed by immunohistochemistry.
Results
Of the 103 tumor samples, expression of p16INK4a was positive in 55 (53.4%) and of this, 32 (56.1%) were positive for HPV whereas 11 (39.3%) were EBV positive but both without a significantly difference (p > 0.05). pRb expression was positive in 78 (75.7%) and a higher frequency of this expression was observed in HPV negative samples (87.0%) (p = 0.021) and in high-risk HPV negative samples (85.2%) (p = 0.010). No difference was observed when comparing pRb expression and EBV infection status (p > 0.05).
Conclusion
Our results support the suggestion that p16INK4a is not a reliable surrogate marker for identifying HPV or EBV infection in LSCC. On the other hand, most of our samples had pRb expression, which was more frequent in tumors without HPV, suggesting that pRb could indicate HPV negativity. However, more studies with a larger number of cases are required, including controls without LSCC and evaluating other molecular markers to determine the real role of p16INK4a and pRb in LSCC.
Similar content being viewed by others


Introduction
Laryngeal squamous cell carcinoma (LSCC) is one of the most common type of head and neck cancer and, although tobacco smoking and alcohol abuse are the principal risk factors, some viral infections are implicated [1, 2]. Human papillomavirus (HPV) is a group of oncoviruses that have been widely associated with the development and clinical prognosis of LSCC tumors [3]. According to their oncogenic potential, HPV are categorized into low-risk (LR-HPV) or high-risk (HR-HPV) genotypes [4]. LR-HPV are associated with warts or skin papillomas, whereas HR-HPV are directly associated with the development of invasive carcinomas [5, 6]. Prevalence studies have reported that HPV-16 and -18 are the most common HR-HPV genotypes found in LSCC although, other HR-HPV, such as 31, 33, 35, 39, 45, 51, 52, 56, 58, and 59 are also important [7, 8]. Epstein–Barr virus (EBV) is strongly associated with onset and progression of several types of epithelial cell tumors such as nasopharyngeal carcinoma or gastric adenocarcinoma [9, 10]. The role of EBV in LSCC is controversial since difficulties have been reported in detecting its presence in this kind of cancer or it has shown a low prevalence [11]. Both HPV and EBV produce oncoproteins that have the potential to induce processes of carcinogenesis and tumor progression [12]. E7 is an oncoprotein coded by HPV that promotes retinoblastoma protein (pRb) degradation by the ubiquitin–proteasome pathway [13]. Degradation of pRb consequently induces the overexpression of the tumor suppressor protein p16INK4a, which is essential in cell cycle progression [14]. Latent membrane protein 1 (LMP1) is one of the major EBV oncoproteins that inactivates transcription factors essential for the expression of p16INK4a [15]. The alteration of p16 INK4a expression leads to hyperphosphorylation of pRb that promotes uncontrolled cellular proliferation [16]. High levels of p16INK4a expression have been suggested as a surrogate marker of HPV and EBV infection in pharyngeal, nasopharyngeal, and oropharynx tumors, whereas in laryngeal tumors are still controversial; therefore, pRb expression may be considered as an additional biomarker, particularly in tumors with infection by HPV and EBV [12, 17,18,19]. This work is aimed to compare the expression of pRb and p16INK4a as possible biomarkers in tumor tissues with and without infection by EBV or different genotypes of HPV from patients with LSCC attending a third-level care referral hospital.
Materials and methods
Samples
Formalin-fixed and paraffin-embedded (FFPE) tissue specimens from patients with LSCC were included in a retrospective study. Samples were taken from a previous study evaluating the HPV and EBV prevalence in patients with LSCC [20]. All patients had undergone surgical resection of the laryngeal tumor between 2012 and 2015 at the Unidad Medica de Alta Especialidad (UMAE) No. 25, a tertiary referral hospital of the Instituto Mexicano del Seguro Social (IMSS) located in northeastern Mexico. The information obtained from clinical records included age, sex, history of alcohol and tobacco consumption, and laryngeal subsite location of the tumor (subglottic, glottic, or supraglottic). Histological and pathological grading of tumors was made using the Broder’s classification [21]. The National Committee of Scientific Research of the IMSS granted ethical approval to carry out the study (R-2014-785-055). Individual informed consent was not obtained as specimens were retrospectively collected.
HPV genotyping and EBV detection
Tumor sections from each FFPE sample were carefully punched off and conducted to a DNA isolation using the NucleoSpin DNA FFPE (Macherey–Nagel, Düren, Germany). The presence and genotype of HPV were evaluated using the INNO-LiPA HPV Genotyping Kit Extra II Amp (Innogenetics, Gent, Belgium), a line probe assay designed for the identification of 32 genotypes of the HPV, including thirteen HR-HPV (HPV-16, HPV-18, HPV-31, HPV-33, HPV-35, HPV-39, HPV-45, HPV-51, HPV-52, HPV-56, HPV-58, HPV-59, and HPV-68), six possible HR-HPV (HPV-26, HPV-53, HPV-66, HPV-70, HPV-73, and HPV-82), nine LR-HPV (HPV-6, HPV-11, HPV-40, HPV-42, HPV-43, HPV-44, HPV-54, HPV-61, and HPV-81), and other four not yet classified HPV genotypes (HPV-62, HPV-67, HPV-83, and HPV-89) [22]. To detect DNA of EBV, a 69 bp fragment flanking the 679–748 position of the viral LMP2 glycoprotein was amplified using the primers 5′-AGC TGT AAC TGT GGT TTC CAT GAC-3′ and 5′-GCC CCC TGG CGA AGA G-3′ with the probe 6FAM5′-CTG CTG CTA CTG GCT TTC GTC CTC TGG-3′TAMRA. All the reactions for EBV detection were performed after the HPV genotyping assays using the TaqMan Universal PCR MasterMix (Applied Biosystems, Foster City CA, USA) in the Light Cycler (Roche). Synthetic DNA fragment (gBlocks Gene Fragment, IDT) containing the 69 bp sequence of the amplicon of EBV was used as amplification control and to evaluate the efficiency and detection limits of the assay.
p16INK4a and pRb expression
Immunohistochemical (IHC) staining method for p16INK4a and pRb was performed on 5-µm-thick FFPE tissue cross-sections using the mouse and rabbit specific HRP/DAB (ABC) detection IHC kit (Abcam, Cambridge, UK) with the monoclonal anti-CDKN2A/p16INK4a antibody (clone EPR1473, ab108349, dilution 1:100; Abcam, Cambridge, UK) and the monoclonal anti-Rb antibody (clone EPR17512, ab181616, dilution 1:250; Abcam, Cambridge, UK). Hematoxylin–eosin (HE) stains were also prepared for histological evaluation of tumors. Two independent pathologists who were blinded to the clinical information and to the HPV or EBV status of the samples evaluated all the IHC and HE stains. Evaluations were made based on staining intensity as other previous reports have done. Specimens were considered positive for p16INK4a expression if they showed ≥ 75% of stained cells, whereas for pRb, ≥ 25% of stained cells were interpreted as a positive expression [23,24,25,26].
Statistical analysis
We used the Mann–Whitney U test, Pearson's X2 test, and Fisher's exact test. A p value < 0.05 was considered statistically significant. All analyzes were performed using the IBM SPSS Statistics program (Version 20, SPSS. Inc., Chicago, USA).
Results
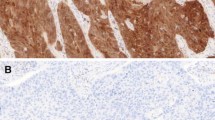
One hundred and three FFPE specimens from the previously published study with sufficient tumor tissue for IHC were eligible for the present work. The age range of the included patients was 40 to 89 years, with a median of 64, and most were 60 years or older (73.8%). Most samples were from men (96.1%), and tobacco smoking was common (98.0%). In contrast, alcohol intake frequency was low (6.8%). The glottis subsite was the most frequent location of tumors (49.5%). We had 57 (55.3%) tumor samples positive for HPV DNA, and 42 (40.8%) of these had at least one HR-HPV genotype. EBV DNA was present in 28 (27.2%) samples. Of these, 16 (15.5%) were in co-infection with HPV, 11 (10.7%) corresponded to co-infections with at least one HR-HPV, and 12 (11.7%) cases had only EBV infection (Table 1). Clinical characteristics of patients with LSCC tumor samples positive for at least one HR-HPV are summarized in Table 2. HPV-52 was the most frequently HR-HPV genotype, with 34 cases corresponding to 59.6% of all the HPV-positive samples. Immunohistochemistry were assessed considering a positive expression of p16INK4a if ≥ 75% of tumor cells were stained and for pRb if ≥ 25% of stained cells were observed (Fig. 1).

Representative examples of immunohistochemical (IHC) staining of tumors from patients with laryngeal squamous cell carcinoma. a Sample of patient No. 175 without infection of HPV or EBV; b sample of patient No. 046 that was positive for the 11 and 16 HR-HPV and negative for EBV; and c sample of patient No. 021 that was negative HPV and positive for EBV (× 40 microscopic magnification)
Of the 103 tumor samples, p16INK4a expression was positive in 55 (53.4%). According to the surgical source of the sample, biopsies (64.5%) had a higher frequency of expression of this protein than laryngectomies (p = 0.009 by the Pearson's chi-squared test). Samples cataloged as Grade III by Broder's classification showed a higher frequency of p16INK4a expression (80.9%) compared with those of grade I (50.0%) and II (42.1%) (p < 0.05 by the Mann–Whitney U test). Only one of the seven alcohol consumers showed p16INK4a expression (14.3%) (p = 0.048 by the Fisher's Exact Test). No significant difference was observed when comparing p16INK4a expression with the presence of HPV or EBV (p > 0.05 by the Fisher's Exact Test). Regarding pRb expression, 78 (75.7%) samples were positive. Specimen’s obtained from biopsies (84.2%) showed a higher frequency of pRb expression than laryngectomy samples (p = 0.025 by the Pearson's chi-squared test). The frequency of pRb expression was higher in HPV negative samples (87.0%) (p = 0.021 by the Fisher's Exact Test). A higher frequency of pRb expression was also observed in the group of HR-HPV negative samples (85.2%) (p = 0.010 by the Fisher's Exact Test). No significant differences (p > 0.05) were observed in the expression of p16INK4a or pRb by age and sex of patients, laryngeal tumor subsite, and tobacco consumption habits of the patients (Table 1).
Discussion
To assess the expression of p16 INK4a and pRb in LSCC specimens with and without infection by EBV or different genotypes of HPV, 103 FFPE samples retrospectively collected from patients were evaluated by IHC analysis. The epidemiological characteristics of the studied sample are consistent with those previously described for this disease [11, 19, 27,28,29,30,31,32,33]. p16INK4a status has been well characterized in HPV-positive head and neck tumors such oropharyngeal carcinoma and has been suggested as a surrogate marker for infection of HPV and progression, but this has not been definitively established for LSCC [34, 35]. In this study, 55 (53.4%) of 103 patients were positive for p16INK4a. Tong et al. found that 115 (54%) of 211 LSCC specimens were positive for p16INK4a [36]. Elhadj et al. show that the expression positive of p16INK4a was found in 36 (51.43%) of 70 LSCC cases [37]. Expression of p16INK4a might be affected by genetic or epigenetic mechanisms [38]. Some studies suggest hypermethylation may represent an early event in carcinogenesis of different neoplasms, such as endometrial cancer [39]. In LSCC, expression level of p16INK4a is significantly reduced and hypermethylation has been shown to be a common mechanism causing this downregulation [40]. We found that 80.9% of our specimens classified as grade III presented a higher p16INK4a expression. In contrast to our results, Tong and et al. found that p16INK4a expression was observed more commonly in well-differentiated samples [36]. In our study, only 7 (6.8%) patients were alcohol consumers, and one of them expressed p16INK4a. Although this low number of cases precludes reliable statistical comparison, most alcohol consumers were significantly negative for p16INK4a expression (p = 0.048). Elhadj et al. found no association between alcohol consumption and p16INK4a expression when evaluating 30 alcohol-consuming patients [37]. Otherwise, we found that 32 (56.1%) of the fifty-five positive samples for p16 INK4a were also positive for HPV infection. Stephen et al. reported the expression of p16INK4a in 21 (26.0%) of 80 patients, furthermore, 12 (57.0%) of these were positive for HPV infection [34]. Hernandez et al. observed p16INK4a expression in 8 (7.9%) of 101 cases, and only 2 (25.0%) of these were also HPV DNA positive [41]. Sanchez et al. found that 48 (39.0%) of 123 samples were positive for p16INK4a expression, and 14 (29.2%) of these were positive for HPV infection [42]. Dogantemur et al. observed p16INK4a expression in 18 (20.0%) of 90 cases and only 6 (33.3%) of these were also positive for DNA of HPV [43]. The fact that no association between the expression of p16INK4a and HPV infection was observed could support the suggestion that this protein may not be reliable as a surrogate marker for HPV infection [44].
Modifications of the p16INK4a and pRb expression have been delineated in several types of human cancers [45, 46]. We found that pRb expression was present in 78 (75.7%) of 103 specimens. Morshed et al. found that 90 (69%) of 130 patients with LSCC had expression of pRb [47]. Krecicki et al. reported that 51(88%) of 58 samples were positive for pRb expression [48]. Some studies suggest that high pRb expression may be due to different factors. Soares et al. suggested that it can be due to an increase in the proportions of proliferating cells, which is supported by the fact that the hyperphosphorylated pRb inactive form increases during the G2/M phases [49]. IHC evaluation using antibodies against phosphorylated and non-phosphorylated pRb forms could solve this. As pRb is a negative regulator of p16INK4a, its inactivation results in overexpression of p16INK4a. Thus, a positive test for HPV combined with p16INK4a expression has been described as evidence of biologically relevant infection [50, 51]. The frequency of pRb expression was significantly higher in the HPV-negative specimens; we found 40 (87.0%) with positive pRb expression in 46 HPV-negative tumors. However, the clinical and prognostic significance remains poorly described in LSCC. Soares et al. found a significant difference between pRb expression and HPV-positive (9/11, 81.8%) and HPV-negative (15/22, 68.2%) oral squamous cell carcinoma (OSCC) samples [49]. Shaikh et al. demonstrated that pRb expression was predominant in 51 (77.3%) of 66 HPV-negative head and neck cancers cases, but they did not find significant differences [51]. We also observed a significantly higher frequency of pRb expression in HR-HPV negative specimens. The pRb expression was present in 51 (85.2%) of 61 HR-HPV negative samples. By contrast, Nemes et al. reported no statistical difference in 37 (84%) of 44 HR-HPV negative OSCC samples with pRb expression [52]. Various studies have shown that HPV-positive cancers generally exhibit decreased expression of pRb [53]. In addition, the oncoprotein E7 of HPV is known to participate in the degradation of pRb through a ubiquitin–proteasome and other pathways [54]. Thus, the absence of HPV infection could be related to the pRb expression in our samples.
Conclusion
We detected p16INK4a in half of LSCC cases, and in half of these, HPV was also detected. However, the proportion of samples with p16INK4a expression was similar between those with HPV and EBV. Although the proportion of LSCC samples with p16INK4a expression was higher than reported in several previous studies, our findings suggest little value of this marker as a reliable surrogate for identifying HPV in laryngeal cancer. On the other hand, as in previous studies, most of our LSCC samples had pRb expression, this being more frequent in tumors without the presence of HPV, even in those positive for high-risk HPV. Therefore, pRb expression seems to indicate HPV negativity, which could justify not performing other molecular tests for HPV detection in this type of cases, as previously suggested. However, further studies with a larger number of cases, including controls without laryngeal cancer, involving other tumor suppression pathways or other molecular markers, are necessary to determine the real role of p16INK4a and pRb in LSCC.
Availability of data and materials
The raw data analyzed during the current study are provided in a Supplemental File.
References
Onerci Celebi O, Sener E, Hosal S, Cengiz M, Gullu I, Guler TG. Human papillomavirus infection in patients with laryngeal carcinoma. BMC Cancer. 2018;18(1):1–5.
Morshed K. Association between human papillomavirus infection and laryngeal squamous cell carcinoma. J Med Virol. 2010;82(6):1017–23.
Gama RR, Carvalho AL, Filho AL, Scorsato AP, López RVM, Rautava J, et al. Detection of human papillomavirus in laryngeal squamous cell carcinoma: systematic review and meta-analysis. Laryngoscope. 2016;126(4):885–93.
Tan LSY, Fredrik P, Ker L, Yu FG, Wang DY, Goh BC, et al. High-risk HPV genotypes and P16INK4a expression in a cohort of head and neck squamous cell carcinoma patients in Singapore. Oncotarget. 2016;7(52):86730–9.
Chen WC, Chuang HC, Lin YT, Huang CC, Chien CY. Clinical impact of human papillomavirus in laryngeal squamous cell carcinoma: a retrospective study. PeerJ. 2017;2017(5):1–13.
Chow LT, Broker TR. Human papillomavirus infections: Warts or cancer? Cold Spring Harb Perspect Biol. 2013;5(7):1–17.
Duray A, Descamps G, Arafa M, Decaestecker C, Remmelink M, Sirtaine N, et al. High incidence of high-risk HPV in benign and malignant lesions of the larynx. Int J Oncol. 2011;39(1):51–9.
Erkul E, Yilmaz I, Narli G, Babayigit MA, Gungor A, Demirel D. The presence and prognostic significance of human papillomavirus in squamous cell carcinoma of the larynx. Eur Arch Oto-Rhino-Laryngol. 2017;274(7):2921–6.
Ayee R, Ofori MEO, Wright E, Quaye O. Epstein Barr virus associated lymphomas and epithelia cancers in humans. J Cancer. 2020;11(7):1737–50.
Tsao SW, Tsang CM, Lo KW. Epstein–Barr virus infection and nasopharyngeal carcinoma. Philos Trans R Soc B Biol Sci. 2017;372(1732):20160270.
Yang D, Shi Y, Tang Y, Yin H, Guo Y, Wen S, et al. Effect of HPV infection on the occurrence and development of laryngeal cancer: a review. J Cancer. 2019;10(19):4455–62.
Dreyer JH, Hauck F, Barros MHM, Niedobitek G. PRb and cyclind1 complement p16 as immunohistochemical surrogate markers of hpv infection in head and neck cancer. Appl Immunohistochem Mol Morphol. 2017;25(5):366–73.
Vats A, Trejo-Cerro O, Massimi P, Banks L. Regulation of HPV E7 stability by E6-associated protein (E6AP). J Virol. 2022;96(16):e0066322.
Giarrè M, Caldeira S, Malanchi I, Ciccolini F, Leão MJ, Tommasino M. Induction of pRb degradation by the human papillomavirus type 16 E7 protein is essential to efficiently overcome p16INK4a-imposed G1 cell cycle arrest. J Virol. 2001;75(10):4705–12.
Ohtani N, Brennan P, Gaubatz S, et al. Epstein–Barr virus LMP1 blocks p16INK4a-RB pathway by promoting nuclear export of E2F4/5. J Cell Biol. 2003;162(2):173–83.
D’Arcangelo D, Tinaburri L, Dellambra E. The role of p16INK4a pathway in human epidermal stem cell self-renewal, aging and cancer. Int J Mol Sci. 2017;18(7):1591.
Betiol JC, Sichero L, Costa HODO, De Matos LL, Andreoli MA, Ferreira S, et al. Prevalence of human papillomavirus types and variants and p16INK4a expression in head and neck squamous cells carcinomas in São Paulo, Brazil. Infect Agent Cancer. 2016;11(1):1–7.
El-Naggar A, Westra W. p16 expression as a surrogate marker for HPV-related oropharyngeal carcinoma: a guide for interpretative relevance and consistency. Head Neck. 2011;34:459–61.
Jiang W, Chamberlain PD, Garden AS, Kim BYS, Ma D, Lo EJ, et al. Prognostic value of p16 expression in Epstein Bar Virus positive nasopharyngeal carcinomas. Head Neck. 2018;38(Suppl 1):1–17.
Vazquez-Guillen JM, Palacios-Saucedo GC, Rivera-Morales LG, Alonzo-Morado MV, Burciaga-Bernal SB, Montufar-Martinez M, et al. Infection and coinfection by human papillomavirus, Epstein–Barr virus and Merkel cell polyomavirus in patients with squamous cell carcinoma of the larynx: a retrospective study. PeerJ. 2018;6(10):e5834.
Zain R, Sakamoto F, Shrestha P, Mori M. Proliferating cell nuclear antigen (PCNA) expression in oral squamous cell carcinomas. Malays J Pathol. 1995;17(1):23–30.
Xu L, Padalko E, Oštrbenk A, Poljak M, Arbyn M. Clinical evaluation of INNO-LiPA HPV genotyping EXTRA II assay using the VALGENT framework. Int J Mol Sci. 2018;19:2704.
Kiyuna A, Ikegami T, Uehara T, Hirakawa H, Agena S, Uezato J, et al. High-risk type human papillomavirus infection and p16 expression in laryngeal cancer. Infect Agent Cancer. 2019;14(1):1–9.
Mulder FJ, Klufah F, Janssen FME, et al. Presence of human papillomavirus and Epstein–Barr virus, but absence of merkel cell polyomavirus, in head and neck cancer of non-smokers and non-drinkers. Front Oncol. 2021;10:560434.
López López JC, Fernández Alonso N, Cuevas Álvarez J, García-Caballero T, Pastor Jimeno JC. Immunohistochemical assay for neuron-specific enolase, synaptophysin, and RB-associated protein as a diagnostic aid in advanced retinoblastomas. Clin Ophthalmol. 2018;12:1171–9.
Halec G, Holzinger D, Schmitt M, et al. Biological evidence for a causal role of HPV16 in a small fraction of laryngeal squamous cell carcinoma. Br J Cancer. 2013;109(1):172–83.
Herrera-gómez Á, Villavicencio-valencia V, Rascón-ortiz M, Luna-ortiz K. Demografía del cáncer laríngeo en el Instituto Nacional de Cancerología. Cir Ciruj. 2009;77(5):353–7.
Koirala K. Epidemiological study of laryngeal carcinoma in Western Nepal. Asian Pac J Cancer Prev. 2015;16(15):6541–4.
Huerta AA, Rojo SA, Antonio J, Machado L. Frecuencia, aspectos clínicos y factores asociados al cáncer de laringe. Acta Otorrinolaringol Cirugía Cabeza y Cuello. 2017;45(4):240–6.
Orellana G MJ, Chuang Ch Á, Fulle C A, Fernández G R, Loyola B F, Imarai B C. Cáncer de laringe: Serie de casos en 6 años en el Complejo Asistencial Doctor Sótero del Río. Rev Otorrinolaringol Cir Cabeza Cuello. 2017;77(1):35–43.
Marioni G, Marchese-Ragona R, Cartei G, Marchese F, Staffieri A. Current opinion in diagnosis and treatment of laryngeal carcinoma. Cancer Treat Rev. 2006;32(7):504–15.
Gallegos-Hernandez JF, Paredes-Hernandez E, Flores-Diaz R, Minauro-Muñoz G, Apresa-Garcia T, Hernández-Hernandez DM. Virus del papiloma humano asociado con cáncer de cabeza y cuello. Cir Cir. 2007;75(3):151–5.
Rocha A, Bologna R, Rocha C. Virus del papiloma humano y el cáncer de cabeza y cuello: revisión de la literatura desde México y Colombia. Univ Odontol. 2012;31(67):149–57.
Stephen JK, Divine G, Chen KM, Chitale D, Havard S, Worsham MJ. Significance of p16 in site-specific HPV positive and HPV negative head and neck squamous cell carcinoma. Cancer Clin Oncol. 2013;2(1):51–61.
Young RJ, Urban D, Angel C, Corry J, Lyons B, Vallance N, et al. Frequency and prognostic significance of p16 INK4A protein overexpression and transcriptionally active human papillomavirus infection in laryngeal squamous cell carcinoma. Br J Cancer. 2015;112(6):1098–104.
Tong F, Geng J, Yan B, Lou H, Chen X, Duan C, et al. Prevalence and prognostic significance of HPV in laryngeal squamous cell carcinoma in Northeast China. Cell Physiol Biochem. 2018;49(1):206–16.
Ben Elhadj M, Amine OEL, Mokni Baizig N, Ben Ayoub W, Goucha A, El May MV, et al. Expression profile of survivin and p16 in laryngeal squamous cell carcinoma: contribution of Tunisian patients. Ear Nose Throat J. 2021;100(1):7–15.
Lazăr CS, Şovrea AS, Georgiu C, Crişan D, Mirescu ŞC, Cosgarea M. Different patterns of p16INK4a immunohistochemical expression and their biological implications in laryngeal squamous cell carcinoma. Rom J Morphol Embryol. 2020;61(3):697–706.
Guida M, Sanguedolce F, Bufo P, et al. Aberrant DNA hypermethylation of hMLH-1 and CDKN2A/p16 genes in benign, premalignant and malignant endometrial lesions. Eur J Gynaecol Oncol. 2009;30(3):267–70.
Wong TS, Gao W, Li ZH, Chan JY, Ho WK. Epigenetic dysregulation in laryngeal squamous cell carcinoma. J Oncol. 2012;2012:739461.
Hernandez BY, Rahman M, Lynch CF, Cozen W, Unger ER, Steinau M, et al. p16(INK4A) expression in invasive laryngeal cancer. Papillomavirus Res. 2016;2:52–5.
Sánchez Barrueco A, González Galán F, Villacampa Aubá JM, Díaz Tapia G, Fernández Hernández S, Martín-Arriscado Arroba C, et al. p16 influence on laryngeal squamous cell carcinoma relapse and survival. Otolaryngol Head Neck Surg. 2019;160(6):1042–7.
Dogantemur S, Ozdemir S, Uguz A, Surmelioglu O, Dagkiran M, Tarkan O, et al. Assessment of HPV 16, HPV 18, p16 expression in advanced stage laryngeal cancer patients and prognostic significance: assessment of HPV 16, HPV 18, p16 expression in laryngeal cancer. Braz J Otorhinolaryngol. 2020;86(3):351–7.
Schindele A, Holm A, Nylander K, Allard A, Olofsson K. Mapping human papillomavirus, Epstein–Barr virus, cytomegalovirus, adenovirus, and p16 in laryngeal cancer. Discov Oncol. 2022;13(1):18.
Li J, Poi MJ, Tsai M-D. The regulatory mechanisms of tumor supressor p16INK4 and relevance to cancer. Biochemistry. 2011;50(25):5566–82.
Lu DW, El-Mofty SK, Wang HL. Expression of p16, Rb, and p53 proteins in squamous cell carcinomas of the anorectal region harboring human papillomavirus DNA. Mod Pathol. 2003;16(7):692–9.
Morshed K, Korobowicz E, Skomra D, et al. Immunohistochemical study of retinoblastoma protein expression in laryngeal squamous cell carcinoma according to low and high overexpression. Bull Vet Inst Pulawy. 2008;52:675–81.
Krecicki T, Smigiel R, Fraczek M, Kowalczyk M, Sasiadek MM. Studies of the cell cycle regulatory proteins P16, cyclin D1 and retinoblastoma protein in laryngeal carcinoma tissue. J Laryngol Otol. 2004;118(9):676–80.
Soares RC, Oliveira MC, De Souza LB, Costa ADLL, Pinto LP. Detection of HPV DNA and immunohistochemical expression of cell cycle proteins in oral carcinoma in a population of Brazilian patients. J Appl Oral Sci. 2008;16(5):340–4.
Langendijk JA, Psyrri A. The prognostic significance of p16 overexpression in oropharyngeal squamous cell carcinoma: implications for treatment strategies and future clinical studies. Ann Oncol. 2010;21(10):1931–4.
Shaikh MH, Khan AI, Sadat A, Chowdhury AH, Jinnah SA, Gopalan V, et al. Prevalence and types of high-risk human papillomaviruses in head and neck cancers from Bangladesh. BMC Cancer. 2017;17(1):1–11.
Nemes JA, Deli L, Nemes Z, Márton IJ. Expression of p16INK4A, p53, and Rb proteins are independent from the presence of human papillomavirus genes in oral squamous cell carcinoma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102(3):344–52.
Wiest T, Schwarz E, Enders C, Flechtenmacher C, Bosch FX. Involvement of intact HPV16 E6/E7 gene expression in head and neck cancers with unaltered p53 status and perturbed pRb cell cycle control. Oncogene. 2002;21(10):1510–7.
Fiedler M, Müller-Holzner E, Viertler HP, et al. High level HPV-16 E7 oncoprotein expression correlates with reduced pRb-levels in cervical biopsies. FASEB J. 2004;18(10):1120–2.
Acknowledgements
We thank to the Laboratorio de Inmunologia y Virologia from Facultad de Ciencias Biologicas of the Universidad Autonoma de Nuevo Leon for providing all the facilities for the research.
Funding
This work was supported by the Support Program for Scientific and Technological Research of the UANL (Programa de Apoyo a la Investigacion Cientifica y Tecnologica; PAICYT-UANL). Dr. Gerardo C. Palacios-Saucedo was supported by a Research Excellence Scholarship from the IMSS Foundation (Beca de Excelencia en Investigación de la Fundación IMSS A.C.). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
JMVG and GCPS conceived and designed the experiments, performed the experiments, analyzed the data, contributed reagents/materials/analysis tools, prepared figures and/or tables, authored or reviewed drafts of the paper, approved the final draft. AYAV and AHE performed the experiments, prepared figures and/or tables, authored or reviewed drafts of the paper. AZP, LGRM, ACMT, VGV analyzed the data, contributed reagents/materials/analysis tools, prepared figures and/or tables, authored or reviewed drafts of the paper, approved the final draft. JCSH, SJHM, EECM, MSMB, CAAT and ECSF participated in the collection and histological reevaluation of the specimens, performed the histopathological evaluations, and analyzed the clinical data. RSTG and CRP contributed to the financing, analyzed the final data, reviewed and approved the final draft of the paper. All authors reviewed the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The following information was supplied relating to ethical approvals (i.e., approving body and any reference numbers): The National Committee of Investigation of the Instituto Mexicano del Seguro Social granted Ethical approval to carry out the study (Reg. No. R-2014-785-055).
Consent for publication
Not applicable.
Competing interests
The authors declare there are no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Vazquez-Guillen, J.M., Palacios-Saucedo, G.C., Alanis-Valdez, A.Y. et al. p16INK4a and pRb expression in laryngeal squamous cell carcinoma with and without infection by EBV or different genotypes of HPV: a retrospective study. Infect Agents Cancer 18, 43 (2023). https://doi.org/10.1186/s13027-023-00514-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13027-023-00514-x