
Abstract
Background
Patients with amyotrophic lateral sclerosis (ALS) demonstrate great heterogeneity in the age at onset (AAO), which is closely related to the course of disease. However, most genetic studies focused on the risk of ALS, while the genetic background underlying AAO of ALS is still unknown.
Methods
To identify genetic determinants influencing AAO of ALS, we performed genome-wide association analysis using a Cox proportional hazards model in 2,841 patients with ALS (Ndiscovery = 2,272, Nreplication = 569) in the Chinese population. We further conducted colocalization analysis using public cis-eQTL dataset, and Mendelian randomization analysis to identify risk factors for AAO of ALS. Finally, functional experiments including dual-luciferase reporter assay and RT-qPCR were performed to explore the regulatory effect of the target variant.
Results
The total heritability of AAO of ALS was ~ 0.24. One novel locus rs10128627 (FRMD8) was significantly associated with earlier AAO by ~ 3.15 years (P = 1.54E-08, beta = 0.31, SE = 0.05). This locus was cis-eQTL of NEAT1 in multiple brain tissues and blood. Colocalization analysis detected association signals at this locus between AAO of ALS and expression of NEAT1. Furthermore, functional exploration supported the variant rs10128627 was associated with upregulated expression of NEAT1 in cell models and patients with ALS. Causal inference suggested higher total cholesterol, low-density lipoprotein, and eosinophil were nominally associated with earlier AAO of ALS, while monocyte might delay the AAO.
Conclusions
Collective evidence from genetic, bioinformatic, and functional results suggested NEAT1 as a key player in the disease progression of ALS. These findings improve the current understanding of the genetic role in AAO of ALS, and provide a novel target for further research on the pathogenesis and therapeutic options to delay the disease onset.
Similar content being viewed by others

Background
Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative disorder characterized by upper and lower motor neuron loss which ultimately leads to respiratory failure [1]. Though the peak age at onset (AAO) of ALS is 45–49 years for women and 55–59 years for men [2], individuals of any age could be affected. The AAO of ALS is a key phenotypic feature associated with variation in the motor and cognitive phenotypes [3], disease progression, prognosis, and survival [4, 5]. Identification of risk factors influencing AAO of ALS could help better understand the disease etiology and provide clinical guidance for patients and clinicians. However, the mechanisms underlying the heterogeneity in AAO of ALS are complex and still poorly understood.
Epidemiological studies have suggested several clinical factors like sex, family history, and physical activity might influence the AAO of ALS [3, 6]. However, these factors explain only a modest proportion of the variance in AAO of ALS. In recent years, along with the burgeoning genetic research on ALS, growing evidence demonstrated the essential role of genetic background in the AAO of ALS. For example, whole exome sequencing analysis in 89 families with familial ALS and 410 patients with sporadic ALS suggested that multiple rare variants in ALS causative genes like SOD1 could lead to earlier AAO [7]. Meanwhile, a previous genome-wide association study (GWAS) in the European population identified suggestive association between several genomic regions and AAO of ALS [8]. Identifying genetic modifiers for AAO of ALS could help provide additional insights into the disease mechanisms and find out therapeutic options that may postpone the disease onset. However, most genetic studies mainly focused on the risk of ALS, while the genetic risk factors affecting AAO of ALS are mostly unknown, especially in the Asian population.
In this context, we carried out a GWAS in a large ALS cohort to explore genetic modifiers for AAO of ALS. We identified a novel locus rs10128627 (FRMD8) which was significantly associated with earlier AAO of ALS.
Methods
Participants
The participants comprised 2,841 unrelated Chinese patients with ALS recruited from the Department of Neurology of West China Hospital of Sichuan University (Ndiscovery = 2,272, Nreplication = 569). The patients were diagnosed by neurologists specializing in ALS according to the El Escorial revised criteria [9]. AAO was defined as the age when the patient presented with upper or lower motor neuron signs. West China Hospital approved the study, and all participants have signed informed consent.
Genotyping
Genomic DNA was extracted from peripheral blood leukocytes and then genotyped on the Illumina Infinium Asian Screening Array-MD v1.0 for a total of ~ 0.66 million single nucleotide polymorphisms (SNP) [10]. Imputation was performed in Michigan Imputation Server with the reference panel Genome Asia Pilot [11]. Imputed SNPs with r2 < 0.8 and genotype calls with genotype quality < 0.8 were removed.
Quality control
Individuals with mismatched sex or a call rate of less than 95% were removed. Related individuals assessed by IBD analysis using Plink were removed. SNPs with missingness > 0.05 or out of Hardy-Weinberg Equilibrium (P < 1E-06) or with minor allele frequency (MAF) < 0.01 were excluded. To remove potential outliers affecting the regression model, patients with AAO < 20 years or AAO > 89 years (around ± 3 standard deviations from the mean) were excluded. Ancestry outliers identified by the principal component analysis (PCA) based on the 1000 Genomes Project haplotypes were removed.
Genome-wide survival analysis
We first performed genome-wide survival analysis using a Cox proportional hazards model for AAO of ALS in the discovery cohort, adjusting for sex and the first three principal components. Then we applied the same model in the replication cohort, and combined the results from both stages into a meta-analysis using Plink under a fixed-effect model. Log-rank test was used to assess the difference of AAO between categories. The significant level was set as P = 5E-08 at genome-wide, and P = 1E-06 was set as the suggestive significance level.
We next conducted gene-based association analysis using MAGMA (Multi-marker Analysis of GenoMic Annotation) with default parameters to integrate association signals from the variant level into the gene level [12]. The subjects from the East Asian population in the 1000 Genomes Project (Phase 3) were used for the linkage disequilibrium (LD) reference. P value was adjusted by Bonferroni correction according to the number of tested genes.
Polygenic risk score (PRS) has been utilized in estimating the genetic risk of developing specific diseases. In the current study, we evaluated the correlation between AAO and PRS of ALS risk using a Cox proportional hazards model. When calculating PRS of risk with PRSice [13], risk allele dosages scaled by beta coefficients were summed across genome-wide SNPs from the largest GWAS on ALS risk so far [14]. Considering the genetic heterogeneity across ethnicities, we further calculated PRS using summary statistics from a meta-analysis involving two earlier GWAS on risk of ALS in the Asian population [15, 16]. Meta-analysis was performed using Plink with a random-effect model. PRS was converted to Z scores to make the scale of analyses more easily interpretable. To further test the association between ALS of AAO and each risk variant of ALS, we performed survival analysis using a Cox proportional hazards model and linear regression among the targeted risk SNPs of ALS [14]. Statistical analyses were performed in R v3.5.3.
Furthermore, to explore the potential utility of PRS of AAO in clinical trials, we calculated PRS of AAO based on the results from the current GWAS to predict early-onset ALS (AAO < 45 years). Predictability was estimated with receiver operating characteristic (ROC) curves. Considering that overfitting might happen when testing the predictive performance in the same cohort for which the model was trained and thus might bias the results, we tested the performance of the model in samples from the replication stage using summary statistics of AAO of ALS derived from the discovery stage.
Functional interpretation of significant variants
Since most loci identified by GWAS are thought to regulate gene expression, we screened the significant SNPs from our GWAS for cis-eQTL signals in GTEx [17] and QTLbase [18]. Then we searched GeneHancer for gene enhancers [19], which includes known enhancers and their potential gene targets assessed by functional studies. Furthermore, we evaluated the probability of colocalization between influence on AAO of ALS and regulation of gene expression with colocalization analysis using the coloc package [20]. Cis-eQTL dataset for brain and whole blood from GTEx was utilized [21]. Loci with a posterior probability of hypothesis 4 (PP4) of 0.75 or more were considered colocalized due to a single shared causal variant.
Dual-luciferase reporter assay
The pGL3-promoter vector was from Promega, and we modified the vector by replacing the original SV40 promoter in the vector with the promoter of NEAT1 (Additional file 3). About 1000 bp including the lead SNP with reference allele (wildtype) or risk allele (variant) were cloned into the pGL3-promoter vector, which contained the NEAT1 promoter upstream of the firefly luciferase reporter gene. Hela cells were cultured as described previously [22], and plated in 24-well plates and cotransfected with 0.5 µg of pGL3-promoter-WT or pGL3-promoter-MT and 0.4 µg of pRL-TK vector (Promega) as an internal control by using jetPRIME® transfection reagent (Polyplus-Transfection, France). Moreover, the pGL3-basic vector and pGL3-NEAT1-promoter vector were transferred as a systemic control. Luciferase activity was measured 48 h after transfection and the assay was conducted according to the standard protocol of the Promega Dual-Luciferase Reporter Assay System. A minimum of three independent experiments were performed, each including three technical replicates.
All quantitative results of cell assays were presented as the mean and standard error of the mean (SEM) from at least three independent experiments and analyzed with GraphPad Prism 8.0 software. Significant statistical differences between two groups were determined by the two-tailed unpaired Student’s t test and for three or more groups, one-way ANOVA (followed by a Dunnett post hoc test) was used for the statistical analysis. P-values of 0.05 (∗), 0.01 (∗∗) and 0.001 (∗∗∗) were assumed as the level of significance for the statistical tests carried out.
RNA extraction and RT-qPCR assay
We analyzed the RNA expression level of the target gene in the patients with reverse transcription-quantitative PCR (RT-qPCR). Total RNAs were extracted from peripheral blood mononuclear cells (PBMCs) using Trizol reagent (Invitrogen, USA). cDNA was synthesized from 2 µg of total RNA according to the manufacturer’s instructions (Takara, Japan). RT-qPCR was performed using the QuantStudio 3 system (Thermo Fisher Scientific, USA), and the relative gene expression was normalized to the internal control ACTB. Primer sequences of target genes were as follows, and data analysis was performed using the 2−ΔΔCt method.
Gene | Forward (5’-3’) | Reverse (5’-3’) |
|---|---|---|
ACTB | AGAGCCTCGCCTTTGCC | GGGGTACTTCAGGGTGAGGA |
NEAT1 | GATCTTTTCCACCCCAAGAGTACATAA | CTCACACAAACACAGATTCCACAAC |
Mendelian randomization analysis
To identify risk factors influencing AAO of ALS, we further performed Mendelian randomization (MR) analysis to evaluate causal inference among 21 exposures for which there was prior evidence for an association with ALS. These include seven behavioral-related traits: body mass index, years of schooling (educational attainment), alcoholic drinks per week, age of smoking initiation, cigarettes per day, days per week of moderate physical activity and days per week of vigorous activity; three blood pressure traits (coronary artery disease, diastolic blood pressure, and systolic blood pressure); six immune system traits (basophil, eosinophil, lymphocyte, monocyte, neutrophil, and white blood cell counts) and C-reactive protein; and four lipid traits (HDL cholesterol, LDL cholesterol, total cholesterol (TC) and triglyceride levels) (Supplementary Table 1). SNPs that passed the genome-wide significance threshold (P < 5E-08) were chosen as instrumental variables, which were then clumped based on the 1,000 Genomes Project LD structure [23]. Harmonization was undertaken to rule out strand mismatches and ensure alignment of SNP effect sizes.
We performed a two-sample MR analysis using the random effects inverse variance weighted (IVW) method [24], which was most widely used in MR studies and could provide robust causal estimates under the absence of directional pleiotropy. A P value below 2.38E-03 (0.05/21) was considered statistically significant after the Bonferroni correction. In addition, we conducted comprehensive sensitivity analyses to estimate potential violations of the model assumptions in the MR analysis. We conducted Mendelian randomization pleiotropy residual sum and outlier (MR-PRESSO) analysis and leave-one-out analysis to detect outlier instrumental variables. Outlier instrumental variables identified by the MR-PRESSO analysis were removed step-by-step to reduce the effect of horizontal pleiotropy. Cochran’s Q test was executed to check heterogeneity across the individual causal effects. MR-Egger regression was performed to evaluate the directional pleiotropy of instrumental variables. To evaluate the strength of each instrumental variable, we computed the F-statistic of each SNP. The statistical analyses were conducted using R package TwoSampleMR 0.5.5 [25].
Results
Demographics and heritability
The final statistical analysis included a total of 2,788 patients after quality control, with 2,230 in the discovery phase and 558 patients in the replication phase. The average AAO (SD) was 54.56 (11.56) with a sex ratio of 1.40 (male/female: 1301/929) in the discovery phase, and the average AAO (SD) was 54.69 (11.33) with a sex ratio of 1.46 (male/female: 331/227) in the replication phase (Supplementary Table 2). The overall distribution of AAO was shown in Supplementary Fig. 1. Generally, males tend to have later AAO than females (55.00 vs. 54.00), but the difference was not significant (P = 0.2) (Supplementary Fig. 2). The total heritability was 0.24 (SE = 0.09) estimated using GCTA-GREML with default parameters [26], which was less than the heritability of risk for ALS (~ 0.50) [27, 28].
Genome-wide association results
We performed genome-wide association analysis using a Cox proportional hazards model in the discovery and replication phases, and then combined the results from both stages into a meta-analysis. The principal component analysis revealed no descent outlier (Supplementary Fig. 3). The genomic inflation factor λ was 1.020 and 1.025 in two stages, suggesting minimal bias from population stratification. In the discovery stage, one locus rs6801884 (SATB1; KCNH8) reached genome-wide significance level (P = 1.81E-11, beta = 0.99, SE = 0.15), and another locus rs10128627 (FRMD8) was suggestively significant (P = 3.49E-07, beta = 0.31, SE = 0.06).
In the replication stage, the locus rs10128627 was still nominally associated with AAO (P = 0.01, beta = 0.33, SE = 0.13), while the other variant rs6801884 showed no association (P = 0.54, beta = 0.15, SE = 0.25). In the pooled analysis of two stages, both variants were significantly associated with AAO of ALS, namely rs10128627 (P = 1.54E-08, beta = 0.31, SE = 0.05) and rs6801884 (P = 1.15E-09, beta = 0.77, SE = 0.13) (Fig. 1). The variant rs10128627 resulted in earlier AAO by ~ 3.15 years, and the trend was similar in males (~ 2.86 years) and females (~ 3.25 years) (Fig. 2A-C). The variant rs6801884 resulted in earlier AAO by ~ 6.52 years, and the trend was similar in males (~ 6.59 years) and females (~ 6.32 years) (Fig. 2D-F). However, heterogeneity was detected for the locus rs6801884 using Cochran’s Q test between two stages (Cochran’s Q statistics: 88.23, Cochran’s Q P value: 3.60E-03). Therefore, further replication for this locus in additional cohort was still necessary. Gene-based association analysis showed association between FRMD8 and AAO of ALS (P = 1.25E-06) (Supplementary Fig. 4).

Genome-wide association analysis of AAO of ALS. (A) Manhattan plot showing GWAS results for AAO of ALS. (B) Regional plot of the association signal of rs10128627 by LocusZoom. (C) Regional plot of the association signal of rs6801884 by LocusZoom. Reference data of Asian population from 1,000 Genomes were used for linkage disequilibrium calculation

Effect of target risk loci on AAO of ALS. Kaplan-Meier survival curves of AAO of ALS (A) in both sexes, (B) in males, and (C) in females in relation to rs10128627. Kaplan-Meier survival curves of AAO of ALS (D) in both sexes, (E) in malesm and (F) in females in relation to rs6801884
Functional annotation of the significant signals
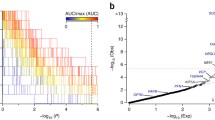
Based on data from GTEx and QTLbase, we found that rs10128627 was a cis-eQTL for NEAT1 in multiple brain tissues and whole blood (Table 1; Fig. 3A, Supplementary Fig. 5), while no cis-eQTL was identified for rs6801884. Given the findings from the eQTL analysis, we further performed colocalization analysis, and identified colocalization signals between locus rs10128627 and eQTLs regulating the expression of NEAT1 in the brain and whole blood, suggesting the locus rs10128627 might be associated with the AAO of ALS by functionally modulating the expression of NEAT1 (Supplementary Table 3). Meanwhile, a chromatin looping interaction between rs10128627 and the NEAT1 promoter was detected using data from GeneHancer in GeneCards (GH11J065402).

Functional analysis of lead SNP rs10128627. (A) The effect of rs10128627 on NEAT1 expression in brain tissues and blood based on data from GTEx. (B, C) The schematic diagram shows the structure of firefly luciferase reporter plasmid. (D) The plasmid with the variant T > C significantly increased the ratio of firefly/Renilla luciferase reporter gene expression compared to the wild type. Data are shown as the mean ± SEM values and are the result of three independent experiments. *P < 0.05, **P < 0.01 and ***P < 0.001. NES, normalized effect size. (E) RT-qPCR analysis of peripheral blood mononuclear cells (PBMCs) showing higher expression of NEAT1 in patients with variant rs10128627. Pneat1 denotes the promoter of NEAT1.
To further explore the regulatory function of rs10128627 on NEAT1 expression, we conducted a dual-luciferase reporter assay in Hela cells. We observed that the rs10128627-C risk allele significantly increased the luciferase activity relative to the rs10128627-T reference allele, indicating the T > C alteration was associated with the upregulation of NEAT1, consistent with the results from the cis-eQTL analysis (Fig. 3B-D). To further explore the effect of the variant rs10128627 on the expression of NEAT1, we assessed the RNA levels among totally 40 age- and sex-matched patients with or without rs10128627 via RT-qPCR. We found significantly higher expression of NEAT1 in the patients with rs10128627 than those without (P = 0.012) (Fig. 3E). Taken together, the combined evidence pointed to the hypothesis that the identified locus rs10128627 might be associated with the AAO of ALS by functionally modulating the expression of NEAT1, which needed further exploration.
PRS and AAO of ALS
PRS based on disease risk loci identified from GWAS has been recognized as a genetic predictor for AAO of other neurodegenerative disorders like PD [29] and AD [30], while it has not been estimated for ALS. In the current study, we evaluated the association between AAO of ALS and PRS calculated from summary statistics on risk of ALS in the European and Asian populations respectively. However, we did not identify significant association (Fig. 4A, B). In the targeted analysis of risk SNPs for ALS, no variant was significantly associated with AAO of ALS. However, such results should be interpreted with caution since the significant SNPs were based on individuals of European ancestry, while these SNPs showed no association in the Asian population [14].

Results for target SNP and PRS analysis. (A) Cox proportional HRs for genome-wide significant SNPs, and PRS on age at onset (AAO) of ALS. Estimated HRs are displayed with error bars corresponding to 95% CIs. Higher effect corresponds to earlier AAO. (B) Effect estimates from a linear regression model of AAO of ALS. Lower effect estimates correspond to earlier AAO. Effect estimates from linear regression are displayed with error bars corresponding to 95% CIs. (C) Differential AAO in patients with different PRS of AAO of ALS. “0” denotes the patients in the first quartile of the PRS distribution, while “1” denotes the patients in the last quartile of the PRS distribution. (D) ROC curves for prediction of early-onset ALS. The black curve was plotted with PRS of risk of ALS. The red curve was plotted with PRS of AAO of ALS.
In addition, we calculated PRS of AAO for each individual using summary statistics of AAO of ALS from our analysis. The individuals in the first quartile of the PRS distribution had significantly earlier AAO than those in the last quartile (53.28 vs. 57.06) (Fig. 4C), suggesting PRS of AAO might provide valuable information in predicting AAO of ALS. Then we evaluated the potential utility of PRS in predicting early-onset ALS. The model using PRS from AAO of ALS could achieve a higher area under curve (AUC) of 0.59, compared with the model using PRS from risk of ALS (AUC: 0.53) (Fig. 4D).
MR analysis
Previous epidemiological studies have identified a number of non-genetic risk factors implicated in the risk of ALS. However, whether they could influence AAO of ALS was still unexplored. In the current study, we studied 21 putative risk factors to infer causal association using the MR approach. Results showed that higher eosinophil, TC, and LDL were nominally associated with earlier AAO, while higher monocyte was associated later AAO of ALS (Fig. 5, Supplementary Figs. 6–9). The Cochran’s Q test did not detect heterogeneity of effects across the instrumental variables (Supplementary Table 4). The F statistics of all the instrumental variables were above 10 (ranging from 29 to 5033), indicating absence of weakness in the selected instruments. No apparent horizontal pleiotropy was observed as the intercept of MR-Egger was not significantly deviated from zero. Meanwhile, no potential instrumental outlier was detected by the MR-PRESSO analysis. The leave-one-out results suggested that the causal effect was not driven by a single instrumental variable.

Forest plot showing results from the Mendelian randomization analysis. Estimates are per 1 standard deviation (SD) increase in the trait. Red line denotes nominal association (P < 0.05)
Discussion
Several GWAS have been conducted to explore the genetic factors for susceptibility of ALS, while the genetic determinants for AAO of ALS were still less explored. To fill this research gap, we performed a GWAS in 2,841 Chinese patients with ALS, and identified a novel locus rs10128627 (FRMD8) associated with earlier AAO of ALS by ~ 3.15 years. Colocalization and functional analyses suggested the locus rs10128627 might function by regulating the expression of NEAT1. Our results enhanced the current understanding of the genetic background in AAO of ALS, and provided a novel research target for the pathogenesis of ALS.
The significant locus rs10128627, which was associated with earlier AAO of ALS, was suggested to up-regulate the expression of NEAT1 in multiple brain tissues and whole blood. Although NEAT1 has not been identified as risk gene for ALS by GWAS, multiple functional studies on NEAT1 suggested its essential role in neurodegenerative diseases including ALS [31]. NEAT1 is a highly and ubiquitously expressed long non-coding RNA (lncRNA) forming a scaffold for a specific RNA granule in the nucleus and the paraspeckle, which plays an important role specifically in degenerating spinal motor neurons [32]. Previous findings have suggested that NEAT1 might act as a scaffold of RNAs and RNA-binding proteins in the nuclei of motor neurons in ALS, thus modulating the functions of ALS-associated RNA-binding proteins during the early phase of ALS [33]. Increased paraspeckle formation has also been reported in the spinal cords of ALS patients relative to healthy individuals, suggesting paraspeckle formation might be a common hallmark of ALS patients [34]. Moreover, TDP-43 and FUS, the two major pathological proteins in ALS, both showed functional links to NEAT1. Using novel cell lines with the FUS gene modified by CRISPR/Cas9 and human patient fibroblasts, a previous study found that endogenous levels of mutant FUS caused accumulation of NEAT1 isoforms and paraspeckles, and further hypothesized that perturbed structure and functionality of paraspeckles accompanied by accumulation of non-paraspeckle NEAT1 may contribute to the disease severity in ALS-FUS [32]. Additionally, TDP-43 nuclear bodies are partially colocalized with nuclear paraspeckles, and increase of NEAT1 promotes TDP-43 liquid-liquid phase separation (LLPS) in vitro [35]. In addition, NEAT1 is highly enriched in neurons of the anterior horn of the spinal cord and cortical tissues of ALS patients [34, 36]. These multiple lines of evidence suggested the essential role of NEAT1 in the pathogenesis of ALS. In the current study, we illuminated the role of NEAT1 in the pathology of AAO of ALS from genetic and functional perspectives. The significant locus rs10128627 was suggested to up-regulate the expression of NEAT1, while CRISPR-assisted up-regulation of endogenous NEAT1 has been shown to cause neurotoxicity [37]. In our study, patients with the minor allele of rs10128627 showed earlier AAO by ~ 3.15 years. Cis-eQTL and enhancer analysis suggested the variant rs10128627 might upregulate the expression of NEAT1, while dual-luciferase reporter assay and RT-qPCR experiments further reinforced such hypothesis. Therefore, upregulated expression of NEAT1 might expedite the development of ALS and thus lead to earlier AAO, though further exploration was still necessary to investigate how this variant was involved in the pathogenesis of the disease. Notably, this variant was nominally associated with risk of ALS in two previous GWAS on ALS susceptibility (P = 0.027; beta = 0.04 and P = 0.02; beta = 0.04 respectively) [15, 38], suggesting this variant might increase the risk of ALS as well, consistent with our results that this variant was associated with earlier AAO. These results suggested potential shared pathogenesis between AAO and risk of ALS. However, another subsequent study showed insignificant association for this variant (P = 0.511), though the effect direction was the same (beta = 0.01) [39]. In addition, no significant association was identified for this variant in previous GWAS on AAO of ALS in the European population [8]. Notably, The MAF of the variant rs10128627 differs between different populations, ranging from 0.06 in East Asians, to 0.16 in Europeans and 0.26 in Latino/Admixed American based on data from gnomAD v3.1.2 (Supplementary Fig. 10), suggesting potential different effect of this variant in different populations. Therefore, further exploration in additional cohorts was warranted to better understand the association between this variant and disease risk and progression.
Another intergenic locus rs6801884 was significantly associated with AAO of ALS in the discovery stage. We tried to locate the driver gene for the significant locus using SnpEff and existent cis-eQTL evidence in available eQTL resources including GTEx, eQTLGen, Braineac, Brain xQTL Serve, and PsychEncode, but failed to map rs6801884 to a functional gene. Regulatory functions searched in RegulomeDB and HaploReg did not show clear associations either. Around the locus rs6801884 were two protein-coding genes KCNH8 and SATB1. Functionally, KCNH8 encodes a voltage-gated potassium channel that is primarily expressed in the nervous system, and plays a role in transmission pathways across chemical synapses and potassium channels, which is closely involved in the pathogenesis of ALS [40]. It has been suggested that the fasciculations in ALS are caused by an imbalance between functional sodium and potassium channels, and this ion channel dysfunction could be responsible for the motor neuron degeneration [41]. The main functions of KCNH8 include regulating neurotransmitter release and neuronal excitability. Previous study has demonstrated motor neuron hyperexcitability for ALS and its sensitivity to Kv7 agonists across iPSC lines, patients, and genotypic etiologies, and differential expression of voltage-gated potassium channels including KCNH8 was observed in ALS motor neurons [42]. These evidence suggested the potential role of KCNH8 in the pathogenesis of ALS through regulating potassium channel abnormalities. SATB1 is a ubiquitously expressed chromatin organizing factor, and mediates the transcriptional response of midbrain dopamine neurons to toxic insult [43]. Previous GWAS have identified SATB1 as a risk gene for PD, another common neurodegenerative disorder [44, 45], while no prominent reports about SATB1 in ALS were found. One lncRNA (SATB1-AS1) and one miRNA (MIR4791) were in the vicinity of this variant, but the functions of the two RNAs were still poorly studied, and we did not find evidence supporting their potential role in the pathogenesis of ALS. Notably, no significant association was identified for the variant rs6801884 in the replication phase, and Cochran’s Q test detected heterogeneity in the meta-analysis of discovery and replication stages. Failure of replication might be due to limited sample size since the MAF of this variant rs6801884 in East Asians is low (MAF = 0.01) (Supplementary Fig. 11). There is a high risk that the results might be susceptible to bias from the small sample size and the observed effect was due to chance. Therefore, further replication was necessary to verify the association between this locus and AAO of ALS.
Common genetic variants associated with ALS risk have a small but consistent effect on disease etiology, and might combine to expedite the onset of the disease. In the current study, we did not identify association between PRS and AAO of ALS, consistent with a recent study in the European population [14]. However, the results should be interpreted with caution due to the population stratification across populations and limited sample size of the Asian GWAS. Further exploration based on summary statistics from larger GWAS was still warranted. In addition, we demonstrated that PRS of AAO could aid in the prediction of early-onset ALS, suggesting potential to apply PRS of AAO in clinical trials to identify patients susceptible to early-onset ALS.
Previous observational studies have shown conflicting evidence regarding different risk factors in the risk of ALS. The unavoidable confounding factors and reverse causality also challenged the interpretation of these results. Using the MR approach, we demonstrated that higher TC and LDL were causally associated with earlier AAO of ALS. Correspondingly, previous studies have shown that higher TC and LDL might increase risk of ALS [14, 46, 47], suggesting the two lipids might play a harmful role in the pathogenesis of ALS. Neuroinflammation also plays an important role in the pathophysiology of ALS. Previous study has shown that changes in peripheral inflammatory markers contribute to the pathologic features of ALS [48]. In the current study, we demonstrated that higher eosinophil levels were causally associated with earlier AAO, while higher monocyte levels might delay the onset age. Similarly, infiltration of peripheral monocytes in the central nervous system was suggested to improve motor neuron survival in a genetic ALS mouse model [49], suggesting the potential protective role of monocytes in the disease. Meanwhile, eosinophil-derived neurotoxin level was significantly increased in the serum of patients with ALS as compared with healthy controls, suggesting the potentially harmful role of eosinophil in the pathophysiology of ALS [50]. However, the results should be interpreted with caution since only nominal association was identified. Meanwhile, the instrumental variables were obtained from GWAS in the European population, which might bring some bias. Therefore, further replication was still warranted.
Conclusions
We performed a GWAS on AAO of ALS in a large Chinese ALS cohort and identified a novel locus which might lead to earlier AAO by regulating the expression of NEAT1. Our findings supplement the current knowledge on the genetic architecture for AAO of ALS, and provide a novel target for further research on the pathogenesis of ALS and potential therapeutic options to delay the disease onset.
Data Availability
Summary statistics of the risk of ALS can be found in the original publication. Summary statistics of the risk factors for ALS in Mendelian randomization can be found in the original publication.
Abbreviations
- ALS:
-
amyotrophic lateral sclerosis
- GWAS:
-
genome-wide association study
- SNP:
-
single nucleotide polymorphisms
- MAF:
-
minor allele frequency
- PCA:
-
principal component analysis
- PRS:
-
polygenic risk score
- AUC:
-
area under curve
- ROC:
-
receiver operating characteristic
- eQTL:
-
expression quantitative trait loci
- LS:
-
linkage disequilibrium
- MR:
-
Mendelian randomization
- IVW:
-
inverse variance weighted
- RT-qPCR:
-
reverse transcription-quantitative PCR
- TC:
-
total cholesterol
- LDL:
-
low-density lipoprotein
- HDL:
-
high-density lipoprotein
References
van Es MA, Hardiman O, Chio A, Al-Chalabi A, Pasterkamp RJ, Veldink JH, van den Berg LH. Amyotrophic Lateral Sclerosis. Lancet (London England). 2017;390:2084–98.
Liu MS, Cui LY, Fan DS. Age at onset of Amyotrophic Lateral Sclerosis in China. Acta Neurol Scand. 2014;129:163–7.
Chio A, Moglia C, Canosa A, Manera U, D’Ovidio F, Vasta R, Grassano M, Brunetti M, Barberis M, Corrado L, et al. ALS phenotype is influenced by age, sex, and genetics: a population-based study. Neurology. 2020;94:E802–10.
Ferraro PM, Cabona C, Meo G, Rolla-Bigliani C, Castellan L, Pardini M, Inglese M, Caponnetto C, Roccatagliata L. Age at symptom onset influences cortical thinning distribution and survival in amyotrophic lateral sclerosis. Neuroradiology 2021.
Atsuta N, Watanabe H, Ito M, Tanaka F, Tamakoshi A, Nakano I, Aoki M, Tsuji S, Yuasa T, Takano H, et al. Age at onset influences on wide-ranged clinical features of sporadic Amyotrophic Lateral Sclerosis. J Neurol Sci. 2009;276:163–9.
Pupillo E, Bianchi E, Vanacore N, Montalto C, Ricca G, Della Cuna FSR, Fumagalli F, Castellani M, Poli F, Romeo F, et al. Increased risk and early onset of ALS in professional players from Italian Soccer teams. Amyotroph Lateral Scher Frontotemp Degenerat. 2020;21:403–9.
Naruse H, Ishiura H, Mitsui J, Takahashi Y, Matsukawa T, Tanaka M, Doi K, Yoshimura J, Morishita S, Goto J, et al. Burden of rare variants in causative genes for Amyotrophic Lateral Sclerosis (ALS) accelerates age at onset of ALS. J Neurol Neurosurg Psychiatry. 2019;90:537–42.
Langefeld CD, Consortium A. Age of onset of Amyotrophic Lateral Sclerosis is modulated by a locus on 1p34.1. Neurobiol Aging 2013, 34.
Brooks BR, Miller RG, Swash M, Munsat TL. El Escorial revisited: revised criteria for the diagnosis of Amyotrophic Lateral Sclerosis. Amyotroph Lateral Scler Other Motor Neuron Disorders: Official Publication World Federation Neurol Res Group Motor Neuron Dis. 2000;1:293–9.
Li C, Hou Y, Ou R, Gu X, Chen Y, Zhang L, Liu K, Lin J, Cao B, Wei Q, et al. Genetic determinants of Survival in Parkinson’s Disease in the Asian Population. Mov Disorders: Official J Mov Disorder Soc. 2022;37:1624–33.
Das S, Forer L, Schönherr S, Sidore C, Locke AE, Kwong A, Vrieze SI, Chew EY, Levy S, McGue M, et al. Next-generation genotype imputation service and methods. Nat Genet. 2016;48:1284–7.
de Leeuw CA, Mooij JM, Heskes T, Posthuma D. MAGMA: generalized gene-set analysis of GWAS data. PLoS Comput Biol. 2015;11:e1004219.
Choi SW, O’Reilly PF. PRSice-2: polygenic risk score software for biobank-scale data. GigaScience 2019, 8.
van Rheenen W, van der Spek RAA, Bakker MK, van Vugt JJFA, Hop PJ, Zwamborn RAJ, de Klein N, Westra H-J, Bakker OB, Deelen P, et al. Common and rare variant association analyses in Amyotrophic Lateral Sclerosis identify 15 risk loci with distinct genetic architectures and neuron-specific biology. Nat Genet. 2021;53:1636–48.
Benyamin B, He J, Zhao Q, Gratten J, Garton F, Leo PJ, Liu Z, Mangelsdorf M, Al-Chalabi A, Anderson L, et al. Cross-ethnic meta-analysis identifies association of the GPX3-TNIP1 locus with Amyotrophic Lateral Sclerosis. Nat Commun. 2017;8:611.
Nakamura R, Misawa K, Tohnai G, Nakatochi M, Furuhashi S, Atsuta N, Hayashi N, Yokoi D, Watanabe H, Watanabe H, et al. A multi-ethnic meta-analysis identifies novel genes, including ACSL5, associated with Amyotrophic Lateral Sclerosis. Commun Biology. 2020;3:526.
Gamazon ER, Segrè AV, van de Bunt M, Wen X, Xi HS, Hormozdiari F, Ongen H, Konkashbaev A, Derks EM, Aguet F, et al. Using an atlas of gene regulation across 44 human tissues to inform complex disease- and trait-associated variation. Nat Genet. 2018;50:956–67.
Zheng Z, Huang D, Wang J, Zhao K, Zhou Y, Guo Z, Zhai S, Xu H, Cui H, Yao H, et al. QTLbase: an integrative resource for quantitative trait loci across multiple human molecular phenotypes. Nucleic Acids Res. 2019;48:D983–91.
Fishilevich S, Nudel R, Rappaport N, Hadar R, Plaschkes I, Iny Stein T, Rosen N, Kohn A, Twik M, Safran M et al. GeneHancer: genome-wide integration of enhancers and target genes in GeneCards. Database: The Journal of Biological Databases and Curation 2017, 2017.
Giambartolomei C, Vukcevic D, Schadt EE, Franke L, Hingorani AD, Wallace C, Plagnol V. Bayesian test for colocalisation between pairs of genetic association studies using summary statistics. PLoS Genet. 2014;10:e1004383.
Ardlie KG, DeLuca DS, Segre AV, Sullivan TJ, Young TR, Gelfand ET, Trowbridge CA, Maller JB, Tukiainen T, Lek M, et al. The genotype-tissue expression (GTEx) pilot analysis: Multitissue gene regulation in humans. Sci (New York NY). 2015;348:648–60.
Li C, Hou Y, Ou R, Gu X, Chen Y, Zhang L, Liu K, Lin J, Cao B, Wei Q, et al. Genetic determinants of Survival in Parkinson’s Disease in the Asian Population. Mov Disord. 2022;37:1624–33.
Li C, Liu J, Lin J, Shang H. COVID-19 and risk of neurodegenerative disorders: a mendelian randomization study. Translational Psychiatry. 2022;12:283.
Li C, Ou R, Shang H. Rheumatoid arthritis decreases risk for Parkinson’s Disease: a mendelian randomization study. Npj Parkinson’s Disease. 2021;7:17.
Hemani G, Zheng J, Elsworth B, Wade KH, Haberland V, Baird D, Laurin C, Burgess S, Bowden J, Langdon R et al. The MR-Base platform supports systematic causal inference across the human phenome. eLife 2018, 7.
Yang J, Lee SH, Goddard ME, Visscher PM. GCTA: a tool for genome-wide complex trait analysis. Am J Hum Genet. 2011;88:76–82.
Ryan M, Heverin M, McLaughlin RL, Hardiman O. Lifetime risk and heritability of Amyotrophic Lateral Sclerosis. JAMA Neurol. 2019;76:1367–74.
Ryan M, Heverin M, Pender N, McLaughlin R, Hardiman O. Heritability of ALS: a Population-based study over 24 years. (S54.001). Neurology. 2019;92:54001.
Li C, Ou R, Chen Y, Gu X, Wei Q, Cao B, Zhang L, Hou Y, Liu K, Chen X et al. Genetic Modifiers of Age at Onset for Parkinson’s Disease in Asians: A Genome-Wide Association Study. Mov Disorders: Official J Mov Disorder Soc 2021.
Cruchaga C, Del-Aguila JL, Saef B, Black K, Fernandez MV, Budde J, Ibanez L, Deming Y, Kapoor M, Tosto G, et al. Polygenic risk score of sporadic late-onset Alzheimer’s Disease reveals a shared architecture with the familial and early-onset forms. Alzheimer’s Dement J Alzheimer’s Assoc. 2018;14:205–14.
Prinz F, Kapeller A, Pichler M, Klec C. The implications of the long non-coding RNA NEAT1 in non-cancerous Diseases. Int J Mol Sci 2019, 20.
An H, Skelt L, Notaro A, Highley JR, Fox AH, La Bella V, Buchman VL, Shelkovnikova TA. ALS-linked FUS mutations confer loss and gain of function in the nucleus by promoting excessive formation of dysfunctional paraspeckles. Acta Neuropathol Commun. 2019;7:7.
Nishimoto Y, Nakagawa S, Hirose T, Okano HJ, Takao M, Shibata S, Suyama S, Kuwako K, Imai T, Murayama S, et al. The long non-coding RNA nuclear-enriched abundant transcript 1_2 induces paraspeckle formation in the motor neuron during the early phase of Amyotrophic Lateral Sclerosis. Mol Brain. 2013;6:31.
Shelkovnikova TA, Kukharsky MS, An H, Dimasi P, Alexeeva S, Shabir O, Heath PR, Buchman VL. Protective paraspeckle hyper-assembly downstream of TDP-43 loss of function in Amyotrophic Lateral Sclerosis. Mol Neurodegener. 2018;13:30.
Wang C, Duan Y, Duan G, Wang Q, Zhang K, Deng X, Qian B, Gu J, Ma Z, Zhang S, et al. Stress induces dynamic, cytotoxicity-antagonizing TDP-43 Nuclear bodies via Paraspeckle LncRNA NEAT1-Mediated liquid-liquid phase separation. Mol Cell. 2020;79:443–458e447.
Tollervey JR, Curk T, Rogelj B, Briese M, Cereda M, Kayikci M, König J, Hortobágyi T, Nishimura AL, Zupunski V, et al. Characterizing the RNA targets and position-dependent splicing regulation by TDP-43. Nat Neurosci. 2011;14:452–8.
Suzuki H, Shibagaki Y, Hattori S, Matsuoka M. C9-ALS/FTD-linked proline-arginine dipeptide repeat protein associates with paraspeckle components and increases paraspeckle formation. Cell Death Dis. 2019;10:746.
Iacoangeli A, Lin T, Al Khleifat A, Jones AR, Opie-Martin S, Coleman JRI, Shatunov A, Sproviero W, Williams KL, Garton F, et al. Genome-wide Meta-analysis finds the ACSL5-ZDHHC6 locus is Associated with ALS and Links Weight loss to the Disease Genetics. Cell Rep. 2020;33:108323.
van Rheenen W, van der Spek RAA, Bakker MK, van Vugt J, Hop PJ, Zwamborn RAJ, de Klein N, Westra HJ, Bakker OB, Deelen P, et al. Common and rare variant association analyses in Amyotrophic Lateral Sclerosis identify 15 risk loci with distinct genetic architectures and neuron-specific biology. Nat Genet. 2021;53:1636–48.
Maglemose R, Hedegaard A, Lehnhoff J, Dimintiyanova KP, Moldovan M, Grøndahl L, Meehan CF. Potassium channel abnormalities are consistent with early axon degeneration of motor axons in the G127X SOD1 mouse model of Amyotrophic Lateral Sclerosis. Exp Neurol. 2017;292:154–67.
Bostock H, Sharief MK, Reid G, Murray NM. Axonal ion channel dysfunction in Amyotrophic Lateral Sclerosis. Brain. 1995;118(Pt 1):217–25.
Wainger BJ, Kiskinis E, Mellin C, Wiskow O, Han SS, Sandoe J, Perez NP, Williams LA, Lee S, Boulting G, et al. Intrinsic membrane hyperexcitability of Amyotrophic Lateral Sclerosis patient-derived motor neurons. Cell Rep. 2014;7:1–11.
Riessland M, Kolisnyk B, Kim TW, Cheng J, Ni J, Pearson JA, Park EJ, Dam K, Acehan D, Ramos-Espiritu LS, et al. Loss of SATB1 induces p21-Dependent Cellular Senescence in post-mitotic dopaminergic neurons. Cell Stem Cell. 2019;25:514–530e518.
Chang D, Nalls MA, Hallgrimsdottir IB, Hunkapiller J, van der Brug M, Cai F, Kerchner GA, Ayalon G, Bingol B, Sheng M, et al. A meta-analysis of genome-wide association studies identifies 17 new Parkinson’s Disease risk loci. Nat Genet. 2017;49:1511–6.
Nalls MA, Blauwendraat C, Vallerga CL, Heilbron K, Bandres-Ciga S, Chang D, Tan M, Kia DA, Noyce AJ, Xue A, et al. Identification of novel risk loci, causal insights, and heritable risk for Parkinson’s Disease: a meta-analysis of genome-wide association studies. Lancet Neurol. 2019;18:1091–102.
Zeng P, Zhou X. Causal effects of blood lipids on Amyotrophic Lateral Sclerosis: a mendelian randomization study. Hum Mol Genet. 2019;28:688–97.
Mariosa D, Hammar N, Malmström H, Ingre C, Jungner I, Ye W, Fang F, Walldius G. Blood biomarkers of carbohydrate, lipid, and apolipoprotein metabolisms and risk of Amyotrophic Lateral Sclerosis: a more than 20-year follow-up of the Swedish AMORIS cohort. Ann Neurol. 2017;81:718–28.
Murdock BJ, Zhou T, Kashlan SR, Little RJ, Goutman SA, Feldman EL. Correlation of Peripheral Immunity with Rapid Amyotrophic Lateral Sclerosis progression. JAMA Neurol. 2017;74:1446–54.
Zondler L, Müller K, Khalaji S, Bliederhäuser C, Ruf WP, Grozdanov V, Thiemann M, Fundel-Clemes K, Freischmidt A, Holzmann K, et al. Peripheral monocytes are functionally altered and invade the CNS in ALS patients. Acta Neuropathol. 2016;132:391–411.
Liu GT, Hwang CS, Hsieh CH, Lu CH, Chang SL, Lee JC, Huang CF, Chang HT. Eosinophil-derived neurotoxin is elevated in patients with amyotrophic lateral sclerosis. Mediators of inflammation 2013, 2013:421389.
Acknowledgements
We sincerely thank the patients and their families who were enrolled in this study for their time and support.
Funding
This research was supported by the funding of the Sichuan Science and Technology Program (Grant No. 2022ZDZX0023).
Author information
Authors and Affiliations
Contributions
(1) Research project: (A) Conception, (B) Organization, (C) Execution; (2) Statistical Analysis: (A) Design, (B) Execution, (C) Review and Critique; (3) Manuscript: (A) Writing of the First Draft, (B) Review and Critique; (4) A. Patients enrollment and clinical data collection.
LCY: 1 A, 1 C, 2 A, 2B, 2 C, 3 A; WQQ: 3B, 4 A; HYB: 3B, 4 A; LJY: 3B, 4 A; ORW: 3B, 4 A; ZLY: 3B, 4 A; JQR: 3B, 4 A; XY: 3B, 4 A; LKC: 3B, 4 A; CXP: 3B, 4 A; YTM: 3B, 4 A; SW: 3B, 4 A; ZB: 3B, 4 A; WY: 3B, 4 A; SHF: 1B, 2 A, 2 C, 3B. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the West China Hospital of Sichuan University, and all participants have signed informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
13024_2023_669_MOESM1_ESM.docx
Supplementary Material 1. Additional file 1: Supplementary Figure 1. Age at onset distribution in the patients with ALS. Supplementary Figure 2. Effect of gender on age at onset of ALS. Supplementary Figure 3. Principal component analysis plot of populations from 1000 Genomes Project and the ALS patients in our cohort. Supplementary Figure 4. Results from genome-wide gene-based association analysis. Supplementary Figure 5. QTLbase variant-level query results for rs10128627. Supplementary Figure 6. Mendelian randomization analysis results for eosinophil on age at onset of ALS. Supplementary Figure 7. Mendelian randomization analysis results for monocyte on age at onset of ALS. Supplementary Figure 8. Mendelian randomization analysis results for LDL cholesterol on age at onset of ALS. Supplementary Figure 9. Mendelian randomization analysis results for total cholesterol on age at onset of ALS. Supplementary Figure 10. Minor allele frequency of variant rs10128627 in different populations. Supplementary Figure 11. Minor allele frequency of variant rs6801884 in different populations.
13024_2023_669_MOESM2_ESM.docx
Supplementary Material 2. Additional file 2: Supplementary Table 1. Summary data of GWAS used in the Mendelian randomization analysis. Supplementary Table 2. Demographics of the study subjects. Supplementary Table 3. Candidate risk genes identified by colocalization analysis. Supplementary Table 4. Results from heterogeneity and horizontal pleiotropy analysis.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, C., Wei, Q., Hou, Y. et al. Genome-wide analyses identify NEAT1 as genetic modifier of age at onset of amyotrophic lateral sclerosis. Mol Neurodegeneration 18, 77 (2023). https://doi.org/10.1186/s13024-023-00669-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13024-023-00669-6