
Abstract
Vertebral malformations (VMs) pose a significant global health problem, causing chronic pain and disability. Vertebral defects occur as isolated conditions or within the spectrum of various congenital disorders, such as Klippel–Feil syndrome, congenital scoliosis, spondylocostal dysostosis, sacral agenesis, and neural tube defects. Although both genetic abnormalities and environmental factors can contribute to abnormal vertebral development, our knowledge on molecular mechanisms of numerous VMs is still limited. Furthermore, there is a lack of resource that consolidates the current knowledge in this field. In this pioneering review, we provide a comprehensive analysis of the latest research on the molecular basis of VMs and the association of the VMs-related causative genes with bone developmental signaling pathways. Our study identifies 118 genes linked to VMs, with 98 genes involved in biological pathways crucial for the formation of the vertebral column. Overall, the review summarizes the current knowledge on VM genetics, and provides new insights into potential involvement of biological pathways in VM pathogenesis. We also present an overview of available data regarding the role of epigenetic and environmental factors in VMs. We identify areas where knowledge is lacking, such as precise molecular mechanisms in which specific genes contribute to the development of VMs. Finally, we propose future research avenues that could address knowledge gaps.
Similar content being viewed by others


Background
The segmentally organized human vertebral column is built of 31–33 vertebrae, comprising 7 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 2–4 coccygeal vertebrae fused into one bone (i.e. coccyx), housing neurons, the spinal cord, and blood vessels. Development of the embryonic vertebral column is complex, and deep understanding of this process at a molecular level is critical for grasping the origin of vertebral defects. The notochord and somites are the most important structures responsible for the vertebral column formation. Somites develop from the paraxial mesoderm on either side of the midline, and then differentiate into ventromedial sclerotome and dorsolateral dermomyotome. Sclerotome cells migrate around the notochord and the neural tube, subsequently segregating into two distinct regions: a cranial domain comprising loosely arranged cells and a caudal region characterized by densely packed cells. The process ultimately leads to development of the vertebral bodies, arches, and transverse and spinous processes. The notochord plays a role in establishing the embryo's longitudinal axis, determining the vertebral column orientation, and guiding the formation of the nucleus pulposus of the intervertebral discs. On the other hand, the dermomyotome gives rise to the dermis and skeletal muscles [1,2,3,4] (Fig. 1). Chondrification and ossification are the final steps in the formation of the vertebrae [5]. On the molecular level, vertebral column development depends on the proper action of several signaling pathways, including Wnt, fibroblast growth factor (FGF), Notch, Hedgehog (Hh), retinoic acid (RA), transforming growth factor β (TGF-β), and bone morphogenic protein (BMP) [6,7,8]. The primary function of the vertebral column is to provide structural support for the body.

Schematic representation of vertebral development in human embryo. NT – neural tube. Created with Biorender.com
Vertebral malformations (VMs) is an umbrella term describing an etiologically heterogeneous group of congenital defects that may be caused by pathogenic variants in the somitogenesis genes, environmental factors, or a combination of both [9,10,11]. The prevalence of VMs is approximately 1–2 per 2000 live births, however, their actual incidence may be higher due to missed or delayed diagnosis [12, 13]. Depending on which process of the vertebral development has failed, VMs have been divided into segmentation, formation, mixed (both segmentation and formation), or other defects [14]. In addition to vertebral defects, fused or missing ribs or their malalignment are often noted [15]. Vertebral defects may be isolated or associated with other congenital anomalies, including congenital kyphosis or scoliosis, VACTERL association, or syndromes such as Klippel–Feil, spondylocostal dysostosis, spondylothoracic dystrophy, Alagille, Gorlin, CHARGE, Jarcho-Levin, Goldenhar or Joubert syndromes [10, 13, 16, 17]. Patients affected by VMs may be either asymptomatic or present with significant disabilities, resulting in body deformations, motor impairment, respiratory distress or chronic pain which seriously reduces their quality of life [10, 18]. Since there is no cure for VMs, treatment focuses on symptoms managed with either lifestyle or surgical interventions. Surgery is indicated mainly in younger patients with thoracolumbar anomalies and particular VMs, i.e., Klippel–Feil syndrome and congenital scoliosis [19,20,21]. The surgical intervention options encompass convex hemiepiphysiodesis, instrumented fusion, osteotomies, vertebrectomies, and utilization of growth-promoting systems [22].
Herein, we present a comprehensive clinical description of rare congenital vertebral column defects, provide an overview of the most relevant and recent findings concerning the molecular and environmental etiology of VMs, and discuss future research directions. In 2009 and 2013, Giampietro et al. released their two review articles in this field, and since then no other comprehensive reviews of the current literature have been published [11, 13]. Our paper attempts to fill the knowledge gap by synthesizing and interpreting the latest literature to offer new insights into the molecular background of VMs.
Classification of VMs
Vertebral anomalies result from formation, segmentation, or simultaneous formation and segmentation defects [14]. Formation failure is due to the absence of vertebral elements occurring in the anterior, anterolateral, posterior, posterolateral, or lateral region and may be complete (hemivertebra, butterfly vertebra, vertebral aplasia) or partial (wedge vertebra). On the other hand, segmentation failure (unilateral unsegmented bar, block vertebra) arises from abnormal embryological segmentation of the vertebral column (Fig. 2).

Classification of vertebrae malformations based on the segmentation or formation failures. Segmentation defects encompass block vertebra and unilateral unsegmented bar, whereas formation defects include wedge vertebra, hemivertebra, and butterfly vertebra. Hemivertebra is classified into fully segmented, incarcerated, semisegmented, and nonsegmented. Segmentation defects were illustrated using the example of the lumbar spine segment. Created with Biorender.com
Hemivertebra (HV) is one of the most common vertebral anomalies, with an estimated incidence from 1 to 10 per 10,000 live births, and it is mainly detected within the thoracic (Th8) and lumbar spine [23,24,25]. HV occurs when half of the vertebral body fails to develop (unilateral defect), and one pedicle is missing [14]. It has been shown that HV is not a supernumerary vertebra but rather an underdeveloped innate vertebra that originates from asynchronous growth of the hemimetameric pair [26]. Based on the growth pattern and positioning of the HV, the deformity is classified into four subtypes – fully segmented, incarcerated, semi-segmented, and nonsegmented [27]. Importantly, HV represents a common cause of congenital scoliosis [28]. Butterfly vertebra (BV), also termed sagittal cleft vertebra, anterior rachischisis, somatoschisis, or anterior spina bifida, is a rare vertebral malformation of unknown incidence. Due to a lack of midline fusion of two lateral chondrification centers, BV is characterized by two hemivertebrae separated by a cartilaginous septum giving the butterfly appearance on X-ray imaging [29, 30]. The defect occurs primarily in the lumbar spine or less frequently in the thoracic region, and may cause scoliosis or kyphosis [31]. Total aplasia of the vertebral body was proposed to be the consequence of chondrification center defect, and it usually leads to kyphosis. In addition, the presence of the butterfly malformation is associated with various medical conditions, such as Alagille syndrome, Crouzon syndrome, Jarcho-Levin syndrome, and Pfeiffer syndrome [32,33,34,35]. Finally, a wedge vertebra results from a unilateral asymmetry of the vertebral body where two pedicles are present. The anomaly is generally characterized by partial, unilateral chondrification and ossification [14]. Recent findings underscore the role of wedge-shaped vertebrae as a risk factor in the pathogenesis of symptomatic upper lumbar disc herniation [36].
Segmentation failure is usually observed in the cervical and lumbar spine [37]. The most frequent segmentation defect is the unilateral unsegmented bar resulting from a malformation of two or more adjacent vertebrae, leading to the fusion of over three vertebrae. The malformation results in a bony block that involves the disc spaces and facet joints, accompanied by rib fusions on the same side as the bar. A characteristic feature of an unsegmented bar is a lack of growth plates. However, the unaffected side of the vertebral column continues to grow, leading to significant spinal deformities such as congenital scoliosis [21]. The unsegmented bars can occur together with hemivertebrae, which carries a greater risk for the progression of vertebral deformation than each of these defects alone. Block vertebrae are formed due to somite segmentation failure, culminating in partial or complete fusion of the adjacent vertebrae. The morphological features of the condition include a biconcave shape at the fusion site and the presence of residual intervertebral disk material (chorda remnants) in the proximity of the fusion area. Predominantly only two vertebrae within the cervical, thoracic, or lumbar regions of the spine are affected [14]. The most frequent location for the block vertebrae is C2-C3, exhibiting a strong association with Klippel–Feil syndrome [38, 39].
VM genetic etiology
The genetic etiology of VMs remains unexplored in the majority of affected patients. Vertebral defects may accompany the features of various, often rare, congenital syndromes. Based on the Human Phenotype Ontology database, we have listed syndromes characterized by vertebral defects, in which genetic background has been revealed (Table 1). The KIAA1217 gene has not been associated with any syndrome yet. However, very recent investigations suggest its potential involvement in VMs. Rare variants within this gene have been identified in 10 patients with vertebral fusions and other osseous spine abnormalities [40]. In the following chapters of this review, we describe vertebral defects specific to particular segments of the spine currently intensively investigated for their genetic background. Congenital osseous torticollis in the form of Klippel–Feil syndrome was detailed as a cervical spine defect, congenital scoliosis, and spondylocostal dysostoses were depicted as thoracic/lumbar spine defects, developmental spinal stenosis was listed as lumbar spine defect, whereas sacral agenesis as a sacral spine defect. The comprehensive overview of all the genes from our publication is presented in Table 2. Our analysis shows the participation of VM genes in multiple signaling pathways, particularly in Wnt (Wnt/β-catenin, Wnt/PCP), ERK/MAPK, TGF-β, Notch, Hedgehog, BMP, and PI3K/Akt.
Cervical spine
Congenital osseous torticollis—Klippel–Feil syndrome
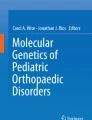
Klippel–Feil syndrome (KFS) is a complex skeletal disorder characterized by the fusion of at least two cervical vertebrae, initially reported by Maurice Klippel and Andre Feil [41]. Congenital vertebral fusions may occur at any cervical spine level, although the most often affected vertebrae are C2-C3 and C5-C6 [42]. Since the first description of this syndrome, three morphological subtypes of the disorder have been identified: type I, characterized by the fusion of cervical and upper thoracic vertebrae, type II, with only one or two pairs of fused cervical vertebrae (Fig. 3), and type III, with the fusion of cervical vertebrae combined with the fusion of lower thoracic or lumbar vertebrae [43]. KFS is reported in 1 of 40,000 to 42,000 newborns worldwide. However, the incidence of this syndrome remains underreported due to a lack of population screening studies and frequent asymptomatic occurrence. Studies involving 2917 patients at the emergency department and 131 patients with cervical spondylotic myelopathy, who underwent spine imaging, revealed the prevalence of KFS to be 0.58% and 3.82%, respectively [42, 44]. A diagnosis of KFS is based on the clinical triad, which includes a short neck, low-set posterior hairline, and limited head and neck movements. Notably, only 34–74% of the affected individuals manifest all three symptoms [45]. KFS can be isolated or associated with numerous abnormalities, including scoliosis, Sprengel deformity, spina bifida occulta, renal abnormalities, vision and hearing impairment, congenital heart defects, and neurological anomalies [46,47,48].

Anteroposterior (A) and lateral (B) cervical spine radiographs showing vertebrae fusion at C6-C7 in a patient with Klippel–Feil syndrome
There are four genetic forms of KFS with dominant and recessive inheritance: KFS1, KFS2, KFS3, and KFS4 (Table 3). In KFS patients, many chromosomal abnormalities have been reported, i.e., inv(8)(q22.2q22.3); t(5;17)(q11.2;q23); inv(2)(p12q34) or t(5;8)(q35.1;p21.1) [49,50,51,52]. Furthermore, according to Online Mendelian Inheritance in Man (OMIM), pathogenic variants in different genes are associated with autosomal dominant KFS, i.e., GDF6 (MIM: 601147), GDF3 (MIM: 606522), and autosomal recessive KFS, i.e., MEOX1 (MIM: 600147), and MYO18B (MIM: 607295). The GDF3 and GDF6 genes are members of the TGF-β/BMP family, and their protein products are essential for forming and developing bones and joints. The MEOX1 gene encodes a homeobox protein MOX-1, a transcription factor expressed in somites. MOX-1 regulates separation of vertebrae from one another during early development. Despite the clinical heterogeneity of KFS, the patients harboring pathogenic variants in the MEOX1 gene display multiple common features, i.e., Sprengel’s deformity, congenital scoliosis, and an ectopic omovertebral bone [53, 54]. The MYO18B gene encodes an unconventional class XVIII myosin, mainly expressed in human cardiac and skeletal muscle. The protein plays a potential role in cellular processes and transcriptional regulation of muscle-specific genes [55]. A null variant in MYO18B was linked to a novel developmental disorder that combines KFS and myopathy. Noteworthy, only a small subset of KFS cases could be explained by pathogenic variants in one of the four mentioned genes [56].
Multiple genes have been proposed as potential candidates responsible for KFS. A homozygous frameshift variant in RIPPLY2 was identified in a patient suffering from KFS with heterotaxy. Studies indicated that variants in RIPPLY2 could be responsible for a new type of KFS. However, further research is required to verify this possible link [57, 58]. Mouse models also identified some variants in the PAX gene family and the Notch signaling pathway as potential genetic cause of the described disorder [59]. Abnormalities in PAX1 have been identified in 8 out of 63 patients with KFS [60]. Furthermore, researchers found out that among five new candidate genes (BAZ1B, FREM2, VANGL1, SUFU, and KMT2D), the variants in BAZ1B had the strongest association with KFS [61]. On the other hand, a study by Li et al. revealed 11 pathogenic missense variants in eight KFS patients, including COL6A1, COL6A2, CDAN1, CHRNG, FLNB, GLI3, MYH3, POR, and TNXB, but none within KFS-related genes – GDF6, GDF3, MEOX1, and MYO18B [62].
Thoracic/lumbar spine
Congenital scoliosis
Congenital scoliosis (CS) is a spinal deformity resulting from the abnormal shape of vertebrae (hemivertebrae, butterfly vertebrae, wedge vertebrae), segmentation failure, or a combination of both [63, 64]. Hemivertebrae are the most common cause of CS. Many CS patients also have defects in other organs, particularly in the heart and the genitourinary system [65]. This condition is estimated to occur in 1 per 2000 live births and manifests as a lateral curvature of the spine (Cobb angle) exceeding 10 degrees. The indication for CS surgery depends on the degree of CS at the time of diagnosis and the disease progression.
The genetic basis of CS is only partially explained. Approximately 10% of the patients harbor heterozygous TBX6 loss-of-function variants or a deletion copy-number variant (CNV) within chromosome 16p11.2, including the TBX6 gene [66,67,68]. Wu et al. reported that CS patients with TBX6 loss-of-function variants carry an additional hypomorphic variant on the second TBX6 allele, which is a specific haplotype corresponding to one of the following common SNVs: rs2289292, rs3809624, and rs3809627 [68]. In two subsequent studies, researchers found these variations in TBX6 in about 9.6% and 7.14% of CS patients, respectively [69, 70]. TBX6 belongs to the T-box family and encodes a transcription factor controlling presomitic mesoderm segmentation and differentiation during development [71, 72]. In 2019, Liu et al. defined TBX6-associated congenital scoliosis (TACS) as a unique clinically recognizable subtype of CS [73, 74].
In addition to 16p11.2 deletion, involving the TBX6 gene, a recent study revealed novel CNVs carried by CS individuals [75]. Lai et al. identified recurrent CNVs encompassing three scoliosis-related genes, including NOTCH2, DSCAM, and SNTG1 and four genes (DHX40, NBPF20, RASA2, and MYSM1) possibly linked to skeletal abnormalities [75].
New CS candidate genes have also been proposed, i.e., TBXT, FBN1, PTK7, SOX9, and Dstyk [76,77,78,79,80,81]. Similarly to TBX6, TBXT (also known as Brachyury or T), a member of the T‐box family, is highly expressed in the notochord and is involved in mesoderm formation and axial elongation [82]. According to some studies, FBN1 may trigger CS by upregulating TGF-β signaling, which is essential for skeletal development [78, 83]. The third candidate gene, PTK7, plays a crucial role in canonical and non-canonical Wnt signaling, whereas the fourth CS candidate gene, SOX9, is involved in chondrocyte differentiation, notochord maintenance, and demarcation of intervertebral disc compartments [84,85,86]. Finally, variants of Dstyk may result in CS-like VMs in zebrafish due to disrupting the formation of the notochord vacuole through the mTORC1/TFEB pathway [81].
Spondylocostal dysostosis
Another congenital spinal disorder, spondylocostal dysostosis (SCD), shares a similar phenotype with CS. SCD is a rare genetic defect characterized by malformations of the ribs and vertebrae (hemivertebrae, butterfly vertebrae, fusion, block, or mixed abnormalities). SCD patients often present with a short neck, short trunk, and scoliosis [17, 87]. To date, SCD has been classified into seven subtypes based on their phenotypes and disease genes: SCD1 with pathogenic variants in DLL3, SCD2 with pathogenic variants in MESP2, SCD3 with pathogenic variants in LFNG, SCD4 with pathogenic variants in HES7, SCD5 with pathogenic variants in TBX6, SCD6 with pathogenic variants in RIPPLY2, and SCD7 with pathogenic variants in DLL1. All these disorders are inherited in an autosomal recessive manner. However, SCD5, in addition to autosomal recessive transmission may also present autosomal dominant inheritance pattern [68, 88,89,90,91,92]. It has been shown that SCD may co-occur with additional cervical and sacral spine malformations or costovertebral malformations. In such phenotypes, pathogenic variants are identified in LFNG or DRMT2, respectively [91, 93, 94]. The results of a functional analysis of the missense LFNG variant (p.Phe188Leu) showed no difference in protein expression between the mutant and wild-type mice [91]. In contrast, the Dmrt2 knock-out mice displayed a similar phenotype to a human neonate with SCD, indicating that pathogenic variants in DMRT2 may be related to a new subtype of SCD [93].
Lumbar spine
Developmental spinal stenosis
Developmental spinal stenosis (DSS), also known as congenital lumbar spinal stenosis, is likely caused by fetal and postnatal abnormal development of the posterior spinal elements [95, 96]. The most common clinical features of DSS include a narrow spinal canal, enlarged lamina, and short pedicles [97]. In some cases, the lumbar vertebrae give the spinal canal a trefoil appearance that leads to lumbar and sacral nerve compression [98]. Genetic predisposition to DSS differs between the upper (L1-L4) and the lower (L5-S1) lumbar spine levels. Genome-Wide Association Study showed that L4 and L5 vertebrae DSS-associated SNVs were located within the ZNF704, and DCC genes, respectively. In addition, three candidate genes, i.e., LRP5, COX2, and VDR can contribute to DSS [99]. DSS is often associated with achondroplasia, a type of skeletal dysplasia resulting from specific FGFR3 activating alterations. Such a complication leads to neurologic symptoms in affected individuals and thus requires surgical interventions [100,101,102]. Sporadically, congenital thoracolumbar stenosis is also noted in alkaptonuria, as described recently [103].
Sacral spine
Sacral agenesis
Sacral agenesis is a congenital absence of the entire sacrum. The classic form of sacral agenesis is autosomal dominant Currarino syndrome (MIM: 176450), in which partial agenesis, i.e., hemisacrum, within S2-S5 vertebrae occurs. In addition, patients present with anorectal malformations, a presacral mass (anterior meningocele, enteric cyst, or presacral teratoma), and urogenital anomalies [104]. Over twenty years ago, a causative gene for this syndrome was found, i.e., MNX1, also known as HLXB9 [105]. Recently, whole exome sequencing studies of 6 patients with Currarino syndrome revealed 7 variants that might be linked to the disorder, i.e., a de novo variant in ETV3L (p.Val126Ile), a de novo variant in NCAPD3, a variant in ARID5A (p.Arg55Leu), a missense variant in CDH2 (p.Arg151Ser), a variant in ITIH2 (p.Ile541Ilefs12), a variant in HOXB4 (p.Lys16Asn), and variant in TLE4 (p.Ser650Leu) [106, 107].
The role of environmental factors and epigenetics in congenital spinal deformities
The role of environmental factors
Neural tube defects
Neural tube defects (NTDs) represent a group of congenital anomalies characterized by incomplete neural tube closure during embryonic development. The defects result from a complex interplay of genetic and environmental factors. NTDs encompass a heterogeneous spectrum of congenital anomalies, including anencephaly, spina bifida (SB), encephalocele, and craniorachischisis [108]. Genetic factors play a key role in the etiology of NTDs, with intragenic susceptibility variants identified in multiple genes, including CCL2 (MIM: 158105), FUZ (MIM: 610622), VANGL1 (MIM: 610132), VANGL2 (MIM: 600533), and TBXT (MIM: 601397) [109,110,111,112,113]. The pathogenic variant in the CCL2 gene predisposes to the development of SB. Notably, the CCL2 gene regulates the export level of monocyte chemotactic protein-1 following treatment with interleukin-1-β in vitro [114]. Research has shown that maternal hyperthermia in the first trimester of pregnancy is associated with a twofold increase in the incidence of SB [115]. Hence, inflammation and increased body temperature, mediated by chemokines, may be contributing factors in the pathogenesis of SB. Jensen et al. linked the CCL2A(-2518)G promoter polymorphism with SB, as the allele could attenuate the response to infection [110]. Another predisposing gene in NTDs, expressed in the emerging neural tube, is the FUZ gene. Seo et al. found 5 missense heterozygous pathogenic substitutions in FUZ in an Italian cohort, i.e., p.Pro39Ser, p.Asp354Tyr, p.Arg404Glu, p.Gly140Glu, and p.Ser142Thr. The variants disrupt primary cilia formation and affect directional cell movement, which are crucial processes in developing the spinal neural tube [113]. Furthermore, several heterozygous missense pathogenic variants within the VANGL1 and VANGL2 genes have been associated with a subset of human NTDs. Merello et al. suggested a correlation between three heterozygous missense variants of VANGL1, p.Ala187Val, p.Asp389His, and p.Arg517His, and the occurrence of NTDs [116]. Interestingly, another research group has indicated a predisposition of pathogenic variants in VANGL2 (p.Ser84Phe, p.Arg353Cys, and p.Phe437Ser) to an increased risk of cranial NTDs in human fetuses [109]. Finally, researchers have identified a pathogenic variant in the TBXT gene, TIVS7-2, in individuals suffering from meningomyelocele. The variant has been concomitantly correlated with elevated predisposition to SB [117]. Numerous studies have also identified other risk-candidate genes such as AMOT, ARHGAP36, CELSR1, COL15A1, DACT1, DISP2, DLC1, DTX1, FREM2, FZD6, GPR50, GRHL3, ITGB1, MTHFR, MYO1E, NKRF, PAX3, PRICKLE1, PTK7, RXRγ, SCRIB, SHROOM3, and TKTL1 [118,119,120,121,122,123,124,125,126]. Despite identifying susceptibility variants responsible for NTDs, recent studies have revealed a significant role of environmental factors in the etiology of NTDs. A prospective study has demonstrated that fever during the first month of pregnancy increases the risk of NTDs [115]. Furthermore, a systematic review and meta-analysis conducted in 2005 confirmed that hyperthermia in early pregnancy is a risk factor for NTDs [127]. Other significant factors contributing to the development of NTDs are maternal diabetes and obesity. Specifically, teratogenic implications of hyperglycemia and hyperinsulinemia increase cellular apoptosis within the developing embryonic neural plate. Women diagnosed with diabetes manifest a notable 2- to tenfold escalation in the risk of NTDs, whereas women affected by obesity demonstrate a 1.5- to 3.5-fold increase, with the severity of risk correlating with maternal body mass index [128,129,130]. Thirdly, inadequate maternal nutritional status during pregnancy, i.e., deficiencies in folate, zinc, and B12, is a factor in the increased risk of NTDs. Notably, research strongly supports the association between folate deficiency and NTDs [131, 132]. The recommended folic acid dosage for women with a previous NTD-complicated pregnancy is 4 mg/day [133]. Among antiepileptic drugs, valproic acid is the most widely recognized teratogenic drug associated with NTDs. The risk of NTDs related to valproate exposure appears to be dose-dependent, necessitating cautionary measures to avoid its use or to limit the dosage [134]. Finally, alcohol and caffeine consumption and maternal exposure to passive smoking are potential risk factors, however, more studies are needed [135,136,137].
Caudal dysgenesis syndrome
Caudal dysgenesis syndrome (CDS; MIM: 600145), also classified as neural tube defect, is a form of sacral agenesis, in which various heterogeneous constellations of symptoms are observed. The CDS phenotype encompasses defects of caudal derivatives, such as anomalies affecting the caudal spine, the spinal cord, the hindgut, the urogenital system, and sporadically the lower extremities (sirenomelia) [138, 139]. Amongst CDS causes, one may list maternal insulin-dependent diabetes during pregnancy (detected in 15–25% of mothers who gave birth to affected children) and pathogenic variants within the VANGL1 or CELSR1 genes [112, 140, 141]. Furthermore, the influence of exogenous substances on the fetus, including retinoic acid and insulin, is also a potential risk factor [142].
The role of epigenetics
Epigenetic factors represent another potential mechanism that may be involved in the pathogenesis of VMs. The epigenetic genes involved in the etiology of vertebral defects are summarized in Table 4. Recent studies showed that aberrant DNA methylation might be linked with the pathogenesis of CS. As compared with healthy individuals, CS patients showed hypermethylation in KAT6B, TNS3, IGHG1, IGHM, IGHG3, RNF213, and GSE1, and hypomethylation in SORCS2, COL5A1, GRID1, RGS3, and ROBO2 [143,144,145]. Moreover, DNA methylation is a critical mechanism in the process of genomic imprinting, an epigenetic mode of inheritance in which genes are expressed exclusively from one parental chromosome, depending on their parental origin. These epigenetic modifications during gametogenesis have been implicated in the etiology of several congenital imprinting disorders (IDs), which present with different clinical features. Silver–Russell syndrome (SRS) and Beckwith–Wiedemann syndrome (BWS) represent examples of imprinting disorders associated with VMs [146]. SRS is characterized by growth retardation, macrocephaly at birth, and dysmorphic facial features (triangular face, prominent forehead). Symptoms associated with VMs include scoliosis, kyphosis, kypho-lordosis, lumbar hypomobility, lumbar hypolordosis with lumbar hypomobility, and abnormally high lumbar vertebrae [147,148,149]. Hypomethylation at the imprinting control region 1 (ICR1) located on chromosome 11p15.5, resulting from the loss of paternal methylation, constitutes a primary cause of SRS. This epigenetic aberration affects the expression of growth-regulatory genes, i.e., IGF2 and H19. Furthermore, patients with SRS carry maternal uniparental disomy of chromosomes 7, 14, 16, and 20, aberrant methylation of 14q32.2, maternal gain-of-function variants in CDKN1C, and paternal loss-of-function variants in IGF2 [150]. BWS manifests clinical features, including macrosomia, macroglossia, abdominal wall defects, and elevated risk for embryonal tumors [151]. Additionally, a recent study identified painful scoliosis with lateralized overgrowth as one of the consequences of BWS [152]. Analogously to SRS, most BWS cases exhibit DNA methylation alterations at the chromosomal locus 11p15.5-11p15.4. In contrast to SRS, BWS is typified by hypermethylation at the ICR1 and hypomethylation at the ICR2, which result in dysregulation of three imprinted genes shared with SRS, namely IGF2, H19, and CDKN1C, and the KCNQ1OT gene [151].
Future perspectives and conclusions
Studies regarding the genetic background of VMs are ongoing worldwide. However, their main limitations remain the rare occurrence of VMs, clinical heterogeneity of these defects, and the economic barrier that all impede performing large cohort research screening using advanced technologies, including whole-genome sequencing, transcriptome profiling via RNA-seq, third-generation sequencing, single-cell sequencing, and other more sophisticated functional studies.
Given the phenotypic heterogeneity of VMs, the application of exact classification systems appears critical for clinical recognition and, next, molecular background research. Studies of clinically homogenous groups of VMs patients are highly needed for identifying the causative genetic lesions underlying vertebral defects and closing the knowledge gap in this area. Simultaneously, exploring the potential contribution of epigenetic factors to the development of vertebral disorders is an interesting avenue for future research. While studies into the epigenetics of CS and IDs have yielded promising results in recent years, there is a knowledge gap in the potential role of epigenetics in other described syndromes. Recent studies on rare diseases such as chromatinopathies and Kabuki syndrome have underscored the crucial role of genome-wide DNA methylation analysis in establishing definitive molecular diagnoses, particularly in the cases where initial genetic screenings yield negative results. Simultaneously, integrating genotype, phenotype, and epigenetic factors has been proposed as a promising approach to unraveling the molecular basis of rare diseases [153, 154]. So far, only one promising study has explored the global genome-wide methylation profile in CS patients, albeit with a small sample size of n = 4 [145]. To expand the scope of methylation investigations in CS and initiate studies in other described VMs disorders, novel methods such as comprehensive whole-genome bisulfite sequencing and methylome arrays covering approximately 850,000 loci could be used. We assume that integrative analyses incorporating multi-omics data, encompassing (epi-)genomic, transcriptomic, and chromatin studies, hold significant promise in providing a comprehensive molecular picture of VMs. Furthermore, to our knowledge, there are no cis-regulatory variants in the non-coding DNA described so far in the medical literature that are causative for VMs. Thus, pathogenic variants located in the regulatory elements of the genes involved in embryonic vertebral development represent another putative disease mechanism. Such causative changes can be identified via array comparative genomic hybridization and whole-genome sequencing analyses.
Importantly, the complexity of VMs etiology cannot be excluded. The involvement of external environmental causes such as maternal drug intake, maternal diseases during pregnancy, or other yet unidentified environmental factors affecting the developing fetus or possibly parents before pregnancy, should also be considered. In VMs disorders influenced by environmental factors, the range of structural abnormalities can differ significantly based on the timing of exposure to these factors during embryonic development and the intensity of their impact. As a result, the affected individuals may display a variety of anomalies, with differences in the type and severity of malformations. Conversely, genetic disorders show a more consistent pattern of inheritance and recurrence within families.
In conclusion, the described heterogeneity of VMs highlights the need for interdisciplinary research approaches that integrate genetics, environmental factors, and epigenetic mechanisms.
Availability of data and materials
Not applicable.
Abbreviations
- VMs:
-
Vertebral malformations
- FGF:
-
Fibroblast growth factor
- HG:
-
Hedgehog
- RA:
-
Retinoic acid
- TGF-β:
-
Transforming growth factor β
- BMP:
-
Bone morphogenic protein
- HV:
-
Hemivertebra
- BV:
-
Butterfly vertebra
- KFS:
-
Klippel–Feil syndrome
- OMIM:
-
Online Mendelian Inheritance in Man
- CS:
-
Congenital scoliosis
- CNV:
-
Copy-number variant
- TACS:
-
TBX6-Associated congenital scoliosis
- SCD:
-
Spondylocostal dysostosis
- DSS:
-
Developmental spinal stenosis
- NTDs:
-
Neural tube defects
- SB:
-
Spina bifida
- CDS:
-
Caudal dysgenesis syndrome
- IDs:
-
Imprinting disorders
- SRS:
-
Silver–Russell syndrome
- BWS:
-
Beckwith–Wiedemann syndrome
- ICR1:
-
Imprinting control region 1
- ICR2:
-
Imprinting control region 2
References
Christ B, Ordahl CP. Early stages of chick somite development. Anat Embryol (Berl). 1995;191(5):381–96. https://doi.org/10.1007/BF00304424.
Christ B, Scaal M. Formation and differentiation of avian somite derivatives. Adv Exp Med Biol. 2008;638:1–41. https://doi.org/10.1007/978-0-387-09606-3_1.
Furdock R, Brouillet K, Luhmann SJ. Organ system anomalies associated with congenital scoliosis: a retrospective study of 305 patients. J Pediatr Orthop. 2019;39(3):190–4. https://doi.org/10.1097/BPO.0000000000001279.
Corallo D, Trapani V, Bonaldo P. The notochord: structure and functions. Cell Mol Life Sci. 2015;72(16):2989–3008. https://doi.org/10.1007/s00018-015-1897-z.
Dias MS. Normal and abnormal development of the spine. Neurosurg Clin N Am. 2007;18(3):415–29. https://doi.org/10.1016/j.nec.2007.05.003.
Lochnes D. The Cdx1 homeodomain protein: an integrator of posterior signaling in the mouse. BioEssays. 2003;25(10):971–80. https://doi.org/10.1002/bies.10340.
Pilon N, Oh K, Jean-Rene S, Savory J, Lochnes D. Wnt signaling is a key mediator of Cdx1 expression in vivo. Development. 2007;134(12):2315–23. https://doi.org/10.1242/dev.001206.
Wu M, Chen G, Yp L. TGF-β and BMP signaling in osteoblast, skeletal development, and bone formation, homeostasis and disease. Bone. 2016;4:16009. https://doi.org/10.1038/boneres.2016.9.
Eckalbar WL, Fisher RE, Rawls A, Kusumi K. Scoliosis and segmentation defects of the vertebrae. Wiley Interdiscip Rev Dev Biol. 2012;1(3):401–23. https://doi.org/10.1002/wdev.34.
Erol B, Tracy M, Dormans J, Zackai E, Maisenbacher M, O’Brien M, et al. Congenital scoliosis and vertebral malformtions: characterization of segmental defects for genetic analysis. J Pediatr Othop. 2004;24(6):674–82.
Giampietro PF, Raggio CL, Blank RD, McCarty C, Broeckel U, Pickart MA. Clinical, genetic and environmental factors associated with congenital vertebral malformations. Mol Syndromol. 2013;4(1–2):94–105. https://doi.org/10.1159/000345329.
Brand M. Examination of the newborn with congenital scoliosis: focus on the physical. Adv Neonatal Care. 2008;8(5):265–73. https://doi.org/10.1097/01.ANC.0000338016.03040.6b.
Giampietro PF, Dunwoodie SL, Kusumi K, Pourquié O, Tassy O, Offiah AC, et al. Progress in the understanding of the genetic etiology of vertebral segmentation disorders in humans. Ann N Y Acad Sci. 2009;1151:38–67. https://doi.org/10.1111/j.1749-6632.2008.03452.x.
Özek MM, Cinalli G, Maixner WJ. Vertebral Anomalies and Spinal Malformations in Myelomeningocele. The Spina Bifida. 2008; 185–196.
Offiah A, Alman B, Cornier AS, Giampietro PF, Tassy O, Wade A, et al. Pilot assessment of a radiologic classification system for segmentation defects of the vertebrae. Am J Med Genet Part A. 2010;152A(6):1357–71. https://doi.org/10.1002/ajmg.a.33361.
Chen Y, Liu Z, Chen J, Zuo Y, Liu S, Chen W, et al. The genetic landscape and clinical implications of vertebral anomalies in VACTERL association. J Med Genet. 2016;53(7):431–7. https://doi.org/10.1136/jmedgenet-2015-103554.
Turnpenny PD, Alman B, Cornier AS, Giampietro PF, Offiah A, Tassy O, et al. Abnormal vertebral segmentation and the notch signaling pathway in man. Dev Dyn. 2007;236(6):1456–74. https://doi.org/10.1002/dvdy.21182.
Giampietro PF, Raggio CL, Reynolds CE, Shukla SK, McPherson E, Ghebranious N, et al. An analysis of PAX1 in the development of vertebral malformations. Clin Genet. 2005;68(5):448–53. https://doi.org/10.1111/j.1399-0004.2005.00520.x.
Chipman JG, Deuser WE, Beilman GJ. Early surgery for thoracolumbar spine injuries decreases complications. J Trauma. 2004;56(1):52–7. https://doi.org/10.1097/01.TA.0000108630.34225.85.
Brokinkel B, Wiebe K, Hesselmann V, Filler TJ, Ewelt C, Müller-Hofstede C, et al. Surgical treatment in a patient with Klippel–Feil syndrome and anterior cervical meningomyelocele: a case report and review of literature. Eur Spine J. 2013;22(Suppl 3):517–20. https://doi.org/10.1007/s00586-013-2769-6.
Oskouian RJ Jr, Sansur CA, Shaffrey CI. Congenital abnormalities of the thoracic and lumbar spine. Neurosurg Clin N Am. 2007;18(3):479–98. https://doi.org/10.1016/j.nec.2007.04.004.
Groves M, Vivas A, Samdani A. Scoliosis and other congenital vertebral anomalies. Textbook of Pediatric Neurosurgery. 2020:2623–2633
Weisz B, Achiron R, Schindler A, Eisenberg VH, Lipitz S, Zalel Y. Prenatal sonographic diagnosis of hemivertebra. J Ultrasound Med. 2004;23(6):853–7. https://doi.org/10.7863/jum.2004.23.6.853.
Powel JE, Sham CE, Spiliopoulos M, Ferreira CR, Rosenthal E, Sinkovskaya ES, et al. Genetics of non-isolated hemivertebra: a systematic review of fetal, neonatal, and infant cases. Clin Genet. 2022;102(4):262–87. https://doi.org/10.1111/cge.14188.
Johal J, Loukas M, Fisahn C, Chapman JR, Oskouian RJ, Tubbs RS. Hemivertebrae: a comprehensive review of embryology, imaging, classification, and management. Child’s Nerv Syst. 2016;32(11):2105–9. https://doi.org/10.1007/s00381-016-3195-y.
Tsou P, Yau A, Hodgson A. Embryogenesis and prenatal development of congenital vertebral anomalies and their classification. Clin Orthop Relat Res. 1980;152:211–31.
Nasca R, Stelling F, Steel H. Progression of congenital scoliosis due to hemivertebrae and hemivertebrae with bars. J Bone Jt Surg Am. 1975;57(4):456–66.
Grimes CK, Blackstone J. Associations and Outcomes. Ultrasound. 2008;27(7):1023–7. https://doi.org/10.7863/jum.2008.27.7.1023.
Ekim A. Butterfly vertebra anomaly: A case report. J Back Musculoskelet Rehabil. 2010;23(3):161–4. https://doi.org/10.3233/BMR-2010-0262.
Stanley JK, Owen R, Koff S. Congenital sacral anomalies. J Bone Jt Surg - Ser B. 1979;61B(4):401–9. https://doi.org/10.1302/0301-620X.61B4.500747.
Cho HL, Kim JS, Paeng SS, Lee SH. Butterfly vertebra with lumbar intervertebral disc herniation: case report. J Neurosurg Spine. 2011;15(5):567–70. https://doi.org/10.3171/2011.6.
Alagille D, Estrada A, Hadchouel M, Gautier M, Odièvre M, Dommergues JP. Syndromic paucity of interlobular bile ducts (Alagille syndrome or arteriohepatic dysplasia): review of 80 cases. J Pediatr. 1987;110(2):195–200. https://doi.org/10.1016/s0022-3476(87)80153-1.
Anderson PJ, Hall CM, Evans RD, Jones BM, Harkness W, Hayward RD. Cervical spine in Pfeiffer’s syndrome. J Craniofac Surg. 1996;7(4):275–9. https://doi.org/10.1097/00001665-199607000-00005.
Anderson PJ, Hall C, Evans RD, Harkness WJ, Hayward RD, Jones BM. The cervical spine in Crouzon syndrome. Spine (Phila Pa 1976). 1997;22(4):402–5. https://doi.org/10.1097/00007632-199702150-00009.
Lawson ME, Share J, Benacerraf B, Krauss CM. Jarcho-Levin syndrome: prenatal diagnosis, perinatal care, and follow-up of siblings. J Perinatol. 1997;17(5):407–9.
Wang F, Dong Z, Li YP, Miao DC, Wang LF, Shen Y. Wedge-shaped vertebrae is a risk factor for symptomatic upper lumbar disc herniation. J Orthop Surg Res. 2019;14(1):265. https://doi.org/10.1186/s13018-019-1314-7.
Oi S. Malformations of the vertebrae. In: Raimondi ACM, Di Rocco C (eds) Principles of pediatric neurosurgery. 1989; pp 1–18
Rush BR. Developmental vertebral abnormalities. In: Auer JA, Stick JA, editors. Equine Surgery. 4th ed. St Louis: Elsevier; 2012. p. 693–9.
Jung C, Asbach P, Niehues SM. Are congenital cervical block vertebrae a risk factor for adjacent segment disease? a retrospective cross-sectional CT and MR imaging study. Diagnostics (Basel). 2021;12(1):90. https://doi.org/10.3390/diagnostics12010090.
Al Dhaheri N, Wu N, Zhao S, Wu Z, Blank RD, Zhang J, et al. KIAA1217: a novel candidate gene associated with isolated and syndromic vertebral malformations. Am J Med Genet A. 2020;182(7):1664–72. https://doi.org/10.1002/ajmg.a.61607.
Klippel M, Feil A. Un cas d’absence des vertebres cervicales avec cage thoracique remontant jusqu’a la base du crane. Nouv Icon Salpet. 1912;25:223–50.
Gruber J, Saleh A, Bakhsh W, Rubery PT, Mesfin A. The Prevalence of Klippel–Feil syndrome: a computed tomography-based analysis of 2917 patients. Spine Deform. 2018;6(4):448–53. https://doi.org/10.1016/j.jspd.2017.12.002.
Krakow D. Spinal abnormalities and Klippel–Feil syndrome. Second Edi. Obstetric Imaging: Fetal Diagnosis and Care. 2nd Edition. Elsevier Inc; 2017;295–297
Nouri A, Tetreault L, Zamorano JJ, Mohanty CB, Fehlings MG. Prevalence of Klippel–Feil syndrome in a surgical series of patients with cervical spondylotic myelopathy: analysis of the prospective, multicenter AOSpine North America study. Glob Spine J. 2015;5(4):294–9. https://doi.org/10.1055/s-0035-1546817.
Jones K, Jones M, del Campo M. Recognizable patterns of human malformations. 7th ed. Elsievier; 2013. p. 796–830.
Hensinger R, Lang J, MacEwen G. Klippel–Feil syndrome; a costellation of associated anomalies. J Bone Jt Surg Am. 1974;56(6):1246–53.
Samartzis D, Herman J, Lubicky JP, Shen FH. Classification of congenitally fused cervical patterns in Klippel-Feil patients: epidemiology and role in the development of cervical spine-related symptoms. Spine (Phila Pa 1976). 2006;31(21):E798-804. https://doi.org/10.1097/01.brs.0000239222.36505.46.
Xue X, Shen J, Zhang J, Tian Y, Zhao H, Wang Y, et al. Klippel-Feil syndrome in congenital scoliosis. Spine (Phila Pa 1976). 2014;39(23):E1353–8. https://doi.org/10.1097/BRS.0000000000000587.
Clarke RA, Singh S, McKenzie H, Kearsley JH, Yip MY. Familial Klippel–Feil syndrome and paracentric inversion inv(8)(q22.2q23.3). Am J Hum Genet. 1995;57(6):1364–70.
Fukushima Y, Ohashi H, Wakui K, Nishimoto H, Sato M, Aihara T. De novo apparently balanced reciprocal translocation between 5q11.2 and 17q23 associated with Klippel–Feil anomaly and type A1 brachydactyly. Am J Med Genet. 1995;57(3):447–9. https://doi.org/10.1002/ajmg.1320570317.
Goto M, Nishimua G, Nagai T, Yamazawa K, Ogata T. Familial Klippel–Feil anomaly and translocation. Am J Med Gen Part A. 2006;140(9):1013–5. https://doi.org/10.1002/ajmg.a.31198.
Papagrigorakis MJ, Synodinos PN, Daliouris CP, Metaxotou C. De novo inv(2)(p12q34) associated with Klippel–Feil anomaly and hypodontia. Eur J Pediatr. 2003;162(9):594–7. https://doi.org/10.1007/s00431-003-1262-3.
Bayrakli F, Guclu B, Yakicier C, Balaban H, Kartal U, Erguner B, et al. Mutation in MEOX1 gene causes a recessive Klippel–Feil syndrome subtype. BMC Genet. 2013;14:1. https://doi.org/10.1186/1471-2156-14-95.
Mohamed JY, Faqeih E, Alsiddiky A, Alshammari MJ, Ibrahim NA, Alkuraya FS. Mutations in MEOX1, encoding mesenchyme homeobox 1, cause Klippel–Feil anomaly. Am J Hum Genet. 2013;92(1):157–61. https://doi.org/10.1016/j.ajhg.2012.11.016.
Schieffer KM, Varga E, Miller KE, Agarwal V, Koboldt DC, Brennan P, et al. Expanding the clinical history associated with syndromic Klippel–Feil: a unique case of comorbidity with medulloblastoma. Eur J Med Genet. 2019;62(8): 103701. https://doi.org/10.1016/j.ejmg.2019.103701.
Chacón-Camacho O, Camarillo-Blancarte L, Pelaez-González H, Mendiola J, Zenteno JC. Klippel–Feil syndrome associated with situs inversus: description of a new case and exclusion of GDF1, GDF3 and GDF6 as causal genes. Eur J Med Genet. 2012;55(6–7):414–7. https://doi.org/10.1016/j.ejmg.2012.03.007.
Alazami AM, Kentab AY, Faqeih E, Mohamed JY, Alkhalidi H, Hijazi H, et al. A novel syndrome of Klippel–Feil anomaly, myopathy, and characteristic facies is linked to a null mutation in MYO18B. J Med Genet. 2015;52(6):400–4. https://doi.org/10.1136/jmedgenet-2014-102964.
Karaca E, Yuregir OO, Bozdogan ST, Aslan H, Pehlivan D, Jhangiani SN, et al. Rare variants in the notch signaling pathway describe a novel type of autosomal recessive Klippel–Feil syndrome. Am J Med Genet Part A. 2015;167A(11):2795–9. https://doi.org/10.1002/ajmg.a.37263.
Erol B, Tracy MR, Dormans JP, Zackai EH, Maisenbacher MK, Brien MLO, Turnpenny PD, et al. Congenital scoliosis and vertebral malformations characterization of segmental defects for genetic analysis. J Pediatr Orthopaed. 2004;24(6):674–82.
McGaughran JM, Oates A, Donnai D, Read AP, Tassabehji M. Mutations in PAX1 may be associated with Klipel-Feil syndrome. Eur J Hum Genet. 2003;11(6):468–74. https://doi.org/10.1038/sj.ejhg.5200987.
Li Z, Zhao S, Cai S, Zhang Y, Wang L, Niu Y, et al. The mutational burden and oligogenic inheritance in Klippel–Feil syndrome. BMC Musculoskelet Disord. 2020;21(1):220. https://doi.org/10.1186/s12891-020-03229-x.
Li Z, Geng M, Zhao S, Wu Z, Zhang J, Wu N, et al. Clinical characteristics and genetic analysis of Klippel–Feil syndrome. Chinese. 2021;43(1):25–31. https://doi.org/10.3881/j.issn.1000-503X.12629.
Hedequist D, Emans J. Congenital scoliosis: a review and update. J Pediatr Orthop. 2007;27(1):106–16. https://doi.org/10.1097/BPO.0b013e31802b4993.
McMaster. The natural history of congenital scoliosis: a study of two hundred and fifty-one patients. J Bone Jt Surg Am. 1982;64(8):1128–47.
Kose N, Campbell RM. Congenital scoliosis. Med Sci Monit. 2004;10(5):104–10.
Al-Kateb H, Khanna G, Filges I, Hauser N, Grange DK, Shen J, et al. Scoliosis and vertebral anomalies: Additional abnormal phenotypes associated with chromosome 16p11.2 rearrangement. Am J Med Genet Part A. 2014;164A(5):1118–26. https://doi.org/10.1002/ajmg.a.36401.
Shen Y, Chen X, Wang L, Guo J, Shen J, An Y, et al. Intra-family phenotypic heterogeneity of 16p11.2 deletion carriers in a three-generation Chinese family. Am J Med Genet Part B Neuropsychiatr Genet. 2011;156(2):225–32. https://doi.org/10.1002/ajmg.b.31147.
Wu N, Ming X, Xiao J, Wu Z, Chen X, Shinawi M, et al. TBX6 null variants and a common hypomorphic allele in congenital scoliosis. N Engl J Med. 2015;372(4):341–50. https://doi.org/10.1056/NEJMoa1406829.
Lefebvre M, Duffourd Y, Jouan T, Poe C, Jean-Marçais N, Verloes A, et al. Autosomal recessive variations of TBX6, from congenital scoliosis to spondylocostal dysostosis. Clin Genet. 2017;91(6):908–12. https://doi.org/10.1111/cge.12918.
Takeda K, Kou I, Kawakami N, Iida A, Nakajima M, Ogura Y, et al. Compound heterozygosity for null mutations and a common hypomorphic risk haplotype in TBX6 causes congenital scoliosis. Hum Mutat. 2017;38(3):317–23. https://doi.org/10.1002/humu.23168.
Papapetrou C, Putt W, Fox M, Edwards YH. The human TBX6 gene: cloning and assignment to chromosome 16p11.2. Genomics. 1999;55(2):238–41. https://doi.org/10.1006/geno.1998.5646.
White PH, Farkas DR, McFadden EE, Chapman DL. Defective somite patterning in mouse embryos with reduced levels of Tbx6. Development. 2003;130(8):1681–90. https://doi.org/10.1242/dev.00367.
Liu J, Wu N, Yang N, Takeda K, Chen W, Li W, et al. TBX6-associated congenital scoliosis (TACS) as a clinically distinguishable subtype of congenital scoliosis: further evidence supporting the compound inheritance and TBX6 gene dosage model. Genet Med. 2019;21(7):1548–58. https://doi.org/10.1038/s41436-018-0377-x.
Yang N, Wu N, Zhang L, Zhao Y, Liu J, Liang X, et al. TBX6 compound inheritance leads to congenital vertebral malformations in humans and mice. Hum Mol Genet. 2019;28(4):539–47. https://doi.org/10.1093/hmg/ddy358.
Lai W, Feng X, Yue M, Cheung PWH, Choi VNT, Song YQ, et al. Identification of copy number variants in a southern Chinese cohort of patients with congenital scoliosis. Genes (Basel). 2021;12(8):1213. https://doi.org/10.3390/genes12081213.
Feng X, Cheung JPY, Je JSH, Cheung PWH, Chen S, Yue M, et al. Genetic variants of TBX6 and TBXT identified in patients with congenital scoliosis in Southern China. J Orthop Res. 2021;39(5):971–88. https://doi.org/10.1002/jor.24805.
Hayes M, Gao X, Yu LX, Paria N, Henkelman RM, Wise CA, et al. Ptk7 mutant zebrafish models of congenital and idiopathic scoliosis implicate dysregulated Wnt signalling in disease. Nat Commun. 2014;5:1–11. https://doi.org/10.1038/ncomms5777.
Lin M, Zhao S, Liu G, Huang Y, Yu C, Zhao Y, et al. Identification of novel FBN1 variations implicated in congenital scoliosis. J Hum Genet. 2020;65(3):221–30. https://doi.org/10.1038/s10038-019-0698-x.
Su Z, Yang Y, Wang S, Zhao S, Zhao H, Li X, et al. The mutational landscape of ptk7 in congenital scoliosis and adolescent idiopathic scoliosis. Genes (Basel). 2021;12(11):1791. https://doi.org/10.3390/genes12111791.
Wu N, Wang L, Hu J, Zhao S, Liu B, Li Y, et al. A recurrent rare SOX9 variant (M469V) is associated with congenital vertebral malformations. Curr Gene Ther. 2019;19(4):242–7. https://doi.org/10.2174/1566523219666190924120307.
Sun X, Zhou Y, Zhang R, Wang Z, Xu M, Zhang D, et al. Dstyk mutation leads to congenital scoliosis-like vertebral malformations in zebrafish via dysregulated mTORC1/TFEB pathway. Nat Commun. 2020;11(1):1–17. https://doi.org/10.1038/s41467-019-14169-z.
Wilkinson D, Bhatt S, Herrmann B. Expression pattern of the mouse T gene and its role in mesorderm formation. Nature. 1990;343(6259):657–9.
Ng CM, Cheng A, Myers LA, Martinez-Murillo F, Jie C, Bedja D, et al. TGF-β-dependent pathogenesis of mitral valve prolapse in a mouse model of Marfan syndrome. J Clin Invest. 2004;114(111):1586–92. https://doi.org/10.1172/JCI22715.
Barrionuevo F, Taketo MM, Scherer G, Kispert A. Sox9 is required for notochord maintenance in mice. Dev Biol. 2006;295(1):128–40. https://doi.org/10.1016/j.ydbio.2006.03.014.
Dolor A, Sampson SL, Lazar AA, Lotz JC, Szoka FC, Fields AJ. Matrix modification for enhancing the transport properties of the human cartilage endplate to improve disc nutrition. PLoS ONE. 2019;14(4):1–18. https://doi.org/10.1371/journal.pone.0215218.
Berger H, Wodarz A, Borchers A. PTK7 faces the Wnt in development and disease. Front Dev Biol. 2017;5:31. https://doi.org/10.3389/fcell.2017.00031.
Karnes PS, Day D, Berry SA, Pierpont MEM. Jarcho-Levin syndrome: four new cases and classification of subtypes. Am J Med Genet. 1991;40(3):264–70. https://doi.org/10.1002/ajmg.1320400304.
Barhoumi T, Nashabat M, Alghanem B, Alhallaj AS, Boudjelal M, Umair M, et al. Delta Like-1 gene mutation: a novel cause of congenital vertebral malformation. Front Genet. 2019;10:534. https://doi.org/10.3389/fgene.2019.00534.
Bulman MP, Kusumi K, Frayling TM, McKeown C, Garrett C, Lander ES, et al. Mutations in the human Delta homologue, DLL3, cause axial skeletal defects in spondylocostal dysostosis. Nat Genet. 2000;24(4):438–41. https://doi.org/10.1038/74307.
McInerney-Leo AM, Sparrow DB, Harris JE, Gardiner BB, Marshall MS, O’Reilly VC, et al. Compound heterozygous mutations in RIPPLY2 associated with vertebral segmentation defects. Hum Mol Genet. 2015;24(5):1234–42. https://doi.org/10.1093/hmg/ddu534.
Sparrow DB, Chapman G, Wouters MA, Whittock NV, Ellard S, Fatkin D, et al. Mutation of the LUNATIC FRINGE gene in humans causes spondylocostal dysostosis with a severe vertebral phenotype. Am J Hum Genet. 2006;78(1):28–37. https://doi.org/10.1086/498879.
Whittock NV, Ellard S, Duncan J, de Die-Smulders CEM, Vles JSH, Turnpenny PD. Pseudodominant inheritance of spondylocostal dysostosis type 1 caused by two familial delta-like 3 mutations. Clin Genet. 2004;66(1):67–72. https://doi.org/10.1111/j.0009-9163.2004.00272.x.
Bouman A, Waisfisz Q, Admiraal J, van de Loo M, van Rijn RR, Dimitra M, et al. Homozygous DMRT2 variant associates with severe rib malformations in a newborn. Am J Med Genet Part A. 2018;176(5):1216–21. https://doi.org/10.1002/ajmg.a.38668.
Otomo N, Mizumoto S, Lu HF, Takeda K, Campos-Xavier B, Mittaz-Crettol L, et al. Identification of novel LFNG mutations in spondylocostal dysostosis. J Hum Genet. 2019;64(3):261–4. https://doi.org/10.1038/s10038-018-0548-2.
Cheung JPY, Ng KKM, Cheung PWH, Samartzis D, Cheung KMC. Radiographic indices for lumbar developmental spinal stenosis. Scoliosis Spinal Disord. 2017;12:3. https://doi.org/10.1186/s13013-017-0113-3.
Kirkaldy-Willis W, Wedge J, Yong-Hing K, Reilly J. Pathology and Pathogenesis of Lumbar Spondylosis and Stenosis. Spine (Phila Pa 1976). 1978;3(4):319–28. https://doi.org/10.1097/00007632-197812000-00004.
Lai MKL, Cheung PWH, Cheung JPY. A systematic review of developmental lumbar spinal stenosis. Eur Spine J. 2020;29(9):2173–87. https://doi.org/10.1007/s00586-020-06524-2.
Eisenstein S. The trefoil configuration of the lumbar vertebral canal: a study of South African skeletal material. J Bone Jt Surg - Ser B. 1980;62B(1):73–7. https://doi.org/10.1302/0301-620X.62B1.7351439.
Cheung JPY, Kao PYP, Sham P, Cheah KSE, Chan D, Cheung KMC, et al. Etiology of developmental spinal stenosis: a genome-wide association study. J Orthop Res. 2018;36(4):1262–8. https://doi.org/10.1002/jor.23746.
Savini R, Gargiulo G, Cervellati S, Di Silvestre M. Achondroplasia and lumbar spinal stenosis. Ital J Orthop Traumatol. 1991;17(2):199–209.
Modi H, Suh S, Song H, Yang J. Lumbar nerve root occupancy in the foramen in achondroplasia a morphometric analysis. Clin Orthop Relat Res. 2008;466:907–13. https://doi.org/10.1007/s11999-008-0142-6.
Calandrelli R, Pilato F, Massimi L, Onesimo R, D’Apolito G, Tenore L, et al. Thoracolumbar stenosis and neurological symptoms Quantitative MRI in achondroplasia. J Neuroimaging. 2022;32(5):884–93. https://doi.org/10.1111/jon.13015.
Ding H, Wang L, Feng G, Song Y, Liu L. Case report: Thoracolumbar spinal stenosis associated with alkaptonuria. Front Surg. 2023;9:1040715. https://doi.org/10.3389/fsurg.2022.1040715.
Currarino G, Coln D, Votteler T. Triad of anorectal, sacral, and presacral anomalies. AJR Am J Roentgenol. 1981;137(2):395–8. https://doi.org/10.2214/ajr.137.2.395.
Ross A, Ruiz-Perez V, Wang Y, Hagan D, Scherer S, Lynch S, et al. A homeobox gene, HLXB9, is the major locus for dominantly inherited sacral agenesis. Nat Genet. 1998;20(4):358–61. https://doi.org/10.1038/3828.
Dworschak GC, Reutter HM, Ludwig M. Currarino syndrome: a comprehensive genetic review of a rare congenital disorder. Orphanet J Rare Dis. 2021;16(1):167. https://doi.org/10.1186/s13023-021-01799-0.
Han L, Zhang Z, Wang H, Song H, Gao Q, Yan Y, et al. Novel MNX1 mutations and genotype-phenotype analysis of patients with Currarino syndrome. Orphanet J Rare Dis. 2020;15(1):155. https://doi.org/10.1186/s13023-020-01442-498.
Hassan AS, Du YL, Lee SY, Wang A, Farmer DL. Spina bifida: a review of the genetics, pathophysiology and emerging cellular therapies. J Dev Biol. 2022;10(2):22. https://doi.org/10.3390/jdb10020022.
Lei YP, Zhang T, Li H, Wu BL, Jin L, Wang HY. VANGL2 mutations in human cranial neural-tube defects. N Engl J Med. 2010;362(23):2232–5. https://doi.org/10.1056/NEJMc0910820.
Jensen LE, Etheredge AJ, Brown KS, Mitchell LE, Whitehead AS. Maternal genotype for the monocyte chemoattractant protein 1 A(-2518)G promoter polymorphism is associated with the risk of spina bifida in offspring. Am J Med Genet A. 2006;140(10):1114–8. https://doi.org/10.1002/ajmg.a.31212.
Morrison K, Papapetrou C, Attwood J, Hol F, Lynch SA, Sampath A, et al. Genetic mapping of the human homologue (T) of mouse T(Brachyury) and a search for allele association between human T and spina bifida. Hum Mol Genet. 1996;5(5):669–74. https://doi.org/10.1093/hmg/5.5.669.
Kibar Z, Torban E, McDearmid JR, Reynolds A, Berghout J, Mathieu M, et al. Mutations in VANGL1 associated with neural-tube defects. N Engl J Med. 2007;356(14):1432–7. https://doi.org/10.1056/NEJMoa060651.
Seo JH, Zilber Y, Babayeva S, Liu J, Kyriakopoulos P, De Marco P, et al. Mutations in the planar cell polarity gene, fuzzy, are associated with neural tube defects in humans. Hum Mol Genet. 2015;24(13):3893. https://doi.org/10.1093/hmg/ddv131.
Rovin BH, Lu L, Saxena R. A novel polymorphism in the MCP-1 gene regulatory region that influences MCP-1 expression. Biochem Biophys Res Commun. 1999;259(2):344–8. https://doi.org/10.1006/bbrc.1999.0796.
Chambers CD, Johnson KA, Dick LM, Felix RJ, Jones KL. Maternal fever and birth outcome: a prospective study. Teratology. 1998;58(6):251–7.
Merello E, Mascelli S, Raso A, Piatelli G, Consales A, Cama A, et al. Expanding the mutational spectrum associated to neural tube defects: literature revision and description of novel VANGL1 mutations. Birth Defects Res A Clin Mol Teratol. 2015;103(1):51–61. https://doi.org/10.1002/bdra.23305.
Shields DC, Ramsbottom D, Donoghue C, Pinjon E, Kirke PN, Molloy AM, et al. Association between historically high frequencies of neural tube defects and the human T homologue of mouse T (Brachyury). Am J Med Genet. 2000;92(3):206–11.
Lei Y, Kim SE, Chen Z, Cao X, Zhu H, Yang W, et al. Variants identified in PTK7 associated with neural tube defects. Mol Genet Genomic Med. 2019;7(4): e00584. https://doi.org/10.1002/mgg3.584.
Lemay P, De Marco P, Emond A, Spiegelman D, Dionne-Laporte A, Laurent S, et al. Rare deleterious variants in GRHL3 are associated with human spina bifida. Hum Mutat. 2017;38(6):716–24. https://doi.org/10.1002/humu.23214.
Lemay P, De Marco P, Traverso M, Merello E, Dionne-Laporte A, Spiegelman D, et al. Whole exome sequencing identifies novel predisposing genes in neural tube defects. Mol Genet Genomic Med. 2019;7(1): e00467. https://doi.org/10.1002/mgg3.467.
Lei Y, Zhu H, Duhon C, Yang W, Ross ME, Shaw GM, Finnell RH. Mutations in planar cell polarity gene SCRIB are associated with spina bifida. PLoS ONE. 2013;8(7): e69262. https://doi.org/10.1371/journal.pone.0069262.
Azzarà A, Rendeli C, Crivello AM, Brugnoletti F, Rumore R, Ausili E, et al. Identification of new candidate genes for spina bifida through exome sequencing. Childs Nerv Syst. 2021;37(8):2589–96. https://doi.org/10.1007/s00381-021-05153-4.
Lemay P, Guyot MC, Tremblay É, Dionne-Laporte A, Spiegelman D, Henrion É, et al. Loss-of-function de novo mutations play an important role in severe human neural tube defects. J Med Genet. 2015;52(7):493–7. https://doi.org/10.1136/jmedgenet-2015-103027.
Robinson A, Escuin S, Doudney K, Vekemans M, Stevenson RE, Greene ND, et al. Mutations in the planar cell polarity genes CELSR1 and SCRIB are associated with the severe neural tube defect craniorachischisis. Hum Mutat. 2012;33(2):440–7. https://doi.org/10.1002/humu.21662.
Beaumont M, Akloul L, Carré W, Quélin C, Journel H, Pasquier L, et al. Targeted panel sequencing establishes the implication of planar cell polarity pathway and involves new candidate genes in neural tube defect disorders. Hum Genet. 2019;138(4):363–74. https://doi.org/10.1007/s00439-019-01993-y.
Shi Y, Ding Y, Lei YP, Yang XY, Xie GM, Wen J, et al. Identification of novel rare mutations of DACT1 in human neural tube defects. Hum Mutat. 2012;33(10):1450–5. https://doi.org/10.1002/humu.22121.
Moretti ME, Bar-Oz B, Fried S, Koren G. Maternal hyperthermia and the risk for neural tube defects in offspring: systematic review and meta-analysis. Epidemiology. 2005;16(2):216–9. https://doi.org/10.1097/01.ede.0000152903.55579.15.
Yazdy MM, Mitchell AA, Liu S, Werler MM. Maternal dietary glycaemic intake during pregnancy and the risk of birth defects. Paediatr Perinat Epidemiol. 2011;25(4):340–6. https://doi.org/10.1111/j.1365-3016.2011.01198.x.
Hendricks KA, Nuno OM, Suarez L, Larsen R. Effects of hyperinsulinemia and obesity on risk of neural tube defects among Mexican Americans. Epidemiology. 2001;12(6):630–5. https://doi.org/10.1097/00001648-200111000-00009.
Avagliano L, Massa V, George TM, Qureshy S, Bulfamante GP, Finnell RH. Overview on neural tube defects: from development to physical characteristics. Birth Defects Res. 2019;111(19):1455–67. https://doi.org/10.1002/bdr2.1380.
Ray JG, Blom HJ. Vitamin B12 insufficiency and the risk of fetal neural tube defects. QJM. 2003;96(4):289–95. https://doi.org/10.1093/qjmed/hcg043.
Morris JK, Addor MC, Ballardini E, Barisic I, Barrachina-Bonet L, Braz P, et al. Prevention of neural tube defects in Europe: a public health failure. Front Pediatr. 2021;9: 647038. https://doi.org/10.3389/fped.2021.647038.
Arth A, Tinker S, Moore C, Canfield M, Agopian A, Reefhuis J. Supplement use and other characteristics among pregnant women with a previous pregnancy affected by a neural tube defect - United States. MMWR Morb Mortal Wkly Rep. 2015;64(1):6–9.
Meador KJ, Baker GA, Finnell RH, Kalayjian LA, Liporace JD, Loring DW, et al. In utero antiepileptic drug exposure: fetal death and malformations. Neurology. 2006;67(3):407–12. https://doi.org/10.1212/01.wnl.0000227919.81208.b2.
Suarez L, Ramadhani T, Felkner M, Canfield MA, Brender JD, Romitti PA, Sun L. Maternal smoking, passive tobacco smoke, and neural tube defects. Birth Defects Res A Clin Mol Teratol. 2011;91(1):29–33. https://doi.org/10.1002/bdra.20743.
Schmidt RJ, Romitti PA, Burns TL, Browne ML, Druschel CM, Olney RS. National birth defects prevention study. Maternal caffeine consumption and risk of neural tube defects. Birth Defects Res A Clin Mol Teratol. 2009;85(11):879–89. https://doi.org/10.1002/bdra.20624.
Grewal J, Carmichael SL, Ma C, Lammer EJ, Shaw GM. Maternal periconceptional smoking and alcohol consumption and risk for select congenital anomalies. Birth Defects Res A Clin Mol Teratol. 2008;82(7):519–26. https://doi.org/10.1002/bdra.20461.
Gardner P, Albright A. Like mother, like son: hereditary anterior sacral meningocele: case report and review of the literature. J Neurosurg. 2006;104:138–42. https://doi.org/10.3171/ped.2006.104.2.11.
Duesterhoeft S, Ernst L, Siebert J, Kapur R. Five cases of caudal regression with an aberrant abdominal umbilical artery: further support for a caudal regression-sirenomelia spectrum. Am J Med Genet. 2007;143A(24):3175–84. https://doi.org/10.1002/ajmg.a.32028.
Allache R, De Marco P, Merello E, Capra V, Kibar Z. Role of the planar cell polarity gene CELSR1 in neural tube defects and caudal agenesis. Birth Defects Res Part A - Clin Mol Teratol. 2012;94(3):176–81. https://doi.org/10.1002/bdra.23002.
Pang D. Sacral agenesis and caudal spinal cord malformations. Neurosurgery. 1993;32(5):755–79. https://doi.org/10.1227/00006123-199305000-00009.
Lee JY, Shim Y, Wang KC. Caudal agenesis : understanding the base of the wide clinical spectrum. J Korean Neurosurg Soc. 2021;64(3):380–5. https://doi.org/10.3340/jkns.2021.0025.
Wu Y, Zhang HQ, Tang M, Guo C, Liu S, Li J, et al. Abnormal TNS3 gene methylation in patients with congenital scoliosis. BMC Musculoskelet Disord. 2022;23(1):797. https://doi.org/10.1186/s12891-022-05730-x.
Wu Y, Zhang H, Tang M, Guo C, Deng A, Li J, et al. High methylation of lysine acetyltransferase 6B is associated with the Cobb angle in patients with congenital scoliosis. J Transl Med. 2020;18(1):210. https://doi.org/10.1186/s12967-020-02367-z.
Liu G, Zhao H, Yan Z, Zhao S, Niu Y, Li X, et al. Whole-genome methylation analysis reveals novel epigenetic perturbations of congenital scoliosis. Mol Ther Nucleic Acids. 2021;23:1281–7. https://doi.org/10.1016/j.omtn.2021.02.002.
Eggermann T, Perez de Nanclares G, Maher ER, Temple IK, Tümer Z, Monk D, et al. Imprinting disorders: a group of congenital disorders with overlapping patterns of molecular changes affecting imprinted loci. Clin Epigenetics. 2015;7:123. https://doi.org/10.1186/s13148-015-0143-8.
Yamaguchi KT Jr, Salem JB, Myung KS, Romero AN Jr, Skaggs DL. Spinal deformity in Russell–Silver syndrome. Spine Deform. 2015;3(1):95–7. https://doi.org/10.1016/j.jspd.2014.06.003.
Bruce S, Hannula-Jouppi K, Peltonen J, Kere J, Lipsanen-Nyman M. Clinically distinct epigenetic subgroups in Silver–Russell syndrome: the degree of H19 hypomethylation associates with phenotype severity and genital and skeletal anomalies. J Clin Endocrinol Metab. 2009;94(2):579–87. https://doi.org/10.1210/jc.2008-1805.
Nagalo K, Douamba S, Kaboré A, Turgeon J, Laberge JM, Yé D. Silver–Russell syndrome with unusual clinical features: a case report. Adv Pediat Res. 2018;5:7. https://doi.org/10.12715/apr.2018.5.7.
Higashimoto K, Watanabe H, Tanoue Y, Tonoki H, Tokutomi T, Hara S, et al. Hypomethylation of a centromeric block of ICR1 is sufficient to cause Silver–Russell syndrome. J Med Genet. 2021;58(6):422–5. https://doi.org/10.1136/jmedgenet-2020-106907.
Wang KH, Kupa J, Duffy KA, Kalish JM. Diagnosis and Management of Beckwith–Wiedemann Syndrome. Front Pediatr. 2020;7:562. https://doi.org/10.3389/fped.2019.00562.
Gazzin A, Carli D, Sirchia F, Molinatto C, Cardaropoli S, Palumbo G, Zampino G, Ferrero GB, Mussa A. Phenotype evolution and health issues of adults with Beckwith–Wiedemann syndrome. Am J Med Genet A. 2019;179(9):1691–702. https://doi.org/10.1002/ajmg.a.61301.
Kerkhof J, Squeo GM, McConkey H, Levy MA, Piemontese MR, Castori M, et al. DNA methylation episignature testing improves molecular diagnosis of Mendelian chromatinopathies. Genet Med. 2022;24(1):51–60. https://doi.org/10.1016/j.gim.2021.08.007.
Marwaha A, Costain G, Cytrynbaum C, Mendoza-Londono R, Chad L, Awamleh Z, et al. The utility of DNA methylation signatures in directing genome sequencing workflow: Kabuki syndrome and CDK13-related disorder. Am J Med Genet A. 2022;188(5):1368–75. https://doi.org/10.1002/ajmg.a.62650.
Shore EM, Xu M, Feldman GJ, Fenstermacher DA, Cho TJ, Choi IH, et al. A recurrent mutation in the BMP type I receptor ACVR1 causes inherited and sporadic fibrodysplasia ossificans progressiva. Nat Genet. 2006;38(5):525–7. https://doi.org/10.1038/ng1783.
Izumi K, Nakato R, Zhang Z, Edmondson AC, Noon S, Dulik MC, et al. Germline gain-of-function mutations in AFF4 cause a developmental syndrome functionally linking the super elongation complex and cohesin. Nat Genet. 2015;47(4):338–44. https://doi.org/10.1038/ng.3229.
Parenti G, Buttitta P, Meroni G, Franco B, Bernard L, Rizzolo MG, et al. X-linked recessive chondrodysplasia punctata due to a new point mutation of the ARSE gene. Am J Med Genet. 1997;73(2):139–43. https://doi.org/10.1002/(sici)1096-8628(19971212)73:2%3c139::aid-ajmg7%3e3.0.co;2-p.
Tompson SW, Bacino CA, Safina NP, Bober MB, Proud VK, Funari T, et al. Fibrochondrogenesis results from mutations in the COL11A1 type XI collagen gene. Am J Hum Genet. 2010;87(5):708–12. https://doi.org/10.1016/j.ajhg.2010.10.009.
Weis MA, Wilkin DJ, Kim HJ, Wilcox WR, Lachman RS, Rimoin DL, et al. Structurally abnormal type II collagen in a severe form of Kniest dysplasia caused by an exon 24 skipping mutation. J Biol Chem. 1998;273(8):4761–8. https://doi.org/10.1074/jbc.273.8.4761.
Shohat M, Lachman R, Carmi R, Bar Ziv J, Rimoin D. New form of spondyloepimetaphyseal dysplasia (SEMD) in Jewish family of Iraqi origin. Am J Med Genet. 1993;46(4):358–62. https://doi.org/10.1002/ajmg.1320460403.
Derry JM, Gormally E, Means GD, Zhao W, Meindl A, Kelley RI, et al. Mutations in a delta 8-delta 7 sterol isomerase in the tattered mouse and X-linked dominant chondrodysplasia punctata. Nat Genet. 1999;22(3):286–90. https://doi.org/10.1038/10350.
Sutton VR, Hyland JC, Phillips WA, Schlesinger AE, Brill PW. A dominantly inherited spondylometaphyseal dysplasia with “corner fractures” and congenital scoliosis. Am J Med Genet A. 2005;133A(2):209–12. https://doi.org/10.1002/ajmg.a.30567.
Cox TC, Lidral AC, McCoy JC, Liu H, Cox LL, Zhu Y, et al. Mutations in GDF11 and the extracellular antagonist, Follistatin, as a likely cause of Mendelian forms of orofacial clefting in humans. Hum Mutat. 2019;40(10):1813–25. https://doi.org/10.1002/humu.23793.
Xuan JY, Hughes-Benzie RM, MacKenzie AE. A small interstitial deletion in the GPC3 gene causes Simpson–Golabi–Behmel syndrome in a Dutch–Canadian family. J Med Genet. 1999;36(1):57–8.
Keipert JA, Fitzgerald MG, Danks DM. A new syndrome of broad terminal phalanges and facial abnormalities. Aust Paediatr J. 1973;9(1):10–3. https://doi.org/10.1111/j.1440-1754.1973.tb02215.x.
Handmaker SD, Campbell JA, Robinson LD, Chinwah O, Gorlin RJ. Dyssegmental dwarfism: a new syndrome of lethal dwarfism. Birth Defects Orig Artic Ser. 1977;13(3D):79–90.
Below JE, Earl DL, Shively KM, McMillin MJ, Smith JD, Turner EH, et al. Whole-genome analysis reveals that mutations in inositol polyphosphate phosphatase-like 1 cause opsismodysplasia. Am J Hum Genet. 2013;92(1):137–43. https://doi.org/10.1016/j.ajhg.2012.11.011.
Alagille D, Odièvre M, Gautier M, Dommergues JP. Hepatic ductular hypoplasia associated with characteristic facies, vertebral malformations, retarded physical, mental, and sexual development, and cardiac murmur. J Pediatr. 1975;86(1):63–71. https://doi.org/10.1016/s0022-3476(75)80706-2.
Cocciadiferro D, Agolini E, Digilio MC, Sinibaldi L, Castori M, Silvestri E, et al. The splice c.1815G>A variant in KIAA0586 results in a phenotype bridging short-rib-polydactyly and oral-facial-digital syndrome: a case report and literature review. Med (Baltimore). 2020;99(8):e19169. https://doi.org/10.1097/MD.0000000000019169.
Sobreira N, Modaff P, Steel G, You J, Nanda S, Hoover-Fong J, et al. An anadysplasia-like, spontaneously remitting spondylometaphyseal dysplasia secondary to lamin B receptor (LBR) gene mutations: further definition of the phenotypic heterogeneity of LBR-bone dysplasias. Am J Med Genet A. 2015;167A(1):159–63. https://doi.org/10.1002/ajmg.a.36808.
Lin J, Zhao L, Zhao S, Li S, Zhao Z, Chen Z, et al. Disruptive NADSYN1 variants implicated in congenital vertebral malformations. Genes (Basel). 2021;12(10):1615. https://doi.org/10.3390/genes12101615.
Gray MJ, Kim CA, Bertola DR, Arantes PR, Stewart H, Simpson MA, et al. Serpentine fibula polycystic kidney syndrome is part of the phenotypic spectrum of Hajdu-Cheney syndrome. Eur J Hum Genet. 2012;20(1):122–4. https://doi.org/10.1038/ejhg.2011.125.
König A, Happle R, Fink-Puches R, Soyer HP, Bornholdt D, Engel H, et al. A novel missense mutation of NSDHL in an unusual case of CHILD syndrome showing bilateral, almost symmetric involvement. J Am Acad Dermatol. 2002;46(4):594–6. https://doi.org/10.1067/mjd.2002.113680.
Lee H, Graham JM Jr, Rimoin DL, Lachman RS, Krejci P, Tompson SW, et al. Exome sequencing identifies PDE4D mutations in acrodysostosis. Am J Hum Genet. 2012;90(4):746–51. https://doi.org/10.1016/j.ajhg.2012.03.004.
White J, Beck CR, Harel T, Posey JE, Jhangiani SN, Tang S, et al. POGZ truncating alleles cause syndromic intellectual disability. Genome Med. 2016;8(1):3. https://doi.org/10.1186/s13073-015-0253-0.
Sillence DO, Kozlowski K, Rogers JG, Sprague PL, Cullity GJ, Osborn RA. Atelosteogenesis: evidence for heterogeneity. Pediatr Radiol. 1987;17(2):112–8. https://doi.org/10.1007/BF02388086.
Priya TP, Philip N, Molho-Pessach V, Busa T, Dalal A, Zlotogorski A. H syndrome: novel and recurrent mutations in SLC29A3. Br J Dermatol. 2010;162(5):1132–4. https://doi.org/10.1111/j.1365-2133.2010.09653.x.
Furuichi T, Kayserili H, Hiraoka S, Nishimura G, Ohashi H, Alanay Y, et al. Identification of loss-of-function mutations of SLC35D1 in patients with Schneckenbecken dysplasia, but not with other severe spondylodysplastic dysplasias group diseases. J Med Genet. 2009;46(8):562–8. https://doi.org/10.1136/jmg.2008.065201.
Sabourdy F, Mourey L, Le Trionnaire E, Bednarek N, Caillaud C, Chaix Y, et al. Natural disease history and characterisation of SUMF1 molecular defects in ten unrelated patients with multiple sulfatase deficiency. Orphanet J Rare Dis. 2015;10:31. https://doi.org/10.1186/s13023-015-0244-7.
Xu Y, Yu X, Huang M. A novel mutation in TNFRSF11A gene causes pediatric osteopetrosis: case report. BMC Surg. 2021;21(1):269. https://doi.org/10.1186/s12893-021-01266-4.
Krakow D, Vriens J, Camacho N, Luong P, Deixler H, Funari TL, et al. Mutations in the gene encoding the calcium-permeable ion channel TRPV4 produce spondylometaphyseal dysplasia, Kozlowski type and metatropic dysplasia. Am J Hum Genet. 2009;84(3):307–15. https://doi.org/10.1016/j.ajhg.2009.01.021.
Stelzer G, Rosen R, Plaschkes I, Zimmerman S, Twik M, et al. The GeneCards Suite: From Gene Data Mining to Disease Genome Sequence Analysis, Current Protocols in Bioinformatics. 2016;54:1.30.1–1.30.33. GeneCards – the human gene database. www.genecards.org
Ye M, Berry-Wynne KM, Asai-Coakwell M, Sundaresan P, Footz T, French CR, et al. Mutation of the bone morphogenetic protein GDF3 causes ocular and skeletal anomalies. Hum Mol Genet. 2010;19(2):287–98. https://doi.org/10.1093/hmg/ddp496.
Tassabehji M, Fang ZM, Hilton EN, McGaughran J, Zhao Z, de Bock CE, et al. Mutations in GDF6 are associated with vertebral segmentation defects in Klippel–Feil syndrome. Hum Mutat. 2008;29(8):1017–27. https://doi.org/10.1002/humu.20741.
Wei Z, Han C, Li H, He W, Zhou J, Dong H, et al. Molecular Mechanism of mesenchyme homeobox 1 in transforming growth factor β1-induced P311 gene transcription in fibrosis. Front Mol Biosci. 2020;7:59. https://doi.org/10.3389/fmolb.2020.00059.
Zhang Z, Zhu J, Huang Y, Li W, Cheng H. MYO18B promotes hepatocellular carcinoma progression by activating PI3K/AKT/mTOR signaling pathway. Diagn Pathol. 2018;13(1):85. https://doi.org/10.1186/s13000-018-0763-3.
Lalli MA, Jang J, Park JH, Wang Y, Guzman E, Zhou H, et al. Haploinsufficiency of BAZ1B contributes to Williams syndrome through transcriptional dysregulation of neurodevelopmental pathways. Hum Mol Genet. 2016;25(7):1294–306. https://doi.org/10.1093/hmg/ddw010.
Ashktorab H, Daremipouran M, Devaney J, Varma S, Rahi H, Lee E, et al. Identification of novel mutations by exome sequencing in African American colorectal cancer patients. Cancer. 2015;121(1):34–42. https://doi.org/10.1002/cncr.28922.
Mizuno K, Nakane A, Nishio H, Moritoki Y, Kamisawa H, Kurokawa S, et al. Involvement of the bone morphogenic protein/SMAD signaling pathway in the etiology of congenital anomalies of the kidney and urinary tract accompanied by cryptorchidism. BMC Urol. 2017;17(1):112. https://doi.org/10.1186/s12894-017-0300-9.
Zhao S, Zhang Y, Hallgrimsdottir S, Zuo Y, Li X, Batkovskyte D, et al. Expanding the mutation and phenotype spectrum of MYH3-associated skeletal disorders. NPJ Genom Med. 2022;7(1):11. https://doi.org/10.1038/s41525-021-00273-x.
Bethesda (MD): National Library of Medicine (US), National Center for Biotechnology Information. 2004–2023. https://www.ncbi.nlm.nih.gov/gene/. Accessed 24 June 2023
Li D, Wan Z, Li X, Duan M, Yang L, Ruan Z, et al. Alternatively spliced down syndrome cell adhesion molecule (Dscam) controls innate immunity in crab. J Biol Chem. 2019;294(44):16440–50. https://doi.org/10.1074/jbc.RA119.010247.
Chen X, Wang W, Li Y, Huo Y, Zhang H, Feng F, et al. MYSM1 inhibits human colorectal cancer tumorigenesis by activating miR-200 family members/CDH1 and blocking PI3K/AKT signaling. J Exp Clin Cancer Res. 2021;40(1):341. https://doi.org/10.1186/s13046-021-02106-2.
Li Y, Wang P, Ye D, Bai X, Zeng X, Zhao Q, et al. IGHG1 induces EMT in gastric cancer cells by regulating TGF-β/SMAD3 signaling pathway. J Cancer. 2021;12(12):3458–67. https://doi.org/10.7150/jca.56056.
Li Y, Yu M, Tan L, Xue S, Du X, Wu X, et al. Robo2 and Gen1 coregulate ureteric budding by activating the mapk/erk signaling pathway in mice. Front Med (Lausanne). 2022;8: 807898. https://doi.org/10.3389/fmed.2021.807898.
Alena Salašová. Identification of novel Wnt/PCP signaling regulators and their role in midbrain dopaminergic neuron development and Parkinson’s disease. Thesis for doctoral degree. Karolinska Institutet. 2018. https://openarchive.ki.se/xmlui/bitstream/handle/10616/46248/Thesis_Alena_Salasova.pdf?sequence=3&isAllowed=y. Accessed 2 June 2023
Sparrow DB, Sillence D, Wouters MA, Turnpenny PD, Dunwoodie SL. Two novel missense mutations in HAIRY-AND-ENHANCER-OF-SPLIT-7 in a family with spondylocostal dysostosis. Eur J Hum Genet. 2010;18(6):674–9. https://doi.org/10.1038/ejhg.2009.241.
Whittock NV, Sparrow DB, Wouters MA, Sillence D, Ellard S, Dunwoodie SL, Turnpenny PD. Mutated MESP2 causes spondylocostal dysostosis in humans. Am J Hum Genet. 2004;74(6):1249–54. https://doi.org/10.1086/421053.
Ono K, Hata K, Nakamura E, Ishihara S, Kobayashi S, Nakanishi M, et al. Dmrt2 promotes transition of endochondral bone formation by linking Sox9 and Runx2. Commun Biol. 2021;4(1):326. https://doi.org/10.1038/s42003-021-01848-1.
Yang WT, Lewis MT, Hess K, Wong H, Tsimelzon A, Karadag N, et al. Decreased 741 TGFbeta signaling and increased COX2 expression in high risk women with increased 742 mammographic breast density. Breast Cancer Res Treat. 2010;119(2):305–14.
Cheng Y, Pan Y, Pan Y, Wang O. MNX1-AS1 is a functional oncogene that induces EMT and activates the AKT/mTOR pathway and MNX1 in breast cancer. Cancer Manag Res. 2019;11:803–12. https://doi.org/10.2147/CMAR.S188007.
Yang X, Pan Q, Lu Y, Jiang X, Zhang S, Wu J. MNX1 promotes cell proliferation and activates Wnt/β-catenin signaling in colorectal cancer. Cell Biol Int. 2019;43(4):402–8. https://doi.org/10.1002/cbin.11096.
Nyati KK, Agarwal RG, Sharma P, Kishimoto T. Arid5a Regulation and the roles of Arid5a in the inflammatory response and disease. Front Immunol. 2019;10:2790. https://doi.org/10.3389/fimmu.2019.02790.
Janesick A, Abbey R, Chung C, Liu S, Taketani M, Blumberg B. ERF and ETV3L are retinoic acid-inducible repressors required for primary neurogenesis. Development. 2013;140(15):3095–106. https://doi.org/10.1242/dev.093716.
Lei D, Yang WT, Zheng PS. HOXB4 inhibits the proliferation and tumorigenesis of cervical cancer cells by downregulating the activity of Wnt/β-catenin signaling pathway. Cell Death Dis. 2021;12(1):105. https://doi.org/10.1038/s41419-021-03411-6.
Yang J, Li Y, Zhang Y, Zhou X, Zhao Y, Han Y. NCAPD3 Regulates tumor growth and predicts prognosis in diffuse large B-cell lymphoma. Blood. 2019;134:5045. https://doi.org/10.1182/blood-2019-123910.
Gschwandtner M, Derler R, Midwood KS. More than just attractive: how CCL2 influences myeloid cell behavior beyond chemotaxis. Front Immunol. 2019;10:2759. https://doi.org/10.3389/fimmu.2019.02759.
Nam H, Jeon S, An H, Yoo J, Lee HJ, Lee SK, Lee S. Critical roles of ARHGAP36 as a signal transduction mediator of Shh pathway in lateral motor columnar specification. Elife. 2019;8: e46683. https://doi.org/10.7554/eLife.46683.
Wang LH, Zhang GL, Liu XY, Peng A, Ren HY, Huang SH, et al. CELSR1 promotes neuroprotection in cerebral ischemic injury mainly through the Wnt/PKC signaling pathway. Int J Mol Sci. 2020;21(4):1267. https://doi.org/10.3390/ijms21041267.
Niu N, Ma X, Liu H, Zhao J, Lu C, Yang F, Qi W. DLC1 inhibits lung adenocarcinoma cell proliferation, migration and invasion via regulating MAPK signaling pathway. Exp Lung Res. 2021;47(4):173–82. https://doi.org/10.1080/01902148.2021.1885524.
Saha SK, Choi HY, Yang GM, Biswas PK, Kim K, Kang GH, et al. GPR50 promotes hepatocellular carcinoma progression via the notch signaling pathway through direct interaction with ADAM17. Mol Ther Oncolytics. 2020;17:332–49. https://doi.org/10.1016/j.omto.2020.04.002.
Lyu X, Ding X, Ye H, Guo R, Wu M, Cao L. KLF14 targets ITGB1 to inhibit the progression of cervical cancer via the PI3K/AKT signalling pathway. Discov Oncol. 2022;13(1):30. https://doi.org/10.1007/s12672-022-00494-1.
Zhou CC, Xiong QC, Zhu XX, Du W, Deng P, Li XB, et al. AFF1 and AFF4 differentially regulate the osteogenic differentiation of human MSCs. Bone Res. 2017;5:17044. https://doi.org/10.1038/boneres.2017.44.
Xi P, Ding D, Zhou J, Wang M, Cong YS. DDRGK1 regulates NF-κB activity by modulating IκBα stability. PLoS ONE. 2013;8(5): e64231. https://doi.org/10.1371/journal.pone.0064231.
Filmus J, Capurro M, Rast J. Glypicans. Genome Biol. 2008;9(5):224. https://doi.org/10.1186/gb-2008-9-5-224.
Chen M, Zhao Y, Yang X, Zhao Y, Liu Q, Liu Y, et al. NSDHL promotes triple-negative breast cancer metastasis through the TGFβ signaling pathway and cholesterol biosynthesis. Breast Cancer Res Treat. 2021;187(2):349–62. https://doi.org/10.1007/s10549-021-06213-8.
Sun X, Cheng L, Sun Y. Autism-associated protein POGZ controls ESCs and ESC neural induction by association with esBAF. Mol Autism. 2022;13(1):24. https://doi.org/10.1186/s13229-022-00502-9.
Zheng C, Lin X, Xu X, Wang C, Zhou J, Gao B, et al. Suppressing UPR-dependent overactivation of FGFR3 signaling ameliorates SLC26A2-deficient chondrodysplasias. EBioMedicine. 2019;40:695–709. https://doi.org/10.1016/j.ebiom.2019.01.010.
Cliffe ST, Kramer JM, Hussain K, Robben JH, de Jong EK, de Brouwer AP, et al. SLC29A3 gene is mutated in pigmented hypertrichosis with insulin-dependent diabetes mellitus syndrome and interacts with the insulin signaling pathway. Hum Mol Genet. 2009;18(12):2257–65. https://doi.org/10.1093/hmg/ddp161.
Ishida N, Kuba T, Aoki K, Miyatake S, Kawakita M, Sanai Y. Identification and characterization of human Golgi nucleotide sugar transporter SLC35D2, a novel member of the SLC35 nucleotide sugar transporter family. Genomics. 2005;85(1):106–16. https://doi.org/10.1016/j.ygeno.2004.09.010.
Settembre C, Arteaga-Solis E, McKee MD, de Pablo R, Al Awqati Q, Ballabio A, Karsenty G. Proteoglycan desulfation determines the efficiency of chondrocyte autophagy and the extent of FGF signaling during endochondral ossification. Genes Dev. 2008;22(19):2645–50. https://doi.org/10.1101/gad.1711308.
Woods S, Humphreys PA, Bates N, Richardson SA, Kuba SY, Brooks IR, et al. Regulation of TGFβ signalling by TRPV4 in chondrocytes. Cells. 2021;10(4):726. https://doi.org/10.3390/cells1004072.
Wang Y, Li N, Zheng Y, Wang A, Yu C, Song Z, et al. KIAA1217 promotes epithelial-mesenchymal transition and hepatocellular carcinoma metastasis by interacting with and activating STAT3. Int J Mol Sci. 2021;23(1):104. https://doi.org/10.3390/ijms23010104.
Maroteaux P, Spranger J, Opitz JM, Kucera J, Lowry RB, Schimke RN, Kagan SM. Le syndrome campomélique [The campomelic syndrome]. Presse Med. 1893;1971(79):1157–62.
Diaz-Meyer N, Day CD, Khatod K, Maher ER, Cooper W, Reik W, et al. Silencing of CDKN1C (p57KIP2) is associated with hypomethylation at KvDMR1 in Beckwith–Wiedemann syndrome. J Med Genet. 2003;40(11):797–801. https://doi.org/10.1136/jmg.40.11.797.
Joyce JA, Lam WK, Catchpoole DJ, Jenks P, Reik W, Maher ER, et al. Imprinting of IGF2 and H19: lack of reciprocity in sporadic Beckwith–Wiedemann syndrome. Hum Mol Genet. 1997;6(9):1543–8. https://doi.org/10.1093/hmg/6.9.1543.
Bartholdi D, Krajewska-Walasek M, Ounap K, Gaspar H, Chrzanowska KH, Ilyana H, et al. Epigenetic mutations of the imprinted IGF2-H19 domain in Silver–Russell syndrome (SRS): results from a large cohort of patients with SRS and SRS-like phenotypes. J Med Genet. 2009;46(3):192–7. https://doi.org/10.1136/jmg.2008.061820.
Bliek J, Maas SM, Ruijter JM, Hennekam RC, Alders M, Westerveld A, et al. Increased tumour risk for BWS patients correlates with aberrant H19 and not KCNQ1OT1 methylation: occurrence of KCNQ1OT1 hypomethylation in familial cases of BWS. Hum Mol Genet. 2001;10(5):467–76. https://doi.org/10.1093/hmg/10.5.467.
Acknowledgements
None.
Funding
This work was supported by a grant from the Polish National Science Centre UMO- 2020/37/B/NZ5/03693 to Aleksander Jamsheer.
Author information
Authors and Affiliations
Contributions
AS – manuscript writing, preparing figures and tables; EB-O – manuscript design, manuscript writing and revision; AJ – manuscript revision and supervision, funding acquisition. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Szoszkiewicz, A., Bukowska-Olech, E. & Jamsheer, A. Molecular landscape of congenital vertebral malformations: recent discoveries and future directions. Orphanet J Rare Dis 19, 32 (2024). https://doi.org/10.1186/s13023-024-03040-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13023-024-03040-0