
Abstract
Background
Phenylketonuria (PKU) is an inborn error of metabolism caused by a deficiency of the enzyme phenylalanine hydroxylase. If untreated, the complications of PKU lead to significant neucognitive and neuropsychiatric impairments, placing a burden on both the individual’s quality of life and on the healthcare system. We conducted a systematic literature review to characterize the impact of PKU on affected individuals and on healthcare resources in Latin American (LATAM) countries.
Methods
Searches of the global medical literature as well as regional and local medical literature up to September 2021. Observational studies on patients with PKU from any LATAM country. Pairs of reviewers independently screened eligible articles, extracted data from included studies, and assessed their risk of bias.
Results
79 unique studies (47 cross-sectional studies, 18 case series, 12 case reports, and two cohort studies) with a total of 4090 patients were eligible. Of these studies, 20 had data available evaluating early-diagnosed PKU patients for meta-analysis of burden outcomes. Intellectual disability in the pooled studies was 18% [95% Confidence Interval (CI) 0.04–0.38; I2 = 83.7%, p = 0.0133; two studies; n = 114]. Motor delay was 15% [95% CI 0.04–0.30; I2 = 74.5%, p = 0.0083; four studies; n = 132]. Speech deficit was 35% [95% CI 0.08–0.68; I2 = 93.9%, p < 0.0001; five studies; n = 162].
Conclusions
There is currently evidence of high clinical burden in PKU patients in LATAM countries. Recognition that there are many unmet neuropsychological needs and socioeconomic challenges faced in the LATAM countries is the first step in planning cost-effective interventions.
Similar content being viewed by others


Background
Phenylketonuria (PKU) is an inborn error of metabolism caused by a deficiency of the enzyme phenylalanine hydroxylase (PAH) which results in elevated levels of phenylalanine (Phe) and reduced levels of tyrosine [1]. The incidence within Latin American (LATAM) countries is estimated at 1 in 23,000 live births [2]. PKU presents a spectrum of severity, and there are several different classifications that have been proposed [2]. Several different classification schemes to determine clinical management have been proposed since PAH deficiency presents a spectrum of severity [1]. Individuals with classical PKU have a complete enzyme deficiency resulting in untreated blood Phe levels > 1200 μmol/L (an average normal Phe level is approximately 60 μmol/L), which is considered the severe form of this disorder [1].
The treatment for PKU is a lifelong dietary restriction of protein supplemented by a Phe-free amino acid fortified medical food [1], and ongoing monitoring of blood Phe levels to maintain a target range of 120–600 μmol/L for patients ≥ 12 years old, and up to 360 μmol/L for those < 12 years old [3]. If left untreated, the disease can manifest as significant intellectual impairment, neuropsychiatric disorders, and seizures [4] which place a burden on the individual’s quality of life, their families, and on the public and private healthcare systems [4]. Even patients diagnosed and treated at an early age face significant challenges related to adherence with the Phe-restricted diet.
Latin America comprises of 20 countries that represent a great diversity not only in terms of geography but also demographics, economies, languages, ethnicities, and health care systems [5]. In a recent review from Borrajo [6], newborn screening (NBS) programs were distinctively implemented in Latin America. While some programs date back from the 1980’s, other countries are still implementing regional NBS programs. Additionally, the number of diseases covered varies significantly across programs. Spefically concerning PKU, this genetic disorder is included in the NBS program for 14 countries (Cuba, Costa Rica, Chile, Uruguay, Argentina, Mexico, Brazil, Guatemala, Paraguay, Panama, Ecuador, Peru, Bolivia and Honduras) [6] with on average 92.3% of newborns in those countries screened for PKU. Regarding the availability of PKU treatment, half of the Latin America countries have fully subsidized medical foods by the government though the special low-protein foods are not available in most of the countries [7].
Evaluating the unmet needs and burden of PKU on affected individuals is important to determine the impact on the LATAM public and private healthcare system. Recognition that there are many challenges that the patient with PKU faces is the first step in planning for cost-effective intervention scenarios. We therefore conducted a systematic literature review and meta-analysis to better characterize the impact of PKU in LATAM countries on selected patient-important outcomes as well as at the economic (socioeconomic, healthcare utilization) level.
Material and methods
Our review followed recommendations for systematic reviews and meta-analyses of observational studies in epidemiology (MOOSE) [8]. This systematic review has been registered in the PROSPERO (International Prospective Register of Systematic Reviews) database under the number CRD42020211417.
Eligibility criteria
We included any epidemiological observational study (ie, cohort, case-control, nested case-control, cross-sectional studies, case series, case reports, surveys) on patients with PKU or phenylalanine hydroxylase deficiency (PAH), regardless of disease severity, including classical, moderate, and mild forms of this disorder, from any LATAM country regardless of whether they reported on any of the pre-defined patient-important outcomes and/or economic burden outcomes as defined below. We also included studies on caregivers of PKU patients.
Studies that only reported disease prevalence or incidence as well as non-human studies and subjective reports of clinical or observational studies such as letters, editorials and commentaries were excluded.
Pre-defined patient-important outcomes of interest included:
-
Neurological, neurocognitive and neuropsychiatric impairments: intellectual disability, mental disorders, autism spectrum disorder, motor deficits, speech deficits and language delay, tremor, Attention Deficit Hyperactivity Disorder (ADHD) and hyperactivity, mood, depression, anxiety, phobias, irritability and/or aggressiveness, frustration, social isolation;
-
Executive function deficit: working memory, sustained attention, inhibitory control, processing speed impairments, impairment in visuomotor coordination;
-
Other comorbidities such as overweight, osteopenia, osteoporosis, skin problems, headaches, fatigue and sleeping disorder;
-
Quality of life measured by non-validated and validated questionnaires, as defined by the included studies; and
-
Patient adherence to clinical recommendations, including frequency of blood testing (ideally biweekly to monthly with targeted Phe concentrations of 120–360 μmol/L as recommended by the American College of Medical Genetics and Genomics (ACMG) guidelines [1] and 120–600 μmol/L for those ≥ 12 years of age by the European guidelines [9] and dietary management including a Phe-restricted diet supplemented by Phe-free amino acid fortified medical foods as well as the use of sapropterin dihydrochloride in patients who are responsive to this pharmacological treatment.
Symptoms of being late-treated for the disease, such as seizures, microcephaly, generalized rash, and peculiar-smelling urine, were not investigated as patient-important outcomes for the purposes of this review.
Pre-defined economic outcomes of interest included:
-
Socioeconomic impact (eg, school / education level, work experience and productivity, marital status, personal independence, living situation, employment, social status);
-
Impact of PKU on caregiver health-related quality of life; and
-
Impact of PKU on the healthcare system (eg, direct and/or indirect costs, treatment costs, health care resource use, cost of comedications, hospitalizations).
Data source and searches
Using Medical Subject Headings (MeSH) based on the terms “phenylketonuria” and “phenylalanine” (Additional file 1: Table 1) we performed the search in the global medical literature using Medical Literature Analysis and Retrieval System Online (MEDLINE, via PubMed, from 1946 to September 2021), Excerpta Medica Database (EMBASE, via Elsevier, from 1974 to September 2021), and Web of Science (to September 2021).
In the regional and local medical literature, both Spanish and English terms were used to search in Latin American and Caribbean Health Sciences Literature (LILACS, 1982 to September 2021), Scientific Electronic Library Online (SciELO, 1997 to September 2021), SciVerse Scopus via Elsevier (to September 2021), the Spanish Bibliographic Index of the Health Sciences (IBECS, 1983 to September 2021), National Bibliography in Health Sciences Argentina (BINACIS, to September 2021), Caribbean Health Sciences Literature (MedCarib, to September 2021), National Medical Sciences Information Center of Cuba (CUMED, to September 2021), Brazilian Bibliography of Dentistry (BBO, to September 2021), Health Information Locator (LIS, to September 2021), Regional Database of Health Technology Assessment Reports of the Americas (BRISA/RedTESA, to September 2021), Nursing Database (BDENF, to September 2021), Index Psychology (IndexPsi, to September 2021), and the WHO Institutional Repository for Information Sharing (WHO IRIS, to September 2021). The date the search was conducted was September 24, 2021 and no starting date restrictions, or language restrictions, were imposed. The search strategy was adapted for each database to achieve more specificity and sensitivity. Duplicate records across databases were removed.
We searched the gray literature including the Brazilian Digital Library of Theses and Dissertations (BDTD). In addition, reference lists of relevant primary studies were hand searched and experts in the field were contacted to obtain additional unpublished data where feasible.
Selection of studies
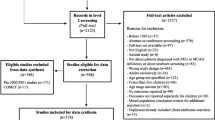
Reviewers independently screened all titles and abstracts identified by the literature search using online software Covidence (https://www.covidence.org), obtained full-text articles of all potentially relevant studies, and evaluated them against the eligibility criteria. Reviewers resolved disagreement by discussion or, if necessary, with third party adjudication. We also considered studies reported only as abstracts and we attempted to contact study authors for additional information where needed. We recorded the selection process and documented via a PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram (Fig. 1).

PRISMA flow diagram
Data synthesis and statistical analysis
We performed a systematic review of studies with pooled analysis of proportions [10, 11], using the method of Stuart-Ord (inverse double arcsine square root) with their respective 95% confidence intervals (CI). Only case series and cross-sectional studies were considered for quantitative analysis; case reports were excluded. To avoid bias related to the effect of delayed implementation of dietary management in late treated patients, only early-diagnosed patients (ie, diagnosed within first three months of life) were included. Studies that did not report whether the treatment was implemented at an early or late age were excluded from the meta-analysis as well as those that did not separate data for the early- or late-diagnosed patients.
Since we expected that there were both clinical and methodological differences among the included studies, a random-effects model [12] was used to perform the pooled analysis of proportions [10, 11]. The meta-analysis was performed with the StatsDirect software, version 2.8.0. (StatsDirect Ltd, Altrincham, Cheshire, UK).
Results
Study selection
Our initial searches identified 3917 citations (n = 3854 from electronic searches; n = 63 identified through the gray literature). After removing duplicates from different databases, 3081 potentially relevant articles were further assessed using title and abstract review. A total of 202 articles were identified for full text assessment. After screening the full texts, we included 79 studies with 11 further publications (ie, multiple publications of the same set of patients) (47 cross-sectional studies, 18 case series, 12 case reports, and two retrospective cohort studies) with a total of 4090 patients [7, 18-17-106]. The reasons for exclusion are listed in the PRISMA flow diagram (Fig. 1). When studies were presented in more than one publication, all applicable references were included.
Six of the included studies were published only as an abstract [13,14,15,16,17,18,19], ten studies as a thesis [20,21,22,23,24,25,26,27,28,29], and the majority (n = 57) were published as full-text in peer-reviewed journals [14, 28, 30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74]. Seven further studies [27, 29, 75,76,77,78,79] were published initially as a thesis followed by a full-text publication [34, 43, 80,81,82,83]. When information regarding risk of bias or other aspects related to study criteria were unavailable in the methods, we attempted to contact study authors for additional information.
Study characteristics
Sixty-four of the 79 included studies reported at least one patient-important outcome at individual or population level, and they are displayed in Table 1 for study characteristics. Regarding study design, 18 were case series [22, 23, 33, 34, 40,41,42, 45, 54, 55, 58, 60, 70, 84,85,86,87], 47 cross-sectional studies [6, 7, 13,14,15, 17,18,19,20,21, 24, 26, 29, 30, 35,36,37,38,39, 43, 46, 47, 53, 56, 59, 61, 62, 67, 68, 71, 73, 75,76,77, 79,80,81, 88,89,90,91], 13 case reports [34, 44, 48, 51, 63, 64, 69, 74, 84, 87, 92,93,94], and two cohort studies [57, 95].
Forty of the included studies were conducted in Brazil [14, 19,20,21,22,23,24, 26, 27, 29, 31, 43, 45, 51, 56, 58, 59, 62, 64, 67, 69,70,71,72,73, 75,76,77,78, 80, 81, 83, 84, 86, 88, 91, 94, 97, 98], seven in Argentina [15, 17, 18, 33,34,35,36,37,38, 46, 47], five in Chile [39,40,41,42, 89], three each in Colombia [48, 54, 74] and Mexico [55, 85, 93], two each in Ecuador [44, 92], Venezuela [60, 63] and Uruguay [32, 90], and one in Cuba [68]. One study [87] was a multicenter conducted in Ecuador, Bolivia, and Paraguay. The case series and cross-sectional studies sample size ranged from two [32] to 420 patients [46, 47]. Patients’ ages ranged from a mean of 3.11 [20] to 19.3 [73] years old (Table 1).
The type of patient-important outcomes most frequently reported among the cross-sectional and case series studies were neurological, neurocognitive and neuropsychiatric impairments (n = 33 studies, 50.8%) [21, 22, 24, 27, 30,31,32,33, 38,39,40, 43, 45, 53,54,55, 59,60,61, 67, 68, 77, 78, 81, 83,84,85,86,87,88,89, 91, 98], followed by overweight (n = 11, 16.9%) [23, 26, 40, 56, 68, 71,72,73, 76, 80, 89, 97], patient adherence to clinical recommendations (n = 10, 15.4%) [7, 22, 33, 62, 66, 67, 70, 79, 82, 83, 87], executive function deficit (n = 6, 92.3%) [21, 24, 58,59,60,61], socioeconomic impact (n = 7, 10.8%) [7, 29, 30, 54, 59, 68, 83, 86], skin problems (n = 4, 6.2%) [54, 55, 68, 96], osteopenia (n = 5, 7.7%) [17,18,19, 23, 27, 68, 78], followed by impact of PKU on caregiver health-related quality of life, quality of life and sleeping disorders (n = 2, 3.1%) [30, 59, 67, 86]. The majority of the cross-sectional, case series, and case report studies (83.1%, n = 64) reported only on patient-important outcomes at an individual level (Table 1).
Among the 12 case report studies, the majority (83.3%, n = 10) assessed neurological, neurocognitive and neuropsychiatric impairments [44, 48, 63, 64, 74, 90, 92,93,94], executive function deficit [34, 44, 64, 90, 92], skin problems [43, 48, 63, 64], and patient adherence to clinical recommendations [23, 25, 61]. Six case report studies [48, 51, 64, 69, 92, 94] evaluated other outcomes such as vomiting [48, 64, 94], weight-height deficit [64], abdominal distention [68], persistent respiratory acidosis [68], gastroesophageal reflux [94], bronchitis [94], megaloblastic anemia [69], and maternal phenylketonuria [51] (Table 1).
Additional file 2: Table 2 describes the 15 studies evaluating other patient-important or economic burden outcomes than those pre-specified for this review; all of these, except for three studies [15, 46, 47, 49], reported that patients received a Phe-restricted diet and/or a Phe-free amino acid fortified medical food. Six studies out of 15 did not report whether patients were receiving treatment [15, 25, 46, 47, 52, 65].
Additional file 3: Table 3 provides additional details around the specific pre-specified patient-important or economic burden outcomes reported among the 12 case report studies. Five out of the 12 studies reported psychosocial outcomes (ie, severe mental retardation and autism, irritability, aggressiveness and intellectual deterioration) [44, 48, 64, 74, 90]; four on physical outcomes (ie, psychomotor retardation) [44, 64, 74, 90]; one study reported on other outcomes (ie, maternal phenylketonuria) [51]; and two studies reported socioeconomic results (ie, delay in school performance, poor socialization, and withdrawal from formal schooling) [64, 74].
Risk of bias assesment
Figure 2 and Additional files 4 and 5: Tables 4 and 5 describe the risk of bias assessment. Overall, the included studies presented a low risk of bias in the majority of the domains. In the cross-sectional studies (Fig. 2, panel A), at least one of the following domains of sample size, statistical significance, statistics methods, or demographic data were rated as “high risk of bias” in five studies (12.8%) [7, 38, 39, 43, 96]. In the case series studies (Fig. 2, panel B), three domains (ie, clear description of both patient’s history and post-intervention clinical condition, and description of a takeaway lesson) were rated as “high risk of bias” in three studies (25.0%) [32, 58, 86].

Risk of bias assessment. (A) cross-sectional studies. (B) case series studies
Meta-analysis results
The results were pooled from case series and cross-sectional studies that reported data only on early-diagnosed patients to avoid bias related to the effects of delayed implementation of dietary management in late-diagnosed patients. Studies that did not provide quantitative data on outcome of interest in papers were also excluded from analysis as well as studies that did not report whether the treatment was implemented at an early or late age. Therefore, out of 67 included studies [14, 16, 19,20,21,22,23,24,25,26,27,28,29, 31,32,33,34, 39,40,41,42,43,44,45, 48,49,50, 52,53,54,55,56,57, 59,60,61,62,63,64,65,66,67,68,69,70, 72,73,74,75,76,77,78,79,80,81,82,83,84,85,86, 88,89,90,91,92,93,94,95,96,97,98,99,100,101], 20 studies [22, 29, 31, 39,40,41,42, 52, 55, 59, 60, 62, 66, 67, 76, 77, 77, 78, 80, 83, 96, 98] qualified for the quantitative analysis described below. None of the included studies evaluating early-diagnosed PKU patients reported symptoms including headache and fatigue, quality of life, or the impact of PKU on the healthcare system.
Neurological, neurocognitive, and neuropsychiatric impairments
Attention deficit hyperactivity disorder (ADHD) and hyperactivity
The pooled proportion of ADHD and hyperactivity was 40% [95% CI 0.21 to 0.61; I2 = 89.2%, p < 0.0001] from eight studies [29, 31, 39, 53, 59, 60, 78, 83, 98] with a total of 222 patients (Fig. 3A). There was significant statistical heterogeneity in the analyses.

Proportional meta-analysis of neurological, neurocognitive, and neuropsychiatric impairments outcomes in early-diagnosed PKU patients. (A) ADHD and hyperactivity. (B) Intellectual disability. (C) Irritability and aggressiveness. (D) Mental disorders. (E) Motor delay. (F) Speech and language deficits
Autism, intellectual disability, irritability and aggressiveness
A single study [49] evaluated early-diagnosed PKU patients who were reported to have autism. Out of 78 patients assessed, two were diagnosed with autistic behaviour.
The pooled proportion of intellectual disability was 18% [95% CI 0.04–0.38; I2 = 83.7%, p = 0.0133] from two studies [67, 77, 81] including a total of 114 patients (Fig. 3B). There was significant statistical heterogeneity in the analyses.
The pooled proportion of irritability and aggressiveness was 44% [95% CI 0.12–0.80; I2 = 96.2%, p < 0.0001] from five studies [22, 29, 39, 59, 60, 83] with a total of 200 patients (Fig. 3C). There was significant statistical heterogeneity in the analyses.
Mental disorders
The pooled proportion of mental disorder was 16% [95% CI 0.01–0.42; I2 = 89.7%, p < 0.0001] from three studies [29, 39, 42, 83] with a total of 115 patients (Fig. 3 D). A study [42] that reported slight retardation was also considered in this analysis. There was significant statistical heterogeneity in the analyses.
Motor delay
The pooled proportion of motor delay was 15% [95% CI 0.04–0.30; I2 = 74.5%, p = 0.0083] from four studies [22, 27, 41, 53, 98] with a total of 132 patients (Fig. 3E). There was significant statistical heterogeneity in the analyses. Any report of motor delay such as low motor development, neuromotor restriction [22], and deficit for gross motor area [27, 98] was considered.
Speech and language deficits
The pooled proportion of speech and language deficits was 35% [95% CI 0.08–0.68; I2 = 93.9%, p < 0.0001] from five studies [22, 27, 39, 53, 60, 98] with a total of 162 patients (Fig. 3F). There was significant statistical heterogeneity in the analyses. Additional reports of speech delay included speech deficits such as “only emits a word” [32], alterations in language [53], and mild to moderate speech disorder [27, 98] were reported.
Other comorbidities
Obesity and overweight
The pooled proportion of obesity was 12% [95% CI 0.09–0.15; I2 = 0%, p = 0.6129] from three studies [40, 71, 76, 80] with a total of 379 patients (Fig. 4, panel A). There was no significant statistical heterogeneity in the analyses.

Proportional meta-analysis of other outcomes in early-diagnosed PKU patients. (A) Obesity. (B) Overweight. (C) Skin alterations. (D) Sleeping disorders. (E) Patient adherence to clinical recommendations
The pooled proportion of overweight was 11% [95% CI 0.07–0.16; I2 = 47.2%, p = 0.1504] from three studies [40, 71, 76, 80] with a total of 379 patients (Fig. 4B). There was no significant statistical heterogeneity in the analyses.
Osteopenia
Only one study [43, 78] evaluating early-diagnosed PKU patients reported on osteopenia. Out of 31 patients, three were diagnosed with osteopenia.
Skin alterations
The pooled proportion of skin alterations was 34% [95% CI 4.9E-3 to 0.85; I2 = 85.7%, p = 0.0081] from two studies [55, 96] with a total of 40 patients (Fig. 4 C). Both included studies reporting lightening of the skin. There was significant statistical heterogeneity in the analyses.
Sleeping disorders
The pooled proportion of sleeping disorders was 71% [95% CI 0.13–0.99; I2 = 86.2%, p = 0.007] from two studies [59, 60] with a total of 22 patients (Fig. 4D). There was significant statistical heterogeneity in the analyses.
Patient adherence to clinical recommendations after treatment
The pooled proportion of patient adherence to clinical recommendation was 53% [95% CI 0.38 to 0.67; I2 = 83.7%, p < 0.0001] from five studies [22, 29, 62, 66, 67, 83] with a total of 260 patients (Fig. 4E). There was significant statistical heterogeneity in the analyses.
Socioeconomic impact
The pooled proportion of socioeconomic impact was 37% [95% CI 0.07–0.75; I2 = 88.5%, p = 0.0032] from two studies [29, 59, 83] with a total of 73 patients (Fig. 5). There was significant statistical heterogeneity in the analyses. The included studies reported the following socioeconomic impact: poor school performance [18], and special education [29, 83].

Proportional meta-analysis of economic outcomes in early-diagnosed PKU patients
Impact of phenylketonuria on caregiver health-related quality of life
The pooled proportion of impact of PKU on caregiver health-related quality of life (ie, did not acquire toilet training [32, 86]) was 42% [95% CI 0.09–0.80; I2 = 0%, p = 0.7519] from two studies [32, 86] with a total of five patients. There was no significant statistical heterogeneity in the analyses.
Descriptive analysis of single studies reporting the outcomes of interest
Four studies [24, 58, 59, 61] reported executive function outcomes with 41% being classified as below average in the assessment of receptive vocabulary using the Peabody Image Vocabulary Test [59]. Malloy-Diniz et al. [61] reported that PKU children with high blood Phe levels (ie, mean Phe levels between 360 and 600 μmol/L) performed significantly worse than both the PKU children with low blood Phe levels and the control children on tasks that assess executive functioning. Morão et al. [24] found that the patients also showed a loss in the score of the Children Gambling Task. Lamônica et al. [58] reported that out of 10 patients, two of them presented outside the normality standards in the development scales. The skills were related to performance in motor, linguistic and cognitive activities. Furthermore, Poloni et al. [7] reported that most LATAM countries did not have low-protein foods, including Phe-free amino acid fortified, and no alternative treatments available. Also, they found that low purchasing power, limited/insufficient availability of low-protein foods, poor adherence, and lack of technical resources to manage the diet were major barriers to treatment. And last, Martins et al. [30] reported that half of the parents and caregivers who completed the survey had financial burden related to PKU management, some had to stop working to care for the PKU patient, and others had to hire a caregiver to assist the PKU patient. With regards to patient’s complaints, irritability was the most reported affected symtom accounting for 78% of the patients, followed by anxiety (67%), and lack of concentration (58%). Despite these findings, 70% of the patients have never undergone a cognitive and/or executive function assessment, and limitation on social activities, impact on professional life, and the effect on self-esteem were also listed as barriers to receive appropriate assessments.
Discussion
Main findings
PKU is a genetic inborn error in the metabolism of Phe. The pathogenic variants that cause PKU are present in high frequency in some LATAM countries such as Brazil and Chile [102].
Based on pooled data from 21 case series and cross-sectional studies [19, 22,23,24, 26, 29, 31,32,33, 39, 40, 42, 44, 52, 56, 59, 60, 67, 70, 71, 78, 80,81,82, 84,85,86, 88, 96,97,98] including 1224 patients, we found evidence demonstrating the impact of PKU on affected individuals in LATAM, with pooled proportions of burden ranging from 9% with osteopenia to 53% with speech and language deficits. Furthermore, only 53% of patients were adherent to clinical recommendations with 37% of patients experiencing socioeconomic impact of PKU. These are higher rates as compared to what we were expecting given that there is the ability to effectively diagnose and treat PKU.Query
Strengths and limitations
Strengths of our review include a comprehensive search; assessment of eligibility, risk of bias and data abstraction independently and in duplicate; and an assessment of risk of bias that included a sensitivity analysis addressing homogeneity of study designs.
The primary limitation of our study is the highly heterogeneous nature of study samples in all studied clinical burden outcomes, except for the outcomes of obesity (Fig. 4, Panel A), osteopenia, and impact of PKU on caregiver health-related quality of life. Sources of this heterogeneity include both clinical and methodological diversities. The studies differed considerably in their mean age of patient selection, phenotype, modalities of implementation of the treatment (eg, newborn screening, access to treatment, lack of knowledgeable caregivers), and study designs (ie, case series and cross-sectional).
Furthermore, out of the 79 studies that met selection criteria, we were only able to include data in the meta-analysis from 21 of them (26.6%). The majority of the studies provided data on only one pre-specified outcome of interest, resulting in small sample sizes for many of the pooled analyses. In addition, there were studies that reported on late diagnosis patients and they were not included in the meta-analysis.
Relation to prior research
One systematic review [103] identified in the literature corroborates our findings showing that even with dietary treatment, long-term physical growth (ie, body weight, height/recumbent length, and body mass index) are not attained in PKU. Another systematic review [104] showed that bone mineral density was lower in PKU patients compared with a control group. With regards to the latter outcome, four studies [105,106,107,108,109] reported a prevalence of osteopenia and osteoporosis ranging from 5 to 14%, which encompass our findings. Although we did not evaluate anthropometric variables in our review, we found a reasonable high prevalence of overweight individuals (11%) and of obesity (12%).
Furthermore, a frequent prevalence of being overweight was described in another systematic review [110] ranging from 7.8 to 32.6% in children and adolescents with PKU, which is also consistent with our findings (23%).
A very high prevalence of ADHD and hyperactivity (40%) and a moderate rate of intellectual disability (19%) were found in our review, which is consistent with others systematic reviews [111, 112] indicating that they are more common in both children and adults with PKU, despite being early diagnosed.
One study [113] conducted in the United States (US) showed that compared to the general population, PKU was associated with a significantly higher prevalence for intellectual disability, autism spectrum disorder, Tourette/tic disorders, eating disorders and behavior/conduct disorder in adult population. Of note, increased prevalence of these comorbidities persisted even when the sample was restricted to younger adults (aged 20–38 years), a subgroup with high probality of being diagnosed at birth and had the opportunity for continuos treatment throughout life. In parallel, a German study [114] not only corroborated that adults PKU patients suffered with neurospycholigical disease burden, but also revealed that this population presented additional comorbidities such as cardiometabolic risk factors. Also, these authors reported a higher intake of prescriptions for gastrointestinal agents, analgesics, antipyretics, statins, and antidepressants. Despite the methodological differences (both studies evaluated adult populations from a single country and were based on data retrieved from their respective healthcare systems), both studies are in line wth our findings that PKU potentially increases the neuropsychological comorbidities.
Conclusions
LATAM PKU patients presented with a high prevalence of clinical complications, regardless of whether there is the possibility of residual confounding due to publication bias and the high heterogeneity in the analysis. Although it is widely accepted that PKU treatment is needed for life, the current approach in LATAM is primarily by using dietary management, which does not seem sufficient to avoid the disease burden outcomes investigated in this research. Furthermore, this review showed that there is a high degree of poor adherence to clinical recommendations. This study also highlights the need to address well-conducted burden of illness studies in PKU patients in LATAM to further elucidate the full spectrum of complications seen in this disease, to inform the healthcare providers taking care of these patients as well as the public health authorities on the ongoing and significant complications of this genetic disorder. [115,116,117,118]
Availability of data and materials
All data generated or analysed during this study are included in this published article and its Additional file 6: information files.
Abbreviations
- ADHD:
-
Attention deficit hyperactivity disorder
- ACMG:
-
American College of Medical Genetics and Genomics guidelines
- HPA:
-
Hyperphenylalaninemia
- LATAM:
-
Latin American
- PRISMA:
-
Preferred reporting items for systematic review and meta-analysis
- MOOSE:
-
Meta-analysis of observational studies in epidemiology
- PAH:
-
Phenylalanine hydroxylase deficiency
- PKU:
-
Phenylketonuria
- PROSPERO:
-
International prospective register of systematic reviews
- MeSH:
-
Medical subject headings
- MEDLINE:
-
Medical literature analysis and retrieval system online
- EMBASE:
-
Excerpta medica database
- CENTRAL:
-
Cochrane central register of controlled trials
- LILACS:
-
Latin American and Caribbean Health Sciences Literature
- SciELO:
-
Scientific electronic library online
- IBECS:
-
Spanish bibliographic index of the health sciences
- BINACIS:
-
National bibliography in health sciences Argentina
- MedCarib:
-
Caribbean health sciences literature
- CUMED:
-
National Medical Sciences Information Center of Cuba
- BBO:
-
Brazilian bibliography of dentistry
- ANVISA:
-
National health surveillance agency
- BDTD:
-
Brazilian digital library of theses and dissertations
- BMI:
-
Body mass index
- JBI:
-
Joanna Briggs Institute
- CI:
-
Confidence interval
- PROSPERO:
-
(International Prospective Register of Systematic Reviews)
References
Vockley J, Andersson HC, Antshel KM, Braverman NE, Burton BK, Frazier DM, et al. Phenylalanine hydroxylase deficiency: diagnosis and management guideline. Genet Med. 2014;16(2):188–200.
Borrajo JCG. Panorama epidemiológico de la fenilcetonuria (PKU) en Latinoamérica. Acta Pediatr Mex. 2012;33(6):279–87.
van Wegberg AMJ, MacDonald A, Ahring K, Belanger-Quintana A, Blau N, Bosch AM, et al. The complete European guidelines on phenylketonuria: diagnosis and treatment. Orphanet J Rare Dis. 2017;12(1):162.
Williams RA, Mamotte CD, Burnett JR. Phenylketonuria: an inborn error of phenylalanine metabolism. Clin Biochem Rev. 2008;29(1):31–41.
Borrajo GJ. Newborn screening in Latin America at the beginning of the 21st century. J Inherit Metab Dis. 2007;30(4):466–81.
Borrajo GJC. Newborn screening in Latin America: a brief overview of the state of the art. Am J Med Genet C Semin Med Genet. 2021;187(3):322–8.
Poloni S, Dos Santos BB, Chiesa A, Specola N, Pereyra M, Saborio-Rocafort M, et al. Current practices and challenges in the diagnosis and management of PKU in Latin America: a multicenter survey. Nutrients. 2021;13(8):2566.
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008–12.
van Spronsen FJ, van Wegberg AM, Ahring K, Bélanger-Quintana A, Blau N, Bosch AM, et al. Key European guidelines for the diagnosis and management of patients with phenylketonuria. Lancet Diabetes Endocrinol. 2017;5(9):743–56.
El Dib R, Touma NJ, Kapoor A. Cryoablation vs radiofrequency ablation for the treatment of renal cell carcinoma: a meta-analysis of case series studies. BJU Int. 2012;110(4):510–6.
El Dib R, Nascimento Junior P, Kapoor A. An alternative approach to deal with the absence of clinical trials: a proportional meta-analysis of case series studies. Acta Cir Bras. 2013;28(12):870–6.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–88.
Downes MJ, Brennan ML, Williams HC, Dean RS. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open. 2016;6(12): e011458.
Amorim T, Boa-Sorte N, Leite MEQ, Acosta AX. Aspectos clínicos e demográficos da fenilcetonúria no Estado da Bahia. Revista Paulista de Pediatria. 2011;29:612–7.
Azcoiti ME, Chiesa A, R. E, Valle G, Mendez V, Gotta G, et al. Implementation of molecular diagnosis for PAH related disorders in a public hospital. Annual Meeting of Bioscience Societes 2020; 10–13 November 2020. MEDICINA2020.
Cornejo EV, Concha M, Cabello JF, Raimann E. Lipids composition diet in phenylketonuric children with early diagnosis. Arch Latinoam Nutr. 2005;55(4):332–5.
Keselman A, Cassinelli H, Fraga C, Gruñeiro-Papendieck L, Chiesa A. Bone mineral density (BMD) and phenylketonuria (PKU). 7th Joint Meeting Paediatric Endocrinology in collaboration with APEG, APPES, JSPE and SLEP; Lyon, France 2005.
Fraga C, Valle MG, Enacan R, Chiesa A. Bone Mineral Density and BH4 Treatment. 13th International Congress of Inborn Errors of Metabolism; 5–8 September 2017; Rio de Janeiro, Brazil: J Inborn Errors Metab Screen; 2017. p. 1–413.
Mendes AB. Fragilidade Óssea dos Fenilcetonúricos, Reflexo da Dietoterapia? – Um estudo com pacientes da APAE-RIO. Revista de Pediatria SOPERJ. 2006;7(2):20.
Cerqueira MMM. O engajamento dos cuidadores na dieta para as suas crianças fenilcetonúricas: influência de fatores sócio-demográficos e psicossociais: Universidade Federal de Minas Gerais – Minas Gerais; 2004.
Dutra VF. Avaliação neuropsicológica de crianças e adolescentes com hiperfenilalaninemias: Faculdade de Ciências Médicas da Universidade de Campinas - São Paulo; 2013.
Figueira VB. Perfil clínico e epidemiológico de pacientes portadores de fenilcetonúria no estado de Goiás: Universidade Federal de Goiás – Goiás; 2018.
Martins FF. Efeito do consumo de biscoitos enriquecidos com cálcio em pacientes com fenilcetonúria: Universidade Federal Fluminense – Rio de Janeiro; 2007.
Morão CPAB. Perfil neuropsicológico e desempenho executivo de crianças com fenilcetonúria tratada: Universidade Presbiteriana Mackenzie; 2017.
Oliveira RF. Condiçöes de saúde dental e gengival em crianças com fenilcetonúria atendidas na Fundaçäo Ecumênica de Proteçäo ao Excepcional (FEPE) no Estado do Paraná 2001.
Sena BS. Estado nutricional e indicadores antropométricos de risco cardiovascular de pacientes com diagnótico de fenilcetonúria atendidos em um serviço de referência do nordeste brasileiro: Universidade Federal de Pernambuco –Pernambuco; 2018.
Silva GK. Habilidades do comportamento comunicativo de crianças com fenilcetonúria tratadas desde o período neonatal: Faculdade de Odontologia de Bauru da Universidade de São Paulo –São Paulo; 2008.
Starling ALP. Densitometria óssea em crianças e adolescentes fenilcetonúricos: Universidade Federal de Minas Gerais – Minas Gerais; 2005.
Vieira TA. Fatores associados a adesão ao tratamento dos pacientes com fenilcetonúria acompanhados pelo serviço de genética médica do hospital de clínicas de Porto Alegre: Universidade Federal do Rio Grande do Sul – Rio Grande do Sul; 2010.
Martins AM, Pessoa ALS, Quesada AA, Ribeiro EM. Unmet needs in PKU and the disease impact on the day-to-day lives in Brazil: results from a survey with 228 patients and their caregivers. Mol Genet Metab Rep. 2020;24: 100624.
Beckhauser MT, Beghini Mendes Vieira M, Moehlecke Iser B, Rozone DELG, Rodrigues Masruha M, Lin J, et al. Attention deficit disorder with hyperactivity symptoms in early-treated phenylketonuria patients. Iran J Child Neurol. 2020;14(1):93–103.
Benítez V, San Julián E, Rodríguez MM. Fenilcetonuria: a propósito de dos pacientes. Arch Pediatr Urug. 2001;72:293–7.
Bernal AC, Eiroa H. Fenilcetonuria de diagnostico tardio. Sociedad Iberoamericana de Información Científica (SIIC). 2017.
Blanco FA, Quintana AB, Martinez CV, Pardo MM. Importance of early diagnosis of phenylketonuria in women and control of phenylalanine levels during pregnancy. Nutr Hosp. 2012;27(5):1658–61.
Pardo-Campos ML, Enacan R, Valle MG, Chiesa A. Parenting styles and coping strategies in PKU early detected children. J Inborn Errors Metab Screen. 2021. https://doi.org/10.1590/2326-4594-jiems-2020-0014.
Pardo-Campos ML, Enacan R, Valle MG, Chiesa A. Parenting styles and coping strategies in PKU children 11th Congress of the Latin American Society of Inborn Errors of Metabolism and Neonatal Screening; 12–15 May 2019; Buenos Aires: J Inborn Errors Metab Screen; 2019.
Pardo-Campos ML, Enacan R, Valle MG, Chiesa A. Cognitive asssessment of early detected and treated PKU children. 11th Congress of the Latin American Society of Inborn Errors of Metabolism and Neonatal Screening; 12–15 May 2019; Buenos Aires: J Inborn Errors Metab Screen; 2019.
Chiesa A, Fraga C, Prieto L, Pardo ML. Modelo de atención de pacientes con fenilcetonuria (PKU) en Argentina. Acta Pediátrica de México. 2012;33(6):308–10.
Colombo MC, Troncoso L, Raimann E, Perates CG, Barros T, Cornejo V. Diagnostico de fenilquetonuria en Chile. Rev Chil Pediatr. 1988;59(4):235–9.
Cornejo EV, Castro G, Fernández E, Cabello JF, Raimann E, De la Parra APS, et al. Modelo chileno de seguimiento a largo plazo para fenilcetonuria (PKU). Acta Pediatr Mex. 2012;33(6):301–7.
Cornejo EV, Manríquez EV, Colombo CM, Mabe SP, Jiménez MM, De la Parra CA, et al. Fenilquetonuria de diagnóstico neonatal y lactancia materna. Rev Med Chile. 2003;131:1280–7.
Cornejo EV, Raimann BE, Godoy PX, Colombo CM. Seguimiento de pacientes con hiperfenilalaninemia diagnosticados precozmente. Rev Chil Pediatr. 1995;66:300–3.
da Silva FGS, de Souza CFM, Schwartz IVD. Attention-deficit hyperactivity disorder in Brazilian patients with phenylketonuria. Acta Neurol Belg. 2020;120(4):893–9.
De Lucca M, Barba-Guzmán C, Cobo-Sevilla V, Latta MA. Fenilcetonuria de diagnóstico tardío y mutaciones asociadas en una familia ecuatoriana. Invest Clin. 2017;58:274–83.
Diament AJ, Lefèvre AB. Fenilcetonúria: estudo clínico e mediante biópsia cerebral. Arq Neuropsiquiatr. 1967;25:1–16.
Enacán R, Prieto L, Nuñez-Miñana M, Fernandez L, Valle MG, Salerno M, et al. Phenylalanine hydroxilase (PAH) genotyping in PKU argentine patients. Congreso Latinoamericano de Erroes Innatos del Metabolismo y Pesquisa Neonatal; 12–15 May 2019; Buenos Aires. J Inborn Errors Metab Screen. 2019.
Enacán R, Miñana MN, Fernandez L, Valle MG, Salerno M, Fraga CI, et al. Phenylalanine Hydroxylase (PAH) Genotyping in PKU Argentine Patients. J Inborn Errors Metab Screen. 2019. https://doi.org/10.1590/2326-4594-jiems-2019-0012.
Escaf M. Fenilcetonuria e hiperfenilalaninemia en recién nacidos. Salud Uninorte. 2003;17:36–9.
Esteves MTC, Chagas ACR, Vignoli VV, Castilho OB. Incidência de fenilcetonúria em pacientes com retardamento mental em Alfenas, Minas Gerais. Rev Esc Farm Odontol Alfenas. 1990;12:99–107.
Fagioli D, Coelho HDS, Maturana N, Almeida EC, Marques T, Masson IB. Práticas alimentares nos primeiros seis meses de vida de crianças com Fenilcetonúria. J Health Sci Inst. 2014;32(1):70–3.
Figueiró-Filho EA, Lopes AHA, Senefonte FRA, Júnior VGS, Botelho CA, Duarte G. Maternal phenylketonuria: a case report. Rev Bras Ginecol Obstet. 2004;26(10):813–7.
Fisberg RM, Silva-Fernandes ME, Schmidt BJ, Fisberg M. Nutritional evaluation of children with phenylketonuria. Sao Paulo Med J. 1999;117:185–91.
Gejão MG, Ferreira AT, Silva GK, Anastácio-Pessan FL, Lamônica DAC. Communicative and psycholinguistic abilities in children with phenylketonuria and congenital hypothyroidism. J Appl Oral Sci. 2009;17:69–75.
Gelvez N, Acosta J, Lopez G, Castro D, Prieto JC, Bermudez M, et al. Phenotypic and molecular characterization of a Colombian family with phenylketonuria. Biomedica Revista del Instituto Nacional de Salud. 2016;36(3):390–6.
Jiménez-Pérez MO, Gómez-Garza G, Ruiz-García M, Fernández-Lainez C, Ibarra-González I, Vela-Amieva M. Resonancia magnética nuclear de encéfalo en pacientes con fenilcetonuria diagnosticada tardíamente. Acta Pediatr de Mex. 2015;36:09–17.
Kanufre VC, Soares RDL, Alves MRA, Aguiar MJB, Starling ALP, Norton RC. Metabolic syndrome in children and adolescents with phenylketonuria. J Pediat. 2015;91:98–103.
Kanufre VC, Starling AL, Leao E, Aguiar MJ, Santos JS, Soares RD, et al. Breastfeeding in the treatment of children with phenylketonuria. J Pediat. 2007;83(5):447–52.
Lamônica DAC, Stump MV, Pedro KP, Rolim-Liporacci MC, Caldeira ACGC, Anastácio-Pessan FL, et al. Acompanhamento do aleitamento materno no tratamento de crianças com fenilcetonúria. J Soc Bras Fonoaudiol. 2012;24(4):3816–9.
Lamônica DAC, Gejão MG, Anastácio-Pessan FL. Fenilcetonúria e habilidades de leitura e escrita. Revista CEFAC. 2015;17:143–50.
Mahfoud A, de Lucca M, Domínguez CL, Arias I, Casique L, Araujo K, et al. Clinical findings and mutational spectrum in Venezuelan patients with delayed diagnosis of phenylketonuria. Rev Neurol. 2008;47(1):5–10.
Malloy-Diniz LF, Cardoso-Martins C, Carneiro KC, Cerqueira MMM, Ferreira APA, Aguiar MJB, et al. Funções executivas em crianças fenilcetonúricas: variações em relação ao nível de fenilalanina. Arq Neuropsiquiatr. 2004;62:473–9.
Mancini PC, Starling ALP, Penna LM, Ramos CAV, Ferreira MIO, Iório MCM. Achados audiológicos em crianças com fenilcetonúria. Revi Soc Bras Fonoaudiol. 2010;15:383–9.
Mariño M, Zarzalejo Z. Tratamiento nutricional de um niño com fenilcetonuria de diagnóstico neo natal. Estudio de caso An Venez Nutr. 2000;13(1):202–9.
Menezes RSB, Ribeiro EM, Coelho FMS, Nogueira HBR. Fenilcetonúria associada à alergia à proteína do leite de vaca. J Health Biol Sci. 2019;7(1):97–100.
Monteiro LTB, Cândido LMB. Fenilcetonúria no Brasil: evolução e casos. Rev Nutr. 2006;19:381–7.
Nalin T, Perry IDS, Refosco LF, Netto CBO, Souza CFM. Fenilcetonúria no sistema único de saúde: avaliação de adesão ao tratamento em um centro de atendimento do Rio Grande do Sul. Rev HCPA. 2010;30(3):225–32.
Vieira Neto E, Filho HSM, Monteiro CB, Carvalho LM, Tonon T, Vanz AP, et al. Quality of life and adherence to treatment in early-treated Brazilian phenylketonuria pediatric patients. Braz J Med Biol Res. 2018. https://doi.org/10.1590/1414-431x20176709.
Paneque OA, Chacón GG, Galcerán TZ, Peña DYV, Ramírez RM, Roca TZO. Evaluación del estado de salud en pacientes con fenilcetonúria. Rev Cubana Pediatr. 2013;85(3):320–9.
Schmidt DE, Norton RC, Starling ALP, Rodrigues VM, Aguiar MJB, Kanufre VC, et al. Deficiência de vitamina B12 e fenilcetonúria. Rev Med Minas Gerais. 2016;26(Supl 2):S31–4.
Silva LF, Rodrigues GRB, Cavalcante RH, Silva JAC. Fenilcetonúria: perfil e abandono de tratamento em centro de referência no Pará. Rev Soc Bras Clin Med. 2016;14(1):13–7.
Silveira AM, Lima PL, Alves MRA, Soares RDL, Kanufre VC, Rodrigues VM, et al. Overweight/obesity in adolescents with phenylketonuria: Protective and predisposing factors. J Pediatr. 2021. https://doi.org/10.1016/j.jped.2021.04.009.
Tanaka NYY, Turcato MF, Nicoletti CF, Nonino CB, Martins LD, Iannetta O, et al. Effects of short-term calcium supplementation in children and adolescents with phenylketonuria. J Clin Densitom. 2018;21(1):48–53.
Tonon T, Martinez C, Poloni S, Nalin T, MacDonald A, Schwartz IVD. Food Neophobia in Patients With Phenylketonuria. J Endocrino Metab. 2019;9(4):108–12.
Urbanes MB, Alvear C, Moreniz C, Alayon AN, Suárez A. Epileptic encephalopathy by phenylcetonuria. Acta Neurol Colomb. 2006;22:316–22.
Brandalize SRC. Avaliação dos resultados do programa de prevenção e promoção da saúde de fenilcetonúricos do estado do Paraná: condição motora dos portadores de fenilcetonúria com diagnóstico precoce: Universidade Estadual de Ponta Grossa – Paraná; 2002.
Camatta GC. Influência do consumo proteico, da prática de atividade física, do controle metabólico, do estágio de maturação sexual e do IMC no percentual de gordura corporal de adolescentes fenilcetonúricos: Universidade Federal de Minas Gerais – Minas Gerais; 2017.
Castro IPS. Avaliação da inteligência de pacientes com fenilcetonúria atendidos pelo programa de triagem neonatal de Minas Gerais: Universidade Federal de Minas Gerais – Minas Gerais; 2008.
Silva FGS. Prevalência de transtorno de déficit de atenção e hiperatividade e outras alterações neurológicas em fenilcetonúricos de um centro do sul do país: Universidade Federal do Rio Grande do Sul – Rio Grande do Sul; 2018.
Teruya KI. Fatores percebidos pelos pacientes como barreiras a adesão ao tratamento de fenilcetonúria no Brasil: Universidade Federal do Rio Grande do Sul – Rio Grande do Sul; 2019.
Camatta GC, Kanufre VC, Alves MRA, Soares RDL, Norton RC, de Aguiar MJB, et al. Body fat percentage in adolescents with phenylketonuria and associated factors. Mol Genet Metab Rep. 2020;23: 100595.
Castro IPS, Borges JM, Chagas HA, Tiburcio J, Starling AL, Aguiar MJ. Relationships between phenylalanine levels, intelligence and socioeconomic status of patients with phenylketonuria. J Pediatr. 2012;88(4):353–6.
Teruya KI, Remor E, Schwartz IVD. Development of an inventory to assess perceived barriers related to PKU treatment. J Patient Rep Outcomes. 2020;4(1):29.
Vieira TA, Nalin T, Krug BC, Bittar CM, Oliveira Netto CB, Schwartz IVD. Adherence to treatment of phenylketonuria: a study in Southern Brazilian Patients. J Inborn Errors Metab Screen. 2015;3:1-7. https://doi.org/10.1177/2326409815579861
Queiroz IRG, Pondé MP. Percepção de pais/cuidados de indivíduos com fenilcetonúria, com e sem autismo, acompanhados em serviço de referência em triagem neonatal. Rev Psicol Divers Saúde. 2015;4(1):87–95.
Sánchez-Peña A, Martínez-de Villarreal L, Arteaga-Alcaraz G, Torres-Sepúlveda R, Marroquín-Escamilla AR, Abrego-Moya V, et al. Secuelas neurológicas en tres pacientes con fenilcetonuria clásica diagnosticada tardíamente. Bol Med Hosp Infant Mex. 2008;65:191–5.
Steiner CE, Acosta AX, Guerreiro MM, Marques-de-Faria AP. Genotype and natural history in unrelated individuals with phenylketonuria and autistic behavior. Arq Neuropsiquiatr. 2007;65(2A):202–5.
Valle MG, Enacan R, Mendez V, Prieto L, Pardo-Campos ML, Chiesa A. PKU Clinical Experience. 11th Congress of the Latin American Society of Inborn Errors of Metabolism and Neonatal Screening; 12–15 May 2019; Buenos Aires, Argentina: J Inborn Errors Metab Screen; 2019.
Brandalize SRC, Czeresnia D. Avaliação do programa de prevenção e promoção da saúde de fenilcetonúricos. Rev Saúde Pública. 2004;38:300–6.
Peredo OP, Raimann BE, Cataldo GX, Gallardo GS, Cornejo EV. Sindrome de fenilquetonuria materna, un nuevo desafío para Chile. Rev Chil Nutr. 2010;37:111–7.
Rasner M, Vomero A, Varacchi C, Peluffo G, Giachetto G, Kanopa V. Fenilcetonuria: descripción de un caso clínico. Arch Pediatr Urug. 2014;85:28–33.
Silva LF. Avaliação dos níveis de marcadores de neurodegeneração em plasma de pacientes fenilcetonúricos: Universidade do Extremo Sul Catarinense – Criciúma; 2016.
Patricio YP, Maritza M. Fenilcetonuria em um neonato de 29 semanas de edad gestacional: reporte de caso clinico. Rev Ecuat Pediatr. 2018;19(1):16–7.
Pereda-Torales L, Calcáneo-García JA, Enríquez-Torrecilla R, Badillo-Báez EM, Soler-Huerta E. Identificación de un caso de fenilcetonuria a través del tamizaje neonatal. Bol Med Hosp Infant Mex. 2008;65:290–6.
Santos MP, Haack A. Fenilcetonúria em escolar: um relato de caso. Com Ciências Saúde. 2013;24(2):187–200.
Santos JS, Aguiar MJB, Starling ALP, Kanufre VC, Tibúrcioz JD, Lima MOB. Consumo alimentar de lactentes com fenilcetonúria em uso de aleitamento materno. Rev de Nutr. 2011;24:863–72.
Andere J, Mota de Avelar-Alchorne M, Schmidt BJ, Schwery-Michalany N. Classic phenylketonuria: dermatological and histopathological aspects in 35 patients. Bol Med Hosp Infant Mex. 1988;45(2):73–8.
Pérsico RS, Nalin T, L.F. R, Vairo FP, Souza CFM. Análise da densidade mineral óssea em pacientes com fenilcetonúria e sua correlação com parâmetros nutricionais. Clin Biomed Res. 2019;39(1):24–31.
Silva GK, Lamônica DAC. Desempenho de crianças com fenilcetonúria no Teste de Screening de Desenvolvimento Denver - II. Pro-Fono. 2010;22:345–50.
Ribeiro PS, Torres TL, Starling ALP, Iório MCM, Mancini PC. Crianças com fenilcetonúria: avaliação audiológica básica e supressão das otoemissões. Rev Soc Bras Fonoaudiol. 2012;17:248–53.
Russo-Estavillo C, Vásquez-Avelar S, Real-Guerrero J, Belmont-Martínez L, Escoto-Delgadillo M, et al. High frequency of severe phenylketonuria in Jalisco, Mexico. Int J Genet. 2018;18(1):1–6.
Stranieri I, Takano OA. Avaliação do Serviço de Referência em Triagem Neonatal para hipotireoidismo congênito e fenilcetonúria no Estado de Mato Grosso. Brasil Arq Bras Endocrinol Metabol. 2009;53:446–52.
Desviat LR, Pérez B, De Lucca M, Cornejo V, Schmidt B, Ugarte M. Evidence in Latin America of recurrence of V388M, a phenylketonuria mutation with high in vitro residual activity. Am J Med Genet A. 1995;57(2):337–42.
Ilgaz F, Pinto A, Gokmen-Ozel H, Rocha JC, van Dam E, Ahring K, et al. Long-term growth in phenylketonuria: a systematic review and meta-analysis. Nutrients. 2019;11(9):2070.
de Castro MJ, de Lamas C, Sanchez-Pintos P, Gonzalez-Lamuno D, Couce ML. Bone status in patients with phenylketonuria: a systematic review. Nutrients. 2020;12(7):2154.
Lage S, Bueno M, Andrade F, Prieto JA, Delgado C, Legarda M, et al. Fatty acid profile in patients with phenylketonuria and its relationship with bone mineral density. J Inherit Metab Dis. 2010;33(Suppl 3):S363–71.
Zeman J, Bayer M, Stepán J. Bone mineral density in patients with phenylketonuria. Acta Paediatr. 1999;88(12):1348–51.
Mendes AB, Martins FF, Cruz WM, da Silva LE, Abadesso CB, Boaventura GT. Bone development in children and adolescents with PKU. J Inherit Metab Dis. 2012;35(3):425–30.
Modan-Moses D, Vered I, Schwartz G, Anikster Y, Abraham S, Segev R, et al. Peak bone mass in patients with phenylketonuria. J Inherit Metab Dis. 2007;30(2):202–8.
Coakley KE, Douglas TD, Singh RH. Using predictive modeling to estimate bone mineral density in children and adults with phenylketonuria. Interdisciplinary symposium on osteoporosis 2013 - Patient-centered care: Developing successful bone health teams, ISO 2013 Chicago, IL United States. 2013. p. S431-S2.
Sena BDS, Andrade MIS, Silva A, Dourado KF, Silva ALF. Overweight and associated factors in children and adolescents with phenylketonuria: a systematic review. Rev Paul Pediatr. 2020;38: e2018201.
Bilder DA, Noel JK, Baker ER, Irish W, Chen Y, Merilainen MJ, et al. Systematic review and meta-analysis of neuropsychiatric symptoms and executive functioning in adults with phenylketonuria. Dev Neuropsychol. 2016;41(4):245–60.
Burlina AP, Lachmann RH, Manara R, Cazzorla C, Celato A, van Spronsen FJ, et al. The neurological and psychological phenotype of adult patients with early-treated phenylketonuria: a systematic review. J Inherit Metab Dis. 2019;42(2):209–19.
Bilder DA, Kobori JA, Cohen-Pfeffer JL, Johnson EM, Jurecki ER, Grant ML. Neuropsychiatric comorbidities in adults with phenylketonuria: a retrospective cohort study. Mol Genet Metab. 2017;121(1):1–8.
Trefz F, Muntau AC, Schneider KM, Altevers J, Jacob C, Braun S, Greiner W, Jha A, Jain M, Alvarez I, Lane P, Zeiss C, Rutsch F. Health economic burden of patients with phenylketonuria (PKU) - A retrospective study of German health insurance claims data. Mol Genet Metab Rep. 2021;27:100764. https://doi.org/10.1016/j.ymgmr.2021.100764.
Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D, et al. The CARE guidelines: consensus-based clinical case report guideline development. J Clin Epidemiol. 2014;67(1):46–51.
Guyatt GH, Busse JW. Modification of Ottawa-Newcastle to assess risk of bias in nonrandomized trials [Available from: http://distillercer.com/resources/].
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
The Nordic Cochrane Centre TCC. Review Manager (RevMan). 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration. 2011.
Acknowledgements
The author would like to thank Camilla Hissamura from BioMarin Farmacêutica do Brasil LTDA for the scientific review and final edit of the manuscript. This manuscript was prepared according to the International Society for Medical Publication Professionals—Good Publication Practice for Communicating Company -Sponsored Medical Research: the GPP3 Guidelines.
Funding
Prof. Regina El Dib (Universidade Estadual Paulista Júlio de Mesquita Filho, UNESP) provided scientific consulting and medical writing support, which was funded by Biomarin Farmaceutica LTDA.
Author information
Authors and Affiliations
Contributions
All authors contributed to study design, interpretation, and analysis. ALSP, AMM, EMR, NS, AC, DV, EJ, DM, and IVDS were responsible for data identification, extraction, and synthesis. All authors read, revised, and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The other authors have declared no conflict of interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table 1
Search strategy.
Additional file 2: Table 2
Fifteen LATAM PKU included studies evaluating other outcomes than those pre-specified as patient-important or economic burden outcomes of interest.
Additional file 3: Table 3
Reported pre-specified patient-important or economic burden outcomes on 12 LATAM PKU case reports studies.
Additional file 4: Table 4
Risk of bias for cross-sectional studies.
Additional file 5: Table 5
Risk of bias for case series studies.
Additional file 6:
Data extraction, risk of bias assessment, subgroup and sensitivity analyses, heterogeneity assessment and publication bias.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Pessoa, A.L.S., Martins, A.M., Ribeiro, E.M. et al. Burden of phenylketonuria in Latin American patients: a systematic review and meta-analysis of observational studies. Orphanet J Rare Dis 17, 302 (2022). https://doi.org/10.1186/s13023-022-02450-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13023-022-02450-2