
Abstract
Background
Hypophosphatasia (HPP) is a rare inherited disorder, which is caused by loss-of-function mutations in the ALPL gene. HPP is a heterogeneous disease that has a wide spectrum of phenotypes. Few studies were carried out in the Chinese population with HPP, especially in children.
Methods
The clinical and genetic characteristics of 10 Chinese children with HPP who were referred to the Beijing Children’s Hospital were described. Previously reported HPP cases of children in China were also reviewed.
Results
A total of 33 cases were identified, which included 2 perinatal lethal HPP, 10 infantile HPP, 10 childhood HPP, and 11 odonto HPP. The male-to-female ratio was 24:9. The average age at onset was 0.69 years (ranged from 2 h after birth to 14 years), while the average age at clinical diagnosis was 3.87 years (ranged from 2 h after birth to 19 years). Serum alkaline phosphatase (ALP) levels were significantly decreased in patients with perinatal lethal/infantile HPP when compared with those with the mild forms of HPP childhood/odonto HPP (P < 0.01). Although serum phosphate levels were not different (P > 0.05), serum calcium levels were elevated, and serum intact parathyroid hormone levels were decreased in patients with perinatal lethal/infantile HPP in comparison with those with the childhood/odonto HPP (P all < 0.01). Genetic analyses identified 40 mutations in 31 HPP cases, including 28 missense mutations, 9 frameshift mutations, 2 splice junction alterations, and 1 regulatory mutation. Of which, 5 novel mutations were identified in our present study: 2 frameshift mutations (p.Arg138GlyfsTer27, p.Leu511Profs*272); 2 missense mutations (p.Ala176Val, p.Phe268Leu), and 1 splice junction alteration (c.297+5G>A). Compound heterozygous mutations accounted for 80.6% of all variants. No mutational “hot-spot” was found. Most mutations of ALPL were located in exons 5, 7, 10, and 3. Notably, subjects that carrying single heterozygous mutations showed milder phenotypes of HPP, while subjects with nonsense mutations were associated with a severer phenotype.
Conclusions
HPP is a rare disease with often delayed diagnosis, and the incidence of HPP in China may be seriously underestimated. The present study expands the phenotypic and genotypic spectrum and the understanding of HPP in Chinese children. These findings will be useful for clinical assessment and shorten the diagnosis time for pediatric HPP in China.
Similar content being viewed by others


Background
Hypophosphatasia (HPP, OMIM: 146300, 241500, 241510), which was initially reported by Rathbun [1], is a rare inherited metabolic disorder. It is caused by the loss-of-function mutations in the ALPL gene (MIM 171760) that encodes the tissue-nonspecific isozyme of alkaline phosphatase (TNSALP), which is a homodimeric phosphohydrolase and abundantly expressed in the skeleton, developing teeth, liver, and kidney [2]. There are three well-known extracellular substrates of TNSALP, including inorganic pyrophosphate (PPi), pyridoxal-5-phosphate (PLP), and phosphoethanolamine (PEA) [3]. Among them, PPi is a potent inhibitor of mineralization [3]. Thus, the reduced TNSALP activity that due to the mutations in the ALPL gene results in the extracellular accumulation of PPi, which further leads to defective mineralization of bones and teeth.
Although HPP is characterized by impaired mineralization of bones and teeth, and reduced serum alkaline phosphatase (ALP) activity, the clinical spectrum of HPP is extremely variable. Based on the age of onset and the clinical symptoms, HPP is currently classified into six phenotypes: perinatal lethal, perinatal benign, infantile, childhood, adult, and odontohypophosphatasia (odonto-HPP) [2]. Both perinatal lethal and infantile were identified as the severe forms of HPP, whereas perinatal benign, childhood, adult, and odonto-HPP were defined as the mild forms of HPP [4,5,6,7,8]. It has been reported that the severe forms of HPP are usually recessively inherited, while the mild forms of HPP show both dominant and recessive inheritance [6]. At present, the diagnosis of HPP remains as before, relied on clinical indications, while the genetic sequencing of the ALPL gene is a useful technique for the precise diagnosis of HPP.
The ALPL gene is located on chromosome 1p36.1-p34 [9] and comprises 12 exons distributed over 70 kb [10]. As of May 2020, a total of 410 different ALPL mutations have been reported worldwide (http://www.sesep.uvsq.fr/03_hypo_mutations.php). Among these reported ALPL mutations, missense mutations are the most prevalent, which account for 71.2%. The remaining mutations are small deletions mutations (11.0%), splicing mutations (4.9%), nonsense mutations (4.6%), small insertions mutations (3.4%), large deletions/duplications mutations (2.9%), insertion/deletion mutations (1.5%) and regulatory mutations (0.2%). Additionally, the great variety of ALPL mutations produces numerous combinations of compound heterozygous mutations, which further promotes the diversity of clinical manifestations of HPP. Previously, Michigami et al. analyzed 98 unrelated Japanese HPP patients found that p.Leu520ArgfsX86 (c.1559delT) and p.Phe327Leu (c.979T>C) were the two most common mutations and were usually associated with the perinatal severe and perinatal benign forms of HPP, respectively [11]. The mutation p.Glu191Lys (c.571G>A) was the most frequent mutations in Caucasian HPP patients and was commonly associated with mild forms of HPP [12]. From this aspect, finding more about the correlation between genotypes and phenotypes is crucial for genetic counseling and prognostication. However, to date, studies on the relationship between genotypes and phenotypes in Chinese HPP patients are limited, especially in children.
Therefore, in the present study, to clarify the clinical characteristic and the relationships between genotypes and clinical manifestations of HPP in Chinese children, ten unrelated children diagnosed with different forms of HPP in our hospital were analyzed. Besides, we also reviewed the clinical and mutational features of the previously reported HPP cases of children in China.
Materials and methods
Subjects
Ten patients diagnosed with HPP in Beijing Children’s Hospital, Capital Medical University, from 2009 to 2020 were retrospectively studied. All patients were born to non-consanguineous patients and were diagnosed as HPP depending on clinical manifestations and biochemical items. Clinical manifestations, physical examinations, biochemical profiles, and radiological results of each patient were obtained from medical records. Our present study was approved by the Ethics Committee of Beijing Children’s Hospital, Capital Medical University. The written informed consent was obtained from all the patients and their parents before they participating in the study.
Clinical information
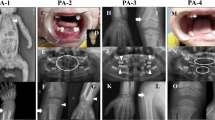
Patient 1 (PA-1) was a 2.5-month-old boy presenting with poor appetite, soft limbs, less activity, cry, and easy to wake up for 2 months. His height was 60.0 cm (25th–50th), and his weight was 5 kg (10th). He showed underweight, low muscular tension, and enlargement of the anterior fontanelle. Biochemistry indexes revealed low serum ALP activity but high serum calcium (Ca) level (Table 2). Serum levels of phosphate (P), intact parathyroid hormone (i-PTH), 25 hydroxyvitamin D3 [25(OH)D3], as well as urinary calcium to creatinine ratio (Ca/Cr), were all in the normal range (Table 1). The X-ray of chest and lower limb long bones demonstrated the decreased bone density of the metaphysis of long bones, distal ribs, and the margin of the irregular bones, the increased distance between epiphysis and metaphysis. Abdominal ultrasound examinations showed calcium deposits in the bilateral renal medulla. He was clinically diagnosed with infantile HPP.
Patient 2 (PA-2) was a 5-month-old girl presenting with poor appetite, failure to gain weight, soft limbs for 4 months. She was 63.0 cm (10th–25th) in height and 4.3 kg (< 3th) in weight. She showed underweight, developmental delay, weak mental response, low muscular tension, rachitic rosary, Harrison groove, craniotabes, and enlargement of the anterior fontanelle. Biochemistry indexes revealed decreased serum ALP and PTH levels, elevated serum Ca and urinary Ca/Cr, and normal serum levels of P and 25(OH)D3 (Table 1). The X-ray of the chest and both carpal bones demonstrated the thin ribs, and decreased density of the ribs, distal ulnar, and radial bones, and also showed multiple low-density lines in the bilateral distal ulnar and radial bones, and the bilateral scapula. Head computed tomography (CT) demonstrated the general widening of cranial sutures and multiple skull osteogenesis imperfecta. Abdominal ultrasound examinations showed diffuse calcium deposits in the medulla of both kidneys. She was clinically diagnosed with infantile HPP.
Patient 3 (PA-3) was a 57.0 cm (< 3th), 5.0 kg (< 3th), 4-month-old boy presenting with feeding difficulties and vomiting for 2 months. He showed underweight, developmental delay, weakness, and enlargement of the anterior fontanelle. Biochemistry indexes revealed decreased serum ALP and i-PTH levels, elevated serum Ca and urinary Ca/Cr, and normal serum levels of P and 25(OH)D3 (Table 1). The X-ray demonstrated uneven long bone density and the widened distance between epiphysis and metaphysics. The spine and skull showed decreased bone density and a thin cranial plate. Chest CT demonstrated the generally decreased bone density and the enlarged soft tissue density at the head of the ribs. Abdominal ultrasound examinations showed diffuse calcium deposits in the medulla of both kidneys. He was clinically diagnosed with infantile HPP.
Patient 4 (PA-4) was a boy, aged 3-month-old, 53.0 cm (< 3th), and 3.6 kg (< 3th), presenting with poor appetite, failure to gain weight, vomiting for 2 months. He showed underweight, developmental delay, weakness, low muscular tension, widely spaced eyes, low ear position, low nasal bridge, and enlarged anterior fontanelle. Biochemistry indexes revealed decreased serum ALP and i-PTH levels, elevated serum Ca and urinary Ca/Cr, and normal serum levels of P and 25(OH)D3 (Table 1). The X-ray demonstrated the uneven bone density and the multiple bone destruction at the metaphysis of long bones. Abdominal ultrasound examinations showed diffuse calcium deposits in the medulla of both kidneys. He was clinically diagnosed with infantile HPP.
Patient 5 (PA-5) was a 3-month-old boy presenting with poor appetite and failure to gain weight for 2 months. His length was 56.0 cm (< 3th) and his weight was 4.1 kg (< 3th). He showed underweight, developmental delay, and enlargement of the anterior fontanelle. Biochemistry indexes revealed decreased serum ALP and i-PTH levels, elevated serum Ca and urinary Ca/Cr, and normal serum levels of P and 25(OH)D3 (Table 1). The X-ray of limbs demonstrated the stubby bones, the unclear boundary of cortex and medulla, the uneven decreased bone density, and the localized lucency shadow in the metaphysis. The X-ray showed decreased bone density and the widening cranial suture, and the cup-like changes in the metaphysis of the left distal radius and ulna. Abdominal ultrasound examinations showed diffuse calcium deposits in the medulla of both kidneys. He was clinically diagnosed with infantile HPP.
Patient 6 (PA-6) was a 54.0 cm (< 3th), 3.7 kg (< 3th), 3-month-old girl presenting with feeding difficulties, and failure to gain weight for 2 months. She showed underweight, developmental delay, and enlargement of the anterior fontanelle. Biochemistry indexes revealed decreased serum ALP and i-PTH levels, elevated serum Ca and urinary Ca/Cr, and normal serum levels of P and 25(OH)D3 (Table 1). The X-ray of the chest demonstrated the thin ribs and the uneven decreased bone density of the ribs. The X-ray of both lower extremities showed the lightly curved tibia, the blurred metaphysis, and the uneven decreased bone density. Abdominal ultrasound examinations showed diffuse calcium deposits in the medulla of both kidneys. She was clinically diagnosed with infantile HPP.
Patient 7 (PA-7) was a 6-year and 5-month-old boy presenting with intermittent claudication for more than 5 years. His body weight was 22 kg (25th–50th). He showed claudication, swelling, and tenderness of the knee joint. Biochemistry indexes revealed decreased serum ALP levels, elevated serum P levels, and normal serum levels of Ca and i-PTH (Table 1). The X-ray of knees showed the multiple bone destruction at the metaphysis and epiphysis of both knees, accompanied by soft tissue swelling. The X-ray of the pelvis showed the small low-density shadow in the bilateral ischia, which suggested the bone destruction of the ischia. The X-ray scans of his hands and ankle joints showed no abnormal signs. Chest and sacroiliac joint CT as well as the abdominal ultrasound examinations also showed no abnormalities. He was clinically diagnosed with childhood HPP.
Patient 8 was a 1 year and 2 months old boy with early deciduous teeth loss. He had a premature loss of deciduous teeth 2 months after the eruption. When he came to our clinic, he had lost two teeth. No bone deformities were found on physical examination. Biochemistry indexes revealed decreased serum ALP levels, elevated urinary Ca/Cr, and normal serum levels of Ca, P, 25(OH)D3, and i-PTH (Table 1). He was diagnosed with odonto-HPP.
Patient 9 was a 1 year and 9 months old boy with the premature loss of the deciduous teeth. He had lost one tooth when he came to our clinic. No bone deformities were found on physical examination. Biochemistry indexes revealed decreased serum ALP levels, elevated serum P levels, and normal serum levels of Ca and i-PTH (Table 1). The X-ray scans of his chest, left carpal bone, knee joint, and hip joint showed no abnormal findings. He was diagnosed with odonto-HPP.
Patient 10 was a 1 year and 2 months old boy with the premature loss of the deciduous teeth. He had lost two teeth when he was 11-month-old. No bone deformities were found on physical examination. Biochemistry indexes revealed decreased serum ALP and i-PTH levels, elevated serum P and urinary Ca/Cr, and normal serum levels of Ca and 25(OH)D3 (Table 1). The X-ray scans of his chest, left carpal bone, skull, spine, and pelvis revealed no abnormality. There were no abnormal signs of abdominal ultrasound examinations. He was diagnosed with odonto-HPP.
ALPL gene mutation analysis
Genomic DNA of patients 2–10 and their relatives available was extracted from peripheral venous blood and sequenced by the Sanger method to screen for genetic variations of the ALPL gene. Sequences generated from samples were compared with the published ALPL sequence (accession no: DNA: NG_008940.1, cDNA: NM_000478.6, protein: NP_000469.3). The variants were recognized as mutations when they were not found in dbSNP (dbSNP, https://www.ncbi.nlm.nih.gov/snp/), in Exome Sequencing Project (http://evs.gs.washington.edu/EVS/), and in the 1000 Genomes Project database (https://www.ncbi.nlm.nih.gov/variation/tools/1000genomes/). Three bioinformatics tools PolyPhen-2 (http://genetics.bwh.harvard.edu/pph), SIFT (http://sift.jcvi.org/), and MutationTaster (http://www.mutationtaster.org/) were used to predict the effects of identified mutations on protein structure and function.
Case review
To provide a comprehensive overview of the reported HPP cases in Chinese children, from March 2005 to April 2019, all publications regarding Chinese children HPP cases in the PubMed database (https://www.ncbi.nlm.nih.gov/pubmed) were reviewed. Additionally, the clinical, biochemical, and molecular characteristics of all previously reported cases were also reviewed.
Statistical analysis
Statistical analysis was conducted using SPSS for Windows version 20.0 (SPSS Inc., Chicago, IL). Results were presented as median (25th, 75th percentiles), and were compared by Mann–Whitney U-test. Chi-square test was used to assess differences in proportions. Graphs were plotted using GraphPad Prism version 7.0 (San Diego, CA) and Illustrator for Biological Sequences (IBS, Wuhan, China). P values < 0.05 were considered statistically significant.
Results
Clinical features
Ten patients in our center were included in this study, and ten published papers with another twenty-three patients were also reviewed. 15/23 (65.22%) cases of the reported HPP were within the past three years, indicating an increasing trend of the awareness, detection, and diagnosis of HPP (Additional file 1: Figure S1). In total, thirty-three Chinese children with HPP were identified, and the clinical features of all patients were summarized in Table 1. Two patients were classified as perinatal lethal HPP (6.1%), ten as infantile HPP (30.3%), ten as childhood HPP (30.3%), and eleven patients as odonto-HPP (33.3%). However, there was no report on perinatal benign HPP in Chinese children. The male-to-female ratio was 24:9. The average onset age was 0.69 years (ranged from 2 h after birth to 14 years), while the average diagnosis age was 3.87 years (ranged from 2 h after birth to 19 years). Twenty-three patients (70%) had delayed diagnosis, which was more serious in the forms of childhood and odonto-HPP. Eighteen (54.5%) patients showed short stature, and fifteen (45.4%) patients showed low body weight, both of which were more common in patients with infantile HPP. Nine out of ten (90.0%) patients with childhood HPP, and all patients with odonto-HPP presented early deciduous tooth loss. All patients had bone deformities. Epilepsies were observed in one patient with perinatal lethal HPP and one patient with infantile HPP. Calcium deposits in the medulla of both kidneys were reported in eight out of ten (80.0%) patients with infantile HPP. Except for three cases lost to follow-up, all patients with perinatal lethal/infantile HPP have died.
Biochemical parameters
The biochemical parameters of thirty-three patients were also shown in Table 1. All patients showed decreased serum ALP levels. Besides, in comparison with patients with the childhood/odonto forms of HPP, serum ALP levels were significantly decreased in patients with perinatal lethal/infantile forms of HPP (P < 0.01) (Fig. 1a). All patients with infantile HPP showed elevated serum Ca levels, and serum Ca levels were elevated in patients with perinatal lethal/infantile forms of HPP when compared with those with the childhood/odonto forms of HPP (P < 0.01) (Fig. 1b). Fifteen patients showed elevated serum P levels (45.4%). No significant difference was found in serum P levels between patients with childhood/odonto and perinatal lethal/infantile forms of HPP (P > 0.05) (Fig. 1c). Only three (0.09%) patients showed decreased serum 25(OH)D3 levels. Eight out of ten (80.0%) patients with infantile HPP had decreased i-PTH levels, and serum i-PTH levels were decreased in patients with perinatal lethal/infantile forms of HPP in comparison with those with the childhood/odonto forms of HPP (P < 0.01) (Fig. 1d). Besides, the elevated random urinary Ca/Cr ratios were observed in six (60.0%) infantile HPP patients.

Comparison of serum ALP (a), Ca (b), P (c) and i-PTH (d) levels between patients with perinatal lethal/infantile HPP and childhood/odonto HPP. Data were shown as median with interquartile. Abbreviations are as follows: ALP alkaline phosphatase, Ca calcium, P phosphate, i-PTH intact parathyroid hormone
ALPL gene mutations
Mutational analysis of the ALPL gene were performed in all patients involved in our present study, except for one patient with infantile HPP. The sequences of ALPL mutations identified in patients 2–9 were shown in Fig. 2, and the sequences identified in patient 10 were shown in our previous published paper [13]. Fourteen mutations were identified in our present study. Nine mutations in PA-2–7 and PA-9–10 were previously identified (p.Tyr28Cys, p.Ala33Val, p.Arg223Gln, p.Ser368del, p.366_367delThrSerinsThr, p. Arg136Cys, p.Arg136His, p.Ala116Thr, p.Tyr388His). The remaining five mutations were novel: two missense mutations (p.Ala176Val, p.Phe268Leu) that found in PA-4 and PA-7, two frameshift mutations (p.Arg138GlyfsTer27, p.Leu511Profs*272) that found in PA-8 and PA-10, and one splice junction alteration (c.297+5G>A) that found in PA-8. According to the ACMG/AMP variant interpretation guidelines, the novel mutations were classified as likely pathogenic (p. Arg138GlyfsTer27, p. Ala176Val, p. Leu511Profs*272) and uncertain (p. Phe268Leu, c.297+5G>A), respectively.

Genetic analysis of ALPL mutations in patients 2–9 and their parents. The arrow indicates the position of the mutation
Additionally, the genetic features of all HPP patients were also summarized. As shown in Table 2, twenty-five (80.6%) patients were compound heterozygous, four (12.9%) were heterozygous, and two (6.5%) were homozygous for mutations in the ALPL gene.
Missense variants (n = 28, 70.0%) and frameshift mutations (n = 9, 22.5%) were responsible for the majority of the allelic alterations, whereas splice junction alterations (n = 2, 5.0%) and regulatory mutations (n = 1, 2.5%) were rare. The most prevalent variants were p. Arg136His (n = 4 alleles, 7.14%), followed by p. Arg136Cys (n = 3 alleles, 5.36%), p. Ala33Val (n = 3 alleles, 5.36%), and p. Tyr388His (n = 3 alleles, 5.36%). As shown in Fig. 3, most mutations of ALPL were located in exons 5, 7, 10, and 3. It is worth noting that in the present study, subjects (patients 16, 17, 22, 24) carrying single heterozygous mutation showed milder phenotypes of HPP. Since no nonsense mutations were found in our study, we analyzed phenotypic differences between nonsense and missense variants, which have been reported in the Tissue Nonspecific Alkaline Phosphatase Gene Mutations Database (http://www.sesep.uvsq.fr/03_hypo_mutations.php). Compared to missense mutations, nonsense mutations were associated with a severer phenotype (P < 0.05) (Fig. 4).

The ALPL mutational spectrum in all patients with HPP. Mutations repeated four times were shown in red color. Mutations repeated three times were shown in purple color. Mutations repeated two times were shown in green color. Mutations repeated only one time were shown in black color. Novel mutations that identified in the present study were bold and colored in blue

Comparison of phenotypes between nonsense and missense ALPL mutations. Abbreviations are as follows: HPP hypophosphatasia. Mutations presented only as severe forms of HPP were shown in red color. Mutations presented only as mild forms of HPP were shown in blue color. Mutations presented as severe/mild forms of HPP were shown in green color
Discussion
HPP is a rare inherited metabolic disorder. Currently, the prevalence of severe HPP has been estimated to be between 1/100,000 and 1/300,000, whereas mild forms of HPP are more common than severe forms (estimated at 1/6370 in Europe) [7]. China has a large territory and the largest population in the world. So far, only 23 children with HPP were reported in China, and 15 cases were reported within the past 3 years. This suggested that the actual number of pediatric HPP cases in China may be underestimated. Here we described the clinical and genetic features of the 23 reported HPP cases as well as 10 HPP cases diagnosed in our hospital to improve the awareness of pediatric HPP in China.
We found that the most common form of HPP in Chinese children was odonto-HPP, followed by infantile and childhood HPP. Only two patients with perinatal lethal HPP, and no patient was documented as perinatal benign HPP, which indicated the low rate of perinatal HPP in China. In contrast to our results, Michigami et al. analyzed 98 unrelated Japanese HPP patients found that perinatal lethal was the most frequent form of HPP in Japan, followed by the perinatal benign form [11]. Diagnostic delay is common among patients with HPP [14]. Vogt et al. conducted a retrospective review of 50 pediatric HPP patients in Germany found the obvious diagnostic delay in infantile (12 months) and childhood HPP (22.5 months) [15]. Similar findings were also identified in our present study. The average age at onset was 0.69 years, while the average age at clinical diagnosis was 3.87 years, indicating a significant delay in diagnosis in China. Additionally, the diagnostic delay was noted in infantile HPP and even obvious in childhood HPP. There may be several reasons for the diagnostic delay, including low awareness, heterogeneity of clinical manifestations, and lack of routine testing of HPP.
As previously described, the clinical spectrum of HPP was highly variable, the main clinical manifestations of the pediatric Chinese patients were in line with those documented in other studies [2, 3, 14]. Failure to thrive was one of the most common manifestations of pediatric HPP patients [16], in the current study, we found that 18 (54.5%) patients showed short stature, and 15 (45.4%) patients showed low body weight, both of which were more common in patients with infantile HPP. Therefore, serum ALP levels should be part of a routine accessory examination in infants and children with problems in gaining weight, growth retardation, and short stature. Similar to other studies [17], we found a higher proportion of males (n = 24, 72.73% approximately) than females (n = 9, 27.27% approximately) diagnosed with pediatric HPP. Indeed, previous studies performed by Grimberga et al. pointed out that compared with boys, girls gained less evaluation for short stature [18]. Thus, the greater parental concern about short stature in sons versus daughters may be one of the explanations for the higher proportion of males in pediatric HPP patients. It is worth noting that contrary to the pediatric HPP, a higher proportion of females than males was observed in adult HPP [14, 19,20,21]. Considering the small number of pediatric HPP patients diagnosed in our country, the sex differences observed in the current study still need to be verified in further studies.
Serum ALP levels were decreased in all HPP patients. From the literature, it is known that serum ALP levels seem to be correlated with the disease severity [15, 22, 23]. Consistent with this, our present study conducted in the Chinese pediatric HPP patients also demonstrated significantly decreased serum ALP levels in patients with perinatal lethal/infantile forms of HPP than those with the childhood/odonto forms of HPP. Interestingly, we observed that serum Ca and i-PTH levels were also correlated with disease severity. Serum Ca levels were elevated, while serum i-PTH levels were decreased in patients with perinatal lethal/infantile forms of HPP in comparison with those with childhood/odonto forms of HPP. In support of our results, previous studies have shown that severe hypercalcemia was common, and circulating PTH levels were physiologically suppressed in infantile HPP [2, 24]. However, in childhood HPP, hypercalcemia was less common and serum PTH levels were usually within the normal range [2]. Our findings together with others [25] supported that serum Ca and PTH could provide important complementary diagnostic information, especially for patients with severe forms of HPP.
Genetic detection is a crucial final step in the diagnosis of HPP. Consistent with international research findings, missense mutations were the most common mutations identified in this study, and exon 5 was the predominantly affected exon. The variety of missense mutations resulted in highly variable clinical expressivity and a large number of compound heterozygous genotypes. Also consistent with other results [15], compound heterozygous mutations were far more common than heterozygous and homozygous mutations. Five novel mutations, including p.Arg138GlyfsTer27, p.Leu511Profs*272, p.Ala176Val, p.Phe268Leu, and c.297+5G>A were found in this study. Although we did not conduct functional in vitro studies of the effects of these mutations, evidence from bioinformatics analysis supported the hypothesis that these mutations were harmful. Three of the identified mutations (p.Arg138GlyfsTer27, p.Leu511 Profs*272, c.297+5G>A) could disrupt the protein structure, result in forming a truncated protein or causing a frame-shift, or loss of protein function by changing splice sites, respectively. For the other two missense mutations we identified (p.Ala176Val, p.Phe268Leu): p.Ala176Val was located in the active site valley, and p.Phe268Leu was located in the calcium-binding site. There are five crucial regions identified in TNSALP, including the active site, the active site valley, the homodimer interface, the crown domain, and the calcium-binding site, and mutations that alter residues at these sites may induce dysfunction of the protein and thus cause the HPP [6, 26, 27]. It is worth noting that our study found obvious differences in the spectrum of ALPL mutations between Chinese individuals and other countries. For example, p.Leu520ArgfsX86 and p.Asp378Val were the most common mutations in Japan [11] and the USA [17], respectively, while no report has been found in Chinese HPP patients. p.Glu191Lys was known to occur with a high frequency (up to 55%) in HPP patients with European ancestry [28]. However, it has been reported only twice in the Chinese population [5]. These results indicated that a Chinese-specific screening panel may be warranted for the diagnose of Chinese HPP patients. To date, the relationship between genotypes and phenotypes in Chinese pediatric HPP patients with ALPL mutations remains unclear. Based on the Tissue Nonspecific Alkaline Phosphatase Gene Mutations Database, we found that nonsense mutations were associated with a severe phenotype in comparison with missense mutations. However, no nonsense mutation was found in pediatric HPP patients in China. Previous studies have shown that patients with a single heterozygous mutation usually presented with mild forms of HPP [14]. The same was seen in our present study, subjects (patients 16, 17, 22, 24) carrying single missense mutation or frameshift mutation showed milder phenotypes of HPP. The number of HPP patients in this study was relatively small considering the large population of China. As the number of HPP patients increases, the genotype–phenotype correlation may be clear in the future.
Our study also showed high mortality in patients with severe forms of HPP. Except for three cases lost to follow-up, all patients with severe forms of HPP (perinatal lethal/infantile HPP) have died. Previous studies have shown that approximately 50% of cases with infantile HPP were predicted to die [2], and if patients manifested with chest deformity, respiratory difficulties, or vitamin B6-dependent seizures before 6 months of age, the mortality was significantly higher [29]. Until recently, the management of HPP in China has been symptomatic and supportive only. In 2015, bone-targeted enzyme-replacement therapy (asfotase alfa) was approved in Japan, and then in Canada, in the European Union, and in the United States to treat pediatric-onset HPP [2]. This enzyme has produced beneficial effects not only in bones but also in other organs, including the lungs and muscle [30]. While asfotase alfa seems very promising, it is not approved in China yet, and many questions regarding its long-term effects and the potential secondary adverse effects remain to be solved in the future.
There are still some limitations in the present study. First, due to its retrospective design, not all clinical or biochemical data were available from all patients. Further follow-up study will be conducted in order to explore the long-term prognosis of patients with mild forms of HPP. Second, although serum ALP, Ca and i-PTH levels were associated with the disease severity, the best cutoffs were unclear. Additionally, PLP and PEA are useful parameters for the diagnostic of HPP and serum PLP levels have been reported to be correlated with the disease severity [12]. However, due to the limited medical equipment in our hospital, PLP and PEA levels were not detected in the present study. Third, in vitro functional experiments will be needed to characterize the function of the novel mutants. Fourth, the number of patients was not big enough due to low awareness. Future research is required to reveal the phenotype-genotype correlations.
In conclusion, our study shows that HPP remains a complex disease with a variable phenotype. Although the number of HPP cases has increased reported in recent years, the incidence of HPP may still be underestimated because of a lack of disease awareness. Diagnosis is often delayed in particular in patients with mild forms of HPP. The mutation spectrum of ALPL in China is quite different from those in other countries. This is the first time to summarize the clinical and genetic characteristics of pediatric HPP patients in China. In the future, further studies in larger cohorts should be conducted to evaluate the phenotype-genotype association in Chinese HPP patients to improve and shorten the diagnosis of HPP.
Availability of data and materials
All data generated and analyzed during this study are included in this published article and are available from the corresponding author upon reasonable request.
Abbreviations
- ALP:
-
Alkaline phosphatase
- Ca:
-
Calcium
- Ca/Cr:
-
Calcium to creatinine ratio
- CT:
-
Computed tomography
- F:
-
Female
- HPP:
-
Hypophosphatasia
- 25(OH)D3:
-
25 Hydroxyvitamin D3
- i-PTH:
-
Intact parathyroid hormone
- M:
-
Male
- P:
-
Phosphate
- PEA:
-
Phosphoethanolamine
- PLP:
-
Pyridoxal-5-phosphate
- PPi:
-
Inorganic pyrophosphate
- SJA:
-
Splice junction alteration
- TNSALP:
-
Tissue-nonspecific isozyme of alkaline phosphatase
References
Rathbun JC. Hypophosphatasia; a new developmental anomaly. Am J Dis Child. 1948;75(6):822–31.
Whyte MP. Hypophosphatasia: an overview for 2017. Bone. 2017;102:15–25.
Linglart A, Biosse-Duplan M. Hypophosphatasia. Curr Osteoporos Rep. 2016;14(3):95–105.
Martins L, Dos SE, de Almeida AB, Machado RA, Lyrio AM, Foster BL, et al. A novel de novo heterozygous ALPL nonsense mutation associated with adult hypophosphatasia. Osteoporos Int. 2020. https://doi.org/10.1007/s00198-020-05490-1.
Mao X, Liu S, Lin Y, Chen Z, Shao Y, Yu Q, et al. Two novel mutations in the ALPL gene of unrelated Chinese children with hypophosphatasia: case reports and literature review. BMC Pediatr. 2019;19(1):456.
Xu L, Pang Q, Jiang Y, Wang O, Li M, Xing X, et al. Four novel mutations in the ALPL gene in Chinese patients with odonto, childhood, and adult hypophosphatasia. Biosci Rep. 2018;38(4):BSR20171377.
Mornet E. Hypophosphatasia. Metabolism. 2018;82:142–55.
Scott LJ. Asfotase Alfa: a review in paediatric-onset hypophosphatasia. Drugs. 2016;76:255–62.
Greenberg CR, Evans JA, McKendry-Smith S, Redekopp S, Haworth JC, Mulivor R, et al. Infantile hypophosphatasia: localization within chromosome region 1p36.1–34 and prenatal diagnosis using linked DNA markers. Am J Hum Genet. 1990;46(2):286–92.
Weiss MJ, Ray K, Henthorn PS, Lamb B, Kadesch T, Harris H. Structure of the human liver/bone/kidney alkaline phosphatase gene. J Biol Chem. 1988;263(24):12002–10.
Michigami T, Tachikawa K, Yamazaki M, Kawai M, Kubota T, Ozono K. Hypophosphatasia in Japan: ALPL mutation analysis in 98 unrelated patients. Calcif Tissue Int. 2020;106(3):221–31.
Hérasse M, Spentchian M, Taillandier A, Mornet E. Evidence of a founder effect for the tissue-nonspecific alkaline phosphatase (TNSALP) gene E174K mutation in hypophosphatasia patients. Eur J Hum Genet. 2002;10(10):666–8.
Liang X, Gong C, Min L. Odonto hypophosphatasia: a case report and gene mutation analysis. Chin J Appl Clin Pediatrics. 2014;29(20):1595–7.
Högler W, Langman C, Gomes DSH, Fang S, Linglart A, Ozono K, et al. Diagnostic delay is common among patients with hypophosphatasia: initial findings from a longitudinal, prospective, global registry. BMC Musculoskelet Disord. 2019;20(1):80.
Vogt M, Girschick H, Schweitzer T, Benoit C, Holl-Wieden A, Seefried L, et al. Pediatric hypophosphatasia: lessons learned from a retrospective single-center chart review of 50 children. Orphanet J Rare Dis. 2020;15(1):212.
Whyte MP, Wenkert D, Zhang F. Hypophosphatasia: natural history study of 101 affected children investigated at one research center. Bone. 2016;93:125–138.
Whyte MP, Zhang F, Wenkert D, McAlister WH, Mack KE, Benigno MC, et al. Hypophosphatasia: Validation and expansion of the clinical nosology for children from 25 years experience with 173 pediatric patients. Bone. 2015;75:229–239.
Grimberg A, Feemster KA, Pati S, Ramos M, Grundmeier R, Cucchiara AJ, et al. Medically underserved girls receive less evaluation for short stature. Pediatrics. 2011;127(4):696–702.
Berkseth KE, Tebben PJ, Drake MT, Hefferan TE, Jewison DE, Wermers RA. Clinical spectrum of hypophosphatasia diagnosed in adults. Bone. 2013;54(1):21–7.
McKiernan FE, Berg RL, Fuehrer J. Clinical and radiographic findings in adults with persistent hypophosphatasemia. J Bone Miner Res. 2014;29(7):1651–60.
García-Fontana C, Villa-Suárez JM, Andújar-Vera F, González-Salvatierra S, Martínez-Navajas G, Real PJ, et al. Epidemiological, clinical and genetic study of hypophosphatasia in a spanish population: identification of two novel mutations in the alpl gene. Sci Rep. 2019;9(1):9569.
Whyte MP, Walkenhorst DA, Fedde KN, Henthorn PS, Hill CS. Hypophosphatasia: Levels of bone alkaline phosphatase immunoreactivity in serum reflect disease severity. J Clin Endocrinol Metab. 1996;81(6):2142–8.
Whyte MP. Hypophosphatasia—aetiology, nosology, pathogenesis, diagnosis and treatment. Nat Rev Endocrinol. 2016;12(4):233–46.
Mochizuki H, Saito M, Michigami T, Ohashi H, Koda N, Yamaguchi S, et al. Severe hypercalcaemia and respiratory insufficiency associated with infantile hypophosphatasia caused by two novel mutations of the tissue-nonspecific alkaline phosphatase gene. Eur J Pediatr. 2000;159(5):375–9.
Salles JP. Hypophosphatasia: biological and clinical aspects, avenues for therapy. Clin Biochem Rev. 2020;41(1):13–27.
Mornet E, Stura E, Lia-Baldini AS, Stigbrand T, Ménez A, Le Du MH. Structural evidence for a functional role of human tissue nonspecific alkaline phosphatase in bone mineralization. J Biol Chem. 2001;276(33):31171–8.
Millán JL. Protein structure and functional domains. In: Mammalian alkaline phosphatases: from biology to applications in medicine and biotechnology. Wiley‐VCH Verlag GmbH & Co. KGaA; 2006.p. 25–66.
Hofmann C, Girschick H, Mornet E, Schneider D, Jakob F, Mentrup B. Unexpected high intrafamilial phenotypic variability observed in hypophosphatasia. Eur J Hym Genet. 2014;22(10):1160–4.
Whyte MP, Rockman-Greenberg C, Ozono K, Riese R, Moseley S, Melian A, et al. Asfotase alfa treatment improves survival for perinatal and infantile hypophosphatasia. J Clin Endocrinol Metab. 2016;101(1):334–42.
Whyte MP, Greenberg CR, Salman NJ, Bober MB, McAlister WH, Wenkert D, et al. Enzyme-replacement therapy in life-threatening hypophosphatasia. N Engl J Med. 2012;366(10):904–13.
Yu F, Wang J, Xu X. Lethal perinatal hypophosphatasia caused by a novel compound heterozygous mutation: a case report. BMC Pediatr. 2019;19(1):109.
Chang KC, Lin PH, Su YN, Peng SS, Lee NC, Chou HC, et al. Novel heterozygous tissue-nonspecific alkaline phosphatase (TNAP) gene mutations causing lethal perinatal hypophosphatasia. J Bone Miner Metab. 2012;30(1):109–13.
Li DF, Lan D, Zhong JZ, Dewan RK, Xie YS, Yang Y. Infantile hypophosphatasia caused by a novel compound heterozygous mutation: a case report and pedigree analysis. Zhongguo Dang Dai Er Ke Za Zhi. 2017;19(5):539–44.
Chou YY, Ou HY, Wu TJ, Tsai SC, Lin SJ, Yu EH. Hypophosphatasia in Taiwan: report of two cases. Kaohsiung J Med Sci. 2005;21(3):134–7.
Zhao Z, Xia WB, Xing XP, Li M, Wang O, Jiang Y, et al. Infantile hypophosphatasia due to mutations in the tissue-nonspecific alkaline phosphatase gene. Zhonghua Nei Ke Za Zhi. 2013;52(10):824–8.
Chen B, Li L, Ren W, Yi L, Wang Y, Yan F. A novel missense mutation in the ALPL gene causes dysfunction of the protein. Mol Med Rep. 2017;16(1):710–8.
Yang H, Wang L, Geng J, Yu T, Yao RE, Shen Y, et al. Characterization of six missense mutations in the tissue-nonspecific alkaline phosphatase (TNSALP) gene in Chinese children with hypophosphatasia. Cell Physiol Biochem. 2013;32(3):635–44.
Zhang H, Ke YH, Wang C, Yue H, Hu WW, Gu JM, et al. Identification of the mutations in the tissue-nonspecific alkaline phosphatase gene in two Chinese families with hypophosphatasia. Arch Med Res. 2012;43(1):21–30.
Wei KW, Xuan K, Liu YL, Fang J, Ji K, Wang X, et al. Clinical, pathological and genetic evaluations of Chinese patients with autosomal-dominant hypophosphatasia. Arch Oral Biol. 2010;55(12):1017–23.
Zhou W, Li LL, Chen B, Yan FH, Li HX. Hypophosphatasia: a case report and gene mutation analysis. Zhonghua Kou Qiang Yi Xue Za Zhi. 2017;52(9):578–9.
Wan J, Zhang L, Liu T, Wang Y. Genetic evaluations of Chinese patients with odontohypophosphatasia resulting from heterozygosity for mutations in the tissue-non-specific alkaline phosphatase gene. Oncotarget. 2017;8(31):51569–77.
Acknowledgements
We are grateful to the patients and families who participated in this study.
Funding
This study was funded by The Pediatric Medical Coordinated Development Center of Beijing Hospitals Authority (XTYB201808), the Public Health Project for Residents in Beijing (Z151100003915103), and the National Key Research and Development Program of China (2016YFC0901505).
Author information
Authors and Affiliations
Contributions
All authors helped to perform the research; Meijuan Liu wrote the manuscript; Min Liu contributed to the project management; Xuejun Liang, Di Wu, Wenjing Li, Chang Su, Bingyan Cao, and Jiajia Chen took part in the collection of clinical samples; Chunxiu Gong conceived and designed the project as well as revised the manuscript. All listed authors revised the paper critically and approved the final version of the submitted manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The research protocol was approved by the ethics committee of Beijing Children’s Hospital, Capital Medical University, and written informed consent was received from all the patients and their parents before they participating in the study.
Consent for publication
Consent was obtained from all patients for publication.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Figure S1.
The number of HPP cases diagnosed in Chinese children from 2005 to 2019. Abbreviations are as follows: HPP hypophosphatasia.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, M., Liu, M., Liang, X. et al. Clinical and genetic characteristics of hypophosphatasia in Chinese children. Orphanet J Rare Dis 16, 159 (2021). https://doi.org/10.1186/s13023-021-01798-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13023-021-01798-1