
Abstract
Background
Aortic regurgitation with dilated annulus presents a technical challenge for conventional transcatheter aortic valve implantation (TAVI) procedures.
Case presentation
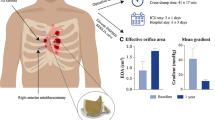
We report a case of an 84-year-old frail patient with a history of breathlessness found to have severe aortic regurgitation and moderately impaired left ventricular systolic function. The patient underwent a successful TAVI procedure using the XL-Myval 32 mm transcatheter heart valve (THV) via an anterior right mini-thoracotomy with a direct aortic approach. The patient recovered well post-operatively with good hemodynamic resolution.
Conclusions
This first in human case highlights the efficacy and potential of applying innovative approaches, such as the new sizes of Myval THV and direct aortic access via anterior right mini thoracotomy, in addressing challenging anatomical variations in TAVI procedures with good outcome.
Similar content being viewed by others

Background
Transcatheter Aortic Valve Implantation (TAVI) has become a widely accepted intervention, particularly in aortic stenosis cases. However, its application in aortic regurgitation (AR) remains less common, presenting challenges, especially when dealing with a significantly enlarged aortic annuli.[1]
This case report presents a significant milestone as the first documented case of inserting a size 32 mm MyVal THV for pure AR via anterior right mini-thoracotomy (ART), showing the feasibility and effectiveness of this novel technique in addressing AR with larger annulus sizes.
Case presentation
An 84-year-old frail man was admitted electively for TAVI with symptomatic severe AR with NYHAIII symptoms. He is an ex-smoker with a history of COPD, symptomatic PVD, and awaiting urgent TEVAR for a large abdominal aortic aneurysm (AAA). Trans-thoracic echocardiography showed severe AR, dilated LVEDD (65 mm), and moderately impaired LV function (Video 1).Coronary angiogram showed non-obstructive coronary artery disease.
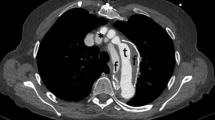
A cardiac CT showed a large aortic annulus (perimeter 90.5 mm, area 635mm2) (Fig. 1) with no calcification and a saccular infrarenal aortic aneurysm measuring 52 mm. There may have been a previous contained rupture. He was discussed by the HEART team and the consensus was for alternative access TAVI.

Annulus measurements on CT scan preoperatively
Under general anaesthesia without using CPB, a DA TAVI via 4 cm anterior right mini-thoracotomy (ART) in the 2nd ICS (Fig. 2) was performed. A bronchial blocker for isolated lung ventilation was used. The right internal mammary artery (RIMA) was clipped and divided. Using a soft tissue retractor, the pericardium was opened and traction sutures on the pericardium inserted.

Direct aortic access site via the anterior right thoracotomy

Additional small satellite puncture site above the 2nd rib
Arterial/venous access via the right radial artery and right femoral vein for pigtail catheter and temporary pacing wire inserted respectively. Pigtail catheter advanced into aortic root to delineate anatomy. Puncture zone identified along distal ascending aorta and 2 × 4/0 Prolene Teflon pledgeted sutures inserted. Following successful puncture via a separate access site (1st ICS) to facilitate alignment and preventing kinking of the device (Fig. 3). A 33 cm 26-Fr Gore® DrySeal flex introducer sheath (GoreMedical) (Minimum I.D 8.7 mm) was delivered over a Safari Large wire into the ascending aorta. This was used instead of the 14-Fr Python™ expandable introducer sheath (Meril’s Life Sciences Pvt. Ltd) to avoid blood loss from the expanding segments. A size 32 mm MyVal was then positioned and deployed (nominal inflation) under rapid ventricular pacing. Angiogram showed no coronary obstruction with good valve positioning and no PVL (Video 2, Video 3, Video 4). TOE confirmed good functioning prosthesis and no PVL (Video 5). Aorta secured with good haemostasis and heparin reversed. The right pleura was drained via the satellite incision site.(Fig. 4). Ultrasound guided right serratus anterior block was done at the end of the procedure. Patient was extubated shortly afterwards and moved for a short period in CSICU. He was discharged home uneventfully on Day 5 postoperatively. Echo pre-discharge demonstrated good functioning aortic prosthesis with AR PHT 560 ms and VTI 0.77. Patient has been reviewed at 6 weeks with good improvement in symptoms, (Video 6).

Final image of the wound appearance at the end of operation (Left) and on discharge(Right)
Discussion
Innovations of transcatheter heart valves and relating delivery systems are continuously evolving.[2] Myval-XL THV (Meril Life Sciences Pvt. Ltd., India) is a balloon-expandable valve available in larger sizes, 30.5 and 32 mm, serving to treat patients with large annulus.[3] It can protect against valve embolisation and residual PVL in non-calcified aortic valves with dilated annulus and can be a good option for treatment of pure AR in high risk patients.[4]
In instances where peripheral access is prohibitive, a trans-apical approach(through left anterior thoracotomy) or a direct aortic approach( performed through upper mini- sternotomy or anterior right mini-thoracotomy) can be considered. The ART access has been shown to reduce the risk of complications and recovery time compared to traditional surgical valve replacement.[5] In comparison to Trans-apical approach, ART is less invasive and associated with lower mortality and morbidity.[6] Additionally, using a soft tissue retractor and avoiding a rib spreader in ART results in less postoperative pain. Trans apical access was not suitable for this patient due to impaired LV function and the large size of the sheath required for the procedure. Compared to the upper mini-sternotomy approach, ART is less invasive and provides better alignment for valve implantation, although it demands a steeper learning curve for the surgeon.[7]
This patient presented with significant comorbidities and frailty, compounded by symptomatic impaired left ventricular systolic function (LVSF) .Following heart team discussion, the patient was referred for TAVI assessment. With a diagnosis of pure aortic regurgitation (AR) and an annulus measuring (Area 635mm2, perimeter 90.5 mm), meticulous sizing was imperative to mitigate the risk of prosthesis embolisation and a size 32 mm Myval valve (nominal implant) was deemed appropriate to provide approximately 25% oversizing. While tans-femoral TAVI is the conventional licenced approach for this valve, the patient’s history of a large saccular AAA necessitated an alternative approach. Consequently, a direct aortic approach via ART was preferred over TA access due to the larger sheath size required in addition to a moderately impaired LV. Precise guidance for the aortic puncture site under fluoroscopy was essential in addition to the pre-operative CT information. Additionally, device alignment was a critical consideration prompting the additional access site from above the ART access incision (above the 2nd rib). Following this, the TAVI procedure progressed smoothly. An effective strategy in achieving optimal valve positioning is to initially position the valve slightly deeper, facilitating subsequent adjustments upwards, rather than starting too high where re-adjustment becomes limited. In addition, DA approach allows for better proximal control of the device.
Conclusion
This case report demonstrates the successful use of the Myval transcatheter heart valve to treat pure aortic regurgitation with a large annulus. Using a direct ascending aorta approach via ART, along with thorough pre-procedural planning and intraoperative techniques, led to favourable outcome despite the patient’s complex condition. The availability of larger valve sizes, like the size 32 mm Myval, was crucial in overcoming anatomical challenges. This emphasises the need for a tailored approach in patients with aortic valve disease and complex comorbidity. Further research and long-term follow-up are necessary to validate the effectiveness and durability of this approach.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- TAVI:
-
Transcatheter aortic valve implantation
- ART:
-
Anterior right mini-thoracotomy
- AR:
-
Aortic Regurgitation
- THV:
-
Transcatheter heart valve
- NYHA:
-
The New York Heart Association classification
- PVD:
-
Peripheral vascular disease
- TEVAR:
-
Thoracic endovascular aortic repair
- AAA:
-
Abdominal aortic aneurysm
- COPD:
-
Chronic obstructive pulmonary disease
- LVEDD:
-
Left ventricle end-diastolic diameter
- CPB:
-
Cardiopulmonary bypass
- DA:
-
Direct aortic
- ICS:
-
Intercostal space
- RIMA:
-
Right internal mammary artery
- I.D:
-
Internal diameter
- TOE:
-
Transoesophageal echocardiography
- PVL:
-
Paravalvular leak
- SAVR:
-
Surgical aortic valve replacement
- CSICU:
-
Cardiac surgery intensive care unit
References
1. - Thielmann M, Tsagakis K, El Gabry M, Jakob H, Wendt D. Transcatheter aortic valve implantation (TAVI) in patients with aortic regurgitation. Ann Cardiothorac Surg. (2017) 6:558–60. 10.21037/acs.2017.09.16
2. - Schneeberger Y, Seiffert M, Schaefer A, Bhadra OD, Schofer N, Pecha S, Westermann D, Blankenberg S, Reichenspurner H, Conradi L. TAVI for Pure Non-calcified Aortic Regurgitation Using a Self-Expandable Transcatheter Heart Valve. Front Cardiovasc Med. 2022 Jan 25;8:743579. doi: 10.3389/fcvm.2021.743579. PMID: 35146003; PMCID: PMC8823702.
3. - Elkoumy A, Terkelsen CJ, Abdelshafy M, Ellert-Gregersen J, Elzomor H, Thim T, Serruys PW, Soliman O and Nissen H (2022) Case report: Transcatheter aortic valve replacement in a large bicuspid anatomy using the XL-Myval 32 mm. Front. Cardiovasc. Med. 9:1045280. doi: 10.3389/fcvm.2022.1045280
4. - Hamieh M, Nassereddine Z, Moussa M, Al Ali F, Dbouk M, Saab M. Transcatheter aortic valve implantation for aortic regurgitation in HeartMate II supported patient using Myval THV: a case report. Oxf Med Case Reports. 2023 Oct 23;2023(10):omad086. doi: 10.1093/omcr/omad086. PMID: 37881260; PMCID: PMC10597617.
5. - Seth A, Kumar V, Singh VP, Kumar D, Varma P, Rastogi V. Myval: A Novel Transcatheter Heart Valve for the Treatment of Severe Aortic Stenosis. Interv Cardiol. 2023 Apr 10;18:e12. doi: 10.15420/icr.2020.32. PMID: 37398875; PMCID: PMC10311401.
6. - M. Branny, et al., Alternative access routes for transcatheter aortic valve implantation (TAVI), Cor et Vasa 59 (2017) e10–e16. doi.org/10.1016/j.crvasa.2017.01.024
7. - Vohra HA, Salmasi MY, Mohamed F, Shehata M, Bahrami B, Caputo M, Deshpande R, Bapat V, Bahrami T, Birdi I, Zacharias J. Consensus statement on aortic valve replacement via an anterior right minithoracotomy in the UK healthcare setting. Open Heart. 2023 Mar;10(1):e002194. doi: 10.1136/openhrt-2022-002194. PMID: 37001910; PMCID: PMC10069572.
Acknowledgements
We extend our gratitude to the anaesthesia, operating theatre, and Cath-Lab teams for their contributions to this work.
Funding
none to declare.
Author information
Authors and Affiliations
Contributions
All authors participated equally in this work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval is N/A, however, an informed Consent to participate form is completed and signed by the patient and available on request.
Consent for publication
This was included in the consent form signed by the patient.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
Supplementary Material 3
Supplementary Material 4
Supplementary Material 5
Supplementary Material 6
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Aljanadi, F., McNeilly, G., Manoharan, G. et al. Direct aortic TAVI via anterior right mini-thoracotomy using 32 mm myval for pure aortic regurgitation. J Cardiothorac Surg 19, 506 (2024). https://doi.org/10.1186/s13019-024-02982-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13019-024-02982-7