
Abstract
A 33-year male patient presented with a 6-month history of cough and shortness of breath upon physical activity. Echocardiography demonstrated right ventricular space-occupying lesions. Contrast-enhanced computed tomography of the chest showed multiple emboli in the pulmonary artery and its branches. Right ventricle tumor (myxoma) resection, tricuspid valve replacement, and clearance of the pulmonary artery thrombus were performed under cardiopulmonary bypass. Minimally invasive forceps and balloon urinary catheters were used to clear the thrombus. Clearance was confirmed by direct visualization using a choledochoscope. The patient recovered well and was discharged. The patient was prescribed oral warfarin 3 mg/day, and the international normalized ratio for prothrombin time was maintained between 2.0 and 3.0. Pre-discharge echocardiogram showed no lesion in the right ventricle or pulmonary arteries. The 6-month follow-up echocardiography indicated that the tricuspid valve was functioning well and showed no thrombus in the pulmonary artery.
Similar content being viewed by others


Introduction
Primary tumors of the heart are uncommon and mostly benign, with an overall incidence of 0.17–0.19% [1]. A right ventricular tumor can cause outflow obstruction and tricuspid valve regurgitation producing symptoms including palpitation, chest tightness, and edema. As most benign heart tumors are soft and loose, they can dislodge from the heart tissue. When a right ventricular tumor (e.g. myxoma) dislodges, it can cause a pulmonary embolism and pulmonary hypertension leading to dyspnea, chest pain, and hemoptysis. Resection of a right ventricular tumor together with thromboembolectomy and the use of a flexible fiber scope to guide and visualize clearance of a pulmonary embolism has been reported. In this case report, we describe the successful resection of a right ventricle myxoma, tricuspid valve replacement, and clearance of a pulmonary embolism using a balloon urinary catheter guided by a choledochoscope.
Case report
Patients and methods
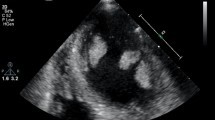
A 33-year male presented with history of cough and shortness of breath for 6 months. The patients presented with the following: blood pressure = 133/89 mmHg, heart rate = 124 beats/min, respiratory rate = 20/min, and body temperature = 36.3 °C. Chest exam was normal. At admission the patient had a D-dimmer of 0.99 µg/Ml (range 0–0.5 µg/mL) and N-terminal pro B type natriuretic peptide level of 219 pg/ml (range 0–125 pg/ml). Contrast-enhanced computed tomography (CECT) of the chest showed an extensive emboli formation in the pulmonary artery and its branches, including left and right pulmonary arteries, and a soft tissue mass protruding into the right ventricle (Fig. 1). Echocardiography showed pulmonary hypertension (systolic pressure = 78 mmHg), right ventricular space-occupying lesion (31 × 34 mm), and moderate grade tricuspid regurgitation [2] (Fig. 1).

a Contrast-enhanced computed tomography showed emboli formation in the pulmonary artery and its branches; b Transthoracic echocardiography before surgery showed a right ventricular space-occupying lesion
Results
The patient underwent a median sternotomy under cardiopulmonary bypass. The ventricular tumor was resected, the tricuspid valve was replaced, and embolism was cleared successfully during the same procedure.
A longitudinal right atriotomy revealed a wide-base mass of 3 × 3 cm originating from the right ventricle anterior wall that was adhered to the regulatory fascicles, papillary muscles, chordae tendineae, and trabeculae. The right ventricle neoplasm was excised from its base and its affected tissue including the chordae tendineae and trabeculae. The anterior and posterior leaflets of the tricuspid valve were removed and replaced with a bioprosthetic valve (mosaic 29# biological valve).
The thrombus in the pulmonary trunk and left and right branches was cleared using balloon urinary catheters and minimally invasive forceps (GEISTER, Germany). Clearance was confirmed under direct visualization using a choledochoscope (Olympus, America) (Fig. 2a). A 5F balloon urinary catheter (Folley) was used to clear the thrombus. The catheter was passed through the distal branch, the balloon was inflated, and the thrombus was pulled out (Fig. 3). The procedure was repeated until the thrombus was cleared.

a Thrombus found in the pulmonary trunk; b Clearance of thrombus guided by Choledochoscope

A #5 urinary catheter was placed in the distal end of the pulmonary artery
Histopathological diagnosis of the right ventricle mass was myxoma (Fig. 4). The patient recovered without any major event and was discharged with oral warfarin 3 mg/day. The international normalized ratio for prothrombin time was maintained between 2.0 and 3.0. The pre-discharge echocardiogram showed no mass in the right ventricular and no obstructive lesion on the pulmonary trunk or left and right pulmonary arteries. At the 6-month follow-up there was no obstructive lesion in the pulmonary arteries, and the patient’s general condition was good.

Tumor pedicle; pathology shows a myxoma
Discussion
This case of right ventricular myxoma with tricuspid valve regurgitation and pulmonary artery embolism was successfully treated in a single setting with mass resection, valve replacement, and emboli clearance using a balloon catheter confirmed visually with a choledochoscope.
The incidence of heart tumors is 0.02%, and 75% of these tumors are benign. Myxoma is the most common type of benign tumor in adult patients with cardiac tumors, three-quarters of which are located in the left atrium. The incidence of right ventricular myxoma reported in the literature is 3–4%. The location and size of a myxoma determines its clinical manifestations with regards to embolism and obstruction [3, 4].
The patient presented in this report had a right ventricular myxoma on the anterior wall of the right ventricle with a pulmonary thrombus embolism. The traditional treatment of acute pulmonary embolism is anticoagulant thrombolysis and percutaneous catheter-directed therapy. However, there is no clear guideline for treating pulmonary embolisms combined with right ventricular tumors. One study reported the use of warfarin to treat a pulmonary embolism following incomplete surgical resection of a right ventricular myxoma, with no recurrence of emboli after 20 months [5]. Another case study reported resection of a right ventricular myxoma of 9.5 × 5.0 cm. However, resection of a ventricular tumor combined with clearance of a pulmonary embolism has not often been reported [6].
Pulmonary embolectomy has rarely been used to treat acute right ventricle dysfunction caused by a pulmonary embolism. However, the procedure and outcome of surgical pulmonary embolectomy have been greatly improved by the use of intraoperative flexible fiber scopes (i.e. fiberoptic bronchoscope, endoscope) to clear and directly visualize the pulmonary arteries [7,8,9]. In the present case report, we successfully used a choledochoscope to visualize and guide the clearance of a pulmonary tree thromboembolism.
In conclusion, a right ventricular myxoma involving the tricuspid valve and regurgitation leading to complications such as pulmonary artery embolism can be treated in a single setting. Tumor resection and removal of a thrombus using a balloon catheter and visual clearance of thrombus with a choledochoscope could be considered for patients with cardiac tumors.
Availability of data and materials
None.
References
Elbardissi AW, Dearani JA, Daly RC, Mullany CJ, Orszulak TA, Puga FJ, Schaff HV. Survival after resection of primary cardiac tumors: a 48-year experience. Circulation. 2008;118(14 Suppl):S7-15.
Oghbi WA, Adams D, Bonow RO, et al. Recommendations for noninvasive evaluation of native valvular regurgitation: a report from the american society of echocardiography developed in collaboration with the society for cardiovascular magnetic resonance. J Am Soc Echocardiogr. 2017;30(4):303–71.
Jain S, Maleszewski JJ, Stephenson CR, et al. Current diagnosis and management of cardiac myxomas. Expert Rev Cardiovasc Ther. 2015;13(4):369–75.
Poterucha TJ, Kochav J, O’Connor DS. Cardiac tumors: clinical presentation, diagnosis, and management. Curr Treat Options Oncol. 2019;20(8):66.
Assaf Y, Nasser M, Jneid H, et al. Pulmonary embolism following incomplete surgical resection of a right ventricular myxoma: a case report and review of the literature. Cardiol Ther. 2018;7(1):107–17.
Lu C, Yang P, Hu J. Giant right ventricular myxoma presenting as right heart failure with systemic congestion: a rare case report. BMC Surg. 2021;21(1):64.
Raman K, Ramanathan S, Sankar J, et al. Flexible fibre optic bronchoscopy as angioscope to ascertain completeness of pulmonary embolectomy: surgery for pulmonary embolism-how I do it. Indian J Thorac Cardiovasc Surg. 2022;38(1):118–21.
Ngaage DL, Shah R, Sanjay SP, et al. Cardiopulmonary endoscopy: an effective and low risk method of examining the cardiopulmonary system during cardiac surgery. Eur J Cardiothorac Surg. 2001;19(2):152–5.
Eini ZM, Houri S, Cohen I, et al. Massive pulmonary emboli in children: does fiber-optic-guided embolectomy have a role? Review of the literature and report of two cases. Chest. 2013;143(2):544–9.
Acknowledgements
We thank Xinqiang Guan, Yanchun Zhang, and Yaxiong Zhou for their assistance during treatment of the patient. We thank Medjaden Inc. for scientific editing of this manuscript.
Funding
None.
Ethics declarations
Ethical approval and consent to participate
Ethical approval was not required for this study as it was a retrospective case review.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mao, Y., Wang, C., Wei, Y. et al. Choledochoscope-guided treatment of pulmonary embolism caused by ventricular myxoma. J Cardiothorac Surg 18, 143 (2023). https://doi.org/10.1186/s13019-023-02250-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13019-023-02250-0