
Abstract
Background
The donor’s mode of brain death (BD), being associated with impairment of myocardial function and hemodynamic performance, impacts the prognosis of the heart transplantation (HTx) recipient.
Methods
All patients who underwent HTx between 1996 and 2017 were categorized according to donor’s BD mechanism: traumatic BD (TBD) versus non-traumatic BD (NTBD).
Results
The TBD group included 105 recipients, and the NTBD group, 85 recipients. Kaplan-Meier survival analysis showed that overall survival was significantly higher for recipients of TBD hearts (10-year survival 58.1 vs. 37.6%, p = 0.044). Consistently, multivariate analysis showed that TBD was independently associated with a significant 43% reduction in mortality [95% confidence interval (CI) 0.42–0.75, p = 0.033]. Rejection rate was lower in the TBD group (total rejection score 0.44 ± 0.32 vs. 0.51 ± 0.38, p = 0.04; any rejection score 0.38 ± 0.26 vs. 0.45 ± 0.31, p = 0.030), and freedom from cardiac allograft vasculopathy (CAV) was significantly higher in recipients of traumatic vs. non-traumatic donors (10 years: 82.9 vs. 62.4%, log-rank p-value = 0.024). Multivariate analysis showed a significant 42% reduction in CAV [hazard ratio (HR) = 0.58, 95% CI 0.51–0.85, p = 0.022).
Conclusion
Mode of brain death significantly impacts HTx outcomes, with TBD being associated with reduced mortality, rejections and CAV.
Similar content being viewed by others


Background
In heart transplantation (HTx), proper matching between donor and recipient is of paramount importance. Nonetheless, donor selection remains a complex and controversial topic, with most of the recommendations being based on consensus of opinion [1, 2]. It is thus critical that we, as heart surgeons, constantly review basic assumptions that rely on previous studies, since the ongoing progress in all fields of medicine is eminently evident at the donor-recipient crossroad at which several areas of medicine meet. It is thus not surprising that the criteria that are used for defining the suitability characteristics for donor hearts are constantly being revised [3, 4], particularly in light of the shortage of available donor hearts, combined with increased demand.
The above notwithstanding, brain dead donors remain the main contributors to organ, particularly heart, transplants worldwide [5]. The importance of this statistic lies in the consensus that the mode of brain death (BD) of the donor may influence the recipient’s outcome [6,7,8]. BD can cause significant heart injury as a result of excessive catecholamine secretion and endocrine and/or hemodynamic disturbances with consequent organ hypoperfusion, resulting in ischemia/reperfusion injury after transplantation [9, 10]. Furthermore, vasopressors will have been administered to > 90% of BD donors [11]. Among the different etiologies that underlie BD, there has been a relative decline in the last decade in the proportion of donors with traumatic brain injury and an increase in those with anoxic brain injury, as reflected in epidemiological data for the distribution of causes of BD in organ donors [12,13,14,15].
Even though early results suggest that the mode of donor BD might impact recipient survival and vasculopathy [6, 7], the impact of this factor on HTx outcomes has been poorly studied and quantified. Such data are likely to be of significant importance in today’s era of technological developments and changing criteria for donor characteristics. Therefore, the present study was conducted to quantify the impact of the mode of donor BD on HTx outcomes.
Methods
Study population and registry design
Our study population comprised 190 consecutive adult patients (> 18 years of age) transplanted at a single center between July 1996 and July 2017. Data for each patient were systematically recorded upon enrollment in the study and during each subsequent visit or medical contact. Clinical data, recorded on prospectively designed forms, included comprehensive information regarding the transplantation procedure, immunosuppression, occurrence of major cardiac events, and treatment during long-term follow-up. Donors’ data were obtained from the National Organ Transplantation Center and from the records of the hospitals at which the donors had died. The study was approved by our institutional review board.
Definitions of brain death mechanism
Brain death diagnosis was determined in accordance with clinical guideline for physicians regulated by the Ministry of Health, followed by the Brain Respiratory Death Act which was established in 2008. HTx patients were divided into two groups based on the mechanism of donor BD, namely, traumatic BD (TBD) vs. non-traumatic BD (NTBD) [6, 7], where TBD was defined as BD resulting from a blunt and penetrating head trauma (e.g., gunshot wound to the head, accidental head trauma) or a clearly definable intracranial bleed that progressed rapidly to brain death [6].
Immunosuppression
All patients were treated with a triple-drug maintenance immunosuppression regimen, comprising steroids, an antimetabolite, and a calcineurin inhibitor. Conversion to everolimus was based on the patient’s risk profile. All patients received induction therapy with anti-thymocyte globulin.
Rejections, surveillance and classification
Rejections were diagnosed by routine institutional follow-up or clinically indicated endomyocardial biopsy (EMB), and were classified according to the revised International Society of Heart and Lung Transplantation (ISHLT) classification system for rejection [16]. Routine EMBs were performed every week for the first 4 weeks after HTx, twice a month in the second and third months, once a month for the next 3 months, and thereafter every 3 months until the end of the first year. From the end of the first year until the end of the fifth year, biopsies were performed annually. Total rejection score (TRS), which reflected the severity of the rejection, and any rejection score (ARS), which represented the total number of rejections regardless of severity, were calculated for each patient as follows: TRS as 0R = 0, 1R = 1, 2R = 2, and 3R = 3, and ARS, as 0R = 0, 1R = 1, 2R = 1, 3R =1. All scores were normalized by dividing the cumulative scores by the total number of biopsy specimens taken for each patient throughout the study period [17].
Cardiac allograft vasculopathy and primary graft dysfunction
The institutional post-transplant care protocol includes annual invasive coronary angiography for the first 5 years following HTx, and thereafter every other year, along with echocardiogram and right heart catheterization. Cardiac allograft vasculopathy (CAV), diagnosed by coronary angiography, and invasive hemodynamic assessment, along with clinical assessment and echocardiography, combined according to the recommended ISHLT standardized nomenclature for CAV [18]. Primary graft dysfunction (PGD) was restricted to 24 h post-surgery and was based on echocardiographic and/or hemodynamic assessment, according to the ISHLT consensus conference recommendations [19].
Outcome measures
The primary end-point was all-cause mortality. Mortality data were obtained from the Population Registry of the State of Israel, where all deaths are registered, as required by law. Secondary endpoints were: 1) rejections 2) freedom from CAV; and 3) freedom from non-fatal major adverse cardiac events (NF-MACE), defined as the development of acute myocardial infarction, congestive heart failure, stroke, new-onset peripheral vascular disease or the need for percutaneous coronary intervention or implantable cardiac defibrillation.
Statistical analysis
Descriptive statistics were produced using means and standard deviations for continuous variables (e.g. age), and frequencies for categorical variables (e.g., gender). To examine differences between groups in continuous variables, Mann-Whitney procedures were used to avoid bias for non-normal distributions. To examine differences between groups in categorical variables, Chi-Square tests were conducted. The Kaplan–Meier estimator was used to assess the time to the first occurrence of each endpoint by BD mechanism, and groups were compared using the log-rank test. Multivariable Cox proportional hazard regression analysis was used to evaluate the association between the BD mechanism and the first occurrence of endpoints during follow-up. Covariates included in the multivariate models were identified using the best subset procedure among variables that were predictive of the endpoint and were unbalanced between the two groups; candidate covariates are listed in Tables 1 and 2. Due to significant differences between groups, the following variables were statistically controlled in further analyses: donor’s age and height, hospitalization length, cardiopulmonary resuscitation and hemodynamics on presentation.
To validate our findings, we calculated a propensity score using binary logistic regression. We included the covariates that were found to be significantly different according to Tables 1, 2, 3 (donor’s age, hospitalization length, cardio-pulmonary resuscitation and blood pressure on admission). Data were analyzed with SPSS software version 23. A two-sided 0.05 significance level was used for hypothesis testing.
Results
Patient characteristics and early results
The current analysis was based on 190 patients, who were classified into two groups according to donor’s BD mechanism: TBD (n = 105) and NTBD (n = 85). Baseline clinical characteristics of the study patients by donor’s BD mechanism are shown in Table 1. Recipients’ baseline characteristics were similar in the two groups in terms of age, gender, pre-existing cardiovascular risk factors and hemodynamics prior to the HTx. Donors’ characteristics, according to TBD and NTBD, are shown in Table 2. For both TBD and NTBD groups, donors were younger than recipients and most were males. Donors of the TBD group were 10 years younger than those in the NTBD group, and were characterized by shorter hospitalization prior to donation, shorter brain injury interval until BD determination, reduced incidence of cardio-pulmonic resuscitation, and lower blood pressure on admission. Early in-hospital outcomes were similar between the TBD and NTBD groups, respectively, as follows: in-hospital mortality 15.2 vs. 18.2%, p = 0.102; PGD 20.2 vs. 21.5%, p = 0.842; and length of hospitalization 21.8 ± 14.2 vs. 23.1 ± 7.6 days, p = 0.721 (Table 3). The average follow-up of the groups was similar.
Mortality
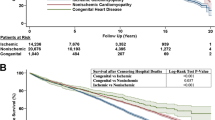
Kaplan-Meier survival analysis showed that overall survival was significantly higher for the TBD vs. the NTBD group: At 10 years of follow-up, the rates of survival were 58.1% in the TBD group and 37.6% in the NTBD group (log-rank p-value = 0.044 for the comparison between the two groups during follow-up) (Fig. 1). Consistently, multivariate analysis showed that TBD was independently associated with a significant 43% reduction in mortality [hazard ratio (HR) = 0.57, 95% confidence interval (CI) 0.42–0.75, p = 0.033; Table 4]. These findings were further validated by propensity score analysis (HR = 0.58, 95% CI 0.44–0.77, p = 0.050, Table 4). In addition, it was found that higher donor blood pressure on admission was associated with lower recipient mortality (Systolic: HR = 0.97, 95% CI 0.92–0.98, p = 0.042; Diastolic: HR = 0.94, 95% CI 0.89–0.96, p = 0.029).

Kaplan–Meier curve of survival by traumatic vs. non-traumatic brain death
Rejections, CAV and NF-MACE
Recipients of hearts from TBD donors had lower TRS (reflecting the severity of rejection) and ARS (representing the total number of rejections, regardless of severity) than recipients from NTBD donors (TRS: 0.44 ± 0.32 vs. 0.51 ± 0.39, respectively, p = 0.040; ARS: 0.38 ± 0.26 vs. 0.45 ± 0.31, respectively, p = 0.030). Kaplan-Meier analysis showed that freedom from CAV was significantly higher in recipients of TBD hearts compared with recipients of NTBD organs (10 years: 82.9 vs. 62.4%, log-rank p-value = 0.024; Fig. 2). Consistently, multivariate analysis showed that TBD was independently associated with a significant 42% reduction in CAV (HR = 0.58, 95% CI 0.51–0.85, p = 0.022; Table 5). These findings were further validated by propensity score analysis (HR = 0.57, 95% CI 0.51–0.81, p = 0.025; Table 5). There was no significant difference in 10-year freedom from NF-MACE between the groups (22.9 vs. 27.1%, log rank p = 0.553, for TBD vs. NTBD, respectively).

Kaplan–Meier curve of CAV-free survival by traumatic vs. non-traumatic brain death
Discussion
It has been postulated that the “ideal” donor would be a young healthy individual with no pre-existing comorbidities who died as a result of an isolated head trauma [20]. Nonetheless, animal and human post-mortem studies focusing on brain death due to a rapid increase in intracranial pressure have not provided unequivocal validation of this premise [9, 21,22,23]. An analysis of our results, which serve to expand the limited and somewhat scattered literature regarding the effect of mode of donor BD on outcomes of HTx patients, reveals some new – and at times controversial – findings, as discussed below. In summary, we showed that: 1) late mortality is affected by the mechanism of donor BD, with a survival advantage for recipients from TBD donors; 2) TRS and ARS are influenced by donor events that precede the actual engraftment process and are negatively affected by NTBD; 3) the incidence of CAV is significantly lower in recipients of TBD donors; and 4) early outcomes, including PGD and in-hospital mortality, are not influenced by the mechanism of donor BD.
A review of the general transplantation literature reveals that graft function is inferior in kidney transplants from BD donors compared with live donors [24, 25]. Similarly, heart recipients from live donors (domino hearts) show decreased incidence and severity of transplant-associated coronary artery disease compared with recipients from dead donors [26]. BD induces significant systemic derangements, including hemodynamic instability and the release of proinflammatory cytokines, causing significant injury to the organ to be transplanted before procurement. BD also causes a rise in serum catecholamines, which may result in coronary vasoconstriction and myocardial ischemia. In addition, a spinal shock phase may occur, resulting in severe hypotension and hence requiring the use of inotropes and vasopressors to maintain organ perfusion [27, 28]. Indeed, regardless of the BD mechanism, most of the donors in this study were supported with inotropes, with approximately 40% being supported by combination of more than two inotropes. The types and doses of inotropes and hormones were similar, irrespective of the cause of BD, and the resulting systolic and diastolic blood pressures were similar prior to procurement, despite the facts that NTBD donors presented with higher systolic and diastolic blood pressure on admission and cardiopulmonary resuscitation (CPR) was necessitated for more patients of this group.
In the current study, we showed a survival advantage and a lower incidence of CAV for recipients from TBD donors. Our results thus appear to contradict the seminal pioneering study of Mehra et al. [6], who evaluated, by intravascular ultrasound (IVUS), the coronary arteries of 61 consecutive HTx recipients between 1993 and 1995, according to ‘explosive’ (equivalent to ‘traumatic’ in our study) vs ‘non-explosive’ BD donors. They showed that HTx recipients with allografts from explosive BD donors demonstrated increased maximal intimal thickness of the arteries and more cardiac events and hence lower survival. Their IVUS study was performed at an average of 2.4 years post HTx, with a follow up of an average of 4 years after the index ultrasound. In our study, CAV assessment in did not include IVUS, so we are not able to make a direct comparison. Moreover, in our study, the survival curves diverged after more than 2 years, with more than 90% of the recipients of TBD hearts currently being treated with statins and having an average LDL of 111 mg/dl (vs 30% and 140 mg/dl, respectively, in the study of Mehra et al. [6]). In general, comparisons are problematic because patient and donor characteristics are significantly different among various studies in terms of ischemic time, donor age, and immunosuppressive protocols. Nonetheless, the findings of the current study complement those of similar studies reporting major discoveries and significant progress in the field [29, 30].
The importance of the nature of the donor brain injury lies in its effect on the donor heart. Traumatic injury to the brain is accompanied by an acute increase in intracranial pressure, which was shown in experimental models to produce more severe hemodynamic alterations and myocardial collapse than other modes of brain injury (due to a steeper rise in epinephrine levels and irreversible myocardial damage secondary to catecholamine-mediated toxicity) [21, 31,32,33,34]. In contrast, it had previously been shown that despite BD-associated hemodynamic deterioration in vivo, after explantation and ex vivo assessment, the myocardial function of hearts removed from BD and sham-operated dogs was not significantly different [35]. In an in situ isolated perfused heart model, it was demonstrated that if coronary perfusion pressure was de-coupled from aortic pressure and elevated to pre-brain death levels, coronary blood flow and myocardial contractility were also restored to baseline levels [36]. The above findings imply that cardiac dysfunction after BD is reversible and that changes in donor myocardial function may reflect altered loading conditions and coronary perfusion rather than irreversible injury due to an initial Cushing-type reaction and subsequent hormone depletion. Thus, it has been suggested that donor hearts should be carefully evaluated by load-independent indices of cardiac function and that the normalization of loading conditions in the BD donor may lead to an improvement of cardiac performance. An increasing number of clinical studies have indeed demonstrated that cardiac dysfunction can be reversed in potential organ donors and that the clinical outcome of transplant patients receiving hearts from primary marginal donors is comparable to those of normal donors [35,36,37,38]. Our results are in accord with these findings.
Mode of brain death significantly impacts long term HTx outcomes, while early outcomes, including PGD and in-hospital mortality, are not influenced by the mechanism of donor BD. Brain death leads to dramatic changes in loading conditions in a decrease of contractile function via the Arnep and garden-hose effects as well as the Frank-Starling mechanism [38,39,40]. These physiologic regulatory mechanisms give a plausible explanation for decreased cardiac function, without the necessity of irreversible tissue damage or “true” dysfunction. However, early abnormalities (i.e. abnormal plasma catecholamines values and intracellular calcium handling) may eventually lead to endothelial damage, a primary precipitating event in CAV pathogenesis, a major cause of long-term mortality following HTx.
The impressive advance in mechanical circulatory support devices has not yet resulted in a true alternative to HTx. Thus, while HTx will continue to be the gold standard treatment for end-stage heart failure and donors will continue to change in terms of causes of BD toward a non-traumatic etiology [4], HTx surgery will continue to be significantly more challenging with longer and more complex surgeries and increased ischemia times for organs that were previously considered to be borderline or non-transplantable. Nonetheless, despite the increasing complexity of recipients and donors, results of HTx have improved progressively. It is therefore of particular importance to continue research aimed at defining and characterizing the factors that may affect the results of HTx. Once we will have defined the factors associated with less favourable outcomes, the next step will be to find the correct donor-recipient matching parameter that will neutralize the negative influence in the most significant way. An example is a study showing that differences in donor–recipient predicted heart mass modulated the survival associated with donor–recipient sex mismatch [41]. Redistributing organs to recipients most likely to derive maximal benefit will result in expanded organ allocation potential, underscoring the importance of the current study. It is our hope that our findings will contribute to targeting novel strategies aiming to optimize graft preservation, including donation after circulatory determined death and ex-vivo perfusion of hearts [42].
Study limitations
The major limitation of our study lies in its observational nature. Not all possible confounders were recorded or adjusted for this single-center study with relatively small sample size. No measurements of specific biological markers of BD in the donors were made. Therefore, we could not evaluate objectively the extent of the brain damage and the correlation with recipient outcomes.
Conclusions
The modality of donor BD significantly influences long-term outcomes after HTx: TBD is associated with reduced mortality, CAV, and a lower rejection score. The mode of BD does not affect early HTx outcomes, including PGD and in-hospital mortality. We conclude by emphasizing that the results of our study do not argue against utilizing NTBD donors but rather represent opportunities for greater utilization of these donors. Survival prediction models should incorporate the BD mechanism with the aim to further optimize matching of donor and recipient. Additional prospective studies are warranted to better delineate the pathophysiologic consequences of BD. The effects of donor and recipient treatment protocols in addition to organ-specific aspects of injury and repair still need to be assessed.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ARS:
-
Any rejection score
- BD:
-
Brain death
- CAV:
-
Cardiac allograft vasculopathy
- CI:
-
Confidence interval
- CPR:
-
Cardiopulmonary resuscitation
- EMB:
-
Endomyocardial biopsy
- HR:
-
Hazard ratio
- HTx:
-
Heart transplantation
- ISHLT:
-
International Society of Heart and Lung Transplantation
- IVUS:
-
Intravascular ultrasound
- NF-MACE:
-
Non-fatal major adverse cardiac events
- NTBD:
-
Non-traumatic brain death
- PGD:
-
Primary graft dysfunction
- TBD:
-
Traumatic brain death
- TRS:
-
Total rejection score
References
Khush KK, Zaroff JG, Nguyen J, Menza R, Goldstein BA. National decline in donor heart utilization with regional variability: 1995-2010. Am J Transplant. 2015;15:642–9.
O'Neill TJ 4th, Pisani B. Size matching in heart transplantation donor selection: “too big to fail”? J Heart Lung Transplant. 2017;36:934–5.
Nativi JN, Brown RN, Taylor DO, Kfoury AG, Kirklin JK, Stehlik J, et al. Temporal trends in heart transplantation from high-risk donors: are there lessons to be learned? A multi-institutional analysis. J Heart Lung Transplant. 2010;29:847–52.
Peris A, Lazzeri C, D'Antonio L, Bombardi M, Bonizzoli M, Guetti C, et al. Epidemiological changes in potential heart donors after brain death: a retrospective 15 year cohort study. Intern Emerg Med. 2018;14(3):371–5.
Urban M, Booth K, Schueler S, Netuka I, MacGowan G. Donor and recipient risk factor analysis of inferior postheart transplantation outcome in the era of durable mechanical assist devices. Clin Transpl. 2018;32:e13390.
Mehra MR, Uber PA, Ventura HO, Scott RL, Park MH. The impact of mode of donor brain death on cardiac allograft vasculopathy: an intravascular ultrasound study. J Am Coll Cardiol. 2004;43:806–10.
Cohen O, De La Zerda DJ, Beygui R, Hekmat D, Laks H. Donor brain death mechanisms and outcomes after heart transplantation. Transplant Proc. 2007;39:2964–9.
Taylor DO, Edwards LB, Mohacsi PJ, Boucek MM, Trulock EP, Keck BM, et al. The registry of the International Society for Heart and Lung Transplantation: twentieth official adult heart transplant report--2003. J Heart Lung Transplant. 2003;22:616–24.
Pratschke J, Wilhelm MJ, Kusaka M, Basker M, Cooper DK, Hancock WW, et al. Brain death and its influence on donor organ quality and outcome after transplantation. Transplantation. 1999;67:343–8.
Plenz G, Eschert H, Erren M, Wichter T, Böhm M, Flesch M, et al. The interleukin-6/interleukin-6-receptor system is activated in donor hearts. J Am Coll Cardiol. 2002;39:1508–12.
Salim A, Martin M, Brown C, Belzberg H, Rhee P, Demetriades D. Complications of brain death: frequency and impact on organ retrieval. Am Surg. 2006;72:377–81.
Kramer AH, Baht R, Doig CJ. Time trends in organ donation after neurologic determination of death: a cohort study. CMAJ Open. 2017;5:E19–27.
Callahan DS, Kim D, Bricker S, Neville A, Putnam B, Smith J, et al. Trends in organ donor management: 2002 to 2012. J Am Coll Surg. 2014;219:752–6.
Desschans B. Evrard P; coordinator transplant section of the Belgian transplant society. Organ donation and transplantation statistics in Belgium for 2012 and 2013. Transplant Proc. 2014;46:3124–6.
Saidi RF, Markmann JF, Jabbour N, Li Y, Shah SA, Cosimi AB, et al. The faltering solid organ donor pool in the United States (2001-2010). World J Surg. 2012;36:2909–13.
Stewart S, Winters GL, Fishbein MC, Tazelaar HD, Kobashigawa J, Abrams J, et al. Revision of the 1990 working formulation for the standardization of nomenclature in the diagnosis of heart rejection. J Heart Lung Transplant. 2005;24:1710–20.
Raichlin E, Edwards BS, Kremers WK, Clavell AL, Rodeheffer RJ, Frantz RP, et al. Acute cellular rejection and the subsequent development of allograft vasculopathy after cardiac transplantation. J Heart Lung Transplant. 2009;28:320–7.
Mehra MR, Crespo-Leiro MG, Dipchand A, Ensminger SM, Hiemann NE, Kobashigawa JA, et al. International Society for Heart and Lung Transplantation working formulation of a standardized nomenclature for cardiac allograft vasculopathy-2010. J Heart Lung Transplant. 2010;29:717–27.
Kobashigawa J, Zuckermann A, Macdonald P, Leprince P, Esmailian F, Luu M, et al. Report from a consensus conference on primary graft dysfunction after cardiac transplantation. J Heart Lung Transplant. 2014;33:327–40.
Singhal AK, Sheng X, Drakos SG, Stehlik J. Impact of donor cause of death on transplant outcomes: UNOS registry analysis. Transplant Proc. 2009;41:3539–44.
Shivalkar B, Van Loon J, Wieland W, Tjandra-Maga TB, Borgers M, Plets C, et al. Variable effects of explosive or gradual increase of intracranial pressure on myocardial structure and function. Circulation. 1993;87:230–9.
Tsai FC, Marelli D, Bresson J, Gjertson D, Kermani R, Patel J, et al. Use of hearts transplanted from donors with atraumatic intracranial bleeds. J Heart Lung Transplant. 2002;21:623–8.
Mehra MR, Prasad A, Uber PA, Park M. The impact of explosive brain death on the genesis of cardiac allograft vasculopathy: an intravascular ultrasound study. J Heart Lung Transplant. 1999;18(1):49.
Chudoba P, Krajewski W, Wojciechowska J, Kamińska D. Brain death-associated pathological events and therapeutic options. Adv Clin Exp Med. 2017;26:1457–64.
Zens TJ, Danobeitia JS, Leverson G, Chlebeck PJ, Zitur LJ, Redfield RR, et al. The impact of kidney donor profile index on delayed graft function and transplant outcomes: a single-center analysis. Clin Transpl. 2018;32:e13190.
Anyanwu AC, Banner NR, Mitchell AG, Khaghani A, Yacoub MH. Low incidence and severity of transplant-associated coronary artery disease in heart transplants from live donors. J Heart Lung Transplant. 2003;22:281–6.
Ullah S, Zabala L, Watkins B, Schmitz ML. Cardiac organ donor management. Perfusion. 2006;21:93–8.
Balsam B, Robbins RC. Current trends in heart transplantation. Scand J Surg. 2007;96:125–30.
Kobashigawa JA, Katznelson S, Laks H, Johnson JA, Yeatman L, Wang XM, et al. Effect of pravastatin on outcomes after cardiac transplantation. N Engl J Med. 1995;333:621–7.
Costanzo MR, Dipchand A, Starling R, Anderson A, Chan M, Desai S, et al. International Society of Heart and Lung Transplantation Guidelines. The International Society of Heart and Lung Transplantation Guidelines for the care of heart transplant recipients. J Heart Lung Transplant. 2010;29:914–56.
Takada M, Nadeau KC, Hancock WW, Mackenzie HS, Shaw GD, Waaga AM, et al. Effects of explosive brain death on cytokine activation of peripheral organs in the rat. Transplantation. 1998;65:1533–42.
Busson M, N'Doye. P, Benoit G, Hannoun L, Adam R, Pavie A, et al. Donor factors influencing organ transplant prognosis. Transplant Proc. 1995;27:1662–4.
Powner DJ, Hendrich A, Nyhuis A, Strate R. Changes in serum catecholamine levels in patients who are brain dead. J Heart Lung Transplant. 1992;11:1046–53.
Ciccone AM, Stewart KC, Meyers BF, Guthrie TJ, Battafarano RJ, Trulock EP, et al. Does donor cause of death affect the outcome of lung transplantation? J Thorac Cardiovasc Surg. 2002;123:429–34 discussion 434-6.
Szabó G, Sebening C, Hackert T, Hagl C, Tochtermann U, Vahl CF, et al. Effects of brain death on myocardial function and ischemic tolerance of potential donor hearts. J Heart Lung Transplant. 1998;17:921–30.
Szabó G, Hackert T, Sebening C, Vahl CF, Hagl S. Modulation of coronary perfusion pressure can reverse myocardial dysfunction after brain death. Ann Thorac Surg. 1999;67:18–25.
Wheeldon DR, Potter CD, Oduro A, Wallwork J, Large S. Transforming the “unacceptable” donor: outcomes from the adoption of standardized donor management technique. J Heart Lung Transplant. 1995;14:734–42.
Szabó G. Physiologic changes after brain death. J Heart Lung Transplant. 2004;23:S223–6.
Asanoi H, Ishizaka S, Kameyama T, Sasayama S. Neural modulation of ventriculoarterial coupling in conscious dogs. Am J Phys. 1994;266:H741–8.
Klautz RJ, Teitel DF, Steendijk P, van Bel F, Baan J. Interaction between afterload and contractility in the newborn heart: evidence of homeometric autoregulation in the intact circulation. J Am Coll Cardiol. 1995;25:1428–35.
Reed RM, Netzer G, Hunsicker L, Mitchell BD, Rajagopal K, Scharf S, Eberlein M. Cardiac size and sex-matching in heart transplantation: size matters in matters of sex and the heart. JACC Heart Fail. 2014;2:73–83.
Ardehali A, Esmailian F, Deng M, Soltesz E, Hsich E, Naka Y, et al. Ex-vivo perfusion of donor hearts for human heart transplantation (PROCEED II): a prospective, open-label, multicentre, randomised non-inferiority trial. Lancet. 2015;385:2577–84.
Acknowledgements
Not applicable.
Author information
Authors and Affiliations
Contributions
ER analyzed and interpreted the patient data and wrote the research project and the full manuscript. JL performed study revision and editing. DF performed study revision and editing. EM performed data collection and interpretation. YK performed study revision and editing. LS performed study revision and editing. AK performed study revision and editing. YP analyzed and interpreted the data and wrote the full manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Sheba Medical Center Institutional Ethical Committee (Protocol No 4257).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Ram, E., Lavee, J., Freimark, D. et al. Improved long-term outcomes after heart transplantation utilizing donors with a traumatic mode of brain death. J Cardiothorac Surg 14, 138 (2019). https://doi.org/10.1186/s13019-019-0963-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13019-019-0963-2