
Abstract
Background
Osteoporosis with pathological fractures is a significant public health issue, contributing to morbidity, disability, diminished quality of life, and increased mortality. Understanding mortality trends related to this condition is crucial for developing effective interventions to reduce mortality and improve healthcare outcomes. This study aimed to analyze trends and causes of death associated with osteoporosis and pathological fractures in the United States using a multi-cause approach.
Methods
Annual death and age-standardized mortality rate (ASMR) data from 1999 to 2020 were obtained from the Centers for Disease Control and Prevention (CDC) mortality database. Death certificates listing ICD-10 M82 (osteoporosis with pathological fracture) as an underlying or related cause of death were analyzed. Epidemiological data were analyzed, and the ASMR data were calculated for each year, and trends were assessed using the Cochran-Armitage trend test.
Results
From 1999 to 2020, there were 40,441 deaths related to osteoporosis with pathological fractures in the United States, with a female-to-male ratio of 5.6:1. Among these, 12,820 deaths (31.7%) listed osteoporosis with pathological fractures as the underlying cause of death (UCD), yielding a female-to-male ASMR ratio of approximately 5.0-7.7:1. When classified as a non-UCD, the ASMR ratio was approximately 4.8–6.2:1. At the same time, we found that the total number of deaths classified as UCD and multiple causes of death (MCD), but the trend ratio of the two groups in different years did not change statistically significant (P > 0.05), and the ASMR of both groups showed a downward trend. The UCD-to-MCD ratio increased between 1999 and 2007, then decreased from 2007 to 2020. As MCD, the number of female deaths was more than that of male, and both showed a decreasing trend, but there was no statistical significance in the change of trend ratio in different years (P > 0.05). Deaths were predominantly concentrated in individuals over 75 years of age, with those over 84 years being the most affected. The number of deaths in different age groups showed a decreasing trend, and the change of trend ratio in different years was statistically significant (P < 0.05). White individuals had the highest number of deaths. The leading causes of death were heart diseases, chronic lower respiratory diseases, and alzheimer’s disease. In addition, the number of deaths of patients with prostate cancer and breast cancer showed a significant downward trend, and the change of trend ratio between the two groups in different years was statistically significant (P < 0.05).
Conclusions
Although mortality from osteoporosis with pathological fractures is decreasing, anti-osteoporosis therapy remains essential for elderly patients. Healthcare providers should remain vigilant for potential complications, including malignant neoplasms, and ensure timely diagnosis and treatment to further reduce mortality in this population.
Similar content being viewed by others


Background
Osteoporosis is a systemic bone disease characterized by low bone mass, deterioration of bone tissue microstructure, increased bone fragility, and a heightened susceptibility to fractures [1]. It is a serious, chronic, progressive, and clinically asymptomatic condition, and it is the most common metabolic bone disease [2]. Osteoporosis is more prevalent in the elderly, typically affecting men over 65 years of age and women over 55 years of age [3, 4]. The overall prevalence of osteoporosis is approximately 20% [5], with a global prevalence of about 12% in men and 23% in women [6, 7].
Starting at the age of 50, one in three women and one in five men will experience an osteoporotic fracture [4]. In 2000, there were an estimated 9 million new osteoporotic fractures worldwide, including 1.7 million forearm fractures, 1.4 million clinical vertebral fractures, and 1.6 million hip fractures [8]. Fragility fractures of the spine and hip are associated with an increased risk of mortality [9]. Studies have shown that the one-year mortality rate for older adults with osteoporotic fractures is approximately 15% for women and 22% for men. By 2009, the annual mortality rate had decreased to 11.2% for women and 18% for men, and by 2010, it had further declined to 2.8% for women and 3.6% for men [10]. However, the number of deaths related to osteoporosis and pathological fractures, as well as the trend in age-standardized mortality rates (ASMR) in the United States, remain unclear.
Cancer and cardiovascular disease are the leading causes of death among the elderly, and when osteoporosis is combined with pathological fractures, the risk of death increases [11]. However, the underlying cause of death in cases of osteoporosis with pathological fractures and the sequence of events leading to death remain unclear. Additionally, bone metastasis occurs in 65–90% of prostate cancer cases and 65–75% of breast cancer cases [12, 13]. Bone involvement is less common in other malignancies, ranging from approximately 10% in colorectal cancer to 17–64% in lung cancer [12, 13]. Bone metastasis is a major risk factor for bone loss and fractures [14]. This is attributable both to the direct effects of cancer cells on bone and the detrimental effects of cancer-specific therapies on bone cells [15]. Bone is also the most common site of metastasis, leading to bone destruction and the formation of pathological fractures [16]. In recent years, the mortality trends for osteoporosis combined with pathological fractures in the context of breast and prostate cancer remain unclear, warranting further investigation.
Therefore, this study aimed to describe the mortality associated with osteoporosis and pathological fractures, as well as to identify the leading causes of death, using multiple cause-of-death data from Centers for Disease Control and Prevention (CDC) death certificates spanning the past 22 years.
Methods
Using a multi-cause approach, we extracted annual mortality data (1999–2020) from the CDC mortality database, selecting all deaths associated with osteoporosis and pathological fractures (International Classification of Diseases and Related Health Problems, Tenth Revision [ICD-10] category M80: osteoporosis with pathological fracture). These cases were identified when osteoporosis with pathological fracture was listed as a cause of death on any line or in any part of the International Medical Certificate of Cause of Death (the medical certificate section of the death certificate) [17]. The underlying cause (Part I of the medical certificate section) and complications or contributing causes (Part II of the medical certificate section) were collectively designated as related (non-underlying) causes of death.
According to the ICD-10, osteoporosis with pathological fractures as a cause of death includes the following subcategory codes: M80.0 (postmenopausal osteoporosis with pathological fracture), M80.1 (postoophorectomy osteoporosis with pathological fracture), M80.2 (osteoporosis of disuse with pathological fracture), M80.3 (postsurgical malabsorption osteoporosis with pathological fracture), M80.4 (drug-induced osteoporosis with pathological fracture), M80.5 (idiopathic osteoporosis with pathological fracture), M80.8 (other osteoporosis with pathological fracture), and M80.9 (unspecified osteoporosis with pathological fracture). Additional comorbidities considered include subcategory codes C50 (malignant neoplasm of the breast) and C61 (malignant neoplasm of the prostate).
We analyzed mortality, proportions, and historical trends to examine the distribution of the following variables: sex, age at death (categorized as < 65 years, 65–74 years, 75–84 years, and > 84 years), race, year of death, underlying cause of death, total contribution from each cause of death, and deaths from combined malignancies.
To identify relevant causes listed on the death certificate as contributing to death, we compiled a comprehensive list of commonly associated and frequently mentioned causes. The number of causes of death was categorized according to the range of ICD-10 classifications (subcategories, categories, blocks, and sections). We exported all causes of death into a table and filtered them by “subcategories, categories, blocks, and chapters” to determine their inclusion as causes of death. Deaths resulting from osteoporosis and pathological fractures were not counted in the total number of causes of death. If two or more causes listed in the medical certificate section fell within the same category, only one was recorded according to the ICD-10 category code. This approach prevented the duplication of causes, as presented in the summary table.
We calculated annual deaths from osteoporosis with pathological fractures and ASMR per 100,000 population. Mortality for the entire study period (1999–2020) was determined based on the number of deaths identified as the underlying or related cause and the total number of cited cases.
Data analysis was conducted using SPSS 26.0 (IBM, Armonk, New York, USA), and graphical representations were created using Graphpad Prism 8.0. The Cochran-Armitage trend test was used to assess trends across different years. A p-value of < 0.05 was considered statistically significant, and all tests were conducted in a two-sided manner.
Results
In the United States, 6,746,356,647 deaths were recorded between 1999 and 2020, of which 40,441 were related to osteoporosis with pathological fractures. Among these, 34,334 (84.9%) were women and 6,107 (15.1%) were men, resulting in a female-to-male ratio of approximately 5.6:1 (Table 1). When classified as the underlying cause of death (UCD), there were 12,820 deaths (31.7%), with a female-to-male ASMR ratio (per 100,000 population) of approximately 5.0-7.7:1 (Table 1). When classified as a non-UCD, the number of deaths was 27,621 (68.3%), with the ASMR (per 100,000 population) for women and men being approximately 4.8–6.2:1 (Table 1). Additionally, we observed a downward trend in the total number of deaths classified as UCD and multiple causes of death (MCD). However, there was no statistically significant change in the trend ratio between the two groups across different years (p > 0.05) (Fig. 1). The ASMR for both groups also showed a downward trend. The ratio of UCD to MCD exhibited an increasing trend from 1999 to 2007, followed by a decreasing trend from 2007 to 2020 (Table 2).

Trends in the overall number of UCD and MCD deaths
When osteoporosis combined with pathological fracture was considered as a MCD, the number of deaths was higher in females than in males, with both showing a decreasing trend. This decline was more pronounced in females; however, the trend ratio between the two groups across different years was not statistically significant (p > 0.05) (Fig. 2). In terms of mortality, the ASMR was significantly higher in women than in men, and both sexes exhibited a downward trend, and this decline was more pronounced in women than in men (Fig. 3).

Deaths by gender in the US from 1999 to 2020

ASMR by gender in the US from 1999 to 2020
Regarding the number of deaths by age group, the majority of deaths occurred in patients over 75 years of age, with those over 84 years of age being the most affected (Table 1). Across all age groups, there was a downward trend in the number of deaths, with the trend ratio showing statistical significance over different years (p < 0.05). The decline was observed year by year, and the older the age group, the more rapid the decrease (Fig. 4). In terms of race, the highest number of deaths occurred among White individuals, accounting for 39,090 deaths (96.7% of the total), This was followed by Asian or Pacific Islanders with 624 deaths (1.5%), Black or African Americans with 587 deaths (1.5%), and American Indian or Alaska Native individuals with 140 deaths (0.3%).

The number of deaths in different age groups
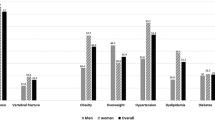
The UCD over the 22-year study period, ranked in descending order by the total number of mentions, are presented in Table 3. Diseases of the heart were the leading cause of death, followed by chronic lower respiratory diseases and alzheimer’s disease.
Our study also found that between 1999 and 2020, when osteoporosis combined with pathological fracture was associated with malignant tumors as an MCD, the number of deaths in patients with prostate cancer and breast cancer was 329 and 813, respectively. The trend ratio between these two groups across different years was statistically significant (p < 0.05). However, the overall trend showed a decline, with the downward trend being more pronounced when prostate cancer was involved (Fig. 5).

The number of deaths from different comorbidities
Discussion
The results of this study show that from 1999 to 2020, the number of deaths from osteoporosis combined with pathological fractures was consistently higher in women than in men, with a mortality ratio of approximately 5.5:1. This higher number of deaths among women is associated with their higher morbidity rates. Generally, the incidence of fractures in women is nearly double that of men, with approximately 75% of such cases occurring in women [18]. Men have a lower risk of osteoporosis and fragility fractures than women, due to factors such as smaller bone diameters, lower peak bone mass, the bone resorption processes associated with menopause, and a higher risk of falls in women [19]. In the United States, 2 million osteoporotic fractures occur annually (71% in women and 29% in men) [20]. Our study also found that the ASMR was consistently higher in women than in men. However, previous studies have shown that men experience more osteoporosis-related complications and have higher mortality rates after osteoporotic fractures than women [21,22,23]. For instance, a 10-year study in Australia reported that the mortality rate after low-grade trauma fractures was 48% for women and 57% for men [24]. The reasons for the higher mortality rate in men are not entirely clear, but a higher risk of infection among males may be a contributing factor [25]. This discrepancy with our findings suggests the need for further investigation. Additionally, our study observed a downward trend in the annual mortality rate among elderly individuals with osteoporosis and pathological fractures starting in 1999 for both women and men [26]. This is generally consistent with our results, which showed a declining trend in ASMR in both sexes.
When osteoporosis with pathological fracture was considered either as an UCD or MCD, the number of deaths showed a decreasing trend. Moreover, the ratio of UCD to MCD also decline in the later stages, which may be attributed to the early diagnosis of osteoporosis through bone density screening and the timely treatment provided by clinicians [19]. Furthermore, the incidence of vertebral fractures in women begins to increase around the age of 60 and accelerates significantly after the age of 80. The incidence of hip fractures in women rises sharply after the age of 70 and peaks after the age of 80 [4]. For men, a Norwegian study reported that the incidence of hip fractures was 0.49 per 1000 person-years in men aged 60 and 12.3 per 1000 person-years in men aged 85 [27]. This indicates that osteoporosis and pathological fractures begin to rise sharply after the age of 70 and reach a peak after the age of 80. The spike in morbidity is likely closely related to the number of deaths, which, according to our findings, are predominantly concentrated in patients over 75 years of age, with those over 84 years of age being the most affected. Concurrently, we observed a downward trend in the number of deaths across all age groups, which may be linked to early diagnosis and the use of anti-osteoporosis medications [23, 28]. In our study, the highest number of deaths by race occurred among White individuals, which aligns with previous studies indicating the incidence of osteoporosis is approximately 50% among White individuals, compared to 38% and 39% among Hispanics and African Americans, respectively. A prospective study of 159,579 women aged 50 to 79 years found that White individuals (2%) and Native Americans (2%) had the highest annualized fracture rates, followed by Hispanics (1.3%), Asians (1.2%), and African Americans (0.9%) [29, 30]. The incidence of osteoporosis with pathological fractures was highest among White women (140.7 per 100,000), followed by Asian women (85.4 per 100,000), African American women (57.3 per 100,000), and Hispanic women (49.7 per 100,000) [31]. This corresponds to the higher number of deaths observed among White individuals in our study.
Osteoporosis with pathological fractures is closely associated with increased mortality, particularly in the period following the fracture event [32]. Osteoporotic fractures, especially hip fractures, are often precipitated by falls, leading to a high risk of complications and rapid health deterioration. In fact, a significant proportion (53.8%) of early deaths (within 30 days) following a hip fracture are attributed to accidents involving injury, which are identified as the UCD—these are events that trigger a cascade of morbid events directly leading to death. This underlying cause of death remains prominent in the months following the fracture, accounting for about a quarter of all deaths within a year after the incident. In the later stages, circulatory diseases (particularly cardiovascular diseases) became the leading cause of death, followed by tumors, respiratory diseases, mental and behavioral disorders, and diseases of the nervous system and sensory organs [33]. A Swedish study corroborates these findings, identifying cardiovascular disease, cancer, and pneumonia as the leading causes of death [34]. Consistent with previous studies, our study found that the leading cause of death was heart disease. However, our findings differed slightly in that respiratory diseases, neurological diseases, and tumors followed in descending order as causes of death, which contrasts with some earlier studies and suggests the need for further research to confirm these trends.
The occurrence and treatment of bone metastases in malignant tumors, particularly breast and prostate cancer, can exacerbate bone loss and increase the incidence of osteoporosis and osteoporotic fractures [35]. Osteoporosis with pathological fractures is a significant concern for survivors of breast and prostate cancer and can severely impact patient quality of life. However, the risk of low bone density varies among individuals. For instance, lumbar bone mineral density (BMD) and total hip BMD decrease by 2.76% and 4.27%, respectively, in breast cancer patients treated with tamoxifen, which is associated with an increased risk of fractures [36]. Additionally, other adjuvant treatments can raise the risk of fractures by 34% over 2.5 to 5 years [37]. Regarding prostate cancer, a cohort study of 179,744 Swedish men revealed that the use of androgen deprivation therapy was associated with a higher incidence of fractures, including hip fractures [38]. Despite the significantly increased risk of fractures and mortality in patients with breast and prostate cancer, our study found a decrease in the number of deaths over the past 22 years. This reduction may be related to the early detection of osteoporotic fractures through modern risk assessment tools, such as bone densitometry and trabecular bone score. Furthermore, early treatment interventions, including calcium and vitamin D supplementation and anti-bone resorption therapy [14], may have contributed to reducing the risk of death from osteoporosis with pathological fractures.
This study re-examined the mortality associated with osteoporosis and pathological fractures over the past 22 years. A key strength of this study is its use of MCD analysis, which allowed for the identification of the maximum possible number of deaths associated with osteoporosis and pathological fractures [39]. By categorizing these conditions as related causes of death, the analysis captured 68.3% of deaths where osteoporosis with pathological fractures was classifies as a contributing factor. The potential underestimation of rheumatic diseases in mortality statistics is attributed to complications such as infections or cardiovascular diseases, which are often identified as the underlying cause of death. This study has certain limitations. First, despite the automated processing of mortality data in the United States the task of coding causes of death is performed by trained professionals who may occasionally introduce errors or incorrect ICD-10 codes. Second, the relatively small number of deaths also precluded subgroup analyses for patients with various complications related to osteoporosis and pathological fractures. Third, relevant missing information on death certificates was not available through this system.
Conclusion
Our study indicates that older women are more frequently affected by mortality related to osteoporosis with pathological fractures compared to men. The number of deaths and mortality rates associated with these conditions has been decreasing and is anticipated to continue this trend in the coming years. Cardiovascular disease remains the primary UCD among patients with osteoporosis with pathological fractures. The observed reduction in mortality is likely attributable to advancements in diagnostic methods and the use of anti-bone resorption therapies. However, management and prevention for osteoporosis with pathological fractures remain inadequate in many countries. Therefore, it is crucial for health services to prioritize addressing mortality associated with osteoporosis and pathological fractures. Developing and implementing strategies for diagnosis and treatment can help mitigate losses and further reduce mortality among patients with these conditions.
Data availability
No datasets were generated or analysed during the current study.
References
Genant HK, Cooper C, Poor G, Reid I, Ehrlich G, Kanis J, et al. Interim report and recommendations of the World Health Organization task-force for osteoporosis. Osteoporos Int. 1999;10(4):259–64. https://doi.org/10.1007/s001980050224
Aibar-Almazán A, Voltes-Martínez A, Castellote-Caballero Y, Afanador-Restrepo DF, Carcelén-Fraile MDC, López-Ruiz E. Current status of the diagnosis and management of osteoporosis. Int J Mol Sci. 2022;23(16):9465. https://doi.org/10.3390/ijms23169465
Cooper C, Campion G, Melton LJ. Hip fractures in the elderly: a world-wide projection. Osteoporos Int. 1992;2(6):285–9. https://doi.org/10.1007/BF01623184
Lorentzon M, Johansson H, Harvey NC, Liu E, Vandenput L, McCloskey EV, et al. Osteoporosis and fractures in women: the burden of disease. Climacteric. 2022;25(1):4–10. https://doi.org/10.1080/13697137.2021.1951206
Chen P, Li Z, Hu Y. Prevalence of osteoporosis in China: a meta-analysis and systematic review. BMC Public Health. 2016;16(1):1039. https://doi.org/10.1186/s12889-016-3712-7
Zamani M, Zamani V, Heidari B, Parsian H, Esmaeilnejad-Ganji SM. Prevalence of osteoporosis with the World Health Organization diagnostic criteria in the Eastern Mediterranean Region: a systematic review and meta-analysis. Arch Osteoporos. 2018;13(1):129. https://doi.org/10.1007/s11657-018-0540-7
Salari N, Ghasemi H, Mohammadi L, Behzadi MH, Rabieenia E, Shohaimi S, et al. The global prevalence of osteoporosis in the world: a comprehensive systematic review and meta-analysis. J Orthop Surg Res. 2021;16(1):609. https://doi.org/10.1186/s13018-021-02772-0
Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17(12):1726–33. https://doi.org/10.1007/s00198-006-0172-4
Ioannidis G, Papaioannou A, Hopman WM, Akhtar-Danesh N, Anastassiades T, Pickard L, et al. Relation between fractures and mortality: results from the Canadian multicentre osteoporosis study. CMAJ. 2009;181(5):265–71. https://doi.org/10.1503/cmaj.081720
Tai TW, Huang CF, Huang HK, Yang RS, Chen JF, Cheng TT, et al. Clinical practice guidelines for the prevention and treatment of osteoporosis in Taiwan: 2022 update. J Formos Med Assoc. 2023;122(Suppl 1):S4–13. https://doi.org/10.1016/j.jfma.2023.01.007
Li CC, Hsu JC, Liang FW, Chang YF, Chiu CJ, Wu CH. The association between osteoporosis medications and lowered all-cause mortality after hip or vertebral fracture in older and oldest-old adults: a nationwide population-based study. Aging. 2022;14(5):2239–51. https://doi.org/10.18632/aging.203927
Venetis K, Piciotti R, Sajjadi E, Invernizzi M, Morganti S, Criscitiello C, et al. Breast cancer with bone metastasis: molecular insights and clinical management. Cells. 2021;10(6):1377. https://doi.org/10.3390/cells10061377
Sousa S, Clézardin P. Bone-targeted therapies in cancer-induced bone disease. Calcif Tissue Int. 2018;102(2):227–50. https://doi.org/10.1007/s00223-017-0353-5
Choi YJ. Cancer treatment-induced bone loss. Korean J Intern Med. 2024;39(5):731–45. https://doi.org/10.3904/kjim.2023.386
Rachner TD, Coleman R, Hadji P, Hofbauer LC. Bone health during endocrine therapy for cancer. Lancet Diabetes Endocrinol. 2018;6(11):901–10. https://doi.org/10.1016/S2213-8587(18)30047-0
Drake MT. Osteoporosis and cancer. Curr Osteoporos Rep. 2013;11(3):163–70. https://doi.org/10.1007/s11914-013-0154-3
Santo AH, Silva-Filho LVRFD. Cystic fibrosis-related mortality trends in Brazil for the 1999–2017 period: a multiple-cause-of-death study. J Bras Pneumol. 2021;47(2):e20200166. https://doi.org/10.36416/1806-3756/e20200166
Jordan KM, Cooper C. Epidemiology of osteoporosis. Best Pract Res Clin Rheumatol. 2002;16(5):795–806. https://doi.org/10.1053/berh.2002.0264
Björnsdottir S, Clarke BL, Mannstadt M, Langdahl BL. Male osteoporosis-what are the causes, diagnostic challenges, and management. Best Pract Res Clin Rheumatol. 2022;36(3):101766. https://doi.org/10.1016/j.berh.2022.101766
Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Min Res. 2007;22(3):465–75. https://doi.org/10.1359/jbmr.061113
Haentjens P, Magaziner J, Colón-Emeric CS, Vanderschueren D, Milisen K, Velkeniers B, et al. Meta-analysis: excess mortality after hip fracture among older women and men. Ann Intern Med. 2010;152(6):380–90. https://doi.org/10.7326/0003-4819-152-6-201003160-00008
Bliuc D, Alarkawi D, Nguyen TV, Eisman JA, Center JR. Risk of subsequent fractures and mortality in elderly women and men with fragility fractures with and without osteoporotic bone density: the Dubbo osteoporosis epidemiology study. J Bone Min Res. 2015;30(4):637–46. https://doi.org/10.1002/jbmr.2393
Rinonapoli G, Ruggiero C, Meccariello L, Bisaccia M, Ceccarini P, Caraffa A. Osteoporosis in men: a review of an underestimated bone condition. Int J Mol Sci. 2021;22(4):2105. https://doi.org/10.3390/ijms22042105
Bliuc D, Nguyen ND, Milch VE, Nguyen TV, Eisman JA, Center JR. Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. JAMA. 2009;301(5):513–21. https://doi.org/10.1001/jama.2009.50
Wehren LE, Hawkes WG, Orwig DL, Hebel JR, Zimmerman SI, Magaziner J. Gender differences in mortality after hip fracture: the role of infection. J Bone Min Res. 2003;18(12):2231–7. https://doi.org/10.1359/jbmr.2003.18.12.2231
Wang CB, Lin CF, Liang WM, Cheng CF, Chang YJ, Wu HC, et al. Excess mortality after hip fracture among the elderly in Taiwan: a nationwide population-based cohort study. Bone. 2013;56(1):147–53. https://doi.org/10.1016/j.bone.2013.05.015
Diamantopoulos AP, Rohde G, Johnsrud I, Skoie IM, Johnsen V, Hochberg M, et al. Incidence rates of fragility hip fracture in middle-aged and elderly men and women in southern Norway. Age Ageing. 2012;41(1):86–92. https://doi.org/10.1093/ageing/afr114
Tai TW, Hwang JS, Li CC, Hsu JC, Chang CW, Wu CH. The impact of various anti-osteoporosis drugs on all-cause mortality after hip fractures: a nationwide population study. J Bone Min Res. 2022;37(8):1520–6. https://doi.org/10.1002/jbmr.4627
Cauley JA, Wu L, Wampler NS, Barnhart JM, Allison M, Chen Z, et al. Clinical risk factors for fractures in multi-ethnic women: the women’s health initiative. J Bone Min Res. 2007;22(11):1816–26. https://doi.org/10.1359/jbmr.070713
Cauley JA. Defining ethnic and racial differences in osteoporosis and fragility fractures. Clin Orthop Relat Res. 2011;469(7):1891–9. https://doi.org/10.1007/s11999-011-1863-5
Silverman SL, Madison RE. Decreased incidence of hip fracture in hispanics, asians, and blacks: California hospital discharge data. Am J Public Health. 1988;78(11):1482–3. https://doi.org/10.2105/ajph.78.11.1482
Katsoulis M, Benetou V, Karapetyan T, Feskanich D, Grodstein F, Pettersson-Kymmer U, et al. Excess mortality after hip fracture in elderly persons from Europe and the USA: the CHANCES project. J Intern Med. 2017;281(3):300–10. https://doi.org/10.1111/joim.12586
Holvik K, Ellingsen CL, Solbakken SM, Finnes TE, Talsnes O, Grimnes G, et al. Cause-specific excess mortality after hip fracture: the Norwegian epidemiologic osteoporosis studies (NOREPOS). BMC Geriatr. 2023;23(1):201. https://doi.org/10.1186/s12877-023-03910-5
von Friesendorff M, McGuigan FE, Wizert A, Rogmark C, Holmberg AH, Woolf AD, et al. Hip fracture, mortality risk, and cause of death over two decades. Osteoporos Int. 2016;27(10):2945–53. https://doi.org/10.1007/s00198-016-3616-5
Bruyère O, Bergmann P, Cavalier E, Gielen E, Goemaere S, Kaufman JM, et al. Skeletal health in breast cancer survivors. Maturitas. 2017;105:78–82. https://doi.org/10.1016/j.maturitas.2017.08.008
Powles TJ, Hickish T, Kanis JA, Tidy A, Ashley S. Effect of tamoxifen on bone mineral density measured by dual-energy x-ray absorptiometry in healthy premenopausal and postmenopausal women. J Clin Oncol. 1996;14(1):78–84. https://doi.org/10.1200/JCO.1996.14.1.78
Goldvaser H, Barnes TA, Šeruga B, Cescon DW, Ocaña A, Ribnikar D, et al. Toxicity of extended adjuvant therapy with aromatase inhibitors in early breast cancer: a systematic review and meta-analysis. J Natl Cancer Inst. 2018;110(1). https://doi.org/10.1093/jnci/djx141
Wallander M, Axelsson KF, Lundh D, Lorentzon M. Patients with prostate cancer and androgen deprivation therapy have increased risk of fractures-a study from the fractures and fall injuries in the elderly cohort (FRAILCO). Osteoporos Int. 2019;30(1):115–25. https://doi.org/10.1007/s00198-018-4722-3
Walsh SJ, DeChello LM. Excess autoimmune disease mortality among school teachers. J Rheumatol. 2001;28(7):1537–45.
Funding
No funding was received for this work.
Author information
Authors and Affiliations
Contributions
RXH, CCW and YTY performed and wrote the manuscript; YY, XCH, DLM and YJH collected the references, designed the table, and drew the figures; XXH and JYL review and proofread manuscripts. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and informed consent
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Huo, R., Wei, C., Huang, X. et al. Mortality associated with osteoporosis and pathological fractures in the United States (1999–2020): a multiple-cause-of-death study. J Orthop Surg Res 19, 568 (2024). https://doi.org/10.1186/s13018-024-05068-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-024-05068-1