
Abstract
Background
Detailed preoperative information is associated with superior outcomes. We aimed to describe the recovery pattern after decompression of central lumbar spinal stenosis (CLSS).
Methods
50 patients aged 51–85 years who underwent decompression without fusion due to CLSS were followed from before to after surgery (post-op day 1, 7, and 14). Back and leg pain were evaluated using the Numeric Rating Scale (NRS; 0 = no pain 0, 10 = worst pain) and quality of life using the EuroQol-5D index (0 = death, 1 = best), and EQ-5D-visual analogue scale (VAS; 0 = worst, 100 = best).
Results
NRS leg pain was reduced from preoperative to first postoperative day by 5.2 (6.1, 4.3) (mean (95%CI)], and NRS back pain from postoperative day 1–7 by 0.6 (1.2, 0.03) and from day 7 to 14 by 0.7 (1.3, 0.2)]. In contrast, EQ-5D index increased from preoperative to first postoperative day by 0.09 (0.06, 0.13) and from day 1 to 7 by 0.05 (0.02,0.08), and EQ-5D VAS from preoperative to first postoperative day by 13.7 (9.1, 18.3) and from day 1 to 7 by 6.0 (2.0, 10.0). After two weeks, 51% of the patients had improved above the minimal clinically important difference (MCID) in back pain and 71% in leg pain.
Conclusions
Patients scheduled for decompression due to CLSS should be informed that improvement in leg pain and quality of life in general can be expected within one day of surgery, that quality of life improves a little further in the first postoperative week, and that back pain improves in the first 2 postoperative weeks. In most patients, decompression without fusion due to CLSS seems to achieve clinically relevant improvement within 2 weeks.
Similar content being viewed by others

Background
There is no generally accepted definition of central lumbar spinal stenosis (CLSS), i.e. spinal canal reduction, and/or this type of anatomic abnormalities. Several different classifications are available [1, 2], with no gold standard [3]. This makes it difficult to compare results from different studies and cohorts [3]. However, when using a sagittal canal diameter of ≤ 10 mm as the definition of absolute CLSS, the prevalence has been reported to be 4% in individuals aged < 40 years and 20% in ages 60–69 years [1]. When using ≤ 12 mm as a relative/absolute CLSS, the prevalence was 20% and 47% in the two above age groups [1].
To complicate matters, a radiographically identified CLSS may occur with or without clinical symptoms. Neurogenic claudication is regarded as the most typical symptom, usually precipitated by prolonged standing and/or walking, and relived by sitting and/or bending forward [4, 5]. The pathophysiology behind neurogenic claudication is usually referred to bulging discs, osteoarthritis of the facet joints, and/or infolding of the ligamentum flavum, resulting in a mechanical compression of neural elements [6, 7] and/or ischaemia of lumbosacral nerve roots [6, 7]. CLSS may or may not also be accompanied by back pain [4, 5]. Previous studies have found no clear association between narrowing of the spinal canal and clinical symptoms [3, 8]. Finally, CLSS morbidity is often described as being associated with marked loss of independence and decreased quality of life [9].
Most CLSS patients in need of intervention are given patient education, physiotherapy, pain medication and/or epidural injections [10, 11]. One reason is that CLSS symptoms are often mild and fluctuating [7, 12]. With more persisting disability that does not respond to non-surgical treatment, decompressive surgery is regarded as the gold standard treatment [10, 13,14,15]. Randomised controlled trials (RCT) have found superior outcomes with decompressive surgery compared to non-operative treatment [14, 16, 17], with similar outcomes with and without fusion [13, 15]. Presently, it is not clear if certain subgroups of CLSS patients may in fact attain better outcome through an accompanying fusion [18].
The mid- and long-term outcomes after CLSS surgery have been evaluated [10, 13,14,15,16,17,18]. When conducting such evaluations, it is important to not only evaluate statistically significant differences, but also whether improvements exceed the minimal clinically important differences (MCID) [19]. To our knowledge, no study has evaluated recovery patterns after CLSS surgery in the immediate postoperative period. This is important, as improved knowledge about the postoperative period may make patient information more accurate. Currently, 54% of patients with degenerative lumbar spine surgery report that they are dissatisfied with the preoperative information [20]. Inadequate information is associated with inferior surgical outcomes and less satisfied patients [21,22,23]. Improved knowledge regarding the recovery pattern after CLSS surgery would therefore not only provide realistic expectations and improved ability to optimise aftercare planning and pain medication, but possibly also contribute to more satisfied patients.
The primary aims of this study were to identify (1) if decompression due to CLSS surgery within the first 2 postoperative weeks is associated with reduced pain and improved quality of life, (2) if the recovery pattern in back and/or leg pain and quality of life differ, (3) if there are sex differences, and (4) if improvement exceeds minimal clinical important difference.
Material and method
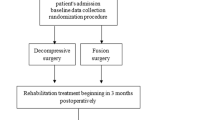
From March 2020 to January 2022, we invited fifty patients scheduled for CLSS surgery at Ängelholm County Hospital, Sweden, due to symptoms not responding to non-surgical treatment. This hospital only conducts spinal surgery in patients in ASA (American Society of Anaesthesiologists) class 1 or 2. In order to be asked to participate in our study, the patients had to have 1–4 levels of CLSS confirmed by magnetic resonance imaging (MRI) [2], be scheduled for CLSS decompression surgery without fusion, and be over age 50 without cognitive impairment and with sufficient knowledge of Swedish to complete the questionnaire. All invited patients accepted, 25 men with a mean age of 66 years (range 51–82) and 25 women with a mean age of 72 years (range 55–85). Forty-six of the patients had both neurogenic claudication and back pain, 3 had only neurogenic claudication and one only back pain. Orthopaedic spine surgeons from Skåne University Hospital (SUS), Malmö, Sweden, performed the surgical procedures.
We retrieved pre- and perioperative data from SweSpine (the Swedish National Registry for Spine Surgery) [24,25,26]. The registry collects patient-reported data on age, sex, smoking habits, self-estimated walking distance in four categories [(1) < 100 m (m), (2) 100–500 m, (3) 500–1000 m, (4) > 1000 m], consumption of analgesics in three categories [(1) no use, (2) intermittent use or (3) continuous use], and use of opioid-related compounds. SweSpine also includes patient-reported outcome scores (PROMs), i.e. level of leg and back pain according to Numeric Rating Scale (NRS; 0 = no pain, 10 = worst imaginable pain) and quality of life according to EuroQol 5D index (EQ-5D index; 1 = best possible quality of life, 0 = death, negative values indicate conditions “worse than death”) and EQ5D visual analogue scale (EQ-5D VAS; 100 = best possible quality of life, 0 = worst). The surgeon reports the perioperative data to SweSpine, including whether the surgery was acute or elective, diagnosis, type of surgical procedure, level(s) of surgery, surgery-related complications, e.g. dural tear or injury to nerve roots and postoperative complications during the hospital stay through dichotomous answers (yes/no) on questions regarding death, postoperative haematoma, urinary retention, urinary tract infection, pulmonary embolism, wound infection, Cauda Equina Syndrome, thrombosis or “other complications”.
Two independent observers, uninvolved in the treatment of the patients, undertook interviews for this specific study on day 1, 7 and 14 after the operation. The observers then registered NRS back and NRS leg pain, EQ-5D index, EQ-5D VAS and pain medication. We regarded an improvement of ≥ 40% in NRS leg pain and of ≥ 33% in NRS back pain as clinically important differences based on previous research on minimal clinically important differences (MCID) [19].
We used Statistica version 12 (Stat Soft®) for all statistical calculations. Descriptive data are reported as means ± standard deviations (SD), means (ranges) or proportions (%). Inferential statistics are reported as means with 95% confidence interval (95% CI). Group comparisons for continuous variables were done using the Student unpaired t test, for repeated measurements with Student paired t test and analyses of variance (ANOVA), and for categorical variables using McNemar’s test. A p value of < 0.05 was regarded as a statistically significant difference. All patients gave written consent. The study was approved by the ethics committee in Lund, Sweden (EPN Dnr 2016/159).
Results
Table 1 shows pre- and perioperative patient characteristics. Table 2 and Fig. 1 show NRS back and leg pain preoperative, day 1, 7, and 14 after the operation. Table 3 and Fig. 1 show the EQ-5D index and EQ-5D VAS. Table 4 shows analgesic use. Seven patients were on continuous morphine/opioid opioanalogue medication preoperatively; one day after surgery the figure was 48 patients, after 7 days 33 patients, and after 14 days 17 patients.

Patient-reported back and leg pain (Numeric Rating Scale; NRS) quality of life [EQ-5D index and EQ-5D VAS (visual analogue scale] before and 1, 7, and 14 days after surgery in 50 patients aged 51–85 years who underwent decompression due to central lumbar spinal stenosis (CLSS). Data are shown as mean with 95% confidence intervals (95% CI)
NRS back pain was similar between preoperative and day 1 after surgery, but then decreased, from day 1 to 7 after surgery [− 0.6 (− 1.2, − 0.03)] and from day 7 to 14 (− 0.7 (− 1.3, − 0.2)] (Table 5). NRS leg pain decreased from preoperative to day 1 after surgery [− 5.2 (− 6.1, − 4.3)], but thereafter remained stable (Table 5). The EQ-5D index improved from preoperative to day 1 after surgery [+ 0.09 (0.06, 0.13)] and from day 1 to day 7 after surgery [+ 0.05 (0.02, 0.08)], but thereafter remained stable (Table 5). The EQ-5D VAS improved from preoperative to day 1 after surgery [+ 13.7 (9.1, 18.3)] and from day 1 to day 7 after surgery [+ 6.0 (2.0, 10.0)], but then remained stable (Table 5).
Two weeks after surgery, 51% of the patients had improved above the minimal clinically important difference (MCID) in back pain and 71% in leg pain (Table 6).
We found no sex differences in NRS leg pain, NRS back pain, EQ-5D index, or EQ-5D VAS preoperative day 1, 7 or 14 after surgery (Tables 2, 3) and no apparent sex differences in improvement after surgery (Table 5).
Discussion
Decompression due to CLSS is generally followed by reduction in leg pain and improvement in quality of life within the first day of surgery; quality of life improves further the first postoperative week, and back pain decreases the first postoperative weeks. It is also important to emphasise that surgery is not only associated with statistically significant improvement, but in the majority of the patients also improvement of a clinically important difference [19]. Our data supported that decompression without fusion in CLSS patient is within weeks associated with favourable outcomes in the majority of the patients [10, 13,14,15].
We found that the recovery patterns for back and leg pain differ, without apparent sex differences. Leg pain improved within a day of surgery, while back pain improved gradually during the first 2 postoperative weeks. A similar temporal recovery pattern in pain improvement has previously been reported after lumbar disc herniation surgery [27]. Therefore, we speculate that the reduction in leg pain is predominantly the result of instant mechanical decompression of the nerve roots, while reduction in back pain may be influenced by other pathophysiological pathways, such as gradual reduction in the chemical inflammation associated with bulging discs, nucleus pulposus, and spinal canal compression [28, 29]. The slower improvement in back pain may also reflect the surgical trauma. Our data also indicate the importance of both back and leg pain for quality of life, as the EQ-5D index and EQ-5D VAS improved both from before to the first postoperative day (corroborating with reduction in leg pain) and the first postoperative week (corroborating with reduction in back pain).
The lower NRS leg pain and higher quality of life in the immediate postoperative period in our cohort compared to the one-year outcome after this type of operation that has been reported with SweSpine data (VAS leg pain 34, EQ 5D index 0.63, EQ5D VAS 64) [25, 26] may have several explanations. The well-known placebo effect of surgical interventions may influence the immediate postoperative PROMs rating. The personal contact between the patients and the researchers during the weeks before and after the operation may also influence the PROMs ratings, as good communication and thorough information is associated with favourable outcomes [21,22,23]. We also speculate, as PROMs rating is entirely subjective, that the first weeks of improvement after a longstanding disability could be perceived by the patient as a marked difference, leading to a high PROMs scoring. If the patient then expects further improvement that does not occur, this may lead to lower PROMs rating at the one-year follow-up. It is also possible that new pathological conditions, e.g. scar tissue and/or bulging discs, deteriorate the clinical status during the first postoperative year, also resulting in lower PROMs ratings at the one-year follow-up compared to the immediate postoperative period. Finally, ageing may be another contributing factor, as higher age is associated with lower PROMs rating.
Study strengths include the use of validated PROMs, and the inclusion of several surgeons with different experience, mimicking the general health care system. Even if this study only includes a small sample, we are of the opinion that our inferences can be generalised, as the preoperative NRS leg and back pain and the age and sex distribution were similar to nationally reported data [26]. Another strength is that none of the participants were lost to follow-up. The use of independent observers, unaware of the expectations of the surgeon or patient, preoperative treatments, radiological findings, surgical procedure, level(s) of surgery and/or complications are other study strengths. Limitations include the small sample size mentioned above and also that the patients were not consecutively included, and that only patients with ASA grade 1 and 2 and patients that understood Swedish were included.
Conclusions
We conclude that decompression without fusion due to CLSS is associated with improvement in leg pain and quality of life already within one day of surgery, that quality of life improves further during the first postoperative week, and that back pain gradually decreases during the first 2 postoperative weeks. Decompression without fusion due to CLSS seems to achieve improvement with a clinically relevant difference in a majority of patients within 2 weeks.
Availability of data and materials
The data are available upon ethical review and permission from the SweSpine board.
Abbreviations
- CLSS:
-
Central lumbar spinal stenosis
- MCID:
-
Minimal clinical important difference
- NRS:
-
Numeric Rating Scale
- EQ-5D:
-
EuroQol-5D
- RCT:
-
Randomised Controlled Trial
References
Kalichman L, Cole R, Kim DH, Li L, Suri P, Guermazi A, et al. Spinal stenosis prevalence and association with symptoms: the Framingham Study. Spine J. 2009;9(7):545–50.
Schizas C, Theumann N, Burn A, Tansey R, Wardlaw D, Smith FW, et al. Qualitative grading of severity of lumbar spinal stenosis based on the morphology of the dural sac on magnetic resonance images. Spine (Phila Pa 1976). 2010;35(21):1919–24.
Andreisek G, Hodler J, Steurer J. Uncertainties in the diagnosis of lumbar spinal stenosis. Radiology. 2011;261(3):681–4.
Comer CM, Redmond AC, Bird HA, Conaghan PG. Assessment and management of neurogenic claudication associated with lumbar spinal stenosis in a UK primary care musculoskeletal service: a survey of current practice among physiotherapists. BMC Musculoskelet Disord. 2009;10:121.
Suri P, Rainville J, Kalichman L, Katz JN. Does this older adult with lower extremity pain have the clinical syndrome of lumbar spinal stenosis? JAMA. 2010;304(23):2628–36.
Porter RW. Spinal stenosis and neurogenic claudication. Spine (Phila Pa 1976). 1996;21(17):204620–52.
Bal S, Celiker R, Palaoglu S, Cila A. F wave studies of neurogenic intermittent claudication in lumbar spinal stenosis. Am J Phys Med Rehabil. 2006;85(2):135–40.
Iwahashi H, Yoshimura N, Hashizume H, Yamada H, Oka H, Matsudaira K, et al. The association between the cross-sectional area of the dural sac and low back pain in a large population: the Wakayama spine study. PLoS ONE. 2016;11(8):e0160002.
Jansson KA, Nemeth G, Granath F, Jonsson B, Blomqvist P. Health-related quality of life (EQ-5D) before and one year after surgery for lumbar spinal stenosis. J Bone Jt Surg Br. 2009;91(2):210–6.
Weinstein JN, Tosteson TD, Lurie JD, Tosteson A, Blood E, Herkowitz H, et al. Surgical versus nonoperative treatment for lumbar spinal stenosis four-year results of the Spine Patient Outcomes Research Trial. Spine (Phila Pa 1976). 2010;35(14):1329–38.
Kreiner DS, Shaffer WO, Baisden JL, Gilbert TJ, Summers JT, Toton JF, et al. An evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spinal stenosis (update). Spine J. 2013;13(7):734–43.
Johnsson KE, Rosen I, Uden A. The natural course of lumbar spinal stenosis. Clin Orthop Relat Res. 1992;279:82–6.
Forsth P, Olafsson G, Carlsson T, Frost A, Borgstrom F, Fritzell P, et al. A randomized, controlled trial of fusion surgery for lumbar spinal stenosis. N Engl J Med. 2016;374(15):1413–23.
Weinstein JN, Tosteson TD, Lurie JD, Tosteson AN, Blood E, Hanscom B, et al. Surgical versus nonsurgical therapy for lumbar spinal stenosis. N Engl J Med. 2008;358(8):794–810.
Bae HW, Rajaee SS, Kanim LE. Nationwide trends in the surgical management of lumbar spinal stenosis. Spine (Phila Pa 1976). 2013;38(11):916–26.
Atlas SJ, Keller RB, Robson D, Deyo RA, Singer DE. Surgical and nonsurgical management of lumbar spinal stenosis: four-year outcomes from the Maine lumbar spine study. Spine (Phila Pa 1976). 2000;25(5):556–62.
Malmivaara A, Slatis P, Heliovaara M, Sainio P, Kinnunen H, Kankare J, et al. Surgical or nonoperative treatment for lumbar spinal stenosis? A randomized controlled trial. Spine (Phila Pa 1976). 2007;32(1):1–8.
Ghogawala Z, Dziura J, Butler WE, Dai F, Terrin N, Magge SN, et al. Laminectomy plus fusion versus laminectomy alone for lumbar spondylolisthesis. N Engl J Med. 2016;374(15):1424–34.
Austevoll IM, Gjestad R, Grotle M, Solberg T, Brox JI, Hermansen E, et al. Follow-up score, change score or percentage change score for determining clinical important outcome following surgery? An observational study from the Norwegian registry for Spine surgery evaluating patient reported outcome measures in lumbar spinal stenosis and lumbar degenerative spondylolisthesis. BMC Musculoskelet Disord. 2019;20(1):31.
Ronnberg K, Lind B, Zoega B, Halldin K, Gellerstedt M, Brisby H. Patients’ satisfaction with provided care/information and expectations on clinical outcome after lumbar disc herniation surgery. Spine (Phila Pa 1976). 2007;32(2):256–61.
Krupic F, Rolfson O, Nemes S, Karrholm J. Poor patient-reported outcome after hip replacement, related to poor perception of perioperative information, commoner in immigrants than in non-immigrants. Acta Orthop. 2016;87(3):218–24.
Iversen MD, Daltroy LH, Fossel AH, Katz JN. The prognostic importance of patient pre-operative expectations of surgery for lumbar spinal stenosis. Patient Educ Couns. 1998;34(2):169–78.
de Groot KI, Boeke S, Passchier J. Preoperative expectations of pain and recovery in relation to postoperative disappointment in patients undergoing lumbar surgery. Med Care. 1999;37(2):149–56.
Stromqvist B, Jonsson B, Fritzell P, Hagg O, Larsson BE, Lind B. The Swedish National Register for lumbar spine surgery: Swedish Society for Spinal Surgery. Acta Orthop Scand. 2001;72(2):99–106.
Sigmundsson FG, Jonsson B, Stromqvist B. Impact of pain on function and health related quality of life in lumbar spinal stenosis. A register study of 14,821 patients. Spine (Phila Pa 1976). 2013;38(15):E937–45.
Stromqvist B, Fritzell P, Hagg O, Jonsson B, Sanden B, Swedish Society of Spinal S. Swespine: the Swedish spine register: the 2012 report. Eur Spine J. 2013;22(4):953–74.
Stromqvist F. Lumbar disc herniation surgery [Thesis]. Lund University: Faculty of Medicine: Lund University; 2017.
Olmarker K, Blomquist J, Stromberg J, Nannmark U, Thomsen P, Rydevik B. Inflammatogenic properties of nucleus pulposus. Spine (Phila Pa 1976). 1995;20(6):665–9.
Brisby H, Olmarker K, Larsson K, Nutu M, Rydevik B. Proinflammatory cytokines in cerebrospinal fluid and serum in patients with disc herniation and sciatica. Eur Spine J. 2002;11(1):62–6.
Acknowledgements
The authors would like to thank Lars Jehpsson for statistical advice.
Funding
Open access funding provided by Lund University. The corresponding author has received a grant from Swedish Society of Spinal Surgeons. The grant was a general grant without specific demands or requirements. The funding body has no role in the design of this study, nor in the analysis and interpretation of data in this study or in writing the manuscript. The funding body is a non-profit organization which assists with the administration of the SweSpine registry.
Author information
Authors and Affiliations
Contributions
NH analysed the data and drafted the manuscript under supervision from MK. MK proposed the initial study design with NH and SI. SI, BR, MK all contributed to the study design as well as revising the manuscript. All authors discussed the results, read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All patients gave written consent. The study was approved by the ethics committee in Lund, Sweden (EPN Dnr 2016/159).
Consent for publication
No individual data shown.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hareni, N., Ebrahimnia, S., Rosengren, B.E. et al. Recovery pattern after decompression of central lumbar spinal stenosis: a prospective observational cohort study. J Orthop Surg Res 19, 200 (2024). https://doi.org/10.1186/s13018-024-04614-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-024-04614-1