
Abstract
Background
Continuous passive motion (CPM) is commonly used as a postoperative rehabilitation treatment, along with physical therapy, for postoperative knee rehabilitation. However, the comparison between the two in terms of efficacy in postoperative knee replacement recovery is unclear.
Purpose
To compare efficacy and safety of combined CPM versus physical therapy alone in postoperative rehabilitation after knee arthroplasty.
Methods
PubMed, Embase, and Web of Science databases were used to retrieve and access clinical studies on the efficacy of CPM compared with physical therapy. Review Manager software was used for study publication bias assessment and data analysis based on inclusion criteria.
Results
A total of 6 articles covering 557 patients were included in the study. In terms of range of motion (ROM), passive knee flexion was similar between CPM and physical therapy (PT) (WMD, − 0.17; 95% CI, − 0.98–0.64; p = 0.68). At long-term follow-up, passive knee extension was similar between CPM and physical therapy (PT) (WMD, − 0.28; 95% CI, − 1.47 to − 0.92; I2 = 65%, p =0.65). In addition, CPM generates significantly higher in length of stay (WMD, 0.50; 95% CI, − 0.31 to 0.69; I2 = 3%, p < 0.001). CPM generates significantly higher treatment costs and incurs more care costs relative to physical therapy.
Conclusion
Compared to PT, combined with CPM failed to significantly improve ROM of the knees and patient’s satisfaction. In addition, CPM treatment significantly increased the cost of hospitalization.
Similar content being viewed by others


Introduction
Postoperative knee rehabilitation is paramount to maintaining joint motion function [1,2,3,4]. The incidence of knee stiffness is reported to be as high as 35% with no or inappropriate rehabilitation [2, 4,5,6] and significantly affects patient quality of life and satisfaction. Clinically, two intervention strategies can be used to guide patients in postoperative rehabilitation: continuous passive motion (CPM) and traditional physical therapy. CPM was introduced in the 1970s and relies primarily on moving mechanical clips to improve joint mobility and thereby achieve improvement [7,8,9].
CPM has a positive biological effect on tissue healing, edema, and hematoma [10,11,12]. Vasileiadis et al. [13] confirmed the role of CPM in the maturation of heterotopic ossification by performing CPM rehabilitation in a 46-year-old male patient with right deviation. Stopping the progression and maintenance of heterotopic ossification became a useful aid in increasing joint mobility. Traditional physical therapy mainly includes dynamic floor exercises, suspension, gait training, closed chain exercises, open chain exercises, and pedal exercises, and the basic idea is an active activity. At present, both rehabilitation strategies are used to guide postoperative rehabilitation, but there is high controversy in the industry regarding the clinical application of both. Therefore, it is extremely important to conduct high-quality clinical evidence-based studies to explore reasonable rehabilitation strategies after knee surgery to guide clinical practice.
Previous studies have reported that the use of CPM has advantages over physical therapy, including reduced swelling, faster return of joint mobility, and reduced analgesia [14]. However, there is still a great deal of controversy about whether it is beneficial for patients' postoperative recovery in the past two decades of research [4, 15,16,17,18]. Many researchers support these benefits; on the contrary, many studies show that the advantages of CPM compared to physical therapy are not as clear [1, 2].
Hence, based on previously presented evidence from high-quality randomized controlled trials, our evidence-based study aimed to determine the effectiveness of CPM compared to physical therapy in postoperative orthopedic rehabilitation, comparing key outcomes including knee range of motion (ROM), The Western Ontario and McMaster University Osteoarthritis Index (WOMAC) pain scores, length of stay, satisfaction of patients, postoperative complications, and medical costs.
Method
This systematic review and meta-analysis following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement protocol. This study was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42023410252).
Search strategy and eligibility criteria
PubMed, Embase, and Web of Science databases were searched. We take PubMed as an example to demonstrate the search strategy for this study (Additional file 1: Appendice 1). We developed specific search strategies for each database, and references of the identified studies were checked for potential eligibility. Relevant clinical outcomes published in January 2000 and April 2023 were retrieved.
Our inclusion criteria for this meta-analysis included: (1) publications comparing the results for both (physiotherapy interventions including active ground exercise, suspension, gait training, closed chain exercise, open chain exercise, and pedal exercise in the control and experimental groups, and CPM in the experimental group); (2) randomized controlled trial and clinical study; (3) the sample size is feasible and the statistical analysis is scientific; (4) primary selection of patients after knee arthroplasty; (5) published literature in English.
Using a standardized data form, we extracted several data elements from the included studies, and two investigators (JZFand WDF), independent of each other, extracted and screened the literature as well as the data according to the inclusion as well as data extraction. If any disagreements arose, they were resolved by discussion or validation by a third-party investigator (XC).
Data abstraction
We extracted general details and categories mainly including (1) demographics, (2) study characteristics, (3) outcome and prospective measures. Patient statistics included gender, age, and the total number of patients. Characteristics of the trial included author, publication date, study type, CPM, or physical therapy. Outcome measures for this study included ROM (active knee flexion extension and passive knee flexion extension), pain, function, complications, length of hospital stay, and patient satisfaction and were cross-checked.
Prognostic indicators such as postoperative pain were evaluated using the Western Ontario and McMaster University Osteoarthritis Index (WOMAC) score and Visual Analog Scale (VAS) score. The WOMAC Osteoarthritis Index [19] was developed by Bellamy et al. and is one of the most commonly used, patient-reported prognostic indicators for patients with lower extremity osteoarthritis. The WOMAC contains 24 items covering three dimensions: pain (5 items), stiffness (2 items), and function (17 items). The WOMAC has been extensively tested for validity, reliability, feasibility, and responsiveness over time. The VAS has been used since the 1920s to measure intangible indicators of pain, quality of life, and anxiety, and in recent years, the VAS has become a very popular tool for measuring pain [20].
Risk of bias
The quality of the included studies was assessed independently by two reviewers. In this regard, the Jadad Scale (four categories: (1) Randomization, (2) Concealment, (3) Blinded, and (4) Withdraw or drop-out) for RCT , The Cochrane Risk of Bias (ROB) tool for randomized controlled trials was used to assess the methodological quality of the included studies in our study [13]. Each standard was grouped into three various categories of "low risk", "high risk", or "unclear risk" of bias, and then, the quality of the randomized studies was determined according to institutional health research and quality standards.
Statistical analysis
We used RevMan version 5.4 Review Manager software for meta-analysis. Weighted mean differences (WMDs) were used to represent the results for continuous data, and 95% CI was used for interval estimation. If p < 0.05 was satisfied suggesting that the difference was statistically significant. Meanwhile, the heterogeneity test was performed on the included literature, and when p ≥ 0.10 and I2 ≤ 50%, there was no significant heterogeneity, and the fixed-effect model was used to combine the effect sizes for analysis; if p < 0.10 and I2 > 50%, it indicated that the heterogeneity among the included studies was large, and the sources of heterogeneity were further examined, and after excluding the obvious heterogeneity, the randomized effect model was applied for analysis [21].
If the heterogeneity between studies is significant, subgroup or sensitivity analyses are required to clarify the source of heterogeneity. Trials are subject to clinical and methodological differences, and in this study subgroup analysis based on available data according to follow-up time was performed to generate a final forest plot for description.
Results
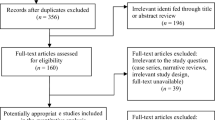
A total of 1025 publications was retrieved according to the search method, and a total of 6 clinical articles were screened for inclusion in the analysis based on the minimum standard. Figure 1 represents the screening process. Six direct comparisons of 557 cases of CPM after TKA as well as other physiotherapy RCT were included in this meta-analysis [8, 22,23,24,25,26]. The baseline information for these studies is listed in Table 1.

PRISMA flowchart
Range of motion
A comparative analysis of passive knee flexion, passive knee extension, active knee flexion, and active knee extension included in the study was mainly conducted to compare the range of knee motion at different periods.
Passive knee flexion
For short-term postoperative recovery, CPM produced better results in the first three days of postoperative recovery compared to physical therapy, and six studies reported long-term (3-month postoperative follow-up) results for passive knee flexion, and we analyzed the results using a random-effects model in which WMD was similar between the experimental and control groups (WMD, − 0.17; 95% CI, − 0.98 to 0.64; p =0.68). There was no clear evidence of statistically significant heterogeneity throughout the analysis (I2=28%; p = 0.23) (Fig. 2A).

Forest plots of range of motion. A Passive knee flexion; B passive knee extension
Passive knee extension
A total of five studies with 471 patients was analyzed, and we used a random-effects model to analyze the results. There were no significant differences between the two groups at long-term follow-up (WMD, − 0.28; 95% CI, − 1.47 to − 0.92; I2=65%, p = 0.65) (Fig. 2B).
Length of hospitalization
A total of 74 patients were included in 2 studies for analysis of length of stay; CPM generates significantly higher in length of stay (WMD, 0.50; 95% CI, − 0.31 to 0.69; I2=3%, p < 0.00001) (Fig. 3).

Forest plots of length of hospital
Pain evaluation
Two studies were scored by WOMAC and analyzed by taking a random-effects model (WMD, 6.75; 95% CI, − 6.75 to 8.10; p = 0.86), with a large heterogeneity between the studies' results. The experimental group scored slightly higher on the WOMAC functional difficulty score, but no significant differences were found after two weeks or on any follow-up measures (Fig. 4A). Moreover, two studies were scored by VAS and analyzed by taking a random-effects model (WMD, 9.41; 95% CI, 3.37–5.45; p = 0.002), with a large heterogeneity between the study results. The experimental group scored slightly higher on the VAS functional difficulty score. The VAS was performed, and there was a significant difference between the experimental and control groups (Fig. 4B).

Forest plots of pain scale. A WOMAC; B VAS
Satisfaction with treatment
For most patients, their status (perceived outcomes) was "better" compared to preoperative. Patients were generally satisfied with their treatment and outcomes in both the experimental and control groups. The CPM group also did not show a significant advantage in terms of patient-perceived outcomes [24].
Cost in hospital
Compared with other physical treatments [24], CPM generates significantly higher treatment costs and incurs more care costs.
Risks of bias
All six included RCTs were unblinded. The six RCTs were relatively well designed with a Jadad score range from 4 to 6 points, which indicated that they were of high quality. The Jadad score is summarized in Table 2. None of the included literature mentioned allocation concealment; the methodological assessment of the quality of the included literature is shown in Fig. 5A, as CPM requires patient consent and signed informed consent, so such studies were unblinded and highly biased in the blinded method. Of the 7 risks of bias domains (blinding of participants and personnel, performance bias) proved to have a high risk of bias. The graph shows "+" for attainment and "-" for non-attainment. Figure 5B shows the quality assessment of each entry of the methodological assessment.

A Assessment of the risk of bias. The traffic lights with “x,” “+,” and “−” represent that the corresponding domains are of high, low, and unclear risk of biases, respectively; B risk of bias summary. The plus sign means low risk, the question mark means unclear risk, and the minus sign means high risk.
Discussion
The present study finds that combined with CPM did not significantly improve postoperative functional recovery compared to physical therapy. There was no difference between the two in terms of time to discharge and patient satisfaction. Overall, CPM did not show an advantage in postoperative patient recovery. Rather, it was associated with increased equipment costs and costs of care. Therefore, the current findings are insufficient to support the routine use of CPM to facilitate the recovery process after arthroplasty. In addition, the heterogeneity of included studies was significant. However, we performed a subgroup analysis of WMD to investigate the source of heterogeneity. The association between CPM and ROM is described at different times, i.e., baseline, day 3 or when the maximum value is reached, probably because these times are highly dependent on the time and angle set by the CPM device. Nonetheless, our subgroup analysis showed that regardless of when ROM was measured, the increase in CPM still produced the same results as physical rehabilitation.
Although several previous studies have confirmed that CPM improves ROM only in the initial postoperative period and does not have much effect on long-term postoperative recovery, this is consistent with the results of our present meta-analysis. The association between CPM and ROM was described at different times, i.e., baseline, day 3, or at the time of maximal value, possibly because these times were highly dependent on the timing and angle of the CPM device settings. However, our subgroup analyses showed that regardless of when ROM was measured, an increase in CPM still produced the same results as physical recovery. Yang et al [27] found that CPM use was not frequently associated with improved knee ROM and functional outcomes from hospital discharge to a final follow-up. In our study, the analysis of patient satisfaction was added, as well as the conclusion that CPM generates more inpatient spending and longer hospital stays. In actual clinical practice, however, the use of CPM devices remains the standard of care in many institutions for rehabilitation [28], although the provision of CPM to patients has now been shown to be associated with insignificant long-term benefits and the short-term therapeutic role of the procedure remains controversial [16, 29]. The primary goal of using a CPM device is to increase short-term postoperative knee ROM, as several studies have reported short-term efficacy of CPM in improving CPM [30], Although most studies have shown nonsignificant results for CPM, CPM is also heavily used, which is related to subjective patient factors as well as recovery expectations, and should be validated by including a larger sample of patients for follow-up. Lee et al studied new CPM machines compared to previous conventional CPM machines to form a clinical assessment of the usefulness and effectiveness of seated CPM machines in patients undergoing total knee arthroplasty, using more objective tools such as digital inclinometers and handheld dynamometers to measure ROM [29].
We clarified that the difference in the effect of CPM and PT on patients' motor function recovery was not significant. On this basis, the patient's satisfaction is important [14]. Several previous studies have shown no statistical difference between the two in terms of patient satisfaction. In Gatewood et al. [31] by analyzing the efficacy of the means of rehabilitation after knee surgery, it was noted that CPM did not improve in terms of patient satisfaction. Wirries et al. [32] prospectively randomized the analysis of patient satisfaction with CPM after TKA through 40 patients, using the WOMAC and the Knee Social Score (KSS), to assess patient satisfaction and knee function, ultimately concluding that there was no significant difference between the both. Our findings also show that CPM does not improve patient satisfaction, possibly because CPM does not show benefit in any of the outcome indicators assessed, provides additional costs, and requires additional training for implementation [33].
In the study conducted by Joshi et al [32], two patients in the CPM group had postoperative complications. One patient was discharged with an acute quadriceps tendon tear and the other had a deep hematoma. One patient in the no-CPM group had a very deep wound dehiscence after a fall. Mau-Moeller et al. [26] systematically evaluated the effectiveness of TKA's new active sling inpatient ROM exercise program; this physical therapy was easy to perform during hospitalization and was less expensive than CPM treatment. Musa Eymir et al. [34] held that AHSE (active heel gliding exercise) therapy provides more practical rehabilitation and leads to beneficial outcomes for patients with TKA. Therefore, their active exercise approach that encourages patients to participate in rehabilitation should be the first choice for acute postoperative rehabilitation after TKA rather than CPM.
Postoperative knee rehabilitation is essential to maintain joint motor function and significantly affects the quality of life and satisfaction of patients. This study describes in detail the clinical applicability of CPM and PT through meta-analysis, which is of great significance for the selection of rehabilitation exercises and the development of the next rehabilitation program for patients in clinical practice. Meanwhile, our meta-analysis also has some limitations. Firstly, CPM protocols and follow-up periods were inconsistent across all studies, which may lead to the possibility of bias. The long-term impact of CPM should be further assessed. Furthermore, due to the nature of the CPM equipment, it was not possible to blind the subjects to CPM grouping. In addition, some patients had received TKA before this study and therefore knew that the use of CPM devices as standard, could lead to effects that could have uncontrolled patient implications. Therefore, an assessment of the risk of bias revealed a generally high risk of bias in allocation concealment (selection bias) and participant blindness (performance bias). In the case of CPM application, however, these situations are unavoidable. These inconsistent results may be due to inappropriate matching of the CPM machine to the patient as well as measurement errors in ROM between studies.
Conclusion
Combined with CPM did not significantly improve postoperative functional recovery relative to physical therapy. There was no difference between the two in terms of time to hospital discharge and patient satisfaction. Overall, CPM did not show superior benefits for postoperative patient recovery. On the contrary, it was associated with increased equipment costs and care expenses. Therefore, the results of the current study are insufficient to support the routine use of CPM to facilitate the recovery process after arthroplasty. We believe that as CPM is used more in orthopedics, further optimization of measurement structures and device innovations are needed for additional evaluation.
Availability of data and materials
Relevant data can be available by contacting the corresponding author.
Abbreviations
- CPM:
-
continuous passive motion
- PT:
-
physical therapy
- ROM:
-
range of motion
References
Fortier LM, Rockov ZA, Chen AF, Rajaee SS. Activity recommendations after total hip and total knee arthroplasty. J Bone Joint Surg Am. 2021;103(5):446–55.
Davila Castrodad IM, Recai TM, Abraham MM, Etcheson JI, Mohamed NS, Edalatpour A, Delanois RE. Rehabilitation protocols following total knee arthroplasty: a review of study designs and outcome measures. Ann Transl Med. 2019;7(Suppl 7):S255.
Konnyu KJ, Thoma LM, Cao W, Aaron RK, Panagiotou OA, Bhuma MR, Adam GP, Balk EM, Pinto D. Rehabilitation for total knee arthroplasty: a systematic review. Am J Phys Med Rehabil. 2023;102(1):19–33.
Papalia R, Vasta S, Tecame A, D’Adamio S, Maffulli N, Denaro V. Home-based vs supervised rehabilitation programs following knee surgery: a systematic review. Br Med Bull. 2013;108:55–72.
Alkire MR, Swank ML. Use of inpatient continuous passive motion versus no CPM in computer-assisted total knee arthroplasty. Orthop Nurs. 2010;29(1):36–40.
Hill AD, Palmer MJ, Tanner SL, Snider RG, Broderick JS, Jeray KJ. Use of continuous passive motion in the postoperative treatment of intra-articular knee fractures. J Bone Joint Surg Am. 2014;96(14):e118.
He ML, Xiao ZM, Lei M, Li TS, Wu H, Liao J. Continuous passive motion for preventing venous thromboembolism after total knee arthroplasty. Cochrane Database Syst Rev. 2014;7:CD008207.
Lenssen TA, van Steyn MJ, Crijns YH, Waltje EM, Roox GM, Geesink RJ, van den Brandt PA, De Bie RA. Effectiveness of prolonged use of continuous passive motion (CPM), as an adjunct to physiotherapy, after total knee arthroplasty. BMC Musculoskelet Disord. 2008;9:60.
Salter RB, Hamilton HW, Wedge JH, Tile M, Torode IP, O’Driscoll SW, Murnaghan JJ, Saringer JH. Clinical application of basic research on continuous passive motion for disorders and injuries of synovial joints: a preliminary report of a feasibility study. J Orthop Res. 1984;1(3):325–42.
Knapik DM, Harris JD, Pangrazzi G, Griesser MJ, Siston RA, Agarwal S, Flanigan DC. The basic science of continuous passive motion in promoting knee health: a systematic review of studies in a rabbit model. Arthroscopy. 2013;29(10):1722–31.
Kuroda Y, Young M, Shoman H, Punnoose A, Norrish AR, Khanduja V. Advanced rehabilitation technology in orthopaedics-a narrative review. Int Orthop. 2021;45(8):1933–40.
McInnes J, Larson MG, Daltroy LH, Brown T, Fossel AH, Eaton HM, Shulman-Kirwan B, Steindorf S, Poss R, Liang MH. A controlled evaluation of continuous passive motion in patients undergoing total knee arthroplasty. JAMA. 1992;268(11):1423–8.
Vasileiadis GI, Varvarousis DN, Manolis I, Ploumis A. The impact of continuous passive motion on heterotopic ossification maturation. Am J Phys Med Rehabil. 2021;100(12):e194–7.
Paravlic AH, Maffulli N, Kovač S, Pisot R. Home-based motor imagery intervention improves functional performance following total knee arthroplasty in the short term: a randomized controlled trial. J Orthop Surg Res. 2020;15(1):451.
Maniar RN, Baviskar JV, Singhi T, Rathi SS. To use or not to use continuous passive motion post-total knee arthroplasty presenting functional assessment results in early recovery. J Arthroplast. 2012;27(2):193–200.
Yang Y, Wang J, Zhang XY, Dong L, Liu AF, Li CY. The effect of continuous passive motion in patients treated with total knee arthroplasty for osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. Am J Phys Med Rehabil. 2021;100(12):1160–9.
Giustra F, Bistolfi A, Bosco F, Fresia N, Sabatini L, Berchialla P, Sciannameo V, Massè A. Highly cross-linked polyethylene versus conventional polyethylene in primary total knee arthroplasty: comparable clinical and radiological results at a 10-year follow-up. Knee Surg Sports Traumatol Arthrosc. 2023;31(3):1082–8.
Risitano S, Cacciola G, Capella M, Bosco F, Giustra F, Fusini F, Indelli PF, Massé A, Sabatini L. Comparison between gaits after a medial pivot and posterior stabilized primary total knee arthroplasty: a systematic review of the literature. Arthroplasty. 2023;5(1):15.
Walker LC, Clement ND, Deehan DJ. Predicting the outcome of total knee arthroplasty using the WOMAC score: a review of the literature. J Knee Surg. 2019;32(8):736–41.
Heller GZ, Manuguerra M, Chow R. How to analyze the Visual Analogue Scale: Myths, truths and clinical relevance. Scand J Pain. 2016;13:67–75.
Polanin JR, Pigott TD. The use of meta-analytic statistical significance testing. Res Synthesis Methods. 2014;6(1):63–73.
Bruun-Olsen V, Heiberg KE, Mengshoel AM. Continuous passive motion as an adjunct to active exercises in early rehabilitation following total knee arthroplasty: a randomized controlled trial. Disabil Rehabil. 2009;31(4):277–83.
Gil-Gonzalez S, Barja-Rodriguez RA, Lopez-Pujol A, Berjaoui H, Fernandez-Bengoa JE, Erquicia JI, Leal-Blanquet J, Pelfort X. Continuous passive motion not affect the knee motion and the surgical wound aspect after total knee arthroplasty. J Orthop Surg Res. 2022;17(1):25.
Joshi RN, White PB, Murray-Weir M, Alexiades MM, Sculco TP, Ranawat AS. Prospective randomized trial of the efficacy of continuous passive motion post total knee arthroplasty: experience of the hospital for special surgery. J Arthroplasty. 2015;30(12):2364–9.
Schulz M, Krohne B, Roder W, Sander K. Randomized, prospective, monocentric study to compare the outcome of continuous passive motion and controlled active motion after total knee arthroplasty. Technol Health Care. 2018;26(3):499–506.
Mau-Moeller A, Behrens M, Finze S, Bruhn S, Bader R, Mittelmeier W. The effect of continuous passive motion and sling exercise training on clinical and functional outcomes following total knee arthroplasty: a randomized active-controlled clinical study. Health Qual Life Outcomes. 2014;12:68.
Yang X, Li GH, Wang HJ, Wang CY. Continuous passive motion after total knee arthroplasty: a systematic review and meta-analysis of associated effects on clinical outcomes. Arch Phys Med Rehabil. 2019;100(9):1763–78.
Gáspár L, Farkas C, Szepesi K, Csernátony Z. Therapeutic value of continuous passive motion after anterior cruciate replacement. Acta Chir Hung. 1997;36(1–4):104–5.
Lee BC, Moon CW, Choi WS, Kim YM, Joo YB, Lee DG, Lee SJ, Choi ES, Ji JH, Suh DW, Cho KH. Clinical evaluation of usefulness and effectiveness of sitting type continuous passive motion machines in patients with total knee arthroplasty: a study protocol for a single-blinded randomized controlled trial. BMC Musculoskelet Disord. 2022;23(1):565.
Lenssen AF, Crijns YH, Waltje EM, Roox GM, van Steyn MJ, Geesink RJ, van den Brandt PA, de Bie RA. Effectiveness of prolonged use of continuous passive motion (CPM) as an adjunct to physiotherapy following total knee arthroplasty: design of a randomised controlled trial [ISRCTN85759656]. BMC Musculoskelet Disord. 2006;7:15.
Gatewood CT, Tran AA, Dragoo JL. The efficacy of post-operative devices following knee arthroscopic surgery: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2017;25(2):501–16.
Wirries N, Ezechieli M, Stimpel K, Skutek M. Impact of continuous passive motion on rehabilitation following total knee arthroplasty. Physiother Res Int. 2020;25(4):e1869.
Harvey LA, Brosseau L, Herbert RD. Continuous passive motion following total knee arthroplasty in people with arthritis. Cochrane Database Syst Rev. 2010;3:004260.
Eymir M, Erduran M, Unver B. Active heel-slide exercise therapy facilitates the functional and proprioceptive enhancement following total knee arthroplasty compared to continuous passive motion. Knee Surg Sports Traumatol Arthrosc. 2021;29(10):3352–60.
Acknowledgements
We thank DaoFeng Wang for his outstanding statistical analysis guidance.
Funding
This work was supported by the special fund of the National Clinical Research Center for Orthopedics, Sports Medicine and Rehabilitation.
Author information
Authors and Affiliations
Contributions
LWH did conceptualization; JZF collected the data; JZF, ZWP analyzed the data; JZF done original manuscript writing; ZWP and XC checked the language; GWL contributed to writing—review and editing. All authors read the final manuscript and approved the publication.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
There are no any ethical/legal conflicts involved in the article.
Consent for publication
All authors have read and approved the content, and agree to submit for consideration for publication in the journal.
Competing interests
Each authors certifies that there is no conflict of interest relevant to this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Appendice 1.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jia, Z., Zhang, Y., Zhang, W. et al. Efficacy and safety of continuous passive motion and physical therapy in recovery from knee arthroplasty: a systematic review and meta-analysis. J Orthop Surg Res 19, 68 (2024). https://doi.org/10.1186/s13018-024-04536-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-024-04536-y