
Abstract
Background
Total joint arthroplasty (TJA) can be associated with the development of periprosthetic joint infection (PJI). It is necessary to determine the modifiable and non-modifiable risk factors of PJI to provide optimum healthcare to TJA candidates.
Methods
This single-center retrospective review investigated 1198 patients who underwent TJA from 2012 to 2022. The data analysis comprised two stages. The first stage was a descriptive analysis, while the second stage was a bivariate analysis. The sociodemographic data, medical history, operative details, and presence of PJI postoperatively were evaluated.
Results
The study sample consisted of 1198 patients who underwent TJA. The mean patient age was 63 years. Among the patients, only 1.3% had PJI. No comorbidity was significantly related to PJI. General anesthesia was used in almost 21% of the patients and was significantly associated with a higher risk of infection (p = 0.049). An increased operative time was also significantly related to PJI (p = 0.012). Conversely, tranexamic acid (TXA) administration was a protective factor against PJI (p = 0.017).
Conclusion
Although PJI is not a common complication of TJA, multiple risk factors such as general anesthesia and prolonged operative time play a significant role in its development. In contrast, TXA administration is thought to reduce the risk of PJI effectively.
Similar content being viewed by others

Background
Total joint arthroplasty (TJA) aims to relieve pain symptoms and restore the joint function in patients with severe arthritis. Periprosthetic joint infection (PJI) is defined as postoperative infection in joint prostheses, occurring at a rate of 0.25–2.0% [1, 2]. Although TJA has been found to improve the overall quality of life of patients with end-stage arthritis, variable complications can potentially occur, jeopardizing procedural outcomes and compromising patients’ health status [3]. Even with the various advancements and improvements in joint prostheses, the incidence of PJI is increasing worldwide [4].
The increasing incidence of PJI can be thought to be related to that of comorbidities in many operative candidates. Owing to the increased life expectancy, there is an assumed future healthcare burden caused by the increasing number of osteoarthritis cases [5]. Consequently, the number of TJA that must be performed is also expected to rise. With the assumed increasing numbers, the incidence of PJI could increase proportionately in the upcoming decades [6, 7]. Based on the significance and the associated healthcare burden of PJI, the potential risk factors of this condition should be identified for early detection.
PJI is influenced by different factors that ultimately increase its risk of occurrence. These factors may include the characteristics of patients undergoing TJA, technique used during the procedure, adequacy of the postoperative period and care provided [8]. Our study aimed to review cases of TJA performed and assess the incidence of PJI and its associated factors.
Methods
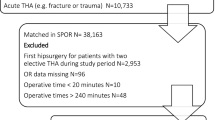
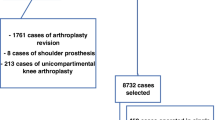
A retrospective study was conducted at King Abdulaziz Medical City (KAMC), a tertiary hospital in Riyadh. All patients of both sexes who underwent TJA from 2012 to 2022 were included. Patients who were aged under 18 years, were immunocompromised, had a history of infection and had missing data were excluded. Patients were recruited via non-probability consecutive sampling.
Data were collected through the BESTCare system at KAMC. The main categories of the data collection sheet used included the following: demographic data, operative data, comorbidities and infection. The operative data included the anesthesia type, operation name, unilaterality or bilaterality, approach, tourniquet usage, estimated blood loss amount, operative period, estimated operative time, time to postoperative infection, drainage and tranexamic acid (TXA) administration.
The presence of infection was based on the 2013 International Consensus Meeting and modified Musculoskeletal Infection Society consensus-based criteria. These criteria included the presence of two periprosthetic positive culture findings with phenotypically identical organism or sinus tract communicating with the joint or the presence of three out of the following five minor criteria: (1) elevated serum C-reactive protein level (more than 10 mg/L) and erythrocyte sedimentation rate (more than 30 mm/h); (2) elevated synovial fluid white blood cell count (more than 3000 cells/μL or++ change on a leukocyte esterase test strip); (3) elevated synovial fluid polymorphonuclear neutrophil percentage (more than 80%); (4) favorable histological finding of periprosthetic tissue; and (5) one positive culture finding.
The data were entered into Microsoft Excel (Microsoft, Redmond, WA, USA) and transferred to the Statistical Package for the Social Sciences v.25 (IBM Corp., Armonk, NY, USA) for statistical analysis. The data were checked for missing information, and new variables were recorded and computed based on the extracted data. All assumptions were satisfied for each analysis. The data analysis comprised two stages. The first stage was a descriptive analysis, wherein categorical variables were described as frequencies and percentages and numerical variables as means and standard deviations. The second stage was a bivariate analysis conducted using the Chi-squared test and Mann–Whitney test. Each analysis was performed at a confidence level of 95% and a p value of < 0.05.
Consent was not required for this retrospective cohort study. No identifying data were asked, ensuring privacy and confidentiality. All data were kept safe, with only the authors having access to the research data.
Results
A total of 1198 adult patients were admitted for TJA at KAMC, Riyadh. Most of them were women (76.6%). The average age of the patients was 63 (range: 19–91) years. The majority were obese (78.4%), followed by overweight (17.9%). The patient demographics are further detailed in Table 1.
Approximately 94.7% underwent total knee arthroplasty (TKA), while the rest underwent total hip arthroplasty (THA). Regarding the anesthesia utilized, the most common type was spinal anesthesia (38.3%), followed by spinal/epidural anesthesia (30%). General anesthesia was used in 21.6% of the patients and epidural anesthesia in almost 9%. Moreover, the approach used in the patients who underwent TKA was either medial parapatellar or subvastus, with most patients undergoing medial parapatellar TKA. Among the patients who underwent THA, either the posterior or lateral approach was used, with most patients undergoing posterior THA. The operative period and estimated operative time were also analyzed, showing that the majority of the procedures were performed in the morning and the minority at night, with a mean operative time of 137.9 ± 56.02 min. In addition, drainage was applied in almost 75% of the patients for a mean duration of 2.72 days. TXA was administered in 36.2% of the patients. Finally, 15 patients had PJI; of them, almost 1.3% (n = 5) had acute PJI, while the rest had chronic PJI. The details are shown in Table 2. The incidence of PJI was 1.3% (Table 3).
The comorbidities of the patients were also studied. Diabetes was found in almost 60% of the patients, hypertension in almost 56% and hyperlipidemia in almost 47%. Other comorbidities are mentioned in Table 4.
The Chi-square test and Mann–Whitney test were used to evaluate the relationship between PJI and the study variables. Table 5 displays the relationship between PJI and the demographic factors. No significant association was found between PJI and all demographic factors (p > 0.05). Table 6 shows the relationship between PJI and the operative details. There was a significant association observed between PJI and general anesthesia and staged bilateral surgery (both p < 0.05). Conversely, TXA administration was found to be associated with a reduced risk of PJI (p < 0.05). Furthermore, there was a significant relationship noted between PJI and the estimated operative time (p < 0.05). Table 7 displays the association between PJI and comorbidities. No significant association was found between them.
Discussion
Obesity has been found to be associated with a proportionately increased risk of other simultaneous comorbidities such as cardiovascular diseases, diabetes, decreased quality of nutritional intake, hypertension and possible mortality [9]. The risk of developing PJI is also likely to increase proportionately with an increasing body mass index [10]. In our study, we found that the body mass index was not a significant predictor of PJI (p = 0.279). In comparison, Jämsen et al. [11] reported that the incidence of PJI tended to increase with an increase in the body mass index; the incidence of PJI was 0.37% in patients who had a normal body mass index in comparison with 4.66% in patients who were considered morbidly obese. Conversely, Bozic et al. [12] noted that the risk of developing PJI postoperatively in association with the presence of obesity was considered significantly lower (19.0%) 1 year after TJA (p < 0.025).
Regarding sex, previous studies have noted that male candidates are more prone to developing PJI than female candidates [13, 14]. Other studies have reported opposite findings, claiming that women are more vulnerable to developing the infection than men [15, 16]. In our study, the women had a higher risk of developing PJI than the men (p = 0.379).
The age of the patients was not a significant predictor of PJI in our study. In a previous study, patients of older age were found to be more prone to developing postoperative infections owing to changes in their immunity [17]. In contrast, a multicenter study that analyzed around 623,253 joint operations reported that a younger age was more associated with developing PJI [18]. Similar to our study results, Wu et al. [19] found that patients aged between 65 and 75 years were at a higher risk of developing PJI by 3.36 folds than those aged between 45 and 65 years.
Comorbidities are risk factors that greatly influence the development of PJI [20]. In our study, no existing comorbidities were significantly associated with PJI. Diabetes was found in almost 61% of the patients, hypertension in 56% and hyperlipidemia in 47%. Different studies have shown that diabetes increases the risk of infection following TJA [11]. In an Indian study, it was found that there was a three-to-sixfold increased risk of PJI in patients with diabetes [21]. Moreover, a recent meta-analysis found that diabetes was associated with a 1.74-fold increased risk of PJI after TJA [22].
Some studies have shown that spinal anesthesia is associated with a lower risk of post-TJA infection and has some protective effects, including reduced amount of blood loss, reduced need for blood transfusion and lower incidence of hyperglycemia [23,24,25]. In our study, the most common anesthesia type was spinal anesthesia (38.3%), followed by spinal/epidural anesthesia (30%). General anesthesia was used in almost 21.6% and epidural anesthesia in almost 9%. Only general anesthesia was significantly associated with PJI (p = 0.049). Scholten et al. [26] showed similar results: Spinal anesthesia was more frequently utilized in patients. In their multivariable logistic regression analysis, general anesthesia yielded a higher risk for early PJI (odds ratio = 2.0; 95% confidence interval = 1.0–3.7).
The operative time is calculated from incision to closure of the skin. Peersman et al. [27] reported a significant association between SSI and subsequent PJI with a prolonged operative time. The recent meta-analysis conducted by Scigliano et al. [28] showed that following TJA, the risk of SSI and PJI was significant in procedures lasting ≥ 120 min compared with that in procedures lasting < 120 min. However, the risk of PJI was not significant when comparing both groups owing to limited data. Moreover, Wang et al. [29] showed that in TJA, an increased operative time was independently linked to PJI and SSI. They found that for every 20-min increase in the operative time, there was a 25% increase in the incidence of PJI. In our study, an increased operative time (mean = 137.9 ± 56.02 min) was significantly related to PJI (p = 0.012). The operative period was also analyzed and was divided into four groups as shown in Tables 2 and 5. No significant association was found with PJI (p = 0.776).
TXA may help reduce bleeding and hence infection by eliminating hematoma formation. Therefore, its administration is thought to have a protective effect against the risk of PJI [30]. The study based on an institutional database conducted by Yazdi et al. showed that TXA administration was associated with a reduced risk of PJI after primary TJA. Similarly, in our study, TXA administration was a protective factor against PJI (p = 0.017).
Different operative approaches are used in TJA based on multiple factors, including the surgeon’s preference and expertise. The optimum operative approach is still up for debate. For TKA, an international study reported that the outcomes at 1 week and 1 year were better with the subvastus approach than with the medial parapatellar approach, although the medial parapatellar approach was more convenient to use [31].
Regarding THA, a recent study was conducted by Aggarwal et al. [32] to assess the incidence of infection between different hip approaches. The authors divided the approaches into either direct anterior or non-anterior approaches and found 2.2-fold higher odds of infection in patients for whom the anterior approach was utilized. In our study, the most common approach used for TKA was the medial parapatellar approach (79%). The posterior approach was more commonly utilized than the lateral approach in almost 92% of the patients. Nevertheless, the approach was not significantly associated with the development of PJI (p = 0.52).
PJI is defined as infection in joint prostheses or surrounding tissues. The incidence of PJI has been found to range from 0.25 to 2.0%, indicating rarity of the infection [1]. Our study found that the risk of infection was around 1.3%. Fifteen patients had PJI, who were then divided into two groups: those with acute PJI and those with chronic PJI at a cutoff duration of 90 days. Approximately 33.3% had acute PJI, whereas the rest had chronic PJI. The recent study conducted by Kim et al. [33] showed that the annual incidence of PJI in Korea was 2.3–2.8%, comparable to 2–2.7% in the USA. The study conducted by Jin et al. [34] showed that the prevalence of PJI in four hospitals in Australia was 1.7% within 2 years following TJA. Similarly but to a lesser extent, 0.8% of the infected cases analyzed in our study were considered chronic PJI.
Postoperative drainage is a well-established standard treatment for orthopedic procedures. It is regarded as a valuable practice but is debatable. Parker et al. [35] demonstrated that operative wound drainage after orthopedic operations was associated with decreased wound discharges, which may minimize the risks of prosthetic infections later. A meta-analysis conducted in China also showed that the use of wound drainage resulted in an increased risk of PJI [36]. In our study, 75% of the patients had postoperative drainage for a mean duration of 2.72 days. Nevertheless, there was no significant association between the use of drainage and the incidence of PJI (p = 0.885).
Tourniquet use during TKA has long been considered to reduce blood loss amount, improve visualization and facilitate operation. However, the medical community has debated upon its role in the risk of PJI. In our study, tourniquet was applied in 89.4% of the patients. There was no significant association between the usage of tourniquet and the risk of PJI (p = 0.596). In their meta-analysis, Zhang et al. [37] concluded that there was no significant difference in the incidence of PJI between patients who underwent operation with and without tourniquet use. However, the recent meta-analysis by Magan et al. [38] noted that using tourniquet in TKA was associated with an increased risk of infection, prolonged length of stay and increased need for blood transfusion.
TKA can be performed in multiple ways, including simultaneous, staged bilateral or unilateral TKA. In the study conducted by Poultsides et al. [39], the incidence of widespread infection in simultaneous bilateral TKA (0.57%) was significantly lower than that in bilateral staged TKA (1.39%) and unilateral TKA (1.1%). Similarly, in our study, there was a significant association between staged bilateral TKA and the incidence of PJI (p = 0.036), representing 46.7% of the PJI cases. Hart et al. [40] showed that simultaneous bilateral TKA was generally safe and did not lead to more hospitalizations than did unilateral TKA. Another meta-analysis conducted by Xu et al. [41] reported that there was no increased risk of PJI following simultaneous bilateral TJA when compared with staged bilateral TJA.
Regarding the limitations of this study, the data were gathered from only one center, potentially restricting the generalizability of the findings. This subject requires more exploration in the area, with a larger sample size involved. In addition, owing to the retrospective study design, there was a limitation in the ability to control for the variables, which might have influenced the results. Moreover, owing to the limited number of studies that investigated the predictors of PJI, we faced difficulties in comparing the results.
Conclusion
PJI is not a common complication of TJA, but risk factors such as general anesthesia and prolonged operative time can lead to its development. Conversely, TXA administration can reduce the risk of PJI. The modifiable risk factors of PJI should be acknowledged and optimized to provide optimum healthcare to patients after TJA.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- TJA:
-
Total joint arthroplasty
- PJI:
-
Periprosthetic joint infection
- KAMC:
-
King Abdulaziz Medical City
- TXA:
-
Tranexamic acid
- TKA:
-
Total knee arthroplasty
- THA:
-
Total hip arthroplasty
References
Lee QJ, Mak WP, Wong YC. Risk factors for periprosthetic joint infection in total knee arthroplasty. J Orthop Surg. 2015;23(3):282–6.
Eka A, Chen AF. Patient-related medical risk factors for periprosthetic joint infection of the hip and knee. Ann Transl Med. 2015;3(16):233.
Shohat N, Fleischman A, Tarabichi M, Tan TL, Parvizi J. Weighing in on body mass index and infection after Total joint arthroplasty: is there evidence for a body mass index threshold? Clin Orthop Relat Res. 2018;476(10):1964–9.
Inoue D, Xu C, Yazdi H, Parvizi J. Age alone is not a risk factor for periprosthetic joint infection. J Hosp Infection. 2019;103(1):64–8.
Cross M, Smith E, Hoy D, Nolte S, Ackerman I, Fransen M, et al. The global burden of hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73(7):1323–30. https://doi.org/10.1136/annrheumdis-2013-204763.
Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89-A(4):780–5. https://doi.org/10.2106/jbjs.f.00222.
Patel A, Pavlou G, Mujica-Mota RE, Toms AD. The epidemiology of revision total knee and hip arthroplasty in England and Wales: a comparative analysis with projections for the United States. A study using the national joint registry dataset. Bone Joint J. 2015;97-B(8):1076–81. https://doi.org/10.1302/0301-620X.97B8.35170.
Kunutsor SK, Whitehouse MR, Blom AW, Beswick AD. Patient-related risk factors for periprosthetic joint infection after total joint arthroplasty: a systematic review and meta-analysis. PloS One. 2016;11(3):e0150866.
Arsoy D, Woodcock JA, Lewallen DG, et al. Outcomes and complications following total hip arthroplasty in the super-obese patient. BMI J Arthroplasty. 2014;29:1899–905.
Malinzak RA, Ritter MA, Berend ME, et al. Morbidly obese, diabetic, younger, and unilateral joint arthroplasty patients have elevated total joint arthroplasty infection rates. J Arthroplasty. 2009;24:84–8.
Jämsen E, Nevalainen P, Eskelinen A, et al. Obesity, diabetes, and preoperative hyperglycemia as predictors of periprosthetic joint infection: a single-center analysis of 7181 primary hip and knee replacements for osteoarthritis. J Bone Joint Surg Am. 2012;94:e101.
Bozic KJ, Lau E, Kurtz S, et al. Patient-related risk factors for periprosthetic joint infection and postoperative mortality following total hip arthroplasty in Medicare patients. J Bone Joint Surg Am. 2012;94:794–800.
Resende VAC, Neto AC, Nunes C, Andrade R, Espregueira-Mendes J, Lopes S. Higher age, female gender, osteoarthritis and blood transfusion protect against periprosthetic joint infection in total hip or knee arthroplasties: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2018;29(1):8–43.
Pedersen AB, Svendsson JE, Johnsen SP, Riis A, Overgaard S. Risk factors for revision due to infection after primary total hip arthroplasty. A population-based study of 80,756 primary procedures in the Danish hip arthroplasty registry. Acta Orthop. 2010;81(5):542–7.
Namba RS, Inacio MC, Paxton EW. Risk factors associated with surgical site infection in 30,491 primary total hip replacements. J Bone Joint Surg Br. 2012;94(10):1330–8.
Ridgeway S, Wilson J, Charlet A, Kafatos G, Pearson A, Coello R. Infection of the surgical site after arthroplasty of the hip. J Bone Joint Surg Br. 2005;87(6):844–50.
Ren X, Ling L, Qi L, et al. Patients’ risk factors for periprosthetic joint infection in primary total hip arthroplasty: a meta-analysis of 40 studies. BMC Musculoskelet Disord. 2021;22:776. https://doi.org/10.1186/s12891-021-04647-1.
Lenguerrand E, Whitehouse MR, Beswick AD, Kunutsor SK, Burston B, Porter M, et al. Risk factors associated with revision for prosthetic joint infection after hip replacement: a prospective observational cohort study. Lancet Infect Dis. 2018;18(9):1004–14. https://doi.org/10.1016/S1473-3099(18)30345-1.
Wu C, Qu X, Liu F, Li H, Mao Y, Zhu Z. Risk factors for periprosthetic joint infection after total hip arthroplasty and total knee arthroplasty in Chinese patients. PloS one. 2014;9(4):e95300. https://doi.org/10.1371/journal.pone.0095300.
NEJM journal watch: summaries of and commentary on original medical and scientific articles from key medical journals. Accessed May 15, 2022. https://www.jwatch.org/na40511/2016/02/26/risk-staphylococcal-prosthetic-joint-infection-after
Sebastian S, Malhotra R, Dhawan B. Prosthetic joint infection: a major threat to successful total joint arthroplasty. Indian J Med Microbiol. 2019;36(4):475–87.
López-de-Andrés A, Hernández-Barrera V, Martínez-Huedo MA, Villanueva-Martinez M, Jiménez-Trujillo I, Jiménez-García R. Type 2 diabetes and in-hospital complications after revision of total hip and knee arthroplasty. PLoS ONE. 2017;12(8):e0183796.
Liu J, Ma C, Elkassabany N, Fleisher LA, Neuman MD. Neuraxial anesthesia decreases postoperative systemic infection risk compared with general anesthesia in knee arthroplasty. Anesth Analg. 2013;117(4):1010–6.
Guay J. The effect of neuraxial blocks on surgical blood loss and blood transfusion requirements: a meta-analysis. J Clin Anesth. 2006;18(2):124–8.
Gottschalk A, Rink B, Smektala R, Piontek A, Ellger B, Gottschalk A. Spinal anesthesia protects against perioperative hyperglycemia in patients undergoing hip arthroplasty. J Clin Anesth. 2014;26(6):455–60.
Scholten R, Leijtens B, Hannink G, Kamphuis ET, Somford MP, van Susante JLC. General anesthesia might be associated with early periprosthetic joint infection: an observational study of 3,909 arthroplasties. Acta Orthop. 2019;90(6):554–8. https://doi.org/10.1080/17453674.2019.1644069. (Epub 2019 Jul 24. PMID: 31339401; PMCID: PMC6844397).
Peersman G, Laskin R, Davis J, Peterson MGE, Richart T. Prolonged operative time correlates with increased infection rate after total knee arthroplasty. HSSJ. 2006;2:70–2.
Scigliano NM, Carender CN, Glass NA, Deberg J, Bedard NA. Operative time and risk of surgical site infection and periprosthetic joint infection: a systematic review and meta-analysis. Iowa Orthop J. 2022;42(1):155–61 (PMID: 35821941; PMCID: PMC9210401).
Wang Q, Goswami K, Shohat N, Aalirezaie A, Manrique J, Parvizi J. Longer operative time results in a higher rate of subsequent periprosthetic joint infection in patients undergoing primary joint arthroplasty. J Arthroplasty. 2019;34(5):947–53. https://doi.org/10.1016/j.arth.2019.01.027.
Yazdi H, Klement MR, Hammad M, Inoue D, Xu C, Goswami K, Parvizi J. Tranexamic acid is associated with reduced periprosthetic joint infection after primary total joint arthroplasty. J Arthroplasty. 2020;35(3):840–4. https://doi.org/10.1016/j.arth.2019.10.029. (Epub 2019 Oct 22 PMID: 31722855).
Bridgman SA, Walley G, MacKenzie G, Clement D, Griffiths D, Maffulli N. Sub-vastus approach is more effective than a medial parapatellar approach in primary total knee arthroplasty: a randomized controlled trial. Knee. 2009;16(3):216–22. https://doi.org/10.1016/j.knee.2008.11.012.
Aggarwal VK, Weintraub S, Klock J, Stachel A, Phillips M, Schwarzkopf R, Iorio R, Bosco J, Zuckerman JD, Vigdorchik JM, Long WJ. Frank Stinchfield Award: a comparison of prosthetic joint infection rates between direct anterior and non-anterior approach total hip arthroplasty: a single institution experience. Bone Joint J 2019; 101(6_Supple_B): 2–8.
Kim HS, Park JW, Moon SY, Lee YK, Ha YC, Koo KH. Current and future burden of periprosthetic joint infection from national claim database. J Korean Med Sci. 2020;35(49):e410. https://doi.org/10.3346/jkms.2020.35.e410. (PMID: 33350183; PMCID: PMC7752258).
Jin X, Gallego Luxan B, Hanly M, Pratt NL, Harris I, de Steiger R, Graves SE, Jorm L. Estimating incidence rates of periprosthetic joint infection after hip and knee arthroplasty for osteoarthritis using linked registry and administrative health data. Bone Joint J. 2022;104-B(9):1060–6. https://doi.org/10.1302/0301-620X.104B9.BJJ-2022-0116.R1.
Parker MJ, Livingstone V, Clifton R, McKee A. Closed suction surgical wound drainage after orthopaedic surgery. Cochrane Database Syst Rev. 2007;3:CD001825.
Zhu Y, Zhang F, Chen W, Liu S, Zhang Q, Zhang Y. Risk factors for periprosthetic joint infection after total joint arthroplasty: a systematic review and meta-analysis. J Hosp Infect. 2015;89(2):82–9. https://doi.org/10.1016/j.jhin.2014.10.008.
Zhang Q, Dong J, He J, Zhu J, Yang X. The effect of tourniquet use in total knee arthroplasty: grading the evidence through an updated meta-analysis of randomized, controlled trials. J Arthroplasty. 2017;32(9):S177–83.
Magan AA, Dunseath O, Armonis P, Fontalis A, Kayani B, Haddad FS. Tourniquet use in total knee arthroplasty and the risk of infection: a meta-analysis of randomised controlled trials. J Exp Orthop. 2022;9(1):62. https://doi.org/10.1186/s40634-022-00485-9.PMID:35776268;PMCID:PMC9249956.
Poultsides LA, Memtsoudis SG, Vasilakakos T, Wanivenhaus F, Do HT, Finerty E, Alexiades M, Sculco TP. Infection following simultaneous bilateral total knee arthroplasty. J Arthroplast. 2013. https://doi.org/10.1016/j.arth.2013.07.005.
Hart A, Antoniou J, Brin YS, Huk OL, Zukor DJ, Bergeron SG. Simultaneous bilateral versus unilateral total knee arthroplasty: a comparison of 30-day readmission rates and major complications. J Arthroplasty. 2016;31(1):31–5. https://doi.org/10.1016/j.arth.2015.07.031. (Epub 2015 Jul 21 PMID: 26297691).
Xu C, Qu P, Deng T, Bell K, Chen J. Does simultaneous bilateral total joint arthroplasty increase deep infection risk compared to staged surgeries? A meta-analysis. J Hosp Infect. 2019;101(2):214–21. https://doi.org/10.1016/j.jhin.2018.08.019. (Epub 2018 Sep 4 PMID: 30194025).
Acknowledgements
Not Applicable.
Funding
No funding was obtained for this research.
Author information
Authors and Affiliations
Contributions
WJ and ZJ developed the idea and designed the methods. ZJ, KH and YH collected the data. ZJ, AA and AS analyzed, interpreted and presented the results. All authors wrote the manuscript. WJ, ZJ and AA critically revised the manuscript for content and finalization. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by King Abdullah International Medical Research Center (KAIMRC). Institutional review board number NRC21R/446/10. The requirement for informed consent was waived due to the retrospective nature of this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Aljuhani, W.S., Alanazi, A.M., Saeed, A.I. et al. Patient-related risk factors of prosthetic joint infections following total hip and knee arthroplasty at King Abdulaziz Medical City, a 10-year retrospective study. J Orthop Surg Res 18, 717 (2023). https://doi.org/10.1186/s13018-023-04210-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-023-04210-9