
Abstract
Background
Open-wedge high tibial osteotomy (OWHTO) is commonly performed for the treatment of medial compartment knee osteoarthritis (KOA), and is classified into proximal tibial tubercle osteotomy (PTO) and distal tibial tubercle osteotomy (DTO). The PTO osteotomy point is generally located about 3–4 cm below the joint of the proximal tibia, and the osteotomy line points to the upper part of the proximal tibiofibular joint. The DTO osteotomy point is generally located about 0.5–1.0 cm below the tibial tubercle, and the osteotomy line points to the contralateral cortex. However, there is currently no consensus on which surgical technique is superior. The purpose of our study was to investigate which among the two is superior for medial KOA, with respect to knee joint parameters, clinical function, and complications.
Methods
This study was conducted as per the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The Cochrane Central Library, MEDLINE, Embase, PubMed, CNKI, and WanFang databases were systematically searched for trials comparing PTO and DTO in patients with medial compartment KOA, from inception until March 2022. The meta-analysis was conducted using RevMan 5.2 software. The Cochrane risk-of-bias tool was used to assess methodological quality. Statistical analysis was performed with Stata 12.0. Outcomes of interest included the Insall-Salvati index (ISI), Caton-Deschamps index (CDI), Blackburne-Peel index (BPI), posterior tibial slope (PTS), and the Hospital for Special Surgery (HSS) knee-rating scale.
Results
A total of 15 retrospective studies (910 knees) were included. There were no significant differences in the age or sex of included patients. There was a significant difference in the ISI, CDI, BPI, and PTS between the two groups (all p ≤ 0.05). Further, DTO was associated with a significantly greater number of postoperative complications (p < 0.05) compared to PTO. However, there was no significant difference in the femorotibial angle (FTA), mechanical medial proximal tibial angle (mMPTA), and HSS knee score (all p > 0.05).
Conclusions
Compared with DTO, PTO is associated with a greater incidence of postoperative patella baja and increased PTS, whereas DTO is associated with more postoperative complications. Nevertheless, both can significantly correct knee varus deformity and improve knee function; their early knee function scores are also similar.
Trial Registration. Prospective Register of Systematic Reviews (PROSPERO) registration number CRD42021284443.
Similar content being viewed by others


Background
Conventional medial open-wedge high tibial osteotomy (OWHTO) is commonly performed for the treatment of medial compartment knee osteoarthritis (KOA) with good clinical efficacy. Depending on the osteotomy position, OWHTO can be divided into proximal tibial tubercle osteotomy (PTO) and distal tibial tubercle osteotomy (DTO) [1, 2]. Recently, several studies have shown that PTO increases contact pressure in the patellofemoral (PF) joint, leads to patella baja, and increases the posterior tibial slope (PTS) [3,4,5]. The occurrence of patella baja can affect the biomechanics of the knee, causing anterior knee pain, patellofemoral arthritis, and reduced range of motion of the knee joint. Further, patella baja and increased PTS may make the revision of total knee arthroplasty difficult and affect subsequent rehabilitation [3, 6]. Studies have shown that about 20% of patients with high osteotomy require TKA after 10 years. Reduced patella height may increase the difficulty of knee replacement. DTO can avoid patella baja and patellar tendon, resulting in scar contraction. Strong internal fixation can improve the defect of long healing time, and has less influence on future joint replacement. Therefore, TKA after PTO is more difficult compare to DTO [7]. The progression of patellofemoral OA due to patella baja is reported as a particular complication related to PTO. In PTO, the tibial tubercle is attached to the distal tibia fragment by ascending osteotomy of the tibial tubercle; therefore, a gap opening at the transverse osteotomy may induce patella baja and a change in patella tracking [8]. It may result in lateral displacement of the tibial tubercle, which lead to an increase in contact pressure or adhesions of the patella ligament [9], and consequent cartilage degeneration in the patellofemoral joint. However, the cause of patellar arthritis after OWHTO is still inconclusive and needs further study. Kim et al. [10] in a study of 114 patients, found that the incidence of patellofemoral OA in the femoral trochlea was 41.2% 2 years after PTO, while that in the patellar articular surface was 21.9%. As per the existing literature, increased PTS may contribute to anterior cruciate ligament (ACL)-injuries, and may be associated with a higher risk of ACL reconstruction failure [11]. There are many disadvantages to DTO, such as the high likelihood of the screw being inserted into the tibial tubercle and penetrating the posterior tibial cortex, which may injure the popliteal neurovascular bundle. Owing to the irregular anatomy of the proximal tibia, the fixation screws for the tibial tubercle after PTO osteotomy need to be implanted from front to back, which further increases the risk of posterior vascular and nerve injury [12,13,14]. To the best of our knowledge, there is no relevant meta-analysis discussing the difference between PTO and DTO techniques in the treatment of medial compartment KOA. Therefore, we performed a meta-analysis of related clinical studies to determine whether PTO is superior to DTO in the treatment of medial compartmental KOA. The aim of the study was to assess whether DTO would change the patellar height (PH) and PTS, and result in improved clinical outcomes compared to PTO. The study hypothesis was that after DTO, (1) there is no changes in patellar position or (2) there is no increased PTS, and (3) there would be clinical improvement as objectively measured by the HSS score.
Materials and methods
Methodology
The meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and the Guidelines for Meta-Analysis (PRISMA) [15]. We searched PubMed, Cochrane Library, Embase, MEDLINE, CNKI, and Wanfang for clinical studies comparing PTO and DTO in the treatment of unicompartmental osteoarthritis of the knee, from inception until March 2022, with no language constraints. RevMan 5.2(Review Manager (RevMan) [Computer program]. Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012.) software was used to carry out the meta-analysis. We optimized the search with the following keywords: (high tibial osteotomy OR open-wedge osteotomy OR open-wedge proximal tibial osteotomy OR open wedge high tibial osteotomy) and (proximal tibial tubercle osteotomy OR descending HTO OR supra-tubercle cut OR monoplanar, distal tibial tubercle osteotomy OR ascending HTO OR infra-tubercle cut OR biplanar). In addition, we examined the list of references in all the included papers to help identify studies that met the inclusion criteria.
Criteria for inclusion and exclusion
The inclusion criteria were as follows: (1) research design: retrospective studies, prospective cohort studies, and randomized controlled trials, (2) participants: patients with OA in the medial compartment of the knee joint, (3) comparison of DTO and PTO outcomes, and (4) inclusion of the following indicators: PH of CDI or BP or ISI, femorotibial angle (FTA), mechanical medial proximal tibial angle (mMPTA), PTS, HSS knee score, and postoperative complications.
Exclusion criteria were (1) Reports on either DTO or PTO (2) non-clinical reports, (3) duplicate publications, (4) meeting proceedings, (5) studies with the above evaluation parameters not included.
Data extraction
Data were collected by two researchers based on the same inclusion criteria, and were checked by a third researcher. Differences were resolved by mutual consensus. The corresponding authors were contacted when data or necessary supporting information was missing. The following data were collected: (1) study information (i.e., author, year of publication, and type of study), (2) study population information (i.e., age, sex), (3) surgery type and follow-up, and (4) principal outcomes (i.e., PH, FTA, mMPTA, PTS, HSS knee score, and complications. As for PH, it included the BPI, ISI, and CDI.
Quality assessment
The risk of bias in the methodological quality of the RCTs was assessed using tools from the Cochrane Collaboration, collected by two independent researchers, and verified by a third researcher [16]. The evaluation included seven items: subject blinding, randomization, missing data, allocation concealment, outcome evaluator blinding, selective reporting, and other biases. Deviation risk was rated as "low", "high," or "uncertain". The nonrandomized studies were evaluated by the Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I) assessment tool [17]. Evaluation is mainly based on the following seven aspects: bias due to confounding, bias in the selection of participants, bias in the measurement of interventions, bias due to departures from intended interventions, bias due to missing data, bias in the measurement of outcomes, and bias in the selection of the reported result.
Statistical analysis
The meta-analysis was performed by RevMan 5.2 software, provided by the Cochrane Collaboration. Heterogeneity tests were performed on the 95% confidence intervals (CIs). The mean (MD) and standard deviation (SD) were calculated for quantitative data, and the odds ratio (OR) with 95% CIs were calculated for count data. A p value less than 0.05 was considered statistically significant (p < 0.05). The Q test and I2 value were used to determine statistical heterogeneity between the included studies. I2 ≤ 50% indicated absence of statistical heterogeneity, and the fixed-effect model was adopted, while I2 ≥ 50% indicated statistical heterogeneity among the included studies, we used a model of random effect.
Results
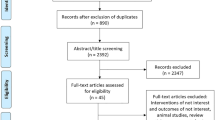
After evaluation, 15 studies met the requirements for inclusion in this meta-analysis, providing a combined sample size of 910 knees (Fig. 1).

The flow chart of literature screening
Risk of bias assessment
All the 15 studies included were retrospective studies (i.e., nRCTs); therefore, were evaluated using the ROBINS-I assessment tool [17], as shown in Table 1. These studies were independently evaluated by two authors and disputes were resolved by a third author until consensus was reached.
Outcome measure
Insall-Salvati index (ISI)
Six studies reported the ISI [18,19,20,21,22,23]; the combined results suggested that PTO decreased the ISI (weighted mean difference (WMD) = -0.08, 95% CI = (-0.15 to 0.00), p = 0.05, I2 = 85%) (Fig. 2).

Forest plot of ISI
Caton-Deschamps index (CDI)
Eight studies [13, 19, 20, 22, 24,25,26,27] r reported the CDI; the combined results suggested that PTO decreased the CDI (WMD = -0.06, 95% CI = (-0.08 to -0.04), p < 0.00001, I2 = 0%) (Fig. 3).

Forest plot of CDI
Blackburne-Peel index (BPI)
Four studies [13, 18, 19, 22] reported the BPI; the combined results suggested that PTO decreased the BPI (WMD = -0.06, 95% CI = (-0.09 to -0.03), p < 0.0001, I2 = 0%) (Fig. 4).

Forest plot of BPI
Posterior tibal slope (PTS)
Eleven studies [13, 18,19,20,21,22, 25,26,27,28] reported the PTS. Since significant heterogeneity was noted among the study groups (I2 = 55%; MD = 0.33, 95% CI: -0.02–0.69, p = 0.01), the random-effects model was adopted. Sensitivity analysis found that the variance of PTS data in one study was not consistent with that in other studies, possibly due to its different measurement methods, and heterogeneity was reduced when this data was removed (I2 = 43%). The results showed that PTO increased PTS (WMD = 0.77, 95% CI = (0.28 to 1.26), p < = 0.002, I2 = 43%) (Fig. 5).

Forest plot of PTS
Femoro tibal angle (FTA)
Eight studies [13, 18, 21,22,23, 26,27,28] reported the FTA; the results suggested no major difference in the FTA between the two groups (WMD = 0.01, 95% CI = (-0.30 to 0.33), p = 0.93, I2 = 31%) (Fig. 6).

Forest plot of FTA
Mechanical medial proximal tibial angle (mMPTA)
Four studies [22, 24, 27, 28] reported the mMPTA; the combined results showed no significant difference in the mMPTA between the two groups (WMD = 0.21, 95% CI = (-0.30 to 0.72), p = 0.43, I2 = 0%) (Fig. 7).

Forest plot of mMPTA
HSS knee score
Five studies [18, 21, 23, 26, 27] reported the HSS knee score; the combined results showed no significant difference in the HSS knee score between the two groups (WMD = -0.14, 95% CI = (-0.68 to 0.39), p = 0.59, I2 = 0%) (Fig. 8).

Forest plot of HSS knee score
Complications
Five studies [12, 18, 19, 23, 29] reported postoperative complications. The complications reported in the included studies mainly included tibial tuberosity fracture, wound infection, and delayed union or nonunion, all of which could be resolved by routine non-surgical treatment. The results suggested that DTO was associated with a greater number of complications (WMD = 0.21, 95% CI = (0.06 to 0.74), p = 0.01, I2 = 0%) (Fig. 9). In the PTO group, only one patient developed a superficial infection. In the DTO group, 12 patients experienced complications: one had deep vein thrombosis, one developed surgical site infection, two patients had delayed wound healing, one had screw dislocation, three patients had tubercle fracture, and four patients were diagnosed with patellar fractures.

Forest plot of complications
Discussion
In this meta-analysis, a total of 15 studies with 910 participants were included to compare whether PTO was superior to DTO in the treatment of medial KOA. The following conclusions were drawn: ①Compared with DTO, PTO was more likely to result in postoperative patella baja, and increase postoperative PTS. ②Compared with PTO, DTO had a higher incidence of postoperative complications. ③The HSS knee score was not different between the two groups. ④Both PTO and DTO increased the mMPTA and FTA, and the extent of increase was not significantly different between the two groups.
To our knowledge, proponents in the field of orthopedic surgery have promoted OWHTO as a common knee surgery since it can reduce the pressure on the medial compartment of the knee joint by correcting the limb alignment, thereby slowing down the progress of the disease, reducing pain, improving symptoms, and avoiding TKA [30,31,32]. However, OWHTO is associated with several complications, such as the change in PH, increase in PTS, bone nonunion, and loss of correction angle, among others [33, 34]. OWHTO is classified into PTO and DTO. Theoretically, PTO has fewer complications and is more conducive to healing than DTO, which is consistent with our study conclusion. DTO does not lead to patella baja, and the osteotomy line is located at the lower 1/3 of the tibial tubercle which have little affect the original morphology and biomechanics of the patellofemoral joint, and may be more beneficial for long-term follow-up. For medial compartment osteoarthritis and varus knee, DTO has less impact on future TKA [46].
The decrease of PH in PTO may cause patella baja and increased PTS in the sagittal plane [4, 35, 36]. In PTO, the osteotomy surface is located on the tibial tubercle. In the process of correction, the tibial tubercle can shift laterally and distally, inevitably leading to a drop in the patellar position. The greater the degree of correction, the more obvious the change in patellar position. This explains the occurrence of postoperative patella baja [12, 37]. In addition, the occurrence of patella baja can seriously affect the joint range of motion and increase the difficulty of TKA in the future [38, 39]. Theoretically, compared with PTO, the osteotomy surface in DTO is under the tibial tubercle; thus, the structure or position of the proximal tibia remains unchanged during the orthopedic process. In view of this advantage, DTO is increasingly being favored by orthopedic surgeons. Recently, several studies [20, 21, 23] have confirmed that there is little change in the patellar position after DTO, consistent with the results of our meta-analysis. Therefore, when the degree of correction is large, we recommend DTO to avoid postoperative patella baja.
The tension in the cruciate ligament and the pressure on the tibial plateau are both influenced by PTS. When the PTS angle is too large, it causes anterior and posterior instability and leads to ACL degeneration [40]. On the contrary, when the PTS angle is too small, the patient's knee flexion-gap increases, resulting in knee instability [41]. Therefore, the interference of PTS needs to be reduced in all knee surgeries. As per reports, PTS increase after OWHTO [42, 43] may be due to the unique anatomical features of the proximal tibia [37, 44]. PTS may also be increased when the osteotomy plane is not level with the sagittal tibial articular plane, the osteotomy gap is wide in the front and narrow at the back, and in cases of hinge fracture [45]. This study found that PTS differed between PTO and DTO, with the PTS in PTO being significantly higher. This may be because the osteotomy surface in PTO is located at the tibial junction. During the orthopedic process, the patellar tendon is subjected to traction during the osteotomy, which is more likely to cause an imbalance between the anterior and posterior osteotomy. However, there is no traction of the patellar tendon in DTO, which was found to have little impact on PTS in this study.
Theoretically, the greater the angle of PTO correction, the easier it is for patella baja to occur. In our study, this was reaffirmed by the lack of difference found between PTO and DTO in the degree of correction (MPTA), thereby excluding the influence of the degree of correction on the position of patella. The meta-analysis also found no difference in the HSS knee function score in the short term between PTO and DTO. Although, when compared with DTO, PTO can lead to a decline in patellar position and an increase in PTS, both of them can significantly improve knee function.
The most common complications after OWHTO are tibial plateau fracture and infrapatellar nerve injury, in addition to complications of conventional lower extremity surgery, such as infections, deep vein thrombosis, and delayed healing of the osteotomy surface [46]. In PTO, the patellar tendon works as a tension band for the anterior flange, which provides the compressive force to the coronal osteotomy plane during knee flexion. On the other hand, in DTO, the patellar tendon can detach the flange during knee flexion. Moreover, we should be paid great attention to during the DTO to avoid excessive penetration of the posterior cortex, which involves a potential risk of popliteal neurovascular bundle injury [47]. Another point to note in surgery is that the tibial tubercle is disadvantageous for bone healing due to its high proportion of cortical bone. Furthermore, screw fixation can be a cause of infection because of the skin irritation by the screw head, which may result in delayed union. The thicker flange for preventing the tuberosity fracture may make the thinner hinge, which can be the source of hinge fracture [48]. The above points are consistent with the results of this study, in that compared with PTO, the incidence of complications with DTO was higher.
Our study had several limitations. First, the studies included were retrospective in design, and the difference in relevant statistical indicators might have been caused by varying skills and expertise of surgeons, or differences in patients themselves, resulting in statistical heterogeneity. Second, the number of included cases was small. Third, most of the included studies had short periods of follow-up and did not reflect differences in long-term outcomes. Finally, the correlation between preoperative and postoperative HSS functional scores, PTS, and tibiofemoral angle changes were not assessed, and need further study.
Conclusions
In this meta-analysis, we found that in comparison to DTO, PH was more likely to decrease and PTS was more likely to increase in PTO. Compared with PTO, DTO was associated with a greater frequency of complications. There were some differences in knee-joint parameters between PTO and DTO; however, their early clinical effects were similar and no differences were observed. We hope that our study provides further clinical evidence for both clinicians and patients making decisions regarding the operation method of OWHTO for medial compartmental OA.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- OWHTO:
-
Open-wedge high tibial osteotomy
- KOA:
-
Knee osteoarthritis
- TKA:
-
Total knee arthroplasty
- PTO:
-
Proximal tibial tubercle osteotomy
- DTO:
-
Distal tibial tubercle osteotomy
- ISI:
-
Insall-Salvati index
- CDI:
-
Caton-Deschamps index
- BPI:
-
Blackburne-Peel index
- PTS:
-
Posterior tibial slope
- HSS:
-
Hospital for Special Surgery
References
Lobenhoffer P, Agneskirchner JD. Improvements in surgical technique of valgus high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2003;11(3):132–8.
Staubli AE, De Simoni C, Babst R, et al. TomoFix: a new LCP-concept for open wedge osteotomy of the medial proximal tibia–early results in 92 cases. Injury. 2003;34(Suppl 2):B55-62.
El-Azab H, Glabgly P, Paul J, et al. Patellar height and posterior tibial slope after open- and closed-wedge high tibial osteotomy: a radiological study on 100 patients. Am J Sports Med. 2010;38(2):323–9.
El-Azab H, Halawa A, Anetzberger H, et al. The effect of closed- and open-wedge high tibial osteotomy on tibial slope: a retrospective radiological review of 120 cases. J Bone Joint Surg Br. 2008;90(9):1193–7.
Kesmezacar H, Erginer R, Ogut T, et al. Evaluation of patellar height and measurement methods after valgus high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2005;13(7):539–44.
Agneskirchner JD, Hurschler C, Stukenborg-Colsman C, et al. Effect of high tibial flexion osteotomy on cartilage pressure and joint kinematics: a biomechanical study in human cadaveric knees. Winner of the AGA-DonJoy Award 2004. Arch Orthop Trauma Surg. 2004;124(9):575–84.
Hui C, Salmon LJ, Kok A, et al. Long-term survival of high tibial osteotomy for medial compartment osteoarthritis of the knee. Am J Sports Med. 2011;39(1):64–70.
Tanaka T, Matsushita T, Miyaji N, et al. Deterioration of patellofemoral cartilage status after medial open-wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2019;27(4):1347–54.
Gaasbeek R, Welsing R, Barink M, et al. The influence of open and closed high tibial osteotomy on dynamic patellar tracking: a biomechanical study. Knee Surg Sports Traumatol Arthrosc. 2007;15(8):978–84.
Kim KI, Kim DK, Song SJ, et al. Medial open-wedge high tibial osteotomy may adversely affect the patellofemoral joint. Arthroscopy. 2017;33(4):811–6.
Shao Q, Macleod TD, Manal K, et al. Estimation of ligament loading and anterior tibial translation in healthy and ACL-deficient knees during gait and the influence of increasing tibial slope using EMG-driven approach. Ann Biomed Eng. 2011;39(1):110–21.
Gaasbeek RD, Sonneveld H, van Heerwaarden RJ, et al. Distal tuberosity osteotomy in open wedge high tibial osteotomy can prevent patella infera: a new technique. Knee. 2004;11(6):457–61.
Horikawa T, Kubota K, Hara S, et al. Distal tuberosity osteotomy in open-wedge high tibial osteotomy does not exacerbate patellofemoral osteoarthritis on arthroscopic evaluation. Knee Surg Sports Traumatol Arthrosc. 2020;28(6):1750–6.
van Egmond N, van Grinsven S, van Loon CJ, et al. Better clinical results after closed- compared to open-wedge high tibial osteotomy in patients with medial knee osteoarthritis and varus leg alignment. Knee Surg Sports Traumatol Arthrosc. 2016;24(1):34–41.
Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7): e1000097.
Furlan AD, Pennick V, Bombardier C, et al. 2009 updated method guidelines for systematic reviews in the Cochrane Back Review Group. Spine. 2009;34(18):1929–41.
Sterne JA, Hern NMA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:4919.
Elmali N, Esenkaya I, Can M, et al. Monoplanar versus biplanar medial open-wedge proximal tibial osteotomy for varus gonarthrosis: a comparison of clinical and radiological outcomes. Knee Surg Sports Traumatol Arthrosc. 2013;21(12):2689–95.
Hoon P, Woo KH, Hwa KJ, et al. Open wedge high tibial osteotomy with distal tubercle osteotomy lessens change in patellar position. BioMed Res Int. 2017;2017:4636809.
Krause M, Drenck TC, Korthaus A, et al. Patella height is not altered by descending medial open-wedge high tibial osteotomy (HTO) compared to ascending HTO. Knee Surg Sports Traumatol Arthrosc. 2018;26(6):1859–66.
Chen YM. Comparative study on the clinical efficacy of upward and downward osteotomy of the medial tibial high biplane. Beihua University; 2019.
Du G, Pei B, Wu L, et al. Effect of ascending or descending medial tibial open wedge osteotomy on patellar height. J Pract Orthop. 2020;26(12):1097–102.
Na L, Desheng C, Binggang W. Comparison of supraticotuberous and subtuberous osteotomy in the treatment of single-room knee osteoarthritis. J Pract Orthop. 2015;21(11):983–7.
Ogawa H, Matsumoto K, Yoshioka H, et al. Distal tibial tubercle osteotomy is superior to the proximal one for progression of patellofemoral osteoarthritis in medial opening wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2020;28(10):3270–8.
Gooi SG, Chan CXY, Tan MKL, et al. Patella Height Changes Post High Tibial Osteotomy. Indian J Orthop. 2017;51(5):545–51.
Zhang ZB, Chen XH, Zhang QW, et al. Comparison of efficacy of single-plane and biplane high tibial osteotomy in the treatment of knee osteoarthritis. Front Med. 2020;10(15):56–7.
Zhang BW. A comparative study of open wedge high tibial osteotomy between distal and proximal tibial nodules in the treatment of knee osteoarthritis with genu varus. Anhui Medical University; 2021.
Jianchun Z, Yirong Z, Wei L, et al. Effects of single-plane and biplane osteotomy on posterior tibial inclination after OWHTO. J Appl Orthop. 2020;26(07):609–13.
Hinterwimmer S, Beitzel K, Paul J, et al. Control of posterior tibial slope and patellar height in open-wedge valgus high tibial osteotomy. Am J Sports Med. 2011;39(4):851–6.
Akizuki S, Shibakawa A, Takizawa T, et al. The long-term outcome of high tibial osteotomy: a ten- to 20-year follow-up. J Bone Joint Surg Br. 2008;90(5):592–6.
Bode G, von Heyden J, Pestka J, et al. Prospective 5-year survival rate data following open-wedge valgus high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2015;23(7):1949–55.
Spahn G, Hofmann GO, von Engelhardt LV, et al. The impact of a high tibial valgus osteotomy and unicondylar medial arthroplasty on the treatment for knee osteoarthritis: a meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2013;21(1):96–112.
Chae DJ, Shetty GM, Lee DB, et al. Tibial slope and patellar height after opening wedge high tibia osteotomy using autologous tricortical iliac bone graft. Knee. 2008;15(2):128–33.
Magyar G, Toksvig-Larsen S, Lindstrand A. Changes in osseous correction after proximal tibial osteotomy: radiostereometry of closed- and open-wedge osteotomy in 33 patients. Acta Orthop Scand. 1999;70(5):473–7.
Brouwer RW, Bierma-Zeinstra SM, Van Koeveringe AJ, et al. Patellar height and the inclination of the tibial plateau after high tibial osteotomy. The open versus the closed-wedge technique. J Bone Joint Surg. 2005;87(9):1227–32.
Cullu E, Aydoğdu S, Alparslan B, et al. Tibial slope changes following dome-type high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2005;13(1):38–43.
Giffin JR, Vogrin TM, Zantop T, et al. Effects of increasing tibial slope on the biomechanics of the knee. Am J Sports Med. 2004;32(2):376–82.
Grelsamer RP. Patella baja after total knee arthroplasty: Is it really patella baja? J Arthroplasty. 2002;17(1):66–9.
Jie L, Xianhua L, Ning Li, et al. Progressive inferior patellar syndrome. Chin J Orthop Surg. 2001;09:25–7.
Suzuki T, Ryu K, Kojima K, et al. The effect of posterior tibial slope on joint gap and range of knee motion in mobile-bearing unicompartmental knee arthroplasty. J Arthroplasty. 2019;34(12):2909–13.
Li MZ. Mete analysis of single condylar mobile platform prosthesis and fixed platform prosthesis in the treatment of knee arthroplasty. Chongqing Medical University; 2021.
Dragosloveanu S, Cristea S, Dragosloveanu C. The effect of high tibial osteotomy on the posterior tibial slope. Maedica. 2014;9(2):173–8.
Jacobi M, Villa V, Reischl N, et al. Factors influencing posterior tibial slope and tibial rotation in opening wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2015;23(9):2762–8.
Noyes FR, Goebel SX, West J. Opening wedge tibial osteotomy: the 3-triangle method to correct axial alignment and tibial slope. Am J Sports Med. 2005;33(3):378–87.
Hanada M, Hotta K, Matsuyama Y. A computer simulation study for preserving the tibial posterior slope in open-wedge high tibial osteotomy. Eur J Orthop Surg Traumatol. 2020;30(7):1285–91.
Zhu JW, Chen DS, Wang TF, et al. Analysis of complications after medial opening wedge high tibial osteotomy. Chin J Surg. 2020;58(6):447–51.
Hou XB. Research progress of complications associated with open wedge high tibial osteotomy. J Orthop Clinic Res 2021;6(03):174–9.
Ogawa H, Matsumoto K, Yoshioka H, Sengoku M, Akiyama H. Fracture of the tibial tubercle does not affect clinical outcomes in medial opening wedge high tibial osteotomy with distal tibial tubercle osteotomy. Arch Orthop Trauma Surg. 2022;142(4):607–13.
Funding
This work was supported by Basic and Applied Basic Research Project of Guangdong Province (Grant numbers 2023A1515012615); Science and Technology Project of Guangzhou (Grant Number: 202002030204); Medical Science and Technology Research Fund Project of Guangdong Province of China (Grant Number: A2021463). The funding bodies had no role in the design of the study, the collection, analysis, or interpretation of the data, or writing the manuscript.
Author information
Authors and Affiliations
Contributions
Conceptualization: Min Song, Weichang Han. Data extraction: Xiaodong Lin, Jingyi Li. Investigation: Xiaodong Lin, Weichang Han. Methodology: Min Song, Jingyi Li. Project administration: Wengang Liu. Resources: Xiaodong Lin, Jingyi Li. Software: Weichang Han. Writing- original draft: Min Song, Xiaodong Lin. Writing- review & editing: Wengang Liu. Min Song orcid: 0000–0003-0960–1964.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not Applicable.
Consent for publication
Not Applicable.
Competing interests
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Song, M., Lin, X., Han, W. et al. Is proximal tibial tubercle osteotomy superior to distal tibial tubercle osteotomy for medial compartmental osteoarthritis? A meta-analysis. J Orthop Surg Res 18, 245 (2023). https://doi.org/10.1186/s13018-023-03725-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-023-03725-5