
Abstract
Background
Osteoarthritis of the knee is an irreversible disease that causes great pain, and genetic factors play an important role in its occurrence and development. There have been many studies on the correlation between ADAM12 polymorphisms and genetic susceptibility to osteoarthritis, but the results remain inconclusive.
Methods
Papers from PubMed, Web of Science, EMbase, Springer, SCOPUS, Google Scholar and other databases were systematically retrieved with a cut-off of January 2022. All case–control studies on ADAM12 rs3740199, rs1871054, rs1044122, and rs1278279 polymorphisms and osteoarthritis were searched. Fixed or random effects models were used for pooled analysis with OR values and 95% confidence intervals (CI), and publication bias was assessed. In addition, the false-positive reporting probability test was used to assess the confidence of a statistically significant association.
Results
Eleven articles were included, which included 3332 patients with osteoarthritis and 5108 healthy controls. Meta-analysis showed that the rs1871054 polymorphism of ADAM12 was associated with osteoarthritis in dominant, recessive, allelic, and homozygote genetic models [C vs. T: OR = 1.34 95% CI (1.05, 1.71), P < 0.001]. Our subgroup analysis revealed an association between the ADAM12 polymorphism rs1871054 in Asians and osteoarthritis [C vs. T: OR = 1.61, 95% CI (1.25, 2.08), P < 0.001], albeit this was only for three studies. In addition, the ADAM12 polymorphism rs1871054 is associated with osteoarthritis in patients younger than 60 years of age [C vs. T: OR = 1.39, 95% CI (1.01, 1.92), P = 0.289]; however, the ADAM12 gene rs3740199, rs1044122, and rs1278279 site polymorphisms were not significantly. Furthermore, when assessing the confidence of the positive results, the positive results were found to be credible (except for Age < 60).
Conclusion
Polymorphism at the rs1871054 site of ADAM12 is associated with genetic susceptibility to osteoarthritis, but rs3740199, rs1044122, and rs1278279 site polymorphisms are not.
Similar content being viewed by others


Introduction
Osteoarthritis (OA) is a chronic progressive joint disease with increasing incidence with age. It can occur in any joint of the body and is characterized by damage to articular cartilage, subchondral sclerosis, and osteophyte formation [1]. Studies have shown that the global prevalence of OA of the knee or hip are 3.8% and 0.85%, respectively [2]. The prevalence of OA is expected to continue to increase in the future due to the aging of the global population, but the etiology of OA is still unknown. Many studies argue that OA is a multifactorial disease, and genetic and environmental factors (age, sex, obesity, physical activity, major trauma, occupation, etc.) are closely related to its development [3, 4]. In recent years, many researchers have attempted to explore the causes of OA at the genetic level, and a variety of genes that may be associated with OA have been identified, including ADAM12, vitamin D receptor, matrix metalloproteinases, estrogen receptor, and interleukins [5,6,7,8]. Currently, it has been found that the mutation of IL-1Ra Ser133Ser does not appear to be associated with immune-mediated and inflammatory diseases in a variety of genetic patterns, suggesting that the mutant allele C of IL-1Ra Ser133Ser does not increase the risk of disease [9]. Studies have also shown that mutations in inflammatory cytokines (G allele at rs361525, T allele at rs419598, and A allele at rs2228145) can lead to increased prevalence of coronavirus disease 2019 [10]. This provides more reliable and sound evidence for basic research and clinical treatment. In addition, since it is difficult to make early diagnosis of basic biomarkers with traditional biomarkers (tumor necrosis factor α, C-reactive protein, cytokines, etc.) [11], the research of new therapeutic options (nanotechnology [11, 12], targeted drugs [11], autophagy regulatory drugs [13], etc.) is also plagued by non-specific targets. Such studies could help in the search for new treatments.
ADAM12 (a disintegrin and metalloproteinase domain 12) is an active protease that is mainly responsible for protein decomposition, adhesion, and signal transduction [14]. It belongs to the ADAM family and is involved in the formation and proliferation of chondrocytes and the differentiation of osteoclasts [15, 16]. Some studies have shown that ADAM12 expression increases continuously in patients with OA [17, 18], and neutralizing antibodies against ADAM12 can significantly reduce the degradation of oligomeric cartilage proteins [19]. Other studies have shown that ADAM12 can promote the proliferation and maturation of chondrocytes by inhibiting insulin-like growth factor 1 (IGF-1) signaling pathway and regulating metalloproteinases and adhesion activities [16, 20]. When ADAM12 genes is mutated, ADAM12 is overexpressed in joints [21], and this protein overexpression induces inflammation by participating in cytokine receptor interactions and the osteoclast differentiation pathway [22]. In addition, ADAM12 polymorphism affects the balance between synthesis and degradation of extracellular matrix (ECM), leading to degradation of chondrocytes [16, 20]. These evidences suggest that ADAM12 is vital in the development of OA.
ADAM12 is expressed in both normal and arthritic articular cartilage. The occurrence and development of OA can be affected by polymorphisms in the ADAM12 gene, and the differences in protein activity and conformation caused by ADAM12 may have varying effects on articular cartilage [5, 21, 23]. In recent years, ADAM12 gene polymorphisms have become a hot topic in the search for genetic factors related to OA risk [24]. ADAM12 mutation is also associated with the severity of OA [25]. So far, there is no consensus on whether ADAM12 polymorphisms are related to disease susceptibility, severity, or phenotype. A study on Estonian patients suggested that ADAM12 gene polymorphisms were closely associated with the occurrence of knee arthritis [26], and the rs1871054 intron C allele was considered to confer susceptibility to advanced OA. A recent Asian study showed similar results [24] and found that this was more likely to occur in female patients. A meta-analysis of ADAM12 suggested a positive correlation with male sex of patients [27]. However, a European study found no significant association between ADAM12 polymorphisms and knee OA [5]. There is still great controversy regarding the relationship between ADAM12 polymorphisms and OA. Is the ADAM12 gene related to OA and gender? In this study, a meta-analysis was conducted on the correlation between G/C, T/C, G/A, and T/C polymorphisms of rs3740199, rs1871054, rs1044122, and rs1278279 of ADAM12 and OA, to evaluate whether ADAM12 mutations are related to susceptibility to OA.
Data and methods
Literature retrieval strategy
We conducted a systematic search for case–control studies of ADAM12 polymorphisms and OA on the Web of Science, PubMed, EMbase, Cochrane Library, SCOPUS, Google Scholar and other databases, with a cut-off of January 2022. There was no language restriction. We searched for keywords including “osteoarthritis,” “OA,” “degenerative joint disease,” “ADAM12,” “gene polymorphism," and “polymorphism”. All obtained studies were screened, and references to relevant articles were retrieved to make the included studies more accurate and comprehensive.
Inclusion and exclusion criteria
Inclusion criteria: (1) Subjects were diagnosed with OA; (2) The study concerned the relationship between ADAM12 polymorphisms and OA; (3) Allele or genotype distribution frequency data were available; (4) Genotypic distribution conformed to Hardy–Weinberg equilibrium (HWE). The exclusion criteria were as follows: (1) Repeated studies and publications; (2) Reviews of literature, case reports, and conference abstracts; (3) animal experiments; and (4) studies with a Newcastle–Ottawa scale (NOS) score < 6 [28].
Literature screening
Data were independently extracted from all eligible studies by two researchers, cross-checked, and discussed with the assistance of a third researcher in cases of disagreement. Information was collected, including author, year of publication, study area, OA site, diagnostic criteria, genotyping method, total number of cases and controls, and ADAM12 genotype frequency.
Quality evaluation
Two researchers independently evaluated eligible studies using the Newcastle–Ottawa Scale (NOS) and discussed them in cases of disagreement. The NOS consists of three parts: study population selection (four items), intergroup comparability (one item), and measurement of exposure factors (three items). The full score was 9, and a score ≥ 6 was considered a high-quality study suitable for meta-analysis [28].
Statistical analysis
All statistical analyses were performed using Stata 15.0 software, and the following five gene models were compared: (1) dominant (CC + GC vs. GG; CC + TC vs. TT; AA + GA vs. GG), (2) recessive (CC vs. GC + GG; CC vs. TC + TT; AA vs. GA + GG), (3) allelic (C vs. G; C vs. T; A vs. G), (4) homozygous (CC vs. GG; CC vs. TT; AA vs. GG), and (5) heterozygous (GC vs. GG; TC vs. TT; GA vs. GG). The correlations between ADAM12 polymorphisms at the rs3740199, rs1871054, rs1044122, and rs1278279 sites (C/G, C/T, A/G, and C/T) and OA were evaluated by summarizing the OR value and 95% CI. The χ2 test was used to confirm whether the genotype frequencies of the included studies were consistent with HWE. Simultaneously, a subgroup analysis based on various regions was conducted to observe the influence of different regions of the results. Moreover, subgroup analysis was conducted to observe the effect of sex on the results. The Q test was used to determine statistical heterogeneity among studies [29]. When there was significant heterogeneity between studies (I2 > 50%), a random-effects model was used for data calculation [30]; when I2 < 50%, a fixed-effects model was used [31]. I2 < 25% indicated low heterogeneity; I2 value between 25 and 75% indicates moderate heterogeneity; I2 > 75% indicated high heterogeneity; if significant heterogeneity was found, sensitivity analysis was performed to explore its possible sources. Egger’s and Begg’s tests were used to detect publication bias. P > 0.05, indicating no obvious publication bias.
False-positive report probability (FPRP) analysis
In this study, positive results from meta-analysis were further applied to FPRPS, which could help us explore the probability of a meaningful association between SNPS and disease [32, 33]. The FPRP threshold was set at 0.2, the prior probabilities were set at 0.25, 0.1, 0.01, 0.001 and 0.0001, and the correlation strength index OR = 1.5.
Results
Literature retrieval results
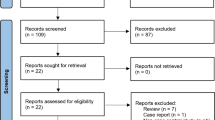
The databases were searched using a retrieval strategy. By reading the title and abstract, studies that may be consistent were preliminarily screened. We retrieved 27 studies were retrieved from the Web of Science database, 20 from PubMed, 20 from Springer, and 18 from Embase. Endnote software was used to remove 66 duplicate studies, and 9 reviews, non-case control studies, studies lacking genotypes [34,35,36], and those with incomplete data were removed from the remaining 19 studies, and the remaining 11 studies were suitable for the meta-analysis [5, 24,25,26, 37,38,39,40,41,42]. In the Literature screening, there was no disagreement among independent researchers about the included studies. A flowchart is shown in Fig. 1. A total of 8440 patients were included in the 11 studies, including 3332 patients with OA in the case group and 5108 patients without OA in the control group. The included studies were consistent with the H–W inheritance law.

Flow diagram of the literature search
Among the included studies, eight articles investigated the association between the rs3740199 polymorphism and OA in 1686 and 2845 patients in the case and control groups, respectively. Seven articles investigated the association between the rs1871054 polymorphism and OA in 1204 and 1425 patients in the case and control groups, respectively. The association between the rs1278279 polymorphism and OA was studied in 316 and 379 patients in the case and control groups from two articles. Finally, four studies investigated the relationship between the rs1044122 polymorphism and OA in 904 and 988 patients in the case and control groups, respectively. Four studies were conducted on European population [5, 26, 37, 41], among which Rodriguez-Lopez et al. [40] included three centers in Spain, Britain, and France, so it was considered an independent study. Five studies were conducted on Asian population [24, 25, 38, 39, 41]. Kerna et al. [26, 37] included tibial and patellar OA in their 2009 and 2013 studies; therefore, they were analyzed as two studies. One study focused on a North American population [42]; therefore, a subgroup analysis was not conducted. In addition, gender analysis was performed in four studies [24, 26, 37, 38] and not in the rest. The basic characteristics and distribution of the alleles and genotypes of the included studies are shown in Tables 1 and 2. All included studies were of high quality, with NOS scores ≥ 6, as shown in Table 1.
Meta-analysis results
Heterogeneity and publication bias
Heterogeneity was analyzed for all genotypes, and it was found that there was no significant heterogeneity in any of the rs3740199 and rs1278279 polymorphisms of ADAM12. A fixed-effects model was used for data calculation. However, there was significant heterogeneity in the polymorphism studies of rs1871054 (CC + TC vs. TT, C vs. T, CC vs. TT) and rs1044122 (all gene models), so a random-effects model was used for data calculation. At the same time, sensitivity analysis was conducted to observe the impact of each study on the overall results by ignoring one study at a time and verifying the stability of the pooled results. The results showed that the I2 value changed from > 50 to < 50% when the research results of Fatima et al. [24] were ignored in rs1044122, so the source of heterogeneity was the research of Fatima et al. [24]. Sensitivity analysis of rs1871054 for ADAM12 did not identify the source of heterogeneity. Through careful reading by Fatima et al. [24], it was found that the inclusion of the case group and the control group met the inclusion criteria, and the ADAM12 gene was also determined by arms-PCR technology. No obvious abnormality was found in the experimental method, and the distribution of genotype data met Hardy Weinberg equilibrium law. However, this study is the only one on Pakistanis. Mukhtar et al. [43] mentioned that 70% of marriages in Pakistan are sincere marriages, which is the main reason for the inheritance of genetic diseases to the next generation, so this may be the source of the existence of heterogeneity. Egger’s and Begg’s tests were carried out for all genotypes, and no obvious publication bias was found, indicating that the results were relatively stable. The P values of the publication bias test for the included polymorphisms of each genotype are shown in Table 3.
Correlation between ADAM12 polymorphism rs3740199 and osteoarthritis
A total of eight included studies focused on the correlation between the ADAM12 rs3740199 polymorphism and OA [5, 25, 37,38,39,40,41,42], among which Rodriguez-Lopez et al. [40] included three centers in Spain, Britain, and France; therefore, the analysis was carried out across three cohorts, but the data in this study were incomplete. Kerna et al. [37] included tibial and patellar OA in their study; therefore, we treated them as two studies for our analysis. A total of 2467 and 4030 cases in the case and control groups were analyzed. The meta-analysis results showed that all gene models of the ADAM12 rs1044122 polymorphism had no significant correlation with susceptibility to OA, and the comparative heterogeneity of all gene models was small [allelic model (C vs. G), OR = 0.98, 95% CI (0.91–1.05), P = 0.174, I2 = 28.4%], as shown in Fig. 2A. Publication bias was detected using the Begg’s test (P = 0.876) and Egger’s test (P = 0.841), and the results showed that the analysis results were fairly robust without obvious bias. No statistical significance was found in the other gene models (CC + GC vs. GG, CC vs. GC + GG, CC vs. GG, GC vs. GG).


A–D show the forest maps of correlations between ADAM12 rs3740199, rs1871054, rs1278279 and rs1044122 polymorphisms and osteoarthritis
According to regional subgroup analysis, there were four studies on Asians and six studies on Europeans, but only one study on North Americans, so subgroup analysis was not carried out on the North American population. The results showed that there were no significant differences in the alleles of ADAM12 rs3740199 and OA susceptibility between Europeans and Asians. In addition, in the subgroup analysis based on sex, six studies were not statistically analyzed according to sex; therefore, only three studies were subjected to sex subgroup analysis, and the results were only meaningful in the female-dominant model [OR = 1.38, 95% CI (1.02–1.86), P = 0.209, I2 = 36.1%]. This does not seem to indicate that female patients are more susceptible to the disease. Subgroup analysis with an average age of 60 years indicated that the rs3740199 polymorphism of ADAM12 and susceptibility to OA may not be significantly associated with age, as shown in Table 3.
Correlation between ADAM12 polymorphism rs1871054 and osteoarthritis
The association between the rs1871054 polymorphism of ADAM12 and OA was analyzed in seven studies [5, 24,25,26, 37, 39, 42], which included 1204 and 1425 patients in the case and control groups, respectively. Kerna et al. [26, 37] included tibial and patellar OA in their study; therefore, the analysis was performed according to two studies. We found no statistically significant differences between ADAM12 Rs1871054 polymorphism and susceptibility to osteoarthritis in the dominant, recessive, allele, and homozygous models [allelic model (T vs. C), OR = 1.34, 95% CI (1.05–1.71), P < 0.001, I2 = 76.4%], as shown in Fig. 2B. However, there was no statistical significance in the heterozygous model [OR = 1.07, 95% CI (0.88–1.30), P = 0.907, I2 = 0%], suggesting patients carrying the TC allele and those with TT had the same risk of disease. In summary, patients with the C allele may be more susceptible, which is consistent with the Kerna result [26]. Due to the large heterogeneity, no source of heterogeneity was found after the sensitivity analysis (Fig. 3D). In the allele model, Begg’s test (P = 0.917) (Fig. 3F), and Egger’s test (P = 0.610) were used to detect publication bias; the results showed that the analysis was fairly robust, without obvious bias.


A Forest map analysis of different regional subgroups related to ADAM12 rs1871054 (C vs. T) polymorphism and osteoarthritis. B Forest map analysis of different sex subgroups related to ADAM12 rs1871054 (C vs. T) polymorphism and osteoarthritis. C Forest map analysis of different age subgroups related to ADAM12 rs1871054 (C vs. T) polymorphism and osteoarthritis. D Sensitivity analysis of ADAM12 rs1871054 (C vs. T) polymorphism and osteoarthritis. E Sensitivity analysis of ADAM12 rs1044122 (C vs. T) polymorphism and osteoarthritis. F Begg’s test for publication bias
Subgroup analysis showed that there was a significant difference between ADAM12 rs1871054 and osteoarthritis susceptibility in Asian samples of dominant, recessive, allelic, and homozygous models [e.g., allelic model (T vs. C), OR = 1.61, 95% CI (1.25–2.08), P = 0.055, I2 = 65.6%] (Fig. 3A); however, only three studies were included. There was no significant difference between ADAM12 rs1871054 in Europeans and the allele conferring susceptibility to osteoarthritis in all gene models [allelic model (T vs. C), OR = 1.33, 95% CI (0.91–1.95), P = 0.019, I2 = 66.0%], suggesting that Asian patients carrying the C allele are more prone to the disease. In addition, in the subgroup analysis based on sex, four studies were not statistically analyzed based on sex, so only three studies were analyzed based on sex subgroups. Kerna et al. [26] only provided data on male patients in their 2013 study. The results showed that ADAM12 gene polymorphism was significant in male recessive models [OR = 1.38, 95% CI (1.02–1.86), P = 0.209, I2 = 36.1%] (Fig. 3B) and in female dominant and recessive models [e.g., dominant model (CC + GG vs. GG), OR = 1.38, 95% CI (1.02–1.86), P = 0.209, I2 = 36.1%]. However, it is uncertain whether ADAM12 polymorphism is associated with OA susceptibility in either male or female patients. Subgroup analysis with a mean age of 60 years showed similar results to subgroup analysis by region, in which the C allele may be associated with disease susceptibility in patients younger than 60 years (Fig. 3C), as presented in Table 3.
Association between ADAM12 polymorphism rs1278279 and osteoarthritis
Two studies on the correlation between the ADAM12 polymorphism rs1278279 and OA were conducted on 316 and 379 patients in the case and control groups, respectively [25, 39], and the results showed that there was no significant difference between the rs1278279 alleles of ADAM12 and OA susceptibility [e.g., allelic model (A vs. G), OR = 1.02, 95% CI (0.80–1.30), P = 0.926, I2 = 0%] (Fig. 3C). As there were only two studies, no subgroup analysis was performed, as shown in Table 3.
Correlation between ADAM12 polymorphism rs1044122 and osteoarthritis
The correlation between the ADAM12 rs1044122 polymorphism and OA was assessed in four studies, which included 904 and 988 patients in the case and control groups, respectively [24,25,26, 39]. The meta-analysis results showed that the rs1044122 polymorphism was not significantly correlated with susceptibility to OA, and the comparative heterogeneity of all gene models was large [e.g., allelic model (C vs. T), OR = 1.20, 95% CI (0.81–1.79), P < 0.001, I2 = 88.1%] (Fig. 2D). The sensitivity analysis showed that the source of heterogeneity was the study of Fatima et al. [24] (Fig. 3E). Begg’s (P = 1.000) and Egger’s tests (P = 0.520) were used to detect publication bias, and the results showed that the analysis was fairly robust without obvious bias. Since all four articles were conducted on Asian populations, subgroup analysis was not performed. In addition, in the subgroup analysis based on sex, only two studies analyzed by sex. The results showed no significant correlation between ADAM12 rs1044122 and OA susceptibility in male and female patients. Subgroup analysis with an average age of 60 years indicated that the rs1044122 polymorphism and susceptibility to OA may not be significantly related to age, as shown in Table 3.
FPRP results
We calculated the value of FPRP under a series of prior probability conditions to determine whether there is a real association between ADAM12 polymorphism and OA. The FPRP results show (Table 4) that when the prior probability is 0.25. The FPRP values of all four genetic models of rs1871054 were less than 0.2. Similarly, with a prior probability of 0.1, the FPRP values of the four genetic models of Asian rs1871054 were all less than 0.2. However, when the prior probability is 0.25, only two genetic models with FPRP values of rs1871054 locus for people younger than 60 years old are less than 0.2. This suggests that ADAM12 rs1871054 polymorphism may have a real association with OA susceptibility, and this association is more real in Asian population, which is worthy of further study. However, in those less than 60 years of age, there is a possibility of false positives between Rs1871054 polymorphism and OA susceptibility.
Discussion
The genetic factors of OA are mediated by both gene and/or protein expression networks. Among them, coding RNAs and non-coding RNAs have been confirmed to participate in and affect the development of OA [44,45,46], such as mRNAs, microRNAs, long non-coding RNAs, etc. Several transcription and growth factors (including SOX family members SOX9, L-SOX5, and SOX6) [47], bone morphogenetic proteins, and transforming growth factor β are involved in the modulation of chondrogenesis [48]. There are also epigenetic mechanisms, including DNA methylation and histone modification, that add additional levels of regulation to the evolution of OA [49]. In the mRNA, ADAM12 is a Zn2+-dependent metalloproteinase that may be involved in various cell interactions and biological processes that regulate cell responses [50]. The importance of the ADAM12 gene in OA has been confirmed by many studies, and its expression is increased to varying degrees [51, 52]. It promotes cell proliferation, differentiation, and migration through outdomain shedding of mesangial epidermal growth factor receptor ligands [53]. Studies have shown that both mRNA and protein levels of ADAM12 are increased in the synovial tissues of OA-associated synovitis [54]. To explore the gene polymorphisms related to the susceptibility of knee arthritis, we can identify susceptible populations by their genetic phenotype [55] to enable targeted prevention and treatment. However, existing reports are inconclusive. rs3740199 is associated with the risk of OA in a recessive model, but not with rs1871054 [42]. Kerna believed that rs3740199 CC is homozygous for the development of patellofemoral OA [37]. However, Shin et al. found no association between rs3740199 and knee OA. Another study found that rs1871054 and rs1044122 were significantly correlated with knee arthritis, especially in female patients, and those with haplotype CC were more prone to bilateral knee arthritis [24]. Valdes and Kerna reported that the rs1871054 polymorphism was not significantly associated with knee arthritis [35, 37], but four studies reported that rs1871054 was associated with knee arthritis [24,25,26, 39].
Based on these different conclusions, five studies analyzed the correlation between ADAM12 polymorphisms and OA. Hu et al. [56] included 10 studies that suggested that rs1871054 is associated with knee arthritis risk. However, there was no significant correlation between rs3740199 and rs1278279, and there were no relevant data in the included studies. Jung et al. [57] included six studies and reported that the risk of knee OA was correlated with rs3740199 and rs1871054. Wu et al. [27] included eight studies and concluded that ADAM12 rs3740199 polymorphism is related to susceptibility in male patients. Khan et al. [58] included 11 studies, 3 of which had no clinical data, and concluded that the risk of knee arthritis was correlated with rs3740199 and rs1871054, but not with rs1044122 and rs1278279. Lv et al. [21] included seven studies, and their conclusion was similar to that of Hu et al.; namely, that the genetic effect of the rs1871054 polymorphism was stronger in Asian populations than that in European populations. The results of these meta-analyses differ greatly. In recent years, several studies have explored the relationship between these two.
This meta-analysis aimed to explore the relationship between ADAM12 polymorphisms and the risk of OA. To date, four important polymorphisms of ADAM12 (rs3740199, rs1871054, rs1278279, and rs1044122) have been associated with OA. The study included 3332 patients with OA in the case group and 5108 patients without OA in the control group. The results show that in dominant, recessive, allelic, and homozygous models, rs1871054 polymorphism was associated with OA. In the subgroup analysis, we found that rs1871054 was associated with OA in Asian populations, but there was no statistical significance in European populations. In addition, people younger than 60 years who carry the C allele may be highly susceptible to the disease, and this conclusion may be a false positive. These differences may be the result of the gene-environment or gene–gene interactions, but the number of studies included is limited. However, the polymorphisms rs3740199, rs1044122, and rs1278279 in ADAM12 were not significantly correlated with OA, and the results showed no significant correlation after excluding heterogeneity.
In conclusion, ADAM12 rs1871054 may be a predictor of OA, and individuals carrying the C allele may be highly susceptible to this disease; in addition, the Asian population may also show high susceptibility. Furthermore, rs3740199, rs1044122, and rs1278279 may not be predictors of OA. Although some studies have been published on the rs3740199, rs1871054, rs1044122, and rs1278279 polymorphisms of the ADAM12 gene and susceptibility to OA, the conclusions are not uniform and lack the support of sufficient homogeneity and large samples in research. If consistent conclusions can be drawn, it will be of great significance for the detection and treatment of OA. Heterogeneity may also be increased due to the different genotyping methods of the included studies. Age and sex differences in region, population, and included population are also important factors affecting the results. Due to the small number of included articles, it is impossible to analyze various interfering factors, and there is certain heterogeneity; therefore, the results need to be carefully interpreted. Whether ADAM12 polymorphisms are related to susceptibility to OA needs to be supported by higher quality case–control studies with larger samples to provide more effective evidence for the pathogenesis and treatment of OA.
Availability of data and materials
For further enquiries about the relevant original materials of this article, please consult the corresponding author.
Change history
25 March 2023
A Correction to this paper has been published: https://doi.org/10.1186/s13018-023-03685-w
References
Kraus VB, Blanco FJ, Englund M, Karsdal MA, Lohmander LS. Call for standardized definitions of osteoarthritis and risk stratification for clinical trials and clinical use. Osteoarthr Cartil. 2015;23:1233–41. https://doi.org/10.1016/j.joca.2015.03.036.
Cross M, Smith E, Hoy D, Nolte S, Ackerman I, Fransen M, Bridgett L, Williams S, Guillemin F, Hill CL, et al. The global burden of hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73:1323–30. https://doi.org/10.1136/annrheumdis-2013-204763.
O’Neill TW, McCabe PS, McBeth J. Update on the epidemiology, risk factors and disease outcomes of osteoarthritis. Best Pract Res Clin Rheumatol. 2018;32:312–26. https://doi.org/10.1016/j.berh.2018.10.007.
Bortoluzzi A, Furini F, Scirè CA. Osteoarthritis and its management—epidemiology, nutritional aspects and environmental factors. Autoimmun Rev. 2018;17:1097–104. https://doi.org/10.1016/j.autrev.2018.06.002.
Haberal B, Şimşek EK, Baysan Çebi HP, Tuç Ö, Verdi H, Ataç FB. Lack of association between MMP13 (Rs3819089), ADAM12 (Rs3740199-Rs1871054) and ADAMTS14 (Rs4747096) genotypes and advanced-stage knee osteoarthritis. Jt Dis Relat Surg. 2021;32:299–305. https://doi.org/10.52312/jdrs.2021.64.
González-Huerta NC, Borgonio-Cuadra VM, Morales-Hernández E, Duarte-Salazar C, Miranda-Duarte A. Vitamin D receptor gene polymorphisms and susceptibility for primary osteoarthritis of the knee in a Latin American population. Adv Rheumatol. 2018;58:6. https://doi.org/10.1186/s42358-018-0002-3.
Dai X, Ying P, Ding W, Li H, Xu P, Huang Z, Zhang N, Liu J. Genetic estrogen receptor alpha gene PvuII polymorphism in susceptibility to knee osteoarthritis in a Chinese Han population: a southern Jiangsu study. Knee. 2020;27:803–8. https://doi.org/10.1016/j.knee.2020.02.010.
Zhang PL, Yang FM, Qiao ZZ, Liu J, Yang QY, Wang YJ, Qi M, Cui LN, Meng L, Li XP. Association between interleukin-17A and 17F single nucleotide polymorphisms and knee osteoarthritis. Zhonghua Yi Xue Za Zhi. 2019;99:1870–4. https://doi.org/10.3760/cma.j.issn.0376-2491.2019.24.007.
Harati-Sadegh M, Sargazi S, Sheervalilou R, Hosseini Teshnizi S, Saravani R, Mirinejad S. Association of IL-1Ra Ser133Ser variant with susceptibility to immune-mediated and inflammatory diseases: a meta-analysis of 2622 cases and 3854 controls. Iran J Public Health. 2020;49:2320–9. https://doi.org/10.18502/ijph.v49i12.4814.
Harati-Sadegh M, Sargazi S, Sheervalilou R, Hosseini Teshnizi S, Saravani R, Mirinejad S. Single nucleotide polymorphisms located in TNFA, IL1RN, IL6R, and IL6 genes are associated w. IJPH. 2020. https://doi.org/10.18502/ijph.v49i12.4814.
Barani M, Rahdar A, Sargazi S, Amiri MS, Sharma PK, Bhalla N. Nanotechnology for inflammatory bowel disease management: detection, imaging and treatment. Sens Bio Sens Res. 2021;32:100417. https://doi.org/10.1016/j.sbsr.2021.100417.
Sargazi S, Arshad R, Ghamari R, Rahdar A, Bakhshi A, Karkan SF, Ajalli N, Bilal M, Díez-Pascual AM. SiRNA-based nanotherapeutics as emerging modalities for immune-mediated diseases: a preliminary review. Cell Biol Int. 2022;46:1320–44. https://doi.org/10.1002/cbin.11841.
Sargazi S, Sheervalilou R, Rokni M, Shirvaliloo M, Shahraki O, Rezaei N. The role of autophagy in controlling SARS-CoV-2 infection: an overview on virophagy-mediated molecular drug targets. Cell Biol Int. 2021;45:1599–612. https://doi.org/10.1002/cbin.11609.
Giebeler N, Zigrino P. A disintegrin and metalloprotease (ADAM): historical overview of their functions. Toxins (Basel). 2016;8:122. https://doi.org/10.3390/toxins8040122.
Verrier S, Hogan A, McKie N, Horton M. ADAM gene expression and regulation during human osteoclast formation. Bone. 2004;35:34–46. https://doi.org/10.1016/j.bone.2003.12.029.
Okada A, Mochizuki S, Yatabe T, Kimura T, Shiomi T, Fujita Y, Matsumoto H, Sehara-Fujisawa A, Iwamoto Y, Okada Y. ADAM-12 (meltrin alpha) is involved in chondrocyte proliferation via cleavage of insulin-like growth factor binding protein 5 in osteoarthritic cartilage. Arthritis Rheum. 2008;58:778–89. https://doi.org/10.1002/art.23262.
Guo F, Lai Y, Tian Q, Lin EA, Kong L, Liu C. Granulin–Epithelin precursor binds directly to ADAMTS-7 and ADAMTS-12 and inhibits their degradation of cartilage oligomeric matrix protein. Arthritis Rheum. 2010;62:2023–36. https://doi.org/10.1002/art.27491.
Liu C, Kong W, Xu K, Luan Y, Ilalov K, Sehgal B, Yu S, Howell RD, Di Cesare PE. ADAMTS-12 associates with and degrades cartilage oligomeric matrix protein. J Biol Chem. 2006;281:15800–8. https://doi.org/10.1074/jbc.M513433200.
Luan Y, Kong L, Howell DR, Ilalov K, Fajardo M, Bai X-H, Di Cesare PE, Goldring MB, Abramson SB, Liu C-J. Inhibition of ADAMTS-7 and ADAMTS-12 degradation of cartilage oligomeric matrix protein by alpha-2-macroglobulin. Osteoarthr Cartil. 2008;16:1413–20. https://doi.org/10.1016/j.joca.2008.03.017.
Kveiborg M, Albrechtsen R, Rudkjaer L, Wen G, Damgaard-Pedersen K, Wewer UM. ADAM12-S stimulates bone growth in transgenic mice by modulating chondrocyte proliferation and maturation. J Bone Miner Res. 2006;21:1288–96. https://doi.org/10.1359/jbmr.060502.
Lv Z-T, Liang S, Huang X-J, Cheng P, Zhu W-T, Chen A-M. Association between ADAM12 single-nucleotide polymorphisms and knee osteoarthritis: a meta-analysis. Biomed Res Int. 2017;2017:5398181. https://doi.org/10.1155/2017/5398181.
King JD, Rowland G, Villasante Tezanos AG, Warwick J, Kraus VB, Lattermann C, Jacobs CA. Joint fluid proteome after anterior cruciate ligament rupture reflects an acute posttraumatic inflammatory and chondrodegenerative state. Cartilage. 2020;11:329–37. https://doi.org/10.1177/1947603518790009.
Hao Z, Li X, Dai J, Zhao B, Jiang Q. Genetic effects of Rs3740199 polymorphism in ADAM12 gene on knee osteoarthritis: a meta-analysis. J Orthop Surg Res. 2017;12:94. https://doi.org/10.1186/s13018-017-0594-z.
Fatima S, Khan B, Khan OY, Amjad M, Zehra S, Azhar A. Tetra-primers ARMS-PCR based association analyses of synonymous and intronic variants in the ADAM12 gene with susceptibility to knee osteoarthritis: a case-control study. Biochem Genet. 2022. https://doi.org/10.1007/s10528-022-10189-5.
Wang L, Guo L, Tian F, Hao R, Yang T. Analysis of single nucleotide polymorphisms within ADAM12 and risk of knee osteoarthritis in a Chinese Han population. Biomed Res Int. 2015;2015:518643. https://doi.org/10.1155/2015/518643.
Kerna I, Kisand K, Tamm AE, Kumm J, Tamm AO. Two single-nucleotide polymorphisms in ADAM12 gene are associated with early and late radiographic knee osteoarthritis in Estonian population. Arthritis. 2013;2013:878126. https://doi.org/10.1155/2013/878126.
Wu Z, Xu X-W, Zhang X-W. The association of ADAM12 polymorphism with osteoarthritis susceptibility: a meta-analysis. Ther Clin Risk Manag. 2017;13:821–30. https://doi.org/10.2147/TCRM.S134581.
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25:603–5. https://doi.org/10.1007/s10654-010-9491-z.
Lau J, Ioannidis JP, Schmid CH. Quantitative synthesis in systematic reviews. Ann Intern Med. 1997;127:820–6. https://doi.org/10.7326/0003-4819-127-9-199711010-00008.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–88. https://doi.org/10.1016/0197-2456(86)90046-2.
Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst. 1959;22:719–48.
Wacholder S, Chanock S, Garcia-Closas M, El Ghormli L, Rothman N. Assessing the probability that a positive report is false: an approach for molecular epidemiology studies. J Natl Cancer Inst. 2004;96:434–42. https://doi.org/10.1093/jnci/djh075.
Harati-Sadegh M, Sargazi S, Khorasani M, Ansari-Moghaddam A, Mirinejad S, Sheervalilou R, Saravani R. IL1A and IL1B gene polymorphisms and keratoconus susceptibility: evidence from an updated meta-analysis. Ophthalmic Genet. 2021;42:503–13. https://doi.org/10.1080/13816810.2021.1925926.
Valdes AM, Hart DJ, Jones KA, Surdulescu G, Swarbrick P, Doyle DV, Schafer AJ, Spector TD. Association study of candidate genes for the prevalence and progression of knee osteoarthritis. Arthritis Rheum. 2004;50:2497–507. https://doi.org/10.1002/art.20443.
Valdes AM, Van Oene M, Hart DJ, Surdulescu GL, Loughlin J, Doherty M, Spector TD. Reproducible genetic associations between candidate genes and clinical knee osteoarthritis in men and women. Arthritis Rheum. 2006;54:533–9. https://doi.org/10.1002/art.21621.
Limer KL, Tosh K, Bujac SR, McConnell R, Doherty S, Nyberg F, Zhang W, Doherty M, Muir KR, Maciewicz RA. Attempt to replicate published genetic associations in a large, well-defined osteoarthritis case-control population (the GOAL study). Osteoarthr Cartil. 2009;17:782–9. https://doi.org/10.1016/j.joca.2008.09.019.
Kerna I, Kisand K, Tamm AE, Lintrop M, Veske K, Tamm AO. Missense single nucleotide polymorphism of the ADAM12 gene is associated with radiographic knee osteoarthritis in middle-aged Estonian cohort. Osteoarthr Cartil. 2009;17:1093–8. https://doi.org/10.1016/j.joca.2009.02.006.
Shin M-H, Lee S-J, Kee S-J, Song S-K, Kweon S-S, Park D-J, Park Y-W, Lee S-S, Kim T-J. Genetic association analysis of GDF5 and ADAM12 for knee osteoarthritis. Jt Bone Spine. 2012;79:488–91. https://doi.org/10.1016/j.jbspin.2011.10.016.
Lou S, Zhao Z, Qian J, Zhao K, Wang R. Association of single nucleotide polymorphisms in ADAM12 gene with susceptibility to knee osteoarthritis: a case-control study in a Chinese Han population. Int J Clin Exp Pathol. 2014;7:5154–9.
Rodriguez-Lopez J, Pombo-Suarez M, Loughlin J, Tsezou A, Blanco FJ, Meulenbelt I, Slagboom PE, Valdes AM, Spector TD, Gomez-Reino JJ, et al. Association of a NsSNP in ADAMTS14 to some osteoarthritis phenotypes. Osteoarthr Cartil. 2009;17:321–7. https://doi.org/10.1016/j.joca.2008.07.012.
Poonpet T, Tammachote R, Tammachote N, Kanitnate S, Honsawek S. Association between ADAM12 polymorphism and knee osteoarthritis in Thai population. Knee. 2016;23:357–61. https://doi.org/10.1016/j.knee.2016.01.007.
Aguilar Muñiz LS, González Galarza FF, Arguello Astorga R, Prieto Hinojosa AI, Hernández Terán F, Méndez Hernández A, Espino Silva PK, Blanco García FJ, Arellano Pérez Vertti RD. Analyses of the genetic polymorphisms Rs3740199 and Rs1871054 of the ADAM12 gene and the alleles at the Rs2073508 loci of the TGFB1 gene and their contribution to susceptibility to primary knee osteoarthritis. Genet Test Mol Biomarkers. 2020;24:375–80. https://doi.org/10.1089/gtmb.2019.0266.
Mukhtar M, Sheikh N, Suqaina SK, Batool A, Fatima N, Mehmood R, Nazir S. Vitamin D receptor gene polymorphism: an important predictor of arthritis development. Biomed Res Int. 2019;2019:8326246. https://doi.org/10.1155/2019/8326246.
Dai M, Sui B, Xue Y, Liu X, Sun J. Cartilage repair in degenerative osteoarthritis mediated by squid type II collagen via immunomodulating activation of M2 macrophages, inhibiting apoptosis and hypertrophy of chondrocytes. Biomaterials. 2018;180:91–103. https://doi.org/10.1016/j.biomaterials.2018.07.011.
Oliviero A, Della Porta G, Peretti GM, Maffulli N. MicroRNA in osteoarthritis: physiopathology, diagnosis and therapeutic challenge. Br Med Bull. 2019;130:137–47. https://doi.org/10.1093/bmb/ldz015.
Huynh NP, Gloss CC, Lorentz J, Tang R, Brunger JM, McAlinden A, Zhang B, Guilak F. Long non-coding RNA GRASLND enhances chondrogenesis via suppression of the interferon type II signaling pathway. Elife. 2020;9:e49558. https://doi.org/10.7554/eLife.49558.
Ikeda T, Kamekura S, Mabuchi A, Kou I, Seki S, Takato T, Nakamura K, Kawaguchi H, Ikegawa S, Chung U. The combination of SOX5, SOX6, and SOX9 (the SOX Trio) provides signals sufficient for induction of permanent cartilage. Arthritis Rheum. 2004;50:3561–73. https://doi.org/10.1002/art.20611.
Goldring MB, Tsuchimochi K, Ijiri K. The control of chondrogenesis. J Cell Biochem. 2006;97:33–44. https://doi.org/10.1002/jcb.20652.
Barter MJ, Bui C, Young DA. Epigenetic mechanisms in cartilage and osteoarthritis: DNA methylation, histone modifications and MicroRNAs. Osteoarthr Cartil. 2012;20:339–49. https://doi.org/10.1016/j.joca.2011.12.012.
Gilpin BJ, Loechel F, Mattei MG, Engvall E, Albrechtsen R, Wewer UM. A novel, secreted form of human ADAM 12 (Meltrin Alpha) provokes myogenesis in vivo. J Biol Chem. 1998;273:157–66. https://doi.org/10.1074/jbc.273.1.157.
Sato T, Konomi K, Yamasaki S, Aratani S, Tsuchimochi K, Yokouchi M, Masuko-Hongo K, Yagishita N, Nakamura H, Komiya S, et al. Comparative analysis of gene expression profiles in intact and damaged regions of human osteoarthritic cartilage. Arthritis Rheum. 2006;54:808–17. https://doi.org/10.1002/art.21638.
Iba K, Albrechtsen R, Gilpin BJ, Loechel F, Wewer UM. Cysteine-rich domain of human ADAM 12 (Meltrin Alpha) supports tumor cell adhesion. Am J Pathol. 1999;154:1489–501. https://doi.org/10.1016/s0002-9440(10)65403-x.
Kveiborg M, Albrechtsen R, Couchman JR, Wewer UM. Cellular roles of ADAM12 in health and disease. Int J Biochem Cell Biol. 2008;40:1685–702. https://doi.org/10.1016/j.biocel.2008.01.025.
Kerna I, Kisand K, Suutre S, Murde M, Tamm A, Kumm J, Tamm A. The ADAM12 is upregulated in synovitis and postinflammatory fibrosis of the synovial membrane in patients with early radiographic osteoarthritis. Jt Bone Spine. 2014;81:51–6. https://doi.org/10.1016/j.jbspin.2013.03.007.
Takahashi H, Nakajima M, Ozaki K, Tanaka T, Kamatani N, Ikegawa S. Prediction model for knee osteoarthritis based on genetic and clinical information. Arthritis Res Ther. 2010;12:R187. https://doi.org/10.1186/ar3157.
Hu X, Sun G, Wang W. Association of ADAM 12 polymorphisms with the risk of knee osteoarthritis: meta-analysis of 5048 cases and 6848 controls. Rheumatol Int. 2017;37:1659–66. https://doi.org/10.1007/s00296-017-3778-2.
Jung JH, Song GG, Kim J-H, Choi SJ. Association of single nucleotide polymorphisms in a disintegrin and metalloproteinase 12 gene with susceptibility to knee osteoarthritis: a meta-analysis. Arch Rheumatol. 2019;34:62–70. https://doi.org/10.5606/ArchRheumatol.2019.6726.
Khan B, Aman S. Association between the genetic variations in Adam12 and the susceptibility to knee osteoarthritis: an updated meta analysis. Int J Biol Biotech. 2021;18:17–27.
Acknowledgements
We thank all the original study authors included in the meta-analysis. We are grateful to Peng-fei Han and Peng-yong Han for their guidance. In addition, thanks to Mr. David Yadeedya for revising this article.
Funding
Grants from Chang Zhi Medical College's 2020 Doctoral Starting Fund (No. BS2020004).
Author information
Authors and Affiliations
Contributions
The article is designed by SY and YW, the data collection is SY and XL, the literature quality control is PH and PH, SY wrote and was responsible for the article. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
All the authors of the article declare that there is no competing interests in the subject research and article writing process.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: The authors affiliations have been revised.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yang, S., Wang, Yp., Li, Xy. et al. The association between ADAM12 gene polymorphisms and osteoarthritis: an updated meta-analysis. J Orthop Surg Res 18, 149 (2023). https://doi.org/10.1186/s13018-023-03626-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-023-03626-7