
Abstract
Background
Percutaneous vertebroplasty is the most common treatment for osteoporotic vertebral compression fracture. However, the morbidity of vertebroplasty-related complications, such as cement leakage, remains high. We tested a new technique of unilateral pulsed jet lavage and investigated its effect on the intravertebral pressure and bone cement distribution.
Methods
Thirty lumbar vertebrae (L1-L5) from six cadaver spines were randomly allocated into two groups (with and without irrigation). Prior to vertebroplasty, pulsed jet lavage was performed through one side of the pedicle by using a novel cannula with two concentric conduits to remove the fat and bone marrow of the vertebral bodies in the group with irrigation. The control group was not irrigated. Then, standardized vertebroplasty was performed in the vertebral bodies in both groups. Changes in the intravertebral pressure during injection were recorded. Computed tomography (CT) was performed to observe the cement distribution and extravasations, and the cement mass volume (CMV) was calculated.
Results
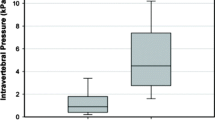
During cement injection, the average maximum intravertebral pressure of the unirrigated group was higher than that of the irrigated group (4.92 kPa versus 2.22 kPa, P < 0.05). CT scans showed a more homogeneous cement distribution with less CMV (3832 mm3 vs. 4344 mm3, P < 0.05) and less leakage rate (6.7% vs. 46.7%, P < 0.05) in the irrigated group than in the control group.
Conclusions
Unilateral pulsed jet lavage can reduce intravertebral pressure and lower the incidence of cement leakage during vertebroplasty. An enhanced bone cement distribution can also be achieved through this lavage system.
Similar content being viewed by others
Background
Percutaneous vertebroplasty (PVP) or percutaneous kyphoplasty (PKP) is effective in the treatment of osteoporotic vertebral compression fractures. These techniques can provide instant pain relief [1,2,3] and stabilize vertebral fracture [3,4,5]. However, leakage during PVP or PKP remains a concern among surgeons. Some studies have shown that intravertebral lavage prior to cement injection can effectively remove the vertebral fat and bone marrow and reduce the morbidity of extravasation [6, 7]. Previously reported lavage methods involved bilateral operation [8,9,10], but the unilateral pulsed jet lavage method has not been described. Thus, we designed and used a unilateral pulsed jet lavage system to investigate the effect of unilateral irrigation prior to vertebroplasty on leakage, intravertebral pressure, and cement distribution.
Methods
Thirty intact cadaver lumbar vertebrae (L1-L5) were harvested from ten human cadaveric spines without a known history of spinal pathology. The age of donors was 71.5 ± 4.9 years (age range, 63–79 years). The periosteum and adjacent discs of the vertebral bodies were intact. The bone density of the vertebrae was assessed by dual-energy X-ray absorptiometry. These specimens were stored at − 20 °C. Before the experiment was conducted, the specimens were thawed at room temperature overnight.
The vertebrae were allocated randomly into two groups (namely, with and without irrigation) with 15 samples per group. Then, an 11-gauge bone biopsy needle (SterilabHiggins KB S.r.l, Buccinasco, Italy) was inserted through the right pedicle of each vertebra, and an irrigation device was installed via the channel made by the biopsy needle. The irrigation device was a novel cannula with two concentric conduits. The outer conduit was used for the pulsed jet lavage, and the inner conduit was used to regain saline (Fig. 1). Saline (200 mL) was pulsed to each vertebra, and regaining started simultaneously. Saline with the vertebral fat and marrow was sucked out completely from the vertebral bodies through the device. No operation was performed on the control group in this step. Before and after irrigation, a miniature video camera system was installed in the vertebral body to assess the lavage effect. Prior to the cement injection, a digital manometer (GM511, Shenzhen Jumaoyuan Science and Technology Co., Ltd., Shenzhen) was placed just beyond the left pedicle-body junction of each vertebra in both groups to monitor and record the intravertebral pressure during cement injection. A 1.5-mL injection cannula was used to inject radio-opaque polymethylmethacrylate bone cement (Simplex P, Stryker Howmedica Osteonics, Mahwah, NJ, USA) twice into each vertebra at a rate of 3 mL/min in accordance with standard vertebroplasty. The bone cement was mixed in accordance with the manufacturer’s instructions (20 mL of monomer to 40 g of powder). Afterward, 3 mL of bone cement was injected into each vertebral body. Computed tomography (CT) was performed to estimate the distribution of cement in the vertebral body and calculate the CMV. The cement mass edge was drawn in each cross-sectional CT image by using the CT software (Mimics Innovation Suite 21), and the area of the marked region was calculated. Then, CMV was obtained by multiplying the cement area with the height of each cross-section.

The irrigation device. a Full view of the device. b The outer conduit and inner conduit. c The holes on the tip of the outer conduit allowed saline to flow in different directions. d Saline used for lavage flowed through the holes of the outer conduit and went around in the vertebral body. Meanwhile, the inner conduit created negative pressure to regain the saline. Arrows indicated the flow of water
The statistical outcomes of the CMV and intravertebral pressure were presented as mean ± standard deviation. A Mann-Whitney U test was used to analyze the differences in the volume and pressure between the two groups. Fisher’s exact test was conducted to analyze the leakage rate. P ≤ 0.05 was considered statistically significant. Statistical analysis was carried out by using SPSS 26.0.
Results
The main outcome measures are listed in Table 1. There is no significant difference in bone density between the two groups. Some images from a video camera and CT scans are displayed in Figs. 2 and 3.

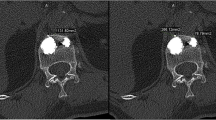
CT scans of vertebrae after vertebroplasty. a CT scans showed that the cement mass in the vertebra with irrigation was homogeneous. b The cement mass was more irregular in the unirrigated specimen than in the irrigated vertebra

The images gained from the video camera. a Before pulsed jet lavage, the vertebral body was filled up with fat and marrow. b After lavage, the intravertebral fat and marrow were removed and the trabecula was recognizable
Leakage rate
Cement leakage was evaluated on the basis of the CT images. Cement leakage occurred in one (6.7%) of the irrigated specimens and in seven (46.7%) of the unirrigated ones (Table 1).
Cement distribution
CT images showed the distinct distributions of cement in the two groups. The bone cement mass was homogeneous and had more uniform density in the irrigated group than in the unirrigated group. The cement distribution of the unirrigated vertebrae was more irregular than that of the irrigated group (Fig. 2).
CMV
The Mann-Whitney U test results revealed smaller CMV in the irrigated group than in the unirrigated group (P < 0.01). The irrigated mass volume was 3832 ± 596 mm3, whereas the unirrigated volume was 4344 ± 653 mm3.
Images from the miniature video camera system
The images from the miniature video camera system showed distinct changes in the trabeculae. Before lavage, the space of the body was filled with fat and marrow. After irrigation, these components were reduced dramatically, and the space was emptied among the trabecula (Fig. 3).
Intravertebral pressure
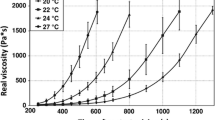
The pressure-time curves in both groups presented two peaks (Fig. 4). A peak indicated the intravertebral pressure produced by 1.5 mL of cement. The maximum pressure of the whole injection process was equal to the top value of the second peak. The average maximum intravertebral pressure in the unirrigated group was almost twice as much as that in the irrigated group. Moreover, the increasing rate of pressure during the first fillings in the unirrigated specimens was more pronounced than that in the irrigated specimens. The half cement volume pressure (the top value of the first peak) of the unirrigated vertebrae was higher than that of the irrigated bodies (P < 0.01). The intravertebral pressure in the first filling was 81% of the maximum pressure in the unirrigated vertebrae, but 64% in the irrigated vertebrae.

The pressure-time curves during cement injection. On the pressure curve, there were two peaks, associated with the injections of cement. Each peak pressure was produced by 1.5-ml cement. The second peak was always higher than the first one
Discussion
The intravertebral pressure and cement distribution in cadaveric vertebroplasty with and without unilateral pulsed jet lavage were recorded and compared. The unilateral lavage method in this study was an original design applied to vertebroplasty. Many reports have shown that lavage technique can remove fat and bone marrow and reduce intravertebral pressure in vertebroplasty compared with those of conventional cement injection [6, 7, 10]. However, these trials were bipedicular, which meant that lavage was performed on one side and suction was conducted from the contralateral side. However, in clinical practice, many surgeons, including our group, still prefer unilateral vertebroplasty because this process has been reported to present short- and long-term clinical outcomes similar to those of the bilateral technique [11, 12]. The unilateral method involves shorter operation time [11, 13] and less X-ray exposure frequency and trauma [14, 15]. To our knowledge, our study was the first to report the application of unilateral lavage in vertebroplasty.
The results showed that unilateral lavage significantly reduced intravertebral pressure and cement leakage. Pulsed saline lavage could remove the fat and marrow, as shown by the intravertebral images from the miniature video camera. After irrigation, the space became clearer, and the trabeculae could be distinguished. Yang et al. [16] also reported the effect of pulsed lavage to remove the bone marrow, and similar positive outcomes were achieved. With less fat and marrow, the space in the trabeculae was expanded and would accommodate more bone cement [17,18,19]. Hence, less pressure would be transmitted and recorded from the contralateral side of the vertebral body. Less bone leakage could also be achieved, and this finding was reported in previous bilateral lavage studies [6, 7].
The results also showed an interesting pattern of the changes in the recorded pressure during vertebroplasty. Two peaks, which corresponded to the two steps of bone cement injection, appeared in the pressure curve. Given the accumulating effect of the bone cement, the second peak did not start from the baseline, and the value was higher than the first peak. This adding-on phenomenon showed that more elaborative inspection should be performed during the latter stage of bone cement injection to rule out cement leakage or other detrimental effects caused by higher intravertebral pressure.
CT scans were used to assess cement distribution. From gross inspection, the cement in the irrigated samples was more even and homogeneous than that in the unirrigated ones. Compared with the control group, the density of bone cement in the irrigation group tended to be more consistent and the borders were smoother. This may be a result of removing the bone marrow and fat which were barriers in the cement diffusion process. The composition of bone cement clumps was simple, and the resistance of bone cement to diffuse was reduced. So the cement diffusion tended to be regular. The leakage rate was lower in the irrigated group than in the unirrigated ones. The CMV was smaller in the former than in the latter. The CMV represented the volume, which included the filled cement, trabecula, and remaining fat and marrow. The decrease in CMV further verified the effect of removing the fat and marrow from the vertebral body through irrigation.
In this study, an originally designed unilateral pulsed jet lavage system was applied and could reduce the intravertebral pressure and leakage during vertebroplasty. One limitation of our study was its in vitro nature. Without in vivo studies, the decreased intravertebral pressure could not be directly correlated with the reduced rate of fat or cement embolism during vertebroplasty. Another limitation was the small sample size, which could cause an adverse effect on data analysis. Further in vivo studies are recommended to validate the clinical values of a unilateral jet lavage system in vertebroplasty.
Conclusions
Unilateral pulsed jet lavage prior to vertebroplasty shows potential for clinical application. This process can reduce the cement leakage rate and improve cement distribution by removing the intravertebral fat and marrow and decreasing the intravertebral pressure.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CT:
-
Computed tomography
- CMV:
-
Cement mass volume
- PVP:
-
Percutaneous vertebroplasty
- PKP:
-
Percutaneous kyphoplasty
- HP:
-
Half volume pressure
- MP:
-
Maximum intravertebral pressure
References
Gerling MC, Eubanks JD, Patel R, Whang PG, Bohlman HH, Ahn NU. Cement augmentation of refractory osteoporotic vertebral compression fractures. Spine. 2011;36(19):E1266–9.
Pneumaticos SG, Triantafyllopoulos GK, Evangelopoulos DS, Hipp JA, Heggeness MH. Effect of vertebroplasty on the compressive strength of vertebral bodies. The Spine Journal. 2013;13(12):1921–7.
Barr JD, Barr MS, Lemley TJ, McCann RM. Percutaneous vertebroplasty for pain relief and spinal stabilization. Spine (Phila Pa 1976). 2000;25(8):923–8.
Heini PF. The current treatment—a survey of osteoporotic fracture treatment. Osteoporotic spine fractures: the spine surgeon’s perspective. Osteoporosis International. 2004;16(S02):S85–92.
Klazen CAH, Lohle PNM, de Vries J, Jansen FH, Tielbeek AV, Blonk MC, et al. Vertebroplasty versus conservative treatment in acute osteoporotic vertebral compression fractures (Vertos II): an open-label randomised trial. The Lancet. 2010;376(9746):1085–92.
Benneker LM, Heini PF, Suhm N, Gisep A. The effect of pulsed jet lavage in vertebroplasty on injection forces of polymethylmethacrylate bone cement, material distribution, and potential fat embolism: a cadaver study. Spine (Phila Pa 1976). 2008;33(23):E906–10.
Boger A, Benneker LM, Krebs J, Boner V, Heini PF, Gisep A. The effect of pulsed jet lavage in vertebroplasty on injection forces of PMMA bone cement: an animal study. Eur Spine J. 2009;18(12):1957–62.
Benneker LM, Krebs J, Boner V, Boger A, Hoerstrup S, Heini PF, et al. Cardiovascular changes after PMMA vertebroplasty in sheep: the effect of bone marrow removal using pulsed jet-lavage. European Spine Journal. 2010;19(11):1913–20.
Albers CE, Schott PM, Ahmad SS, Benneker LM, Nieuwkamp N, Hoppe S. Vertebral body lavage reduces hemodynamic response to vertebral body augmentation with PMMA. Global Spine Journal. 2018;9(5):499–504.
Hoppe S, Elfiky T, Keel MJ, Aghayev E, Ecker TM, Benneker LM. Lavage prior to vertebral augmentation reduces the risk for cement leakage. Eur Spine J. 2016;25(11):3463–9.
Cheng X, Long H-Q, Xu J-H, Huang Y-L, Li F-B. Comparison of unilateral versus bilateral percutaneous kyphoplasty for the treatment of patients with osteoporosis vertebral compression fracture (OVCF): a systematic review and meta-analysis. European Spine Journal. 2016;25(11):3439–49.
Sun H, Li C. Comparison of unilateral and bilateral percutaneous vertebroplasty for osteoporotic vertebral compression fractures: a systematic review and meta-analysis, Journal of Orthopaedic Surgery and Research. 2016;11(1):156.
Zhang LG, Gu X, Zhang HL, Zhang QG, Cai XB, Tao K. Unilateral or bilateral percutaneous vertebroplasty for acute osteoporotic vertebral fracture: a prospective study. J Spinal Disord Tech. 2015;28(2):E85–8.
Yan L, He B, Guo H, Liu T, Hao D. The prospective self-controlled study of unilateral transverse process-pedicle and bilateral puncture techniques in percutaneous kyphoplasty, Osteoporosis International. 2015;27(5):1849–55.
Chen C, Bian J, Zhang W, Zhang W, Zhao C, Wei H. Unilateral versus bilateral vertebroplasty for severe osteoporotic vertebral compression fractures. J Spinal Disord Tech. 2014;27(8):E301–4.
Zhao C, Sun Y, Jiang W, Cory E, Caffrey JP, Hsu FH, et al. Pulsed lavage cleansing of osteochondral grafts depends on lavage duration, flow intensity, and graft storage condition. Plos One. 2017;12(5):e0176934.
Mohamed R, Silbermann C, Ahmari A, Bohner M, Becker S, Baroud G. Cement filling control and bone marrow removal in vertebral body augmentation by unipedicular aspiration technique: an experimental study using leakage model. Spine (Phila Pa 1976). 2010;35(3):353–60.
Hershkovich O, Lucantoni C, Kapoor S, Boszczyk B. Bone marrow washout for multilevel vertebroplasty in multiple myeloma spinal involvement. Technical note. European Spine Journal. 2018;28(6):1455–60.
Li K, Yan J, Yang Q, Li Z, Li J. The effect of void creation prior to vertebroplasty on intravertebral pressure and cement distribution in cadaveric spines with simulated metastases. Journal of Orthopaedic Surgery and Research. 2015;10(1):20.
Acknowledgements
Not applicable
Funding
This study was supported by the National Natural Science Foundation of China (Grant No. 81401849).
Author information
Authors and Affiliations
Contributions
JY performed the experiments and participated in the design of the study. QL performed the experiments and wrote the manuscript. ZL, XG, PL, and PC assisted to perform the experiments. XL, YT, SY, and WX participated in the statistical analysis, literature search, data monitoring, and figure making. YZ conceived the study, participated in its design and coordination, and helped to draft the manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committee of Shandong University.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yan, J., Liu, Q., Zheng, Y. et al. Effect of unilateral pulsed jet lavage prior to vertebroplasty on the intravertebral pressure and cement distribution. J Orthop Surg Res 15, 259 (2020). https://doi.org/10.1186/s13018-020-01779-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-020-01779-3