
Abstract
Background
Patients with locally advanced colon cancer (LACC) have a relatively poor prognosis despite radical resection and adjuvant chemotherapy. This study investigated the treatment efficacy and toxicity of neoadjuvant chemoradiotherapy in patients with LACC.
Methods
We retrospectively reviewed 36 patients with LACC preoperatively treated with chemotherapy and radiotherapy. Patients were administered chemoradiotherapy, which comprised radiotherapy and neoadjuvant chemotherapy involving a 5-fluorouracil, leucovorin, and oxaliplatin regimen every 2 weeks.
Results
Median age was 64 years (45–86 years) and median follow-up period was 23.5 months (5.0–49.1 months). Seven (19.4%) patients developed grade 3 or 4 adverse events during neoadjuvant concurrent chemoradiotherapy. Pathologic responses were not evaluated in two patients who did not undergo radical resection. Of the 34 patients who underwent surgery, nine (26.4%) achieved a pathologic complete response (pCR). The 2-year estimated overall survival and disease-free survival rates were 88.7% and 73.6%, respectively.
Conclusions
Our results demonstrated that neoadjuvant chemoradiotherapy is feasible and safe. A prominent pCR rate with an acceptable toxicity profile suggests that the multimodality therapy might be a treatment option for patients with LACC.
Similar content being viewed by others


Background
Worldwide, colorectal cancer is the third most commonly diagnosed cancer in men and the second most commonly diagnosed cancer in women [1]. In Taiwan, colorectal cancer is the most common cancer, with a rapid increase in its prevalence, and is the third leading cause of cancer-related death [2]. Complete tumor removal surgery with a margin negative resection (R0) is the only curative modality for localized colon cancer. However, treatment results for locally advanced colon cancer (LACC), which is clinically defined as a primary tumor that directly invades adjacent structures or by the presence of extensive nodal involvement that renders curative resection infeasible, remain disappointing despite recent developments in surgery with subsequent adjuvant chemotherapy [3, 4]. The 5-year survival rates for patients with stage IIC, IIIB, and IIIC LACC were reported to be 37.3%, 46.3 and 28%, respectively [5], which has prompted researchers to investigate new treatment approaches for LACC in order to resolve the problems of markedly low survival rates resulting from tumor invasion to adjacent organs or extensive lymph node metastasis.
Neoadjuvant concurrent chemoradiotherapy (CCRT) instead of initial surgery is the current standard treatment for locally advanced rectal cancer, which has been well-established by randomized trials [6, 7]. The Chinese FOWARC randomized phase III trial demonstrated that patients with locally advanced rectal cancer treated with neoadjuvant 5-fluorouracil, leucovorin, and oxaliplatin (FOLFOX)-based CCRT achieved a higher pathologic complete response (pCR) rate than those treated with fluorouracil-based CCRT or perioperative FOLFOX alone [8]. However, the role of radiotherapy in the treatment of LACC remains unclear. Although benefits of postoperative radiotherapy have been reported in selected groups of patients with LACC [9, 10], the intergroup 0130 trial demonstrated that there was no difference in overall survival and disease-free survival between LACC patients receiving postoperative chemotherapy alone and those receiving postoperative CCRT [11]. In addition, hematologic toxicity was higher in the CCRT group. However, the intergroup 0130 trial has been criticized for its slow accrual and a large number of ineligible patients. For neoadjuvant CCRT in patients with LACC invading adjacent organs or extensive lymph node metastasis, the advantages of neoadjuvant CCRT have been reported in limited case reports and two small case series [12–15]. On the basis of our previous reports, which indicated that neoadjuvant FOLFOX-based CCRT resulted in a pCR rate of up to 31.6% in patients with locally advanced rectal cancer [16], we adopted the same treatment modality in patients with LACC to potentially improve their oncologic outcomes.
The present study investigated the treatment efficacy, toxicity and short-term oncologic outcome of neoadjuvant FOLFOX-based CCRT in patients with LACC.
Methods
The present study included 36 consecutive patients who received a histopathological diagnosed of colon adenocarcinoma and were treated with neoadjuvant CCRT followed by radical resection with curative intent in a single institute between January 2012 and June 2016. Multidisciplinary cancer conferences have recommended that patients with potentially suitable for incomplete resection of LACC should receive neoadjuvant CCRT. The potential for incomplete resection was defined by a T3 tumor with extramural extension of >5 mm or a T4 tumor diagnosed by imaging studies. Other inclusion criteria were colon cancer located above 15 cm from the anal verge, an Eastern Cooperative Oncology Group score of 0–2, and no evidence of distant metastasis at diagnosis. The exclusion criteria were a history of previous or synchronous malignancies other than nonmelanoma skin cancer and the presence of serious medical comorbidities that may influence treatment compliance. Medical records were reviewed to analyze the treatment efficacy, toxicity and short-term oncologic outcomes. The present study was approved by the Institutional Ethics Committee of our hospital. Pretreatment evaluation entailed a complete medical history review and physical examination, colonoscopy, tumor biopsy, chest radiography, abdominal and pelvic computed tomography (CT) with or without magnetic resonance imaging, carcinoembryonic antigen (CEA) level assessment, and routine laboratory tests.
Preoperative treatment
The concurrent chemotherapy regimen was a biweekly schedule of FOLFOX. Each cycle of FOLFOX consisted of oxaliplatin (85 mg/m2) and folinic acid (400 mg/m2) infusion on day 1 followed by a 46-h infusion of 5-fluorouracil (5-FU, 2800 mg/m2) repeated every 2 weeks. All patients received concurrent chemotherapy and radiotherapy. After completion of radiotherapy, all patients received chemotherapy twice weekly until surgery. Patients underwent surgery about 4 weeks after completing preoperative chemotherapy.
All patients underwent a planning CT in the supine position and were immobilized with custom thermoplastic immobilization devices before initiating radiotherapy. Target volumes were delineated according to the International Commission on Radiation Units and Measurements reports 50 and 62 [17]. The gross tumor volume (GTV) was defined as the macroscopic tumor and enlarged lymph nodes visible on diagnostic CT images. The clinical target volume (CTV) was the GTV plus a 15- to 20-mm margin, and the planning target volume was the CTV plus a 10- to 15-mm margin. Organs at risk (OAR), namely kidney, small bowel, liver, and spinal cord, were contoured. A radiation dose of 45–50.4 Gy was administered in 25–28 fractions. The dose constraints for OARs were as follows: the V30 of the liver was kept at <30%; the mean dose and V20 of the kidneys were restricted to <15 Gy and <30%, respectively; the volume of small bowel receiving >50 Gy was limited to <1 cc; and the maximal dose to the spinal cord was restricted to <45 Gy.
Surgery and pathology review
Patients underwent elective surgery at >6 weeks after completion of radiotherapy. The pathologic tumor (T) and nodal (N) stages (ypT and ypN, respectively) of the tumor, histological grade, lymphovascular invasion, perineural invasion, tumor regression grade (TRG), and status of the circumferential, proximal, and distal resection margins were documented. The tumor response after CCRT was assessed according to the American Joint Committee on Cancer (AJCC) system as follows [18]: Grade 0, no residual cancer cells; Grade 1, single cell or small group of cancer cells (major regression); Grade 2, residual cancer with desmoplastic response (moderate regression); and Grade 3, minimal evidence of tumor response. A circumferential resection margin (CRM) of <1 mm was defined as an involved CRM [19]. A pCR was defined as the absence of viable cancer cells in the pathological specimens, including primary tumor and lymph nodes (ypT0N0), after neoadjuvant CCRT.
Postoperative chemotherapy
Fifteen patients received an adjuvant chemotherapy regimen of FOLFOX. Adjuvant UFUR (tegafur and uracil) and capecitabine were administered in 11 and 5 patients, respectively; 3 patients did not receive postoperative chemotherapy. Two patients were transferred to the folinic acid, 5-FU, and irinotecan (FOLFIRI) regimen after laparotomy because of a poor response to the FOLFOX-based CCRT and the development of distant metastasis.
Toxicity evaluation and follow-up
During CCRT and in postoperative follow-up, acute adverse events at each visit were graded according to the Common Terminology Criteria for Adverse Events (CTCAE), version 3.0 (http://ctep.cancer.gov/reporting/ctc.html). Late radiation toxicity was scored using the Radiation Therapy Oncology Group Late Radiation Morbidity Scoring System. After surgery, patients were followed monthly for 6 months and subsequently once every 2–3 months to date.
Endpoints and statistics
The pCR rate was the primary endpoint of the study. Secondary endpoints were multimodality therapy-associated toxicities, TGR, and R0 resection rate. Downstaging was determined according to the response between the clinical T or N stage before neoadjuvant CCRT and the postoperative pathological T or N stage.
Descriptive statistics are presented as proportions and medians. The chi-squared test and Fisher’s exact test were used to compare the categorical data, and normally distributed continuous variables were analyzed using the Student t test. Disease-free survival (DFS) was measured from the date of onset of CCRT to the date of any type of recurrence or last follow-up. Overall survival (OS) was defined as the time from the onset of CCRT until death due to any cause or until the final follow-up. Survival rates were estimated using the Kaplan–Meier method. Data analyses were performed using JMP software (version 9.0, SAS Institute Inc., Cary, NC, USA).
Results
The median age was 64 years (45–86 years). Most tumor locations were the sigmoid colon (58.4%) followed by the ascending colon. Four patients received three-dimensional conformal radiotherapy using either three or four fields. Volumetric-modulated arc therapy (VMAT) and helical tomotherapy were administered to 22 and 10 patients, respectively. Table 1 lists the patient and treatment characteristics.
Acute toxicity and treatment compliance
Table 2 presents the acute adverse events during neoadjuvant CCRT. Overall, seven (19.4%) of the 36 patients experienced grade 3 or 4 adverse events during neoadjuvant CCRT. Leukopenia was defined according to the CTCAE, version 3.0, and leucopenia (83.2%) was the most common adverse event; however, most events (69.4%) were of grade 1 or 2 and were manageable in all patients. For non-hematologic toxicity, fatigue and nausea were the leading side effects caused by CCRT. Moreover, there were no grade 4 adverse events or neoadjuvant CCRT-related deaths.
Of all the patients, only one did not complete the prescribed radiation course (50.4 Gy); radiotherapy was interrupted at 46.8 Gy with two fractions remaining because of grade 3 diarrhea and grade 2 vomiting. The patient with sigmoid colon cancer did not complete the radiotherapy during the study period; however, he finally underwent surgery 51 days after completion of radiotherapy. The median radiotherapy duration was 35 days (32–49 days). Two patients temporarily discontinued preoperative chemotherapy because of neutropenic fever (n = 1) and grade 3 diarrhea with dehydration (n = 1), and both of the two patients continued scheduled preoperative chemotherapy after management of those adverse events.
Surgery and pathologic response
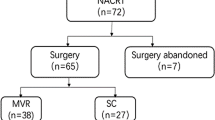
The median interval between radiotherapy completion and surgery was 11 weeks (6–25 weeks). All but two patients underwent surgery after neoadjuvant CCRT. Of the 34 patients receiving surgery, sigmoidectomy was performed in 17 (50%), right hemicolectomy in 12 (35.3%), and left hemicolectomy in five (14.7%) patients. Multivisceral resection was performed in 6 patients: 2 patients underwent colectomy plus partial cystectomy; 2 patients underwent colectomy plus resection of small intestine; 1 patient underwent colectomy plus partial gastrectomy; 1 patient underwent colectomy plus extensive resection of visceral peritoneum. Of the 4 patients diagnosed with bladder invasion, 2 received a partial cystectomy and 2 underwent a simple colectomy while preserve the bladder intact. Two patients did not undergo radical resection after neoadjuvant therapy. One patient with sigmoid colon cancer accompanied by uterus and left ureter invasion did not undergo radical resection after neoadjuvant treatment because of tumor invasion to the common iliac artery, which was observed during the surgery. Therefore, the tumor was not resected and the patient was administered 10 cycles of FOLFOX. Thereafter, FOLFIRI was administered as a second-line chemotherapy, and the patient’s condition was stable for 15 months at the final follow-up. The other patient with ascending colon cancer, T4aN2bM0, developed peritoneal carcinomatosis, which was revealed by CT images, after completion of the neoadjuvant FOLFOX-based CCRT; therefore, surgery was not performed. Two cycles of the FOLFIRI regimen were administered to the patients for disease control; however, the patient died because of tumor progression at 7 months after diagnosis.
Table 3 lists the pathologic results and treatment efficacy. Final pathologic analysis revealed that of the 34 patients, nine (26.4%) achieved ypT0 (no viable tumor in the primary site) and 28 (82.4%) achieved ypN0. The median number of lymph nodes retrieved was 11 (3–26). The resection margin was free of cancer cells in 31 (91.2%) of the 34 patients. Using a univariate analysis of the correlation between positive surgical margins and clinicopathologic features, the unfavorable tumor regression (TRG 3–4 versus TRG 0–1; p = 0.030), CEA level > 5 (p = 0.041), and ypT4 disease (p = 0.042) were associated with positive surgical margins. Of the 34 patients who underwent surgery, pCR, major regression (TRG 1), and moderate regression (TRG 2) were achieved in 9 (26.4%), 11 (32.4%), and 7 patients (20.6%), respectively, and 14 patients (41.2%) downstaged to the ypT0-2 stage. Comparison between the changes in the clinical and pathologic stages revealed that TN downstaging was achieved in 29 (85.3%) of the 34 patients; primary tumor and nodal downstaging were achieved in 24 (70.6%) and 31 (91.2%) of the 34 patients, respectively.
Table 4 summarizes the pathologic evaluation of primary tumor after neoadjuvant CCRT compared with that of the initial clinical stage. Of the 23 patients with clinical T4 tumors, five (21.7%) achieved ypT0 after intensified neoadjuvant CCRT, and clinical T4 tumors in eight patients (34.8%) were downstaged to ypT0-2.
Postoperative complications
Surgical mortality was not observed within 30 days after surgery. Of the 34 patients, five (14.7%) experienced postoperative complications requiring medical or surgical interventions. One patient developed a wound abscess on a previous drainage site, which resulted in a postoperative enterocutaneous fistula at 3 weeks, and this healed following antibiotic treatment. Another patient developed an intra-abdominal infection because of anastomotic leakage at 1 month after right hemicolectomy and temporary ileostomy closure; this patient finally recovered after undergoing another ileostomy along with antibiotic treatment. Two patients required surgical interventions because of adhesion ileus; one patient underwent enterolysis 1 month after left hemicolectomy and the other required segmental resection of small bowel at 32 months after extended left hemicolectomy. One patient developed a postoperative chronic rectovaginal fistula at 7 months and died of tumor progression.
Failure patterns and survival data
Median follow-up period was 23.5 months (5.0–49.1 months). The 2-year estimated OS and DFS rates were 88.7 and 73.6%, respectively (Fig. 1). Of the 34 patients who completed neoadjuvant CCRT and radical resection, four (11.8%) experienced local recurrence and five (14.7%) developed distant metastasis. The most common first site of distant failure was lung metastasis (n = 2), followed by liver metastasis (n = 1), retroperitoneal lymph node metastasis (n = 1), and adrenal gland metastasis (n = 1). Univariate analysis of the correlation between local recurrence and clinicopathologic features, we found that positive surgical margins (p = 0.003), unfavorable tumor regression (TRG 3–4 versus TRG 0–1; p = 0.022), and ypT4 disease (p = 0.055) were associated with local recurrence.

Overall and disease-free survival rates. a Overall survival rate and (b) disease-free survival rate in patients with locally advanced colon cancer receiving neoadjuvant chemoradiation and radical resection
Discussion
According to our review of relevant literature, the present clinical study used the largest sample for investigating the role of combined neoadjuvant oxaliplatin-based chemoradiotherapy in the treatment of primary LACC [20]. Our data demonstrated that the intensified multimodality approach resulted in an excellent pCR rate of 26.4% with an acceptable toxicity profile. However, this multimodal therapy should be used cautiously in clinical practice because of the limited sample size and short follow-up period of the present study. Our results, nevertheless, suggest that intensified neoadjuvant CCRT should be considered as a treatment option for patients with LACC, particularly those with potentially threatened surgical resection margins.
Evidence has indicated that nodal involvement is a major predictor of oncologic outcomes in patients with colorectal cancer [21, 22]. In our study, 82.4% of the patients did not develop nodal diseases after neoadjuvant CCRT. Furthermore, in a surgical series, pathologically positive nodal involvement was observed in approximately 69% patients with LACC [23]. The high pN0 rate in our study may be attributable to the marked influence of the neoadjuvant CCRT. For locally advanced rectal cancer, the neoadjuvant CCRT has been associated with nodal downstaging and a decrease in the pathologic lymph node harvest [16, 24]. Our findings reveal a similar effect of the neoadjuvant CCRT on eradication of lymph node metastasis in LACC. However, OS and DFS rates did not differ significantly between the patients with and without nodal metastasis.
Evidence has demonstrated that patients with locally advanced rectal cancer who achieved a pCR to neoadjuvant CCRT exhibited excellent tumor control and survival rates [25]. Moreover, numerous studies have added oxaliplatin into neoadjuvant fluorouracil-base treatment to enhance pCR rates. Of the six large phase III trials (ACCORD 12/0405-Prodige 2, STAR-01, National Surgical Adjuvant Breast and Bowel Project R04, CAO/ARO/AIO-04, and PETTAC6), only CAO/ARO/AIO-04 demonstrated that the addition of oxaliplatin improved DFS and a pCR rate [26–30]. Garcia-Aguilar et al. reported that extending FOLFOX chemotherapy after neoadjuvant CCRT and before surgery in locally advanced rectal cancer resulted in a pCR arte of 38% [31]. The FOWARC trial demonstrated that FOLFOX chemotherapy administered concurrently with and following radiotherapy resulted in a higher pCR rate than fluorouracil-based CCRT or perioperative FOLFOX alone [8]. Our prior study also showed similar results to FOWARC trial [16]. However, the correlation between a pCR and clinical outcome in colon cancer has been rarely reported. To date, several studies have investigated the role of neoadjuvant chemotherapy in patients with LACC; however, the benefits of combined radiotherapy and chemotherapy for primary LACC have been rarely evaluated. Only a Canadian group reported that of the total 33 patients with LACC that were treated with neoadjuvant concurrent 5-FU and radiotherapy, only one patient (3%) achieved a pCR [14]. The FOxTROT trial assessed the role of neoadjuvant chemotherapy in LACC management by evaluating the efficacy and safety of the preoperative FOLFOX-based chemotherapy in a randomized controlled manner; two patients (2%) of the neoadjuvant group reported pCRs [32]. Furthermore, a phase II trial demonstrated that three (4.2%) of the 71 operated patients achieved a pCR after three cycles of neoadjuvant XELOX [capecitabine (2000 mg/m2) orally administered on days 1–14 (q3w) and oxaliplatin (130 mg/m2) intravenously infused on day 1 (q3w)] [33]. Arredondo et al. investigated 65 patients with LACC treated with either neoadjuvant XELOX- or FOLFOX-based chemotherapy; three patients (4.6%) had a pCR [34]. In the present study, patients with LACC were administered with neoadjuvant FOLFOX-based CCRT that resulted in a pCR rate of 26.4%, which was higher than that reported in other neoadjuvant studies (2–4.6%) [14, 33, 34].
The prognosis in patients with LACC remains discouraging even with the current standard treatment of radical resection followed by adjuvant chemotherapy. Danielle et al. analyzed the Surveillance, Epidemiology, and End Results Program database (1988–2008) and reported that the 5-year OS rates of patients with 7th AJCC stages IIC, IIIB, and IIIC were 54.6%, 59.0, 47.9%, respectively [35]. Therefore, treatment strategies should be modified to improve the oncologic outcomes in patients with LACC. Neoadjuvant CCRT is the standard of care in patients with locally advanced rectal cancer [6]. Although several studies have reported promising results for the neoadjuvant chemotherapy, we aimed to use an intensified multimodality approach of combined chemotherapy and radiotherapy in patients with LACC, particularly in those with clinical T4 tumors. Arredondo et al. investigated the efficacy and safety of neoadjuvant chemotherapy and reported that only 12 patients (18.5%) had T4 tumors [34]. Jakobsen et al. conducted a phase II trial in patients with LACC treated with neoadjuvant chemotherapy and reported that 11 (15%) patients developed T4 tumors [33]. Furthermore, the phase III FOxTROT trial reported on 30 patients (30%) with T4 tumors [32]. In our study, the proportion of patients with a T4 tumor was 63.9% (23 of the 36 patients), which is higher than that reported in other studies. The prognosis of a T4 colon cancer remains the worst, and T4 tumors have been closely associated with an involved resection margin [35, 36]. Therefore, we aimed to maximally treat LACC with a combination of radiotherapy and chemotherapy and obtained a R0 resection rate of 91.2%. Of the 23 patients with cT4 tumors in the present study, two (8.7%) did not undergo surgery because of a poor response to neoadjuvant CCRT, and 18 (85.7%) of the 21 patients received radical resection of cT4 tumors obtained R0 resections in our study.
Several studies have investigated the efficacy and safety of neoadjuvant chemotherapy for LACC [33, 37, 38]. The inclusion criteria for neoadjuvant chemotherapy was T4 or T3 with extramural extension >5 mm. By contrast, the eligibility for neoadjuvant CCRT was the tumor extensively involved other organs/structures on imaging studies or the tumor considered to be unresectable after exploratory laparotomy. Qiu et al. delivered neoadjuvant CCRT for 21 patients with unresectable locally advanced sigmoid colon cancer [20]. Of the 19 patients with clinical T4 diseases, seven patients achieved a pCR after CCRT. The results were similar to our study, in which five patients achieved a pCR after neoadjuvant CCRT among the 23 patients with clinical T4 tumors. For tolerability, both neoadjuvant chemotherapy and neoadjuvant CCRT were well-tolerable in patients with LACC, but toxicity was generally higher in neoadjuvant CCRT [14, 20, 32, 33]. Therefore, clinical T4 tumors, especially unresectable mass or tumors extensively involved adjacent structures, are potential indications for neoadjuvant CCRT. In addition, patients with a locally extensive T3 tumor or patients unable to tolerate CCRT may be candidates for neoadjuvant chemotherapy. However, the indications for neoadjuvant CCRT or chemotherapy need to be validated in more prospective randomized studies.
In en bloc multivisceral resections for primary locally advanced colorectal cancer, R0 resection rates ranged from 40 to 93%, with high postoperative complications (11%–40%) and a nonnegligible mortality up to 9% [36, 39, 40]. Cukier et al. analyzed the oncologic outcomes of neoadjuvant CCRT followed by multivisceral resection for primary LACC and reported a R0 resection rate of 100%, with a postoperative complication rate of 36% and zero surgical mortality [14]. Qiu et al. found that neoadjuvant CCRT can effectively reduce the peripheral tumor infiltration and thereby decrease the necessity for multivisceral resection. Therefore, neoadjuvant CCRT may decrease postoperative complications caused by multivisceral resection [20]. In the present study, the R0 resection rate was 91.2% with a postoperative complication rate of 14.7% and without surgical mortality, despite the intensified neoadjuvant CCRT. Our results suggested that neoadjuvant CCRT followed by radical resection does not increase a postoperative complication rate compared to resection alone (11%–40%).
However, the eligibility criterion of patients with LACC suitable for a neoadjuvant CCRT remains debatable. Moreover, the risk of overtreatment must be minimized because of occasional discrepancies between the clinical and pathologic stages. CT images have been primarily examined to select patients eligible to receive neoadjuvant therapy for colon cancer, and the accuracy of CT staging has improved. Numerous studies have demonstrated that CT can identify T3 tumors with extramural extension or T4 tumors, which are candidates for neoadjuvant therapy [28, 34, 37]. In contrast to tumor depth prediction, accurate nodal status prediction through CT remains difficult. Therefore, we assessed the CT images and T stage to guide neoadjuvant CCRT.
Cukier et al. reported that 9% of the patients with LACC experienced grade 3 or higher grades of adverse events during 5-FU-based CCRT [14]. In the present study, we used oxaliplatin and 5-FU in the neoadjuvant setting to maximize the effect of CCRT on LACC, and 19.4% of patients experienced grade 3 adverse events during neoadjuvant CCRT. Of all the patients, only one patient did not complete the prescribed radiation course, although FOLFOX-based CCRT had a relatively higher toxicity rate than that in 5-FU-based CCRT. However, the incidence of grade 3 or 4 adverse events reported in the present study were considerably lower than those reported in our previous studies or in other studies investigating the influence of FOLFOX-based CCRT in patients with rectal cancer, which ranged from 24% to 40% [16, 28, 37]. In our study, 88.9% of the patients received intensity-modulated radiotherapy with either VMAT or tomotherapy, which might partly contribute to the improved toxicity profiles because of normal organ sparing [41].
The present study has some limitations. First, because of the relatively small sample and short follow-up period, long-term efficacy and adverse events could not be addressed. Second, this was a retrospective study; therefore, the sampling may have been affected by selection bias. Third, the postoperative chemotherapy regimens were varied in our study, which might contribute to disease control and survival.
Conclusions
Our results demonstrate that neoadjuvant chemoradiotherapy is feasible and safe. A high pCR and R0 resection rate with an acceptable toxicity profile suggests that multimodality therapy is a treatment option for patients with LACC. Additional prospective randomized studies are warranted to validate our results.
Abbreviations
- 5-FU:
-
5-fluorouracil
- AJCC:
-
American Joint Committee on Cancer
- CCRT:
-
Concurrent chemoradiotherapy
- CEA:
-
Carcinoembryonic antigen
- CRM:
-
Circumferential resection margin
- CT:
-
Computed tomography
- CTCAE:
-
Common Terminology Criteria for Adverse Events
- CTV:
-
Clinical target volume
- DFS:
-
Disease-free survival
- FOLFIRI:
-
folinic acid, 5-fluorouracil, and irinotecan
- FOLFOX:
-
5-fluorouracil, leucovorin, and oxaliplatin
- GTV:
-
Gross tumor volume
- LACC:
-
Locally advanced colon cancer
- N:
-
Nodal
- OAR:
-
Organs at risk
- OS:
-
Overall survival
- pCR:
-
Pathologic complete response
- R0:
-
Margin negative resection
- T:
-
Tumor
- TRG:
-
Tumor regression grade
- UFUR:
-
Tegafur and uracil
- VMAT:
-
Volumetric-modulated arc therapy
References
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. doi:10.3322/caac.20107.
Ministry of Health and Welfare, the Executive Yuan, Republic of China. Health and Vital Statistics. [http://www.mohw.gov.tw/CHT/Ministry/]. Accessed 2013.
Hohenberger W, Weber K, Matzel K, Papadopoulos T, Merkel S. Standardized surgery for colonic cancer: complete mesocolic excision and central ligation--technical notes and outcome. Colorectal Dis. 2009;11(4):354–64. doi:10.1111/j.1463-1318.2008.01735.x. discussion 64–5.
Andre T, Boni C, Mounedji-Boudiaf L, Navarro M, Tabernero J, Hickish T, et al. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med. 2004;350(23):2343–51. doi:10.1056/NEJMoa032709.
Edge SB, Byrd DR, C. CC, Fritz AG, Greene F, Trotti A. AJCC Cancer Staging Manual 7th edition. 2010; Springer, New York, NY:143–64.
Sauer R, Becker H, Hohenberger W, Rodel C, Wittekind C, Fietkau R, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004;351(17):1731–40. doi:10.1056/NEJMoa040694.
Roh MS, Colangelo LH, O’Connell MJ, Yothers G, Deutsch M, Allegra CJ, et al. Preoperative multimodality therapy improves disease-free survival in patients with carcinoma of the rectum: NSABP R-03. J Clin Oncol. 2009;27(31):5124–30. doi:10.1200/jco.2009.22.0467.
Deng Y, Chi P, Lan P, Wang L, Chen W, Cui L, et al. Modified FOLFOX6 with or without radiation versus fluorouracil and leucovorin with radiation in neoadjuvant treatment of locally advanced rectal cancer: initial results of the Chinese FOWARC multicenter, open-label, randomized three-Arm phase III trial. J Clin Oncol. 2016;34(27):3300–7. doi:10.1200/jco.2016.66.6198.
Willett CG, Fung CY, Kaufman DS, Efird J, Shellito PC. Postoperative radiation therapy for high-risk colon carcinoma. J Clin Oncol. 1993;11(6):1112–7. doi:10.1200/jco.1993.11.6.1112.
Willett CG, Tepper JE, Skates SJ, Wood WC, Orlow EC, Duttenhaver JR. Adjuvant postoperative radiation therapy for colonic carcinoma. Ann Surg. 1987;206(6):694–8.
Martenson Jr JA, Willett CG, Sargent DJ, Mailliard JA, Donohue JH, Gunderson LL, et al. Phase III study of adjuvant chemotherapy and radiation therapy compared with chemotherapy alone in the surgical adjuvant treatment of colon cancer: results of intergroup protocol 0130. J Clin Oncol. 2004;22(16):3277–83. doi:10.1200/jco.2004.01.029.
Mizukami H, Yoshizawa Y, Sasaya S, Nemoto H, Maezawa K, Sanada Y. A case of advanced colon cancer invading the rectum effectively treated with chemoradiation therapy before surgery. Gan To Kagaku Ryoho. 2007;34(6):953–6.
Kuga Y, Tanaka T, Arita M, Okanobu H, Miwata T, Yoshimi S, et al. A case of effective chemotherapy using S-1 and CPT-11 following chemoradiotherapy with UFT and Leucovorin for unresectable advanced sigmoid colon cancer. Gan To Kagaku Ryoho. 2010;37(3):531–4.
Cukier M, Smith AJ, Milot L, Chu W, Chung H, Fenech D, et al. Neoadjuvant chemoradiotherapy and multivisceral resection for primary locally advanced adherent colon cancer: a single institution experience. Eur J Surg Oncol. 2012;38(8):677–82. doi:10.1016/j.ejso.2012.05.001.
Taylor WE, Donohue JH, Gunderson LL, Nelson H, Nagorney DM, Devine RM, et al. The Mayo Clinic experience with multimodality treatment of locally advanced or recurrent colon cancer. Ann Surg Oncol. 2002;9(2):177–85.
Huang CM, Huang MY, Tsai HL, Huang CW, Ma CJ, Yeh YS, et al. An observational study of extending FOLFOX chemotherapy, lengthening the interval between radiotherapy and surgery, and enhancing pathological complete response rates in rectal cancer patients following preoperative chemoradiotherapy. Therap Adv Gastroenterol. 2016;9(5):702–12. doi:10.1177/1756283x16656690.
International Commission on Radiation Units and Measurements. Prescribing, recording and reporting photon beam therapy ICRU report 62. Bethesda, MD: International Commission on Radiation Units and Measurements; 1999, 2010.
Mace AG, Pai RK, Stocchi L, Kalady MF. American Joint Committee on Cancer and College of American Pathologists regression grade: a new prognostic factor in rectal cancer. Dis Colon Rectum. 2015;58(1):32–44. doi:10.1097/dcr.0000000000000266.
Nagtegaal ID, Quirke P. What is the role for the circumferential margin in the modern treatment of rectal cancer? J Clin Oncol. 2008;26(2):303–12. doi:10.1200/jco.2007.12.7027.
Qiu B, Ding PR, Cai L, Xiao WW, Zeng ZF, Chen G, et al. Outcomes of preoperative chemoradiotherapy followed by surgery in patients with unresectable locally advanced sigmoid colon cancer. Chin J Cancer. 2016;35(1):65. doi:10.1186/s40880-016-0126-y.
Chang GJ, Rodriguez-Bigas MA, Skibber JM, Moyer VA. Lymph node evaluation and survival after curative resection of colon cancer: systematic review. J Natl Cancer Inst. 2007;99(6):433–41. doi:10.1093/jnci/djk092.
Ceelen W, Van Nieuwenhove Y, Pattyn P. Prognostic value of the lymph node ratio in stage III colorectal cancer: a systematic review. Ann Surg Oncol. 2010;17(11):2847–55. doi:10.1245/s10434-010-1158-1.
Rowe VL, Frost DB, Huang S. Extended resection for locally advanced colorectal carcinoma. Ann Surg Oncol. 1997;4(2):131–6.
Valentini V, Coco C, Picciocchi A, Morganti AG, Trodella L, Ciabattoni A, et al. Does downstaging predict improved outcome after preoperative chemoradiation for extraperitoneal locally advanced rectal cancer? A long-term analysis of 165 patients. Int J Radiat Oncol Biol Phys. 2002;53(3):664–74.
Martin ST, Heneghan HM, Winter DC. Systematic review and meta-analysis of outcomes following pathological complete response to neoadjuvant chemoradiotherapy for rectal cancer. Br J Surg. 2012;99(7):918–28. doi:10.1002/bjs.8702.
Gerard JP, Azria D, Gourgou-Bourgade S, Martel-Laffay I, Hennequin C, Etienne PL, et al. Comparison of two neoadjuvant chemoradiotherapy regimens for locally advanced rectal cancer: results of the phase III trial ACCORD 12/0405-Prodige 2. J Clin Oncol. 2010;28(10):1638–44. doi:10.1200/jco.2009.25.8376.
Aschele C, Cionini L, Lonardi S, Pinto C, Cordio S, Rosati G, et al. Primary tumor response to preoperative chemoradiation with or without oxaliplatin in locally advanced rectal cancer: pathologic results of the STAR-01 randomized phase III trial. J Clin Oncol. 2011;29(20):2773–80. doi:10.1200/jco.2010.34.4911.
O’Connell MJ, Colangelo LH, Beart RW, Petrelli NJ, Allegra CJ, Sharif S, et al. Capecitabine and oxaliplatin in the preoperative multimodality treatment of rectal cancer: surgical end points from National Surgical Adjuvant Breast and Bowel Project trial R-04. J Clin Oncol. 2014;32(18):1927–34. doi:10.1200/jco.2013.53.7753.
Rodel C, Graeven U, Fietkau R, Hohenberger W, Hothorn T, Arnold D, et al. Oxaliplatin added to fluorouracil-based preoperative chemoradiotherapy and postoperative chemotherapy of locally advanced rectal cancer (the German CAO/ARO/AIO-04 study): final results of the multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2015;16(8):979–89. doi:10.1016/s1470-2045(15)00159-x.
Schmoll H, Haustermans K, Price T, Nordlinger B, Hofheinz R, Daisne J. Preoperative chemoradiotherapy and postoperative chemotherapy with capecitabine and oxaliplatin versus capecitabine alone in locally advanced rectal cancer: Disease-free survival results at interim analysis. Proc Am Soc Clin Oncol. 2014;32(3501a).
Garcia-Aguilar J, Chow OS, Smith DD, Marcet JE, Cataldo PA, Varma MG, et al. Effect of adding mFOLFOX6 after neoadjuvant chemoradiation in locally advanced rectal cancer: a multicentre, phase 2 trial. Lancet Oncol. 2015;16(8):957–66. doi:10.1016/s1470-2045(15)00004-2.
Foxtrot Collaborative G. Feasibility of preoperative chemotherapy for locally advanced, operable colon cancer: the pilot phase of a randomised controlled trial. Lancet Oncol. 2012;13(11):1152–60. doi:10.1016/s1470-2045(12)70348-0.
Jakobsen A, Andersen F, Fischer A, Jensen LH, Jorgensen JC, Larsen O, et al. Neoadjuvant chemotherapy in locally advanced colon cancer. A phase II trial. Acta Oncol. 2015;54(10):1747–53. doi:10.3109/0284186x.2015.1037007.
Arredondo J, Baixauli J, Pastor C, Chopitea A, Sola JJ, Gonzalez I et al. Mid-term oncologic outcome of a novel approach for locally advanced colon cancer with neoadjuvant chemotherapy and surgery. Clin Transl Oncol. 2016. doi:10.1007/s12094-016-1539-4.
Hari DM, Leung AM, Lee JH, Sim MS, Vuong B, Chiu CG, et al. AJCC Cancer Staging Manual 7th edition criteria for colon cancer: do the complex modifications improve prognostic assessment? J Am Coll Surg. 2013;217(2):181–90. doi:10.1016/j.jamcollsurg.2013.04.018.
Mohan HM, Evans MD, Larkin JO, Beynon J, Winter DC. Multivisceral resection in colorectal cancer: a systematic review. Ann Surg Oncol. 2013;20(9):2929–36. doi:10.1245/s10434-013-2967-9.
Rodel C, Liersch T, Becker H, Fietkau R, Hohenberger W, Hothorn T, et al. Preoperative chemoradiotherapy and postoperative chemotherapy with fluorouracil and oxaliplatin versus fluorouracil alone in locally advanced rectal cancer: initial results of the German CAO/ARO/AIO-04 randomised phase 3 trial. Lancet Oncol. 2012;13(7):679–87. doi:10.1016/s1470-2045(12)70187-0.
Arredondo J, Gonzalez I, Baixauli J, Martinez P, Rodriguez J, Pastor C, et al. Tumor response assessment in locally advanced colon cancer after neoadjuvant chemotherapy. J Gastrointest Oncol. 2014;5(2):104–11. doi:10.3978/j.issn.2078-6891.2014.006.
Croner RS, Merkel S, Papadopoulos T, Schellerer V, Hohenberger W, Goehl J. Multivisceral resection for colon carcinoma. Dis Colon Rectum. 2009;52(8):1381–6. doi:10.1007/DCR.0b013e3181ab580b.
Lehnert T, Methner M, Pollok A, Schaible A, Hinz U, Herfarth C. Multivisceral resection for locally advanced primary colon and rectal cancer: an analysis of prognostic factors in 201 patients. Ann Surg. 2002;235(2):217–25.
Huang CM, Huang MY, Tsai HL, Huang CW, Ma CJ, Lin CH et al. A retrospective comparison of outcome and toxicity of preoperative image-guided intensity-modulated radiotherapy versus conventional pelvic radiotherapy for locally advanced rectal carcinoma. J Radiat Res. 2016. doi:10.1093/jrr/rrw098.
Acknowledgments
We thank Kaohsiung Medical University Hospital (KMUH104-4 M44, KMUHS10522, KMUHS10505, KMUHS10418, KMUHGCRC2016002) for assistance.
Funding
This work was supported by grants from the Excellence for Cancer Research Center.
Grant through funding by the Ministry of Science and Technology (MOST105-2325-B-037-001) and the Ministry of Health and Welfare (MOHW105-TDU-B-212-134007), Health and welfare surcharge of tobacco products, Taiwan, Republic of China. The study was supported by Kaohsiung Medical University “Aim for the top University Grant, grant no. KMU-TP105C01, KMU-TP105C11, KMU-TP106005, KMU-TP105A11, KMU-TP105A12, KMU-DK106005, SH000113 (Give2Asia) and the Grant of Biosignature in Colorectal Cancers, Academia Sinica, Taiwan.
Availability of data and materials
All data and materials have been presented in the manuscript.
Authors’ contributions
CMH and JYW participated in the design of the study, performed the statistical analysis and interpretation of data, and drafted the manuscript. CMH wrote the manuscript. CJM, YSY, HLT and CWH recruited patients to the study, and interpreted the clinical data. MYH and CJH are radiation oncologists who contributed to treat the patients. All authors read and approved the final manuscript.
Competing interests
The authors declare no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
This study was approved by the Institutional Review Board in Kaohsiung Medical University Hospital [KMUHIRB-E(II)-20150195]. Eligible patients were given written informed consent.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Huang, CM., Huang, MY., Ma, CJ. et al. Neoadjuvant FOLFOX chemotherapy combined with radiotherapy followed by radical resection in patients with locally advanced colon cancer. Radiat Oncol 12, 48 (2017). https://doi.org/10.1186/s13014-017-0790-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13014-017-0790-3