
Abstract
Background
Most recent publications have provided evidence for brace treatment in spinal deformities. The purpose of this study was to evaluate the rate of overtreatment for AIS and Kyphosis in Greece, according to the Society on Scoliosis Orthopedic Rehabilitation Treatment (SOSORT) and the Scoliosis Research Society (SRS) guidelines for brace treatment. To date, this is the first study to investigate overtreatment percentage in a group of patients with spinal deformities.
Methods
Cross-sectional study design and data analysis were performed in a group of patients that received treatment in a private clinic, in 2014. Of 289 patients treated with a brace, 167 young adolescents (126 females - 41 males, mean age 15, 7 years) were eligible for inclusion criteria (age 9–18 years, brace wearing). Overtreatment was defined as the unnecessary use of brace according to the international indications for brace treatment. Overtreatment was assessed by a BSPTS - Schroth certified physiotherapist. The brace prescription was made by 34 medical doctors from different geographical areas of Greece.
Results
The data analysis revealed that 71 out of 167 subjects (42,5 %) had received some kind of overtreatment. A further analysis showed that in the AIS subgroup, 20 subjects (16,9 %) had Cobb angles < 20°, 7 subjects (5,9 %) had Cobb angles 20 – 25° but good prognosis, 12 subjects (10,2 %) started bracing after Risser 4, and 12 subjects (10,2 %) had delayed brace weaning. It is noticeable that 8 subjects (6,8 %) were at Risser 5 with Cobb angle < 20° and were prescribed a brace. In the Kyphosis subgroup, 11 subjects (22,5 %) showed no signs of Scheuermann’s disease, 3 subjects (6,1 %) started bracing after Risser 4 or 5, and 6 subjects (12,2 %) had delayed brace weaning.
Conclusions
An extremely high rate of overtreatment (42, 5 %) was identified in a random group of adolescents treated with a brace for AIS and Kyphosis. Overtreating a child with a brace can cause social, financial and psychological problems. The present study pinpoints the need for an evidence-based approach to conservative treatment of idiopathic scoliosis and kyphosis. Overtreatment can be avoided when the indications are strictly based on the guidelines published internationally.
Similar content being viewed by others

Background
The Scoliosis Research Society (SRS) and the Society on Scoliosis Orthopedic Rehabilitation Treatment (SOSORT) have produced guidelines for the indications of treatment of Adolescent Idiopathic Scoliosis (AIS) [1, 2]. In general, mild scoliosis (Cobb angle < 25°) should be treated by observation according to SRS or by Physiotherapeutic Scoliosis Specific Exercises (PSSE) according to SOSORT, moderate to severe scoliosis (Cobb angle 25–40°), in skeletally immature adolescents by bracing and PSSE, and severe scoliosis (Cobb angle > 40°) by spinal fusion [1, 2]. The indications for bracing in Scheuermann kyphosis are Cobb angle >55° with vertebra wedging on x-ray [3] (Table 1).
A recent multicentered Randomised Controlled Trial (RCT) in United States confirmed the efficacy of brace treatment for AIS [4], while another RCT in Italy confirmed the efficacy of the PSSE to halt the progression in mild scoliosis [5]. Only a few studies have commented on the existence of the overtreatment of AIS and pinpointed the importance to follow the international guidelines of the SRS and SOSORT [2, 6, 7].
However, to date, there is no study to estimate the exact percentage of overtreatment with bracing in a population with AIS and Scheuermann kyphosis. The aim of this study is to investigate the overtreatment rate of bracing for spinal deformities in Greece, according to the SRS and SOSORT published guidelines.
Methods
Cross-sectional study design and data analysis were performed in a random group of patients that received treatment in a private clinic for conservative treatment of spinal deformities, in Athens during the year 2014. A total of 289 people were treated in the clinic, but only those who were eligible for the inclusion criteria of the study were analyzed. The inclusion criteria were age 9–18 years old and brace prescription for AIS or Scheuermann kyphosis.
Overtreatment is generally defined as the health care provided with a higher volume or cost than the appropriate and for the purpose of this study was defined as the unnecessary use of brace according to the SRS and the SOSORT indications for brace treatment. The overtreated individuals were those that should have never started treatment with a brace or those that brace weaning was very prolonged. Therefore, the variables to evaluate the overtreatment were the Cobb angle, the stage of maturity by Risser sign and age of menarche in girls, the vertebra wedging and Schmorl nodes on x-ray for Scheuermann kyphosis. The above variables were assessed by a Schroth certified physiotherapist (Barcelona Scoliosis Physical Therapy School – BSPTS). In order to avoid a misclassification of overtreatment for the borderline cases, a subsequent analysis of risk prognostic factors, such as the family history, the Angle of Trunk Rotation (ATR) measured by the scoliometer, the thoracic hypokyphosis and the curve type, were also performed for the cases with AIS and Cobb angle 20–29°, along with an analysis of the progression risk based on the Lonstein formula [8] (Table 2).
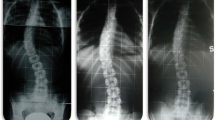
The assessment of the variables and the following statistical analysis was performed by only one Schroth Certified physiotherapist, due to the lack of qualified scoliosis experts in the clinic (Figs. 1, 2, 3 and 4). The brace prescription was made by 34 medical doctors (MD) from different geographical areas of Greece. The methods used for the present research were in compliance with the Helsinki Declaration and a consent form was signed by the subjects for allowance to use their clinical photographs.

Overtreatment case 1. Case 1: 16 years old, first brace at 15 years, 1 ½ year post-menarche, Risser 4, Th (R)11°, Lu (L) 18°, ATR Th(R) 3°, Lu (L) 4°. Brace prescription for 20 h

Overtreatment case 2. 15 years old, Lu (L) 18°, ATR 5°, Risser 5, 4 ½ years post-menarche, Brace prescription for 15-16 h, After 2 PSSE sessions she complained for pain only when she wore her brace

Overtreatment case 3. 17 years old, First brace 12 years, initially (2009) Th-Lu (R) 16°, Risser 0. 03/14: Th-Lu (R) 8°, ATR 4°, Risser 5, continue wearing the brace for 15-16 h, no brace weaning, 4 years post-menarche

Overtreatment case 4. 15 years old, 1 ½ years post-menarche, Risser 4, Th (L) 13°, Lu (R) 15°, ATR Th 2°, Lu 4°. Brace prescription for 18 h (12/14)
Results
Total results
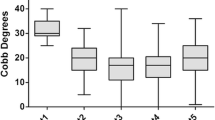
One hundred sixty seven subjects out of totally 289 treated fulfilled the inclusion criteria. All the subjects without a diagnosis of AIS or kyphosis and those treated only with PSSE were excluded from the study. 126 females and 41 males were included, the mean age was 15.7 years old, and 118 of them were diagnosed for AIS and 49 for kyphosis. The data analysis revealed that 71 out of 167 subjects (42.5 %) received some kind of overtreatment (Fig. 5). A simple chi-square test showed that the percentage of overtreatment was not statistically significant different (p = 0.77) for AIS (51/118, 43.2 %) and kyphosis (20/49, 40.8 %).

Lonstein formula and risk for progression
Results for AIS
For the AIS subgroup a further analysis showed that 20 individuals (16.9 %) had Cobb angle < 20°, 7 (5.9 %) had Cobb angle 20 – 25° but good prognosis according to the Lonstein formula, 12 (10.2 %) started their treatment with a brace after Risser 4, and 12 (10.2 %) of them had not reach brace weaning even a long time after skeletal maturity (Fig. 6). It should be noted that 8 individuals (6.8 %) were skeletally mature at Risser 5 with a Cobb angle <20° and were prescribed a brace (Fig. 7).

Total results for overtreatment

Results for AIS
Results for scheuermann kyphosis
For the Kyphosis subgroup a further analysis showed that 11 subjects (22.5 %) showed no Scheuermann’s disease findings on the x-ray (vertebra wedging and Schmorl nodes) and no clinical rigidity, 3 subjects (6.1 %) started brace treatment after Risser 4 and 6 subjects (12.2 %) had not reach brace weaning after growth completion (Fig. 8).

Results for kyphosis
Discussion
The results identified an extremely high percentage of overtreatment (42.5 %) in a random group of patients in Greece that received treatment with a brace for AIS and Kyphosis. This undesired situation in Greece can be attributed to a few different factors. Firstly, the fact that the brace prescription was made by 34 MD’s all over Greece seems that there is inadequate education in the field of conservative treatment of spinal deformities and negligence of the international guidelines for bracing. According to the incidence of progression by Lonstein and Carlson (1984) [8] (Table 3), many of the overtreated patients had actually no risk to progress, so no treatment was needed for them.
Another significant factor might be the still unknown role of the PSSE in the treatment of mild scoliosis. After the recent RCT of Monticone et al. (2014) [5], there is strong evidence that in many cases the PSSE can halt the progression of mild scoliosis (Cobb < 25°), so the PSSE can prevent the overuse of brace for this population. Other possible explanations could be the delayed diagnosis due to the poor school screening and potentially some unspecified non-scientific reasons.
A limitation of the present study could be considered the fact that the assessment was made by only one therapist, which means low inter-reliability. However, the results of the study can be generalized, because the brace prescription was made by 34 MDs from different geographical areas all over Greece.
Conclusions
The present study revealed a very high rate of overtreatment (42.5 %) with bracing for AIS and Kyphosis in Greece. Overtreating a child with a brace can cause social, financial and psychological problems [9]. However, the optimal treatment is not easily achieved (Table 4).
This study highlights the imperative need for an evidence-based approach to conservative treatment of idiopathic scoliosis and Scheuermann kyphosis. The undesired effects of overtreatment can be avoided when the indications for brace treatment are strictly based on the international guidelines. Moreover, the implementation of the PSSE for mild scoliosis could decrease even more the overtreatment rate. Future research in other countries could be useful for comparability of the results.
Abbreviations
- AIS:
-
Adolescent Idiopathic Scoliosis
- BSPTS:
-
Barcelona Scoliosis Physical Therapy School
- ATR:
-
Angle trunk rotation
- MD:
-
Medical doctor
- PSSE:
-
Physiotherapeutic Scoliosis Specific Exercises
- RCT:
-
Randomised Controlled Trial
- SOSORT:
-
Society On Scoliosis Orthopedic Rehabilitation Treatment
- SRS:
-
Scoliosis Research Society
References
The Scoliosis Research Society Brace Mannual. [http://www.srs.org/UserFiles/file/bracing-manual/section1.pdf]. Accessed 15 July 2015.
Negrini S, Aulisa AG, Aulisa L, Circo AB, De Mauroy JC, Durmala J, Grivas TB, Knott P, Kotwicki T, Maruyama T, Minozzi S, O’Brien JP, Papadopoulos D, Rigo M, Rivard CH, Romano M, Wynne J, Villagrasa M, Weiss HR, Zaina F. 2011 SOSORT guidelines: Orthopaedic and Rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis. 2012;7(1):3. doi:10.1186/1748-7161-7-3.
Scoliosis Research Society (SRS) Scheuermann’s Kyphosis/Disease. [https://www.srs.org/professionals/online-education-and-resources/conditions-and-treatments/kyphosis-in-the-adolescent-and-young-adult]. Accessed 15 July 2015.
Weinstein SL, Dolan LA, Wright JG, Dobbs MB. Effects of bracing in adolescents with idiopathic scoliosis. N Engl J Med. 2013;369(16):1512–21.
Monticone M, Ambrosini E, Cazzaniga D, Rocca B, Ferrante S. Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis. Results of a randomized controlled trial. Eur Spine J. 2014;23(6):1204–14.
Kotwicki T, Chowanska J, Kinel E, Czaprowski D, Tomaszewski M, Janusz P. Optimal management of idiopathic scoliosis in adolescence. Adolesc Health Med Ther. 2013;4:59–73.
Kotwicki T, Durmala J, Czaprowski D, Glowacki M, Kolban M, Snela S, Sliwinski Z, Kowalski IM, SOSORT. Conservative management of idiopathic scoliosis- guidelines based on SOSORT 2006 consensus. Ortopedia Traumatologia Rehabilitacja. 2009;11(5):379–95.
Lonstein JE, Carlson JM. The prediction of curve progression in untreated idiopathic scoliosis during growth. J Bone Joint Surg. 1984;66:1061–71.
Korovessis P, Zacharatos S, Koureas G, Megas P. Comparative multifactorial analysis of the effects of idiopathic adolescent scoliosis and Scheuermann kyphosis on the self-perceived health status of adolescents treated with brace. Eur Spine J. 2007;16(4):537–46.
Acknowledgements
I would like to thank my instructors in BSPTS-Schroth method, Dr Manuel Rigo and Beth Janssen, especially Beth for correcting my English, and the SOSORT board for giving me the chance to present my research in the SOSORT meeting in Katowice.
Declarations
This article has been published as part of Scoliosis and Spinal Disorders Volume 11 Supplement 2, 2016. Research into Conservative Management of Spinal Deformities: Short Articles from the SOSORT 2015 Meeting. The full contents of the supplement are available online http://scoliosisjournal.biomedcentral.com/articles/supplements/volume-11-supplement-2.
Availability of data and materials
All data and materials that were used in the results for this study are already present in this paper. There is no restriction for their distribution and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source.
Authors’ contributions
NK carried out the data collection, the variables assessment and the interpretation of the results.
Competing interests
The author declares that he has no competing interests.
Consent for publication
Written consent was obtained from the parents of the patients for publication of the figures.
Ethics approval and consent to participate
The methods used for the present research were in compliance with the Helsinki Declaration.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Karavidas, N.S. Bracing for Adolescent Idiopathic Scoliosis (AIS) and Scheuermann Kyphosis: the issue of overtreatment in Greece. Scoliosis 11 (Suppl 2), 30 (2016). https://doi.org/10.1186/s13013-016-0095-6
Published:
DOI: https://doi.org/10.1186/s13013-016-0095-6