
Abstract
Background
Clinical guidelines recommend that assessment and management of patients with stroke commences early including in emergency departments (ED). To inform the development of an implementation intervention targeted in ED, we conducted a systematic review of qualitative and quantitative studies to identify relevant barriers and enablers to six key clinical behaviours in acute stroke care: appropriate triage, thrombolysis administration, monitoring and management of temperature, blood glucose levels, and of swallowing difficulties and transfer of stroke patients in ED.
Methods
Studies of any design, conducted in ED, where barriers or enablers based on primary data were identified for one or more of these six clinical behaviours. Major biomedical databases (CINAHL, OVID SP EMBASE, OVID SP MEDLINE) were searched using comprehensive search strategies. The barriers and enablers were categorised using the theoretical domains framework (TDF). The behaviour change technique (BCT) that best aligned to the strategy each enabler represented was selected for each of the reported enablers using a standard taxonomy.
Results
Five qualitative studies and four surveys out of the 44 studies identified met the selection criteria. The majority of barriers reported corresponded with the TDF domains of “environmental, context and resources” (such as stressful working conditions or lack of resources) and “knowledge” (such as lack of guideline awareness or familiarity). The majority of enablers corresponded with the domains of “knowledge” (such as education for physicians on the calculated risk of haemorrhage following intravenous thrombolysis [tPA]) and “skills” (such as providing opportunity to treat stroke cases of varying complexity). The total number of BCTs assigned was 18. The BCTs most frequently assigned to the reported enablers were “focus on past success” and “information about health consequences.”
Conclusions
Barriers and enablers for the delivery of key evidence-based protocols in an emergency setting have been identified and interpreted within a relevant theoretical framework. This new knowledge has since been used to select specific BCTs to implement evidence-based care in an ED setting. It is recommended that findings from similar future reviews adopt a similar theoretical approach. In particular, the use of existing matrices to assist the selection of relevant BCTs.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Clinical guidelines recommend that the assessment and management of patients with stroke should commence early in the pre-hospital setting and hospital emergency department (ED) [1]. Despite the recent advances in interventions for the management of acute stroke, only a small proportion of individuals receive recommended evidence-based treatment in the hours following acute stroke [1, 2]. For example, thrombolysis using intravenous tissue plasminogen activator (tPA) is currently one of the few evidence-based treatments available for acute ischaemic stroke, however, internationally rates are variable, ranging from 5% in the USA [3] to 14% in some European Centres [4]. Furthermore, outcomes are improved by early administration (within hours) of tPA after symptom onset. However, in-hospital delays are often a significant obstacle in achieving early administration of tPA [5].
Determining the inhibiting factors (barriers) and supporting factors (enablers) for implementation of research evidence, is a well-established requirement to improve the quality of patient care [6]. It has been demonstrated that a theoretical approach to assessing barriers and enablers can effectively be used for developing tailored informed strategies to support the effective implementation of evidence-based practices, such as hand hygiene [7]. Systematic reviews offer a way to synthesise the broad range of barriers and enablers reported in individual studies and provide a broader understanding of the influences on evidence-based treatment uptake. Findings from such reviews can be used to inform the development of effective interventions to implement evidence-based care in clinical settings.
In stroke, systematic reviews have been conducted to identify barriers and enablers to implementing elements of stroke guidelines. These have usually been studied at an organisational level and have included pre-admission barriers such as non-recognition of stroke [8], triaging of stroke as non-urgent by both ED and ambulance staff [8, 9], delays in accessing imaging [8] and inefficient hospital processes and protocols [8, 9]. Data included in these reviews were based on retrospective analyses of hospital databases [5, 10] national registries [11], or prospective cohort data. The main limitation of these reviews is that the barriers and/or enablers were based on the authors’ perceptions or explanations rather than based on healthcare staffs’ perceptions or beliefs.
Recently, within the implementation science literature there has been increasing importance placed on the development of behaviour change interventions [12, 13] using theoretical models or frameworks such as the Theoretical Domains Framework (TDF) [14]. The use of theory is important to understand the factors that influence healthcare professionals’ behaviours, to inform the use of possible behaviour change techniques (BCTs) and to provide clarity as to how these techniques might work [15, 16]. Interventions are said to be more effective if interventions are based on evidence-based principles drawn from theories of behaviour and behaviour change [17].
The TDF is a framework of originally 12 domains [14] (now 14 domains [18]). The theoretical domains were derived from 33 behaviour change theories and developed using a process of expert consensus with subsequent validation work. To facilitate the application of BCT taxonomy and to assist the selection of relevant BCTs a matrix has been developed which is based on identifying links between specific BCTs and theoretical constructs such as those used in the TDF [19]. The TDF has been used in a number of healthcare settings to study implementation and more specifically assist in the development of implementation interventions [16]. The TDF has also been used as a coding framework for the analysis of barriers in systematic reviews [20–22]. In one study the TDF allowed the researchers to explore, explain and potentially target, using sophisticated behaviour change interventions, complex relationships, for example, limited “knowledge” appeared to influence healthcare professional’s ‘emotions’ [21].
In the Quality in Acute Stroke Care Study (QASC) the investigators demonstrated significant benefits for patients who were cared for in acute stroke units (ASU) in which staff had received support for implementation of protocols to manage fever, hyperglycaemia, and swallowing dysfunction [23]. The QASC trialists recommended future trials to examine the multidisciplinary intervention in other settings, such as the ED, to ensure patients had rapid access to these evidence-based protocols [23]. Prior to the development of an implementation intervention to deliver such evidence-based protocols, we undertook a systematic review of qualitative and quantitative studies to identify the barriers and enablers specific to an ED setting. The findings from this systematic review will inform the use of specific BCTs to develop an implementation intervention.
Aim
The aims of this systematic review were to:
-
Identify the reported barriers and enablers to implementing the following evidence-based care elements (hereonin referred to as target clinical behaviours): appropriate triage, thrombolysis administration, monitoring and management of temperature, blood glucose levels, and of swallowing difficulties and rapid (within 4 h of arrival to ED) transfer to the ASU
-
Classify reported barriers and facilitators using the TDF
-
Select the BCT that best aligned to the strategy each enabler represented using standard taxonomy
Methods
Inclusion and exclusion criteria
Studies were eligible for inclusion, regardless of design, if the study:
-
Aim was to identify the barriers and/or enablers for any one or a combination of the target clinical behaviours in the ED of a hospital (Table 1) and
-
Included the views/perceptions of healthcare professionals regarding the target behaviours who worked in ED.
Abstracts, letters, editorials, and commentaries were excluded. No restrictions were placed on country, written language, or year of publication.
Search methods for identification of studies
The search strategy was developed using search concepts (groups of words; Appendix). Potentially relevant studies were identified through a search (inception to August 2016) of the following electronic databases: CINAHL, OVID SP EMBASE, OVID SP MEDLINE, and Web of Science. Other databases that were searched included: OVID SP PubMed Central; The Joanna Briggs Institute EBP; Database ProQuest Dissertations & Theses Full Text. The following grey literature databases also were searched: Agency for Healthcare Research and Quality (AHRQ); Open Grey and Grey Literature Report.
The Science Citation Index (Web of Science) was searched to identify further studies that had cited the studies included in the review. Reference lists of included publications were searched to identify additional studies.
Search strategy
The search strategy applied to the databases was a combination of Medical Subject Headings (MeSH) terms such as: “Health Plan Implementation” and “Evidence-Based Practice”, as well as additional keywords such as “barrier”, “uptake,” and “enabler”, and relevant synonyms. The MeSH terms and keywords were generated for each of the search concepts by examining the terminology and database indexing used in relevant papers. The search strategies were reviewed by a University Librarian with experience in database searches, prior to the search being undertaken.
Screening process
The titles and abstracts of retrieved references from the search were screened by a single reviewer to exclude obviously irrelevant studies. The full article of any study that met the inclusion criteria was reviewed by at least two of the authors (EM, LC, or SM).
Data extraction
Data were extracted using a standardised form by one reviewer (LC), with a sub-set of included papers (n = 15 [30%]) being extracted by a second reviewer (EM or SM). Data collection included full study characteristics such as author, date of publication, study design and the reported study findings, i.e., barriers and/or enablers. Barriers and/or enablers based on primary data were extracted using theme headings and theme descriptions in qualitative studies and extracted from tables presenting questionnaire responses to pre-specified barriers and/or enablers in the quantitative studies (Table 2). Six of the nine included studies [24–29] focused on one target behaviour which was easily identifiable from the title on screening and the aim and method sections on data extraction. The remaining three studies [30–32] focused on stroke pathways or key stroke care recommendations whereby the target behaviours of interest were identified in the methods and results sections of the individual studies. If the lead author was unclear which target behaviour the data represented this was cross-checked and discussed with another author (SM or EM). Authors of included studies did not distinguish between modifiable and non-modifiable barriers/enablers.
Qualitative studies
Verbatim supporting quotes, where available, were extracted to illustrate the barriers and enablers. Author interpretations or findings from secondary analysis of routine data were not included.
Quantitative studies
To ensure that the review presented findings that were representative and important, certain decisions were made about the data extraction for the survey data. Pre-specified barriers where zero or only one of the participants selected were not extracted [26, 29]. A decision was made to extract only the pre-specified barriers where the majority of participants agreed (>50%) for one study [25] and a further decision was made to extract pre-specified barriers which scored a level of agreement >3 (1 = fully disagree; 5 = fully agree) for the remaining survey [32].
Quality assessment
Quality assessment of qualitative studies was conducted using the Critical Appraisal Skills Programme Qualitative Checklist (CASP) [33]. For the assessment of quantitative studies the Centre for Evidence-Based Management “Appraisal of a Survey” tool was used [34]. Critical appraisal was conducted by one reviewer (LC) for all studies, with second reviewer appraisal (EM or SM) for a sub-set of included papers (the same sub-set subject to second reviewer data extraction). The findings from the two reviewers were compared and any contrasting items were discussed and re-reviewed to reach an agreement.
Data analysis
The extracted data were classified using the TDF [18]. Classification of barriers and enabler data was conducted independently by two researchers experienced in the application of the TDF (LC and NT). Reference was made to the original article regarding the development of the TDF to ensure accurate interpretation of the domains [14]. The TDF constructs [18] and contextual information reported for an individual barrier/enabler were also used to allocate the data to the most appropriate domain. Using the descriptors of each TDF domain, the individual barriers and enablers were classified accordingly. There were two disagreements between the two researchers resulting in the re-classification of two barriers, one from the beliefs about capabilities domain to the social influences domain and the other from the beliefs about capabilities domain to the intentions domain. The TDF was used as a relevant framework to narratively summarise the individual barriers under the relevant theoretical domains; but no thematic synthesis was conducted to identify themes.
Allocating BCT labels to reported enablers
A matrix which assigns the most appropriate BCT to each of the TDF domains has already been developed by Cane et al. [35]. Primarily, this resource has been used in the past to develop behaviour change interventions to address identified key barriers. However, the studies included in our review did not report strategies to overcome specific barriers, so BCTs could not be assigned. However, the enablers reported in each study were able to be aligned with BCTs listed in the Cane matrix, as each reported enabler essentially represented a strategy to promote behaviour. The BCT that best aligned to the enabling strategy was then selected for each of the reported enablers using this matrix [36]. The assignment of BCTs to enablers was independently conducted by two researchers. Both researchers then discussed the allocations collectively and resolved any disagreements by discussion. This approach to classifying enablers to BCT enhances reporting as it provides a standardised label for the reported enabler using a common BCT taxonomy and subsequently increases the transferability of the findings.
Results
The search identified 2114 studies. Following the initial screening of titles and abstracts, duplicate and irrelevant studies were excluded, and the full-text articles of 44 studies were assessed in detail (Fig. 1). One further article was identified through citation searching. No further articles were identified from reviewing the reference lists of the included studies. Overall, nine studies met the selection criteria and were included in the review [24–32].

Search flow
Study characteristics
Table 2 shows the characteristics of the nine studies which were all published between 2004 and 2015. Five studies were qualitative with one using focus group methods [31] and four using semi-structured interviews [24, 27, 28, 30]. The remaining four studies used a survey method, of which two used an online questionnaire [25, 26]. The sample sizes ranged from 8 to 429 healthcare professionals. Four studies were conducted in the USA, two in Australia, one in Sweden, one in the Netherlands, and one in France. Sampling strategies to recruit participants varied. In five studies a convenience sample was used [24, 25, 29, 31, 32] and in four studies a purposive sampling strategy was used [26–28, 30].
In one study, barriers and enablers relating to the triage behaviour were identified [31]. In four studies, barriers and enablers relating to the tPA related behaviours were reported [25, 27–29]. One study only reported barriers (i.e. no enablers) to the tPA related behaviours [26] and one study reported the barriers for both the tPA and transfer related behaviours [32]. In another study, the barriers and enablers relating to both the tPA and the triage related behaviours were reported [30]. Lastly, barriers and enablers to the swallow assessment behavior were reported in a single study [24]. None of the included studies provided evidence on the barriers and enablers for behaviours relating to management of fever, or for the management of blood glucose levels.
Quality of the included studies
The common limitations within the qualitative studies were: no or little information about the relationship between the researcher and participants [24, 27, 28, 30, 31], and a lack of data describing and justifying the approach for analysis [24, 28, 31]. Generally, the strengths of the studies were clearly stated aims, appropriate use of methods and a clear statement of findings (Table 3).
With regard to the quality of the quantitative research (Table 4), the low response rates (13–55%) limits the potential generalisability of these studies. All of these studies had a clearly defined research question.
Participant characteristics
The nine included studies provided data from 590 healthcare professionals working in a hospital ED. In two studies, the mean age of participants was reported (41.1 years [25] and 33.9 years [31]). Out of the four studies where the sex of participants was provided, the percentages that were female ranged from 13.5% [32] to 100% [31]. The type of participants were all nurses in two studies [24, 31], physicians and nurses in the remaining seven studies, of which four of these included participation by other disciplines such as social workers or pharmacists [25–27, 30]. The length of experience working in the ED was reported in two studies and ranged from the majority of participants having worked in ED over 10 years [25] and between 1 month and less than 17 months [30].
Domains of the TDF as represented by the reported barriers and enablers
A summary of barriers and enablers by TDF domain as identified in each of the included studies is provided in Table 5. The review identified 51 barriers and 40 enablers relevant to the target clinical behaviours. The number of barriers and number of enablers reported for triage behaviour were nine and one, respectively. The number of barriers and number of enablers reported for the thrombolysis related behaviours were 21 and 36, respectively. The number of barriers and number of enablers reported for swallow assessment behaviour were four and three, respectively. Only one barrier was reported for transfer-related behaviours.
Knowledge
Barrier and enabler data were available relating to triage and tPA-related behaviours. Both studies investigating triage reported “stroke was not being recognised as a priority” as a barrier [30, 31]. All three studies for the tPA-related behaviours identified barriers associated with lack of knowledge including guideline unfamiliarity [27], awareness [27], or failure to react to deviations in guidelines [28]. The barriers identified by Williams et al. related more to procedural knowledge such as uncertainty with respect to the patient selection criteria for tPA [29]. More specifically, in one study staff (ED nurses and pharmacists) reported that physicians wait until towards the end of the tPA treatment time window to see whether patients’ symptoms improve before committing to tPA, thus delaying time to tPA treatment and potentially lowering tPA treatment rates [26]. Education to provide knowledge about how to offer tPA [27], identification of stroke [25] and interpretation of brain imaging scans was reported as an enabler [25]. Correspondingly, lack of education on symptoms of stroke, tPA use, and lack of pathways and protocols were reported as significant barriers by Williams et al. [29]. More education around dysphagia and evidence-based screening of swallowing post stroke was identified as an enabler by the only study investigating the swallow care behaviours [24].
Skills
Lack of skills was reported in relation to the triage, tPA and swallow care behaviours, but not for the transfer behaviours. Staff reported that a lack of practice and skills development were barriers to administrating tPA, particularly with regards to interpretation of computed tomography scans, clinical diagnostic uncertainty and individual experience in stroke neurology [29]. In one study, the administration and inaccurate interpretation of swallow screening items were reported [24].
Social/professional role and Identity
Social/professional role and identity related issues were reported for the triage and the tPA-related behaviours. A lack of a dedicated nurse to manage stroke patients was reported in one study [26]. Limited social identity, i.e., insufficient recognition by peers and decision makers were barriers to delivering the tPA-related behaviours [28].
Beliefs about capabilities
Data relating to beliefs about capabilities were only reported for the tPA-related behaviours. Barriers relating to this domain included a lack of self-efficacy and motivation [27]. A number of similar enablers, were found in two studies and included experience and exposure of “telemedicine and stroke code protocols”, which were focused on improving physician’s ability to confidently diagnose stroke patients eligible for tPA treatment [29]. Similarly, Grady et al. reported that the majority of survey participants believed that being able to “confidently interpret brain imaging scans” was an enabling factor [25].
Optimism
Data were only reported for the tPA-related behaviours and relevant enablers reported by staff included positive staff attitudes within and outside the stroke unit [28].
Beliefs about consequences
Data were only reported for tPA-related behaviours. In three studies staff beliefs indicated belief in a lack of positive outcome for patients after tPA [27–29] including that staff held “old-fashioned views” about the lack of benefit of tPA for improving outcomes after stroke [28]. Reluctance of staff to administer tPA was reported (participants were ED nurses and ED pharmacists) in one study as a barrier and this was likely to be due to poorly understood beliefs about the benefits of using tPA [26].
Intentions
Data were only reported for the tPA related care elements. Lack of motivation was the only barrier reported which related to this TDF domain [27].
Memory, attention, and decision process
Data were only reported for the swallow assessment behaviours. The only factor relating to this domain was staff reporting difficulty recalling all screening items during administration of a swallow screen [24].
Environmental context and resources
All care elements apart from the management of blood glucose levels and the management of fever had information reported on environmental context and resources. Working with a busy environment with competing demands was a frequently reported barrier for the appropriate triage of patients with stroke. Barriers were largely related to delays and were often categorised as pre-hospital clinical care, in-hospital clinical care and/or administrative to the successful assessment for and delivery of tPA [26, 29]. Communication between departments was believed to play a pivotal role in the success of delivering tPA [26]. Financial resources were reported as a potential barrier in one study, without further specification [31], but in another, no respondents rated cost as a significant barrier [28]. Stecksen et al. identified stressful working conditions, limited time, and lack of continuity as other barriers to assessing patients for suitability for tPA and delivering tPA treatment [28]. In relation to rapid transfer of stroke patients from the ED to the stroke unit, the two barriers reported related to poor patient flow to the appropriate ward [32]. A stroke protocol was the only enabler that was reported in relation to facilitating appropriate triage [31], and similarly, efficient processes was one of the three enabling factors reported to assist in the implementation of a swallow screen tool [24].
Social influences
Social influences were reported in relation to the swallow and tPA related behaviours. A lack of support was reported as a barrier in two studies in relation to the tPA elements [28, 29]. Enablers associated with social influences included sharing of experiences amongst staff [28], the endorsement of the use of tPA [25], and advice from a senior colleague [25]. Social support provided from administrators and the wider multidisciplinary team was perceived by nurses as factors which would assist the uptake of swallow screening practices in ED [24].
Behaviour regulation
Data were only reported for the tPA-related behaviours. One reported enabler relevant to this domain was initiation of an assurance mechanism with continuous feedback on success or otherwise of implementation [28].
No authors attempted to interpret the data using an existing behaviour change theory, framework, or model. A purposefully developed taxonomy was used in one study to classify barriers [27], whilst in one other study enablers were classified into behaviour change domains; however, the framework, model or theory that underpinned these domains was not disclosed [25]. A summary of the TDF domains as represented by the barriers and enablers reported in the studies is shown in Table 6.
The allocation of BCT labels to reported enablers
The total number of BCTs assigned was 18. The BCTs most frequently assigned to the reported enablers were ‘focus on past success’ (n = 8) and ‘information about health consequences’ (n = 5). There were three occasions where more than one technique was considered to align with a reported enabler. No technique was aligned with the reported enabler “positive staff attitudes, within and outside the stroke unit” as the underlying meaning was not clear and no other contextual data was provided in the study. The aligning behaviour change techniques for each reported enabler are provided in Table 5.
Discussion
This study produced new knowledge on the barriers and enablers for the delivery of key evidence-based protocols in an emergency setting and interpreted within a relevant theoretical framework. Barriers and/or enablers were identified for triage, thrombolysis, swallow assessment and patient transfer related clinical behaviours. Barriers relating the environmental context and resources domain such as a lack of time, stressful working conditions and ED delays were common to all four behaviours. Barriers relating to the skills domain such as inconsistent administration of swallow screen tools, and to the memory, attention, and decision processes domain such as difficulty recalling screening items during administration were relevant to only one clinical behaviour. There were no studies which identified barriers or enablers with regards to two of the six target behaviours: monitoring and management of (1) temperature and (2) blood glucose levels. There were no barriers or enablers derived from the systematic review findings that could not be accounted for by one of the TDF domains, indicating that this framework is highly relevant to behaviour change within this clinical context.
The use of the TDF has allowed the comprehensive identification of barriers and enablers for areas such as these where existing evidence is lacking. This process has identified several domains of the TDF where no primary barriers or enablers were identified in the included studies: reinforcement, goals, and emotion. As significant emotional issues such as excessive fear of harm and complications have been identified in other literature [37, 38] regarding thrombolysis in stroke, this emphasises that there remain gaps the published literature where barriers and enablers have not been reported. Evidence suggests that individuals find it more difficult to verbalise their affective attitudes (i.e., emotions) [39]. The TDF has been found to elicit emotion related barriers to behaviour change more effectively than a-theoretical approaches to identifying barriers [7].
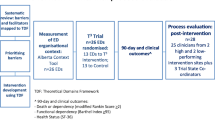
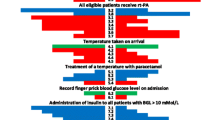
Interestingly, only one included study subsequently used the data from a barrier and enabler assessment to develop an implementation intervention (a dysphagia screening bundle) [24]. The evaluation revealed that swallowing screening practices significantly improved after the implementation of this bundle; however, the author did not state whether this could be attributed to the information yielded by the barrier assessment. Indeed, the findings from this systematic review have since been used to inform the development of an implementation intervention for an ongoing trial (the T3 trial) to target these clinical behaviours in an ED setting. The T3 trial investigators aim to evaluate the supported implementation of key best practice acute stroke care clinical elements relating to the appropriate triage, treatment with tPA, management and monitoring of blood glucose levels, temperature and of swallowing difficulties, and transfer from ED to the ASU.
Although barriers and enablers are often hypothesised to be determinants of behaviour, their actual influence on performing a certain practice has been questioned as other contextual factors may play more significant roles [40]. The large number of barriers and enablers within the environmental context and resources domain highlight the importance of health system environments. A broader health systems approach has been used to investigate the association between health system factors such as urban location and tPA treatment rates [41]. Paul et al. concluded that to improve tPA treatment rates, specific health system factors need to be targeted.
Limitations
There were few studies that met the inclusion criteria for this review included in this review, most likely due to the limited published literature in this field. Due to the limitation of subject headings for the terms “barriers” and “enablers,” electronic indexing synonyms were used for key words to ensure the search was sensitive; however, this may have compromised the precision of the search and as for other reviews of barriers and enablers in healthcare there is potential for studies not to be identified [42]. The quality of the included studies was comprised by small sample sizes for the quantitative studies and the limited reporting and/or lack of robust sampling techniques. The different approaches used to analyse the qualitative and quantitative data within the included studies posed challenges for data extraction. For example, some of the studies referred to stroke care in general, making it difficult to ascertain which barriers related to each of the target clinical behaviours. The use of the TDF for secondary analysis required some subjective interpretation due to the lack of contextual detail reported for some of the barriers and enablers. This limitation has been reported by other authors [21]. No included study used a behaviour change theory, standard taxonomy, or framework to interpret findings.
Researchers have reported that barriers can be represented by more than one domain and have also acknowledged the complex relationship between domains [21]. In this study this was evident when attempting to interpret and map the barriers to the framework with often limited contextual information. For example, “inaccurate interpretation of screening items” in performing a swallow screen was mapped to skills as the primary TDF domain but may also be related to the TDF domain memory, attention, decision processes. In this study, we agreed and reported the primary domain only. Further, research is required to guide how best to select a theoretical domain in these instances, e.g., what process should be taken to identify which of two (or more) domains primarily represents a specific barrier.
There were instances whereby the BCT used in the enabling strategy reported in the included studies did not align with the BCTs that the Cane et al. matrix recommends for use to target domains. For example, the BCTs used in the enabling strategies (habit formation; feedback on outcome of behaviour; feedback on behaviour) for the behavioural regulation domain do not align with the BCT recommended by the Cane et al. matrix (self-monitoring of behaviour). This indicates that Cane et al. matrix is a useful, but not comprehensive tool to identify appropriate enabling strategies. It is likely that the discrepancies are due to individual contextual factors, not accounted for by the matrix; highlighting the ongoing importance of local barrier and enabler assessments for any implementation strategy.
Strengths
Both qualitative and quantitative primary studies were focused on capturing barriers and enablers as reported by healthcare professionals. This provides novel data in comparison to existing reviews in this area which often relied on observational or registry data to characterise barriers, i.e., investigate causes or consequences of pre-determined factors such as in-hospital delays. The review processes used were robust and transparent adhering to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standard. The search strategy underwent extensive review and iteration to ensure efficiency and accuracy in the conduct and output of the search. The data collection process was conducted in duplicate and decisions were cross-checked with another researcher.
The use of the TDF in systematic reviews is an emerging methodology and has only been applied in a few recent studies. The assignment of BCTs to barriers was not conducted as part of this review as the information was not available in the individual studies. However, one potential application of the barrier data is to select; using a panel of experts for example, the most appropriate behaviour change techniques to address the barriers to further inform the T3 trial implementation intervention development. For example, one of the BCTs recommended by the mapping conducted by Cane et al. [18] to overcome barriers classified within the skills domain is behavioural practice/rehearsal [35]. The enabler data from this review could then be applied to inform how this technique can be feasibly employed in clinical practice. For example, the enabler “giving physicians the opportunity to treat stroke cases of varying complexity” could be viewed as a deliverable form of this technique. This approach has been successfully used to develop an implementation intervention to improve the management of traumatic brain injury in the ED [43]. Furthermore, classifying the enablers to the best aligning BCT enhances the reportability and transferability of findings in this process.
Area of future research
The authors of one survey presented and analysed the data by decision makers and non-decision makers and revealed significant difference between the two groups [25]. Therefore, it may be important to further identify and explore the differences and similarities in perceptions between different disciplines, especially when implementing a multidisciplinary intervention. It would be worthy to further investigate whether the barriers identified by the review could be feasibly addressed, possibly by devising a panel of experts to make this judgment. If the barrier is deemed non-modifiable, then it is not likely to be a feasible target for an implementation intervention. The monitoring of barrier status during the implementation of an intervention would provide evidence for the types of barriers that can easily be overcome, the type of barriers which may be intractable and the effectiveness of particular BCT directed at barriers/enablers within various theoretical domains. Currently, mapping of BCTs to the TDF domains is largely based on expert opinion and a more robust higher level of evidence is required. There also needs to be more illustrations of how barrier and/or enabler data has been used to develop implementation interventions. Consistent use of a theoretical framework will assist with progressing this work by enabling meaningful compilation of evidence from a variety of sources. In addition, none of the studies reported monitoring the status of barriers over time or conducted a pre-and post implementation barrier assessment. Such design would add significant weight to the evidence regarding the value of barrier and enabler assessment, and subsequent use to target interventions.
Gaining patient’s and family member’s perceptions of stroke care in the ED were not considered by any of the studies and in the context of shared-decision making is an area that warrants further research. Patient and family preferences for and against practices such as tPA [44] and “nil by mouth” [45] has the potential to impact on the implementation of certain practices.
Conclusion
Barriers and/or enablers have been identified for the majority of the target clinical behaviours which could be used to inform barrier and enabler assessments in similar acute settings. Due to the likely gaps in the evidence base, barrier, and enabler data for some of the clinical behaviours and within some of the theoretical domains, could not be identified. The novel assignment of BCT labels to reported enablers will allow researchers and clinicians to use and potentially modify these techniques to deliver these important clinical behaviours in routine practice. When considering the findings from reviews of barriers and enablers, it is recommended that a reporting framework as illustrated in this paper should be adopted. This would facilitate the comparison, contrasting, and synthesis of barrier and/or enabler data within a consistent context framework and facilitate recognition identification of proven strategies to address such barriers [19].
Abbreviations
- ASU:
-
Acute stroke unit
- ED:
-
Emergency Departments
- T3:
-
Triage, Treatment and transfer
- TDF:
-
Theoretical domains framework
- tPA:
-
Thrombolysis
References
National Stroke Foundation. Clinical Guideline for Stroke Management. 2010.
American Heart Association. Get With The Guidelines®-Stroke Overview. http://www.heart.org/HEARTORG/HealthcareResearch/GetWithTheGuidelines/Get-With-The-Guidelines-Stroke_UCM_306098_SubHomePage.jsp#. Last accessed 15 Dec 2015
American Heart Association. FACTS. Preventable. Treatable. Beatable: Stroke in the United States. USA: AHA; 2013.
Royal College of Physicians. Clinical Effectiveness and Evaluation Unit on behalf of the Intercollegiate Stroke Working Party. Clinical Audit Jan- March. UK: Sentinel Stroke National Audit Programme (SSNAP); 2014.
Romano JG, Muller N, Merino JG, Forteza AM, Koch S, Rabinstein AA. In-hospital delays to stroke tPA: paradoxical effect of early arrival. Neurol Res. 2007; doi: http://dx.doi.org/10.1179/016164107X240035
Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients’ care. Lancet. 2003;362:1225–30.
Dyson J, Lawton R, Jackson C, Cheater F. Development of a theory-based instrument to identify barriers and levers to best hand hygiene practice among healthcare practitioners. Implement Sci. 2013;8:111.
Carter-Jones CR. Stroke tPA: Barriers to implementation. Int Emerg Nurs. 2011; doi: http://dx.doi.org/10.1016/j.ienj.2010.02.005
Eissa A, Krass I, Bajorek BV. Barriers to the utilization of thrombolysis for acute ischaemic stroke. J Clin Pharm Ther. 2012;37(4):399–409. doi:http://dx.doi.org/10.1111/j.1365-2710.2011.01329.x.
Szoeke CE, Parsons MW, Butcher KS, Baird TA, Mitchell PJ, Fox SE, et al. Acute stroke tPA with intravenous tissue plasminogen activator in an Australian tertiary hospital. Med J Aust. 2003;178:324–8.
Lau AYL, Soo YOY, Graham CA, Woo WK, Wong EHC, Leung H, et al. An expedited stroke triage pathway: The key to shortening the door-to-needle time in delivery of tPA. Hong Kong Med. 2010;16:455–62.
Improved Clinical Effectiveness through Behavioural Research G. Designing theoretically-informed implementation interventions. Implement Sci. 2006;1:4. doi:10.1186/1748-5908-1-4.
Eccles M, Grimshaw J, Walker A, Johnston M, Pitts N. Changing the behavior of healthcare professionals: the use of theory in promoting the uptake of research findings. J Clin Epidemiol. 2005;58(2):107–12.
Michie S, Johnston M, Abraham C, Lawton R, Parker D, Walker A, et al. Making psychological theory useful for implementing evidence based practice: a consensus approach. Qual Saf Health Care. 2005;14(1):26–33.
Medical Research Council. A framework for development and evaluation of RCTs for Complex Interventions to improve Health. 2000. Available from: http://www.mrc.ac.uk
French SD, Green SE, O’Connor DA, McKenzie JE, Francis JJ, Michie S, et al. Developing theory-informed behaviour change interventions to implement evidence into practice: a systematic approach using the Theoretical Domains Framework. Implement Sci. 2012;7:38.
Taylor N, Conner M, Lawton R. The impact of theory on the effectiveness of worksite physical activity interventions: a meta-analysis and meta-regression. Health Psychology Review. 2012;6(1):33–73. doi:10.1080/17437199.2010.533441.
Cane J, O’Connor D, Michie S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci. 2012;7(1):37.
Michie S, Johnston M, Francis J, Hardeman W, Eccles M. From theory to intervention: mapping theoretically derived behavioural determinants to behaviour change techniques. Appl Psychol. 2008;57(4):660–80. doi:10.1111/j.1464-0597.2008.00341.x.
Wilkinson SA, McCray S, Beckmann M, Parry A, McIntyre HD. Barriers and enablers to translating gestational diabetes guidelines into practice. Practical Diabetes. 2014;31(2):67–72a. doi:10.1002/pdi.1833.
Heslehurst N, Newham J, Maniatopoulos G, Fleetwood C, Robalino S, Rankin J. Implementation of pregnancy weight management and obesity guidelines: a meta-synthesis of healthcare professionals’ barriers and facilitators using the Theoretical Domains Framework. Obes Rev. 2014;15(6):462–86. doi:10.1111/obr.12160.
Lipworth W, Taylor N, Braithwaite J. Can the theoretical domains framework account for the implementation of clinical quality interventions? BMC Health Serv Res. 2013;13(1):1–13. doi:10.1186/1472-6963-13-530.
Middleton S, Levi CR, D’Este C, Grimshaw J, Cadilhac DA, Considine J, et al. T3 Trial protocol: A CRCT evaluating an organisational intervention to improve triage, treatment and transfer of stroke patients in EDs. Int J Stroke. 2013;8(S1):10.
Daniels SK, Anderson JA, Petersen NJ. Implementation of stroke dysphagia screening in the emergency department. Nursing Research and Practice. 2013. doi:10.1155/2013/304190.
Grady A, Bryant J, Carey M, Paul C, Sanson-Fisher R. Enablers of the implementation of tissue plasminogen activator in acute stroke care: a cross-sectional survey. PLoS ONE. 2014; doi: http://dx.doi.org/10.1371/journal.pone.0114778
Hargis M, Shah JN, Mazabob J, Rao CV, Suarez JI, Bershad EM. Barriers to administering intravenous tissue plasminogen activator (tPA) for acute ischemic stroke in the emergency department: a cross-sectional survey of stroke centers. Clin Neurol Neurosurg. 2015;135:79–84. doi: http://dx.doi.org/10.1016/j.clineuro.2015.04.027.
Meurer WJ, Majersik JJ, Frederiksen SM, Kade AM, Sandretto AM, Scott PA. Provider perceptions of barriers to the emergency use of tPA for acute ischemic stroke: a qualitative study. BMC Emerg. 2011; doi: http://dx.doi.org/10.1186/1471-227X-11-5
Stecksén A, Lundman B, Eriksson M, Glader E-L, Asplund K. Implementing thrombolytic guidelines in stroke care: perceived facilitators and barriers. Qual Health Res. 2014. doi:10.1177/1049732313514137.
Williams JM, Jude MR, Levi CR. Recombinant tissue plasminogen activator (rt-PA) utilisation by rural clinicians in acute ischaemic stroke: a survey of barriers and enablers. Aust J Rural Health. 2013; doi: http://dx.doi.org/10.1111/ajr.12052
Gache K, Leleu H, Nitenberg G, Woimant F, Ferrua M, Minvielle E. Main barriers to effective implementation of stroke care pathways in France: a qualitative study. BMC Health Serv Res. 2014;14:95.
Johnson M, Cohn J, Bakas T. Emergency department nurses’ perceived barriers and facilitators to caring for stroke patients. J Neurosci Nurs. 2011;43(5):238–43.
Van Der Weijden T, Hooi JD, Grol R, Limburg M. A multidisciplinary guideline for the acute phase of stroke: barriers perceived by Dutch neurologists. J Eval Clin Pract. 2004;10:241–6.
Critical Appraisal Skills Programme(CASP).CASP Qualitative Checklist. http://media.wix.com/ugd/dded87_29c5b002d99342f788c6ac670e49f274.pdf. Accessed 15 Dec 2015
Center for Evidence-based Management (CEBMa). Critical Appraisal of a Survey. http://www.cebma.org/wp-content/uploads/Critical-Appraisal-Questions-for-a-Survey.pdf. Accesssed 15 Dec 2015
Cane J, Richardson M, Johnston M, Ladha R, Michie S. From lists of behaviour change techniques (BCTs) to structured hierarchies: comparison of two methods of developing a hierarchy of BCTs. Br J Health Psychol. 2015;20(1):130–50. doi:10.1111/bjhp.12102.
Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013;46(1):81–95. doi:10.1007/s12160-013-9486-6.
Caplan LR. Stroke thrombolysis: slow progress. Circulation. 2006;114(3):187–90. doi:10.1161/circulationaha.106.638973.
Goldstein JN, Marrero M, Masrur S, Pervez M, Barrocas AM, Abdullah A, et al. Management of thrombolysis-associated symptomatic intracerebral hemorrhage. Arch Neurol. 2010;67(8):965–9. doi:10.1001/archneurol.2010.175.
Wilson TD, Dunn DS. Effects of introspection on attitude-behavior consistency: analyzing reasons versus focusing on feelings. J Exp Soc Psychol. 1986;22(3):249–63.
Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci. 2015;10:53. doi:10.1186/s13012-015-0242-0.
Paul CL, Ryan A, Rose S, Attia JR, Kerr E, Koller C, et al. How can we improve stroke thrombolysis rates? A review of health system factors and approaches associated with thrombolysis administration rates in acute stroke care. Implement Sci. 2016;11(1):1–12. doi:10.1186/s13012-016-0414-6.
Duncan E, Murray J. The barriers and facilitators to routine outcome measurement by allied health professionals in practice: a systematic review. BMC Health Serv Res. 2012;12(1):96.
Tavender EJ, Bosch M, Gruen RL, Green SE, Michie S, Brennan SE, et al. Developing a targeted, theory-informed implementation intervention using two theoretical frameworks to address health professional and organisational factors: a case study to improve the management of mild traumatic brain injury in the emergency department. Implement Sci. 2015;10:74.
Slot KB, Berge E. Thrombolytic treatment for stroke: patient preferences for treatment, information, and involvement. J Stroke Cerebrovasc Dis. 2009;18(1):17–22. doi: http://dx.doi.org/10.1016/j.jstrokecerebrovasdis.2008.06.009.
Moss C. Patients’ perspectives on the impact of fasting while in hospital. Evidence Based Nursing. 2016. doi:10.1136/eb-2015-102166.
Acknowledgements
Daun Jung conducted the hand searching and searching of grey literature during her Undergraduate Research Internship program at the Nursing Research Institute. DC was supported by a fellowship from the National Health and Medical Research Council (NHMRC; 1063761 co-funded by National Heart Foundation).
Funding
The T3 trial (registry number is ACTRN12614000939695) is funded by the National Health Medical Research Council ID APP1024812. This project was supported by an infrastructure grant provided by the Australian Catholic University to support the International Stroke Research Collaboration (ISReC).
Availability of data and materials
Not applicable.
Authors’ contributions
LC conducted the systematic review which involved developing the search strategies, running the searches in the databases and screening of references. EM and SM extracted data from a sub-set of included papers. Decisions were cross-checked with EM and SM at both the screening for exclusion, data extraction, and critical appraisal stages. LC and NT classified the barriers and enablers to the relevant domains of the TDF. LC wrote the first draft of the paper with contributions from EM, NT, RG, DC, JC, and SM. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Appendix
Search Strategies
-
1.
exp cerebrovascular disorders/or exp basal ganglia cerebrovascular disease/
-
2.
exp basal ganglia hemorrhage/or exp brain ischemia/
-
3.
exp brain infarction/or exp brain stem infarctions/
-
4.
exp cerebral infarction/or exp infarction, anterior cerebral artery/
-
5.
exp infarction, middle cerebral artery/
-
6.
exp infarction, posterior cerebral artery/
-
7.
exp hypoxia-ischemia, brain/
-
8.
exp “intracranial embolism and thrombosis”/
-
9.
exp intracranial hemorrhages/
-
10.
exp cerebral hemorrhage/
-
11.
exp subarachnoid hemorrhage/or stroke/
-
12.
exp Health Plan Implementation/
-
13.
*“Diffusion of Innovation”/
-
14.
((implementation or implementing) and (care or healthcare)).ti.
-
15.
((effect? or effectiveness or chang$ or improv$ or impact) adj3 practice).ti.
-
16.
(Improv$ adj3 (diagnosis or treatment? or prescribing)).ti.
-
17.
Evidence-Based Practice/
-
18.
(((evidence or evidence-based) adj4 intervention) or evidence-driven).ti,ab.
-
19.
((knowledge adj2 (application or broke$ or creation or diffus$ or disseminat$ or exchang$ or implement$ or management or mobili$ or translat$ or transfer$ or uptake or utili$)) or (evidence$ adj2 (exchang$ or translat$ or transfer$))).ti.
-
20.
“Quality of Health Care”/
-
21.
*Delivery of Health Care/st [Standards]
-
22.
*Treatment Outcome/
-
23.
“Continuity of Patient Care”/
-
24.
(determin$ or facilitate$ or barrier$ or enabler$).ti.
-
25.
(evidence$ adj2 (barrier$ or enabler$ or enabler$ or uptake$ or utilis$ or utiliz$ or diffus$ or disseminat$)).tw.
-
26.
((information or evidence) adj2 uptake).ti.
-
27.
(research adj2 (barrier$ or enabler$ or enabler$ or uptake$ or utilis$ or utiliz$ or diffus$ or disseminat$)).tw.
-
28.
(information adj2 (barrier$ or enabler$ or enabler$ or uptake$ or utilis$ or utiliz$ or diffus$ or disseminat$)).tw.
-
29.
(data adj2 (barrier$ or enabler$ or enabler$ or uptake$ or utilis$ or utiliz$ or diffus$ or disseminat$)).tw.
-
30.
Health Services Accessibility/
-
31.
*Critical Pathways/og [Organization & Administration]
-
32.
Clinical Protocols/
-
33.
Models, Organizational/
-
34.
exp triage/
-
35.
exp delegation, professional/
-
36.
(stroke adj3 (unit or units or ward or wards or hospital or hospitals or centre$ or team or teams)).tw.
-
37.
(“early transfer” or “early referral”).ti.
-
38.
Decision Making/
-
39.
Early Diagnosis/
-
40.
Emergency Nursing/
-
41.
*Stroke/di [Diagnosis]
-
42.
*Stroke/nu [Nursing]
-
43.
*Stroke/dt [Drug Therapy]
-
44.
Emergency Service, Hospital/og [Organization & Administration]
-
45.
*Time Factors/
-
46.
exp Tissue Plasminogen Activator/
-
47.
exp thrombolytic therapy/
-
48.
exp fibrinolytic agents/or plasmin/or plasminogen/or tissue plasminogen activator/
-
49.
((clot$ or thrombus) adj5 (lyse or lysis or dissolve$ or dissolution)).ti,ab.
-
50.
(tPA or t-PA or rtPA or thrombolysis or plasminogen or plasmin or alteplase or actilyse).ti,ab.
-
51.
(anistreplase or streptodornase or streptokinase or urokinase or pro?urokinase or rpro?uk or lumbrokinase or duteplase or lanoteplase or pamiteplase or reteplase or saruplase or staphylokinase or streptase or tenecteplase or desmoteplase or retevase).tw.
-
52.
exp fever/
-
53.
(fever or temperature or hyperthermia or pyrexia).tw.
-
54.
exp Blood Glucose/
-
55.
Hyperglycemia/di [Diagnosis]
-
56.
Hyperglycemia/dt [Drug Therapy]
-
57.
*Hyperglycemia/th [Therapy]
-
58.
Hypoglycemic Agents/ae [Adverse Effects]
-
59.
Hypoglycemic Agents/tu [Therapeutic Use]
-
60.
*Monitoring, Physiologic/nu [Nursing]
-
61.
exp insulins/or insulin infusion systems/
-
62.
*Deglutition Disorders/
-
63.
(swallow$ or dysphagia).ti.
-
64.
13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29
-
65.
1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11
-
66.
12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29
-
67.
30 or 31 or 32 or 33 or 34 or 35 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 58 or 51 or 52 or 53 or 54 or 55 or 56 or 57 or 58 or 59 or 60 or 61 or 62 or 63
-
68.
66 and 67 and 68
-
69.
Letter/or Comment/or Editorial/
-
70.
69 not 70
-
1.
exp clinical pathway/
-
2.
((implementation or implementing) and (care or healthcare)).ti.
-
3.
((effect? or effectiveness or chang$ or improv$ or impact) adj3 (practice or organisation$)).ti.
-
4.
(Improv$ adj3 (diagnosis or treatment?)).ti.
-
5.
*evidence based practice/
-
6.
(((evidence or evidence-based) adj4 intervention) or evidence-driven).ti.
-
7.
((knowledge adj2 (application or broke$ or creation or diffus$ or disseminat$ or exchang$ or implement$ or management or mobili$ or translat$ or transfer$ or uptake or utili$)) or (evidence$ adj2 (exchang$ or translat$ or transfer$))).ti.
-
8.
*health care delivery/
-
9.
*Treatment Outcome/
-
10.
*“Continuity of Patient Care”/
-
11.
(evidence$ adj2 (barrier$ or enabler$ or enabler$ or uptake$ or utilis$ or utiliz$ or diffus$ or disseminat$)).tw.
-
12.
((information or evidence or implement$) adj2 (uptake or determin$ or enabler$ or barrier$ or enabler$)).ti,ab.
-
13.
(research adj2 (barrier$ or enabler$ or enabler$ or uptake$ or utilis$ or utiliz$ or diffus$ or disseminat$)).tw.
-
14.
(information adj2 (barrier$ or enabler$ or enabler$ or uptake$ or utilis$ or utiliz$ or diffus$ or disseminat$)).tw.
-
15.
(data adj2 (barrier$ or enabler$ or enabler$ or uptake$ or utilis$ or utiliz$ or diffus$ or disseminat$)).tw.
-
16.
exp triage/
-
17.
exp delegation, professional/
-
18.
(stroke adj3 (unit or units or ward or wards or hospital or hospitals or centre$ or team or teams)).tw.
-
19.
(“early transfer” or “early referral”).ti.
-
20.
Decision Making/
-
21.
Early Diagnosis/
-
22.
Emergency Nursing/
-
23.
stroke/di, dt, th [Diagnosis, Drug Therapy, Therapy]
-
24.
emergency health service/
-
25.
*time/
-
26.
Tissue Plasminogen Activator/
-
27.
exp thrombolytic therapy/
-
28.
exp fibrinolytic agents/or plasmin/or plasminogen/or tissue plasminogen activator/
-
29.
((clot$ or thrombus) adj5 (lyse or lysis or dissolve$ or dissolution)).tw.
-
30.
(tPA or t-PA or rtPA or thrombolysis or plasminogen or plasmin or alteplase or actilyse).tw.
-
31.
(anistreplase or streptodornase or streptokinase or urokinase or pro?urokinase or rpro?uk or lumbrokinase or duteplase or lanoteplase or pamiteplase or reteplase or saruplase or staphylokinase or streptase or tenecteplase or desmoteplase or retevase).tw.
-
32.
fever/
-
33.
(fever or temperature or hyperthermia or pyrexia).ti.
-
34.
exp Blood Glucose/
-
35.
hyperglycemia/di, dt, rh, si [Diagnosis, Drug Therapy, Rehabilitation, Side Effect]
-
36.
antidiabetic agent/ae, th [Adverse Drug Reaction, Therapy]
-
37.
insulin derivative/
-
38.
dysphagia/
-
39.
(swallow$ or dysphagia).ti.
-
40.
exp cerebrovascular disorders/
-
41.
((cerebral* or cerebellar or brainstem or vertebrobasilar or stroke) adj5 (infarct* or ischaemi* or ischemi* or thrombo* or emboli* or apoplexy)).tw.
-
42.
exp hemiplegia/
-
43.
(hemipleg* or hemipar* or paresis or paretic).tw.
-
44.
(stroke or poststroke or post-stroke or cva* or cerebral vascular accident* or cerebrovascular accident*).tw.
-
45.
((cerebral or brain or subarachnoid) adj5 (haemorrhage* or hemorrhage* or haematoma* or hematoma* or bleed*)).tw.
-
46.
1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15
-
47.
16 or 17 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39
-
48.
40 or 41 or 42 or 43 or 44 or 45
-
49.
46 and 47 and 48
-
50.
Letter/or Editorial/
-
51.
49 not 50
-
S1
(MH “Cerebrovascular Disorders”) OR (MH “Basal Ganglia Cerebrovascular Disease+”) OR (MH “Carotid Artery Diseases+”) OR (MH “Cerebral Ischemia+”) OR (MH “Cerebral Vasospasm”) OR (MH “Intracranial Arterial Diseases+”) OR (MH “Intracranial Embolism and Thrombosis”) OR (MH “Intracranial Hemorrhage+”) OR (MH “Stroke”) OR (MH “Vertebral Artery Dissections”)
-
S2
(MH “Stroke Patients”)
-
S3
TI (stroke or cerebrovasc* or brain vasc* or cerebral vasc* or cva* or apoplex*) or AB (stroke or cerebrovasc* or brain vasc* or cerebral vasc* or cva* or apoplex*)
-
S4
TI (brain* or cerebr* or cerebell* or vertebrobasilar or hemispher* or intracran* or intracerebral or infratentorial or supratentorial or MCA or anterior circulation or posterior circulation or basal ganglia) or AB (brain* or cerebr* or cerebell* or vertebrobasilar or hemispher* or intracran* or intracerebral or infratentorial or supratentorial or MCA or anterior circulation or posterior circulation or basal ganglia)
-
S5
TI (ischemi* or ischaemi* or infarct* or thrombo* or emboli*) or AB (ischemi* or ischaemi* or infarct* or thrombo* or emboli*)
-
S6
TI (brain brain* or cerebr* or cerebell* or intracerebral or intracran* or parenchymal or intraventricular or infratentorial or supratentorial or basal gangli*) or AB (brain* or cerebr* or cerebell* or intracerebral or intracran* or parenchymal or intraventricular or infratentorial or supratentorial or basal gangli*)
-
S7
TI (haemorrhage* or hemorrhage* or haematoma* or hematoma* or bleed*) or AB (haemorrhage* or hemorrhage* or haematoma* or hematoma* or bleed*)
-
S8
MJ implementing
-
S9
TI (uptake or determine$ or enabler$ or enable$ or barrier$)
-
S10
S8 OR S9
-
S11
S1 OR S2 OR S3
-
S12
S4 AND S5
-
S13
S6 AND S7
-
S14
S11 OR S12 OR S13
-
S15
S15 AND S10
-
1.
TS = (stroke or cva or “cerebral vascular” or cerebrovascular)
-
2.
TI = (information OR evidence OR implement*)
-
3.
TI = (uptake or determin$ or enabler$ or enable$ or barrier$)
-
4.
#2 and #3
-
5.
#1 AND #4
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Craig, L.E., McInnes, E., Taylor, N. et al. Identifying the barriers and enablers for a triage, treatment, and transfer clinical intervention to manage acute stroke patients in the emergency department: a systematic review using the theoretical domains framework (TDF). Implementation Sci 11, 157 (2016). https://doi.org/10.1186/s13012-016-0524-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13012-016-0524-1