
Abstract
Objective
Social support is a key factor in the treatment and rehabilitation process of persons who use drug (PWUD). This highlights the need for a valid and reliable tool for assessing social support. The cultural and psychometric properties of community assessment inventory (CAI) in PWUDs under methadone therapy were examined in Iran in 2019.
Methods
The study was carried out as a validation and methodological study. At first, the original tool was translated into Farsi using forward-backward method. After ensuring face validity and content validity, construct reliability of the tool was supported using explorative and confirmatory factor analysis (EFA & CFA) using a sample group of 392 participants. The participants were selected through convenient-quota sampling from 24 drug clinics. Reliability of the questionnaire was supported using Pearson correlation coefficient and internal consistency based on Cronbach’s alpha.
Results
To determine content validity of the tool, CVI and CVR of it were obtained, which were on average equal to 0.79 and 0.59 respectively. The EFA supported correlation of the 37itmes of the tool (KMO = 0.975, Chi-square = 15,051.6, Pvalue=0.0001). The main indices of the model, based on CFA were higher than 0.9, which support goodness of fit of the model (χ2/DF = 2.98, CFI = 0.91, NFI, TLI = 0.905 GF = 0.92, REMSEA = 0.07, R2 = 0.99). Reliability of the tool based on internal consistency (Cronbach’s alpha) for the subscales were in 0.8–0.95 interval and equal to 0.85 for the whole tool.
Conclusion
As the results showed, CAI had acceptable indices for Iranian PWUDs under methadone therapy. The tool can be used for assessing social support level in the study population. It is a reliable and valid tool for studies in pertinent fields.
Similar content being viewed by others


Introduction
Drug use disorders is a chronic, continues, and frequent behavior that creates physical and mental dependence in the individual [1]. In general, according to available statistics, 0.9% of the world’s population suffers from drug use disorders. Drug use disorders, that do not include alcohol, have troubled between 0.4 and 3.5% of the world population and 2% of Iranian population [2].
A persons who use drug (PWUD) tends to have major psychosocial needs that require a comprehensive and organized care to ensure treatment and prevent relapse [3]. Family and social supports in every aspect throughout the treatment and rehabilitation process can be a key factor to prevent relapse [4]. Researches have shown that challenges like undesirable social-economic condition [3, 5], poor family support [6], inadequate perceived social support [4], inter-personal conflicts, stigmatization and discrimination are normally experienced by PWUD care-seekers under treatment [4, 7].
Social support is a situation in which a person considers themself a member of a group or community that is well understood by individuals and supported from various physical, psychological, emotional, social and financial aspects [4]. Social supports attenuate stress, improve self-efficacy [8] and self-esteem, improve social, mental, and physical condition of the individual, and improve performance [9]. Perceived social support can create positive changes in the life of care-seekers and improve their social interactions [8, 9]. Such interactions boost one’s self-esteem and self-efficacy and make them more persistent to continue the rehabilitation process [10]. Social support can be an important factor in continuing treatment as well as preventing relapse in PWUDs [7]. Social support can help them in the difficult process of rehabilitation by creating a sense of empathy and acceptance [11].
There are general tools to measure social support, which are used for PWUDs as well [4, 7, 12]. The Community Assessment Inventory (CAI) is a social support assessment tool designed by Brown et al. (2004) for PWUDs. The tool is specifically used to measure social support in these care-seekers. It contains 37 statements and four subscales namely household, family, friends, and community [13]. Given the statements used in the tool and the fact that it is specifically designed for PWUD, CAI can be a good tool for PWUDs in Iran.
Taking into account the importance of assessing social support in PWUDs and absence of a specially designed, reliable, and normalized tool for this population, the present study is an attempt to examine validity and psychometric characteristics of the tool for Iranian PWUDs under methadone therapy.
Methods
Setting
The study was carried out as a validation and methodological study [14]. Cultural and psychometric characteristics of CAI in Iranian PWUDs under methadone therapy were examined. The study was conducted between September 2018 and July 2019 in Kermanshah – west of Iran.
Participants
To determine face validity of the tool, it was provided to 20 PWUDs in Kermanshah-based drug clinics. With regard to content validity, the tool was provided to 12 faculty board members and researchers. In addition, for explorative factor analysis (EFA) and confirmatory factor analysis (CFA), the tool was provided to 400 PWUDs under methadone therapy [13] from 24 Kermanshah-based drug clinics. The participants were selected through convenient-quota sampling. The demographics of participants are listed in Table 1 (seven questionnaires were omitted for being not completely filled out).
Inclusion criteria were drug use disorder for at least one year, under methadone therapy for at least six months, desire to participate, not using synthetic drugs, and no physical and mental disease (medical file). Questionnaires that were not fully completed (less than 80% answered) were omitted.
Community assessment inventory (CAI)
The CAI was designed in 2004 by Brown et al. and developed for PWUDs. The questionnaire measures support in four fields of household (six items), family (10 items), friends (eight items), and community (13 items). The questionnaire contains 37 items designed based on Likert’s four-point scale (1 = completely disagree, 2 = disagree, 3 = agree, 4 = completely agree). The higher the score, the higher the performance in any of the sub-scales [10].
Cultural validation
After securing required permission for the designer of the tool, it was translated based on Wild et al.’s [15] ten steps following the translation and cultural comparability guideline. The ten steps are as follows:
-
Communicating with the designer and securing the required permissions.
-
Forward translation; two independent competent translators translated the tool from English into Farsi at the same time.
-
The two translations were examined and compared and one version was extracted.
-
Backward translation; the Farsi version was translated into English by two other independent and competent translators. They were asked to translate the meaning rather than word-by-work translation while remaining loyal to the origin.
-
The researchers and experts examined the two translations and one version was extracted.
-
The English translation was sent to the designer for feedbacks. Based on the feedbacks and considering the designer’s opinion, the original version of the tool was translated into Farsi.
-
To ensure qualitative face validity, the tool was provided to 20 drug users under methadone therapy with minimum education level of high school. As to qualitative content validity, the tool was provided to 20 researcher and experts for their opinions (12 returned).
-
The opinions were examined and implemented. None of the statements were removed at this stage.
-
The tool was revised in terms of Farsi grammar and writing style by the research team.
-
The final Farsi version was obtained.
After ensuring content validity through qualitative method, content validity through quantitative method was conducted as a supplementary method. To this end, CVR and CVI were computed (Table 2).
Construct validity was determined using EFA in SPSS (v. 25) and CFA was obtained in Lisrel (v. 8). Reliability of the scale was obtained through internal consistency method. Twenty PWUDs under methadone therapy filled the tool twice with two weeks internal. Afterwards, the obtained scores were compared using intra-class correlation. Cronbach’s alpha was used to determine internal consistency of the tool based on the subscales.
Results
Before performing EFA, adequacy of sampling test was conducted to ensure that the sample size is large enough. The KMO test was obtained equal to 0.97 and confirmed the adequacy of the sample size for EFA. The Bartlett’s test of sphericity was equal to 15.51.6, which confirmed the adequacy of correlation between the scale items for factor analysis (p-value < 0.001). Given that H0 is not supported, a significant relationship between the variables is supported. Therefore, the presumptions of CFA were met and it was conducted on the answers by the subjects to the 37 statements of the scale. Varimax perpendicular rotation and principle component (PC) analysis were used. None of the statements were removed (Fig. 1).

Scree plot of the extracted elements of the questionnaire
Construct validity – Confirmatory Factor Analysis
The mean score of statements ranged from 2.8 to five and the t-value ranged from 1.01–5.01. Skewness and Kurtosis were also at (− 2, 2) range. Therefore, normal distribution of the data is supported. In addition, the statements were at a desirable range given the factor load of each statement (p < 0.001), mean score, and t-value of the statements (Table 2).
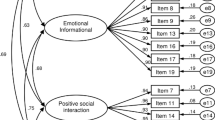
Figure 2 illustrates CFA model of the variable under study in standard mode and without coefficients. Since t-values in all cases are higher than |1.96| and the factor load is higher than 0.3 (Table 2), none of the statements were omitted. Based on the goodness of fit indices in CFA model, the goodness of fit of model with the collected data was supported (Table 3) (Fig. 2).

Four factor model of CVI in Iranian PWUDs
With R2 = 0.99, 99% of variation of the dependent variable (total score of CAI) can be attributed to the independent variable (37 statements). In other words, 99% of changes in depended variable is caused by the independent variable.
With the support of normality of data in CAI items for PWUDs under methadone therapy, Pearson’s correlation test showed a direct and significant correlation at 99% confidence level (Table 4). In addition, there was is a direct and significant relationship between CAI subscales and total score of the tool (Table 5).
To examine internal reliability of CAI, Cronbach’s alpha was computed for the whole tool equal to 0.85. Based on the results, the Farsi version of CAI had an acceptable internal consistency and the coefficient for the subscales of CAI ranged from 0.80 to 0.95 (Table 6).
Discussion
The CAI was translated and validated for PWUDs under methadone therapy in Iran. One feature of the study is that along with using the care-seekers’ opinions about face validity, the experts were also consulted about content validity. Through this, clarity and understandability of the statements were determined. Brown et al. (2004) examined face and content validity using the same method [13].
Construct validity of CAI in the subjects was measured using EFA and CFA. Halamova et al. (2018) followed the same approach [16] and Canty-Mitchel et al. (2000) used CFA to measure construct validity [17]. Clearly, factor analysis methods are commonly used for this purpose.
Factor analysis results supported all the 37 items and goodness of fit indices all were higher than 0.9, which supported goodness of fit of the tool (χ2/DF = 2.98, CFI = 0.91, NFI, TLI = 0.905 GF = 0.92, REMSEA = 0.07, R2 = 0.99). Halamova et al.(2018) also reported that goodness fit indices were above 0.9 (CFI = 0.98, NFI, TLI = 0.984 REMSEA = 0.045) and supported goodness of fit of the tool [16].
Pearson correlation coefficient also supported a significant and direct correlation of CAI subscales with each other and the total score of the tool. Brown et al. (2004) reported a direct and significant correlation between the subscales and the total score of the tool [13]. Canty-Mitchel et al. also reported similar results [17]. To elaborate on the findings, along with validating psychometric characteristics of the tool, consistent with other studies, our results also supported internal consistency of the scale.
As the results showed, the Farsi version of CAI has an acceptable internal consistency for PWUDs in Iran. Reliability of the subscales, based on Cronbach’s alpha was at 0.8–0.95 range. Therefore, the subscales are reliable. Khuong et al.(2018) also reported that Cronbach’s alpha of the tool was less than 0.81 [18]. A similar study by Priede et al. reported Cronbach’s alpha more than 0.7 [19]. Although, the number of subjects in these studies is different, the similar values of Cronbach’s alpha support the findings of the present study.
Data gathering was done using the questionnaire; therefore, it was not possible to examine subjective data. This, however, is a common feature of descriptive and tool validation works. Overcrowded clinics, boredom, muscles and joints pains, and lack of enough time to answer the items of the tool were some of the limitations of the study. These limitations prevented giving accurate answers to the questions in some of the subjects. To solve this problem, the author tried to explain the study design and its necessity and remove ambiguities if any.
Conclusion
As the results showed, CAI had acceptable indices for Iranian PWUDs under methadone therapy. The tool can be used for assessing social support level in the study population. It is a reliable and valid tool for studies in pertinent fields. In general, CAI was a standard and acceptable tool for PWUDs (Natural and industrial drugs) in Iran and future studies can use the tool.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CAI:
-
Community Assessment Inventory
- PWUD:
-
Person/s with use/s drug/s
- CVI:
-
Content Validity Index
- CVR:
-
Content Validity Ratio
- KMO:
-
Kaiser Meyer Olkin
- EFA:
-
Explorative factor analysis
- TLI:
-
Tucker-Lewis Index
- NFI:
-
Normed Fit Index
- GFI:
-
Goodness of Fit Index
- CFA:
-
Confirmatory Factor Analysis
- PC:
-
Principle Components RMSEA Root Mean Square Error of Approximation
- KUMS:
-
Kermanshah University of Medical Sciences
References
Yang M, Mamy J, Gao P, Xiao S. From abstinence to relapse: a preliminary qualitative study of drug users in a compulsory drug rehabilitation Center in Changsha, China. PLoS One. 2015;10(6):1–17.
Ritchie H, Roser M. Opioids, cocaine, cannabis and illicit drugs. Published online at OurWorldInDataorg Retrieved from: https://ourworldindata.org/illicit-drug-use. 2018. Accessed 6 Nov 2020.
Roshani B, Jalali A, Bidhendi S, Ezzati E, Mahboubi M. Study the causes of relapse among Iranian drugs users in Kermanshah. Life Sci J. 2014;11(1):66–71.
Rahimi S, Jalali A, Jalali R. Social support among women undergoing methadone maintenance treatment in Iran. J Addict Nurs. 2018;29(3):179–87. https://doi.org/10.1097/jan.0000000000000234.
Yoosefi Lebni J, Ziapour A, Qorbani M, Baygi F, Mirzaei A, Safari O, et al. The consequences of regular methamphetamine use in Tehran: qualitative content analysis. Subst Abuse Treat Prev Policy. 2020;15(1):33. https://doi.org/10.1186/s13011-020-00277-3.
Jalali A, Yekzaman M, Bazrafshan M, Salari N, Rahmati M. Investigating the effect of family counseling on the acceptance and support of patients under methadone maintenance treatment. Shiraz E-Med J. 2018;19(5):e62347. https://doi.org/10.5812/semj.62347.
Farnia V, Alikhani M, Jalali A, Golshani S, Salemi S, Hookari S, et al. The role of attachment styles and perceived social support in prediction of methamphetamine abuse. J Subst Abus. 2018;23(4):377–83. https://doi.org/10.1080/14659891.2018.1436598.
Cucciare MA, Han X, Curran GM, Booth BM. Associations between religiosity, perceived social support, and stimulant use in an untreated rural sample in the U.S.a. Subst Use Misuse. 2016;51(7):823–34.
Cruz MS, Andrade T, Bastos FI, Leal E, Bertoni N, Lipman L, et al. Patterns, determinants and barriers of health and social service utilization among young urban crack users in Brazil. BMC Health Serv Res. 2013;13(536):1–12.
Elahei Roudposhti N, Jalali A, Khaledi Paveh B, Salari N. Cognitive-behavioral counseling and self-perception of male clients receiving methadone maintenance treatment. Alcohol Treat Q. 2018;36(3):419–27. https://doi.org/10.1080/07347324.2018.1471330.
Jalali A, Seyedfatemi N, Peyrovi H. Relapse model among Iranian drug users: a qualitative study. Int J Commun Based Nurs Midwifery. 2015;3(1):2–11.
Ramaswamy M, Kelly PJ, Li X, Berg KM, Litwin AH, Arnsten JH. Social support networks and primary care use by HIV-infected drug users. J Assoc Nurses AIDS Care. 2013;24(2):135–44.
Brown BS, O'Grady KE, Battjes RJ, Katz EC. The community assessment inventory--client views of supports to drug abuse treatment. J Subst Abus Treat. 2004;27(3):241–51. https://doi.org/10.1016/j.jsat.2004.08.002.
Polit DF, Beck CT. The content validity index: are you sure you know what's being reported? Critique and recommendations. Res Nurs Health. 2006;29:489–97.
Wild D, Grove A, Martin M, Eremenco S, McElroy S, Verjee-Lorenz A, et al. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health. 2005;8(2):94–104. https://doi.org/10.1111/j.1524-4733.2005.04054.x.
Halamová J, Kanovský M, Naništová E. Development and Psychometric Analysis of the Sense of Community Descriptors Scale. Psychol Intrevention. 2018;27(1):44–55. https://doi.org/10.5093/pi2018a8.
Canty-Mitchell J, Zimet GD. Psychometric properties of the multidimensional scale of perceived social support in urban adolescents. Am J Community Psychol. 2000;28(3):391–400. https://doi.org/10.1023/a:1005109522457.
Khuong LQ, Vu T-VT, Huynh V-AN, Thai TT. Psychometric properties of the medical outcomes study: social support survey among methadone maintenance patients in Ho Chi Minh City, Vietnam: a validation study. Substance Abuse Treat Prev Policy. 2018;13(1):8. https://doi.org/10.1186/s13011-018-0147-4.
Priede A, Andreu Y, Martinez P, Conchado A, Ruiz-Torres M, Gonzalez-Blanch C. The factor structure of the medical outcomes study-social support survey: a comparison of different models in a sample of recently diagnosed cancer patients. J Psychosom Res. 2018;108:32–8. https://doi.org/10.1016/j.jpsychores.2018.02.008.
Acknowledgements
We are grateful to the Deputy for Research and Technology, Kermanshah University of Medical Sciences, for cooperating in this research. We thank all the participants in the study.
Funding
This study was drawn from a research project (No. 97529) sponsored by deputy of research and technology of KUMS. The fund was spent on the design and implementation of the study.
Author information
Authors and Affiliations
Contributions
N S, contributed in study concept, study design, data collection and manuscript preparation. A J, contributed in study concept, study design, data Analysis, manuscript preparation and submitting the manuscript. B A, contributed in study concept, study design and manuscript preparation. A A, contributed in study design, data analysis and manuscript preparation. HD, contributed in study concept, study design, data analysis, manuscript preparation. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was carried out after securing a written letter of permission from the designer of the tool and a permission from the Ethics Committee of Kermanshah University of Medical Sciences (IR.KUMS.REC.1397.546). All the ethical codes based on the Declaration of Helsinki were observed.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflict of interest about this work.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Salari, N., Jalali, A., Abdam, B. et al. Validation and psychometric properties of the community assessment inventory in Iranian persons who use drug. Subst Abuse Treat Prev Policy 15, 46 (2020). https://doi.org/10.1186/s13011-020-00290-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13011-020-00290-6