
Abstract
Background
Alcohol use disorder (AUD) is common among people living with HIV/AIDS (PLWHA) and associated with a greater risk of poor medication adherence, unsafe sexual behaviors as well as poor quality of life. To our knowledge, there is no previous systematic review and meta-analysis that reported the pooled prevalence estimate of AUD among PLWHA. Therefore, this review aimed to systematically review the available studies on the prevalence of AUD among PLWHA and forward possible recommendations for future clinical practice and research.
Methods
PubMed, EMBASE, Psych INFO and SCOPUS databases were searched to identify the relevant studies. We have also scanned the reference lists of the eligible studies to supplement our electronic search. We used the Comprehensive Meta-Analysis software versions 3.0 to conduct a meta-analysis. Subgroup and sensitivity analysis were performed and Cochran’s Q- and the I2- test were employed to see the heterogeneity. The presence of publication bias was explored by utilizing Egger’s test and visual inspection of the symmetry in funnel plots.
Results
A total of 25 studies with 25,154 participants across developed and developing countries were included in the final analysis. Our meta-analysis revealed that the pooled prevalence estimate of AUD among PLWHA was found to be 29.80% (95% CI; 24.10–35.76). The prevalence of AUD was higher in males (26.90%) than female (13.37%) HIV patients. In this study, the pooled prevalence of AUD was considerably higher (31.52%) when measured by Alcohol Use Disorders Identification Test (AUDIT) as compared to Composite International Diagnostic Interview (CIDI) (13.51%). In addition, the pooled prevalence of AUD was higher in the developed countries (42.09%) while lower for developing countries (24.52%).
Conclusion
In the current study, the pooled prevalence estimates of AUD among PLWHA was considerably high (29.80%). Screening and appropriate management of AUD among PLWHA are recommended.
Similar content being viewed by others


Background
Human Immunodeficiency Virus (HIV) infection is a major public health concern that claimed the life of 770,000 people in 2018 [1]. Globally, 37.9 million people were living with HIV at the end of 2018 and 1.7 million people becoming newly infected with HIV in 2018 [1]. A significant number of HIV infected individuals suffer from substance use disorders [2].
The World Health Organization (WHO) defines substance use disorder as the harmful or hazardous use of any psychoactive substances, including alcohol and illicit drugs [3]. Kaplan & Sadock’s Synopsis of Psychiatry refers “alcohol use disorder (AUD) as the continuous use of alcohol despite evidence of harm and repeated attempts to cut down the use” [4]. Alcohol use disorder results in short and long term impacts on the physical, mental and socio-economic aspects of individual life [5]. Further, AUD contributes nearly 4% of the global burden of disease [6].
Alcohol use disorder is commonly left undiagnosed among people living with HIV/AIDS (PLWHA), which could potentially lead individuals to engage in a number of high-risk activities such as involvement in unsafe sexual engagement that might enhance the spread of HIV [7, 8] as well as compromise the antiretroviral therapy (ART) response [9].
A study conducted to assess the prevalence of non-HIV cancer risk factors in persons living with HIV/AIDS reported PLWHA are two to four times more likely to use alcohol than the general population [10]. Other similar studies also reported that 40 to 50% of individuals living with HIV/AIDS have a history of alcohol abuse or dependence [11, 12].
There are different rates of prevalence of alcohol use disorder among PLWHA across developed and developing countries [9,10,11,12,13]. For example, a cross-sectional study conducted in Nigeria to assess the prevalence of AUD among PLWHA revealed 39.4% [14] whereas, a prospective cohort study from the United States of America reported 12% prevalence [15].
Alcohol use disorder has a significant impact on PWLHA. For instance, AUD can interfere with the immune system of the body [14], predispose individuals to bacterial infections like tuberculosis [16], may result in liver damage, and alter the metabolism of antiretroviral drugs [17]. AUD is also associated with harmful behavior, such as tobacco smoking, illicit drug use and unsafe sexual practices [18].
The findings from the recent studies revealed AUD among PLWHA was linked with more serious cognitive problems such as reduced response time, executive functioning and verbal or visuospatial learning and memory [19, 20]. Furthermore, PLWHA with AUD have a poor health-related quality of life (QOL) which can put negative influence on the physical and emotional well-being of the individuals [20,21,22,23].
Even though a wide range of studies showed AUD as a significant public health importance, there is no systematic review and meta-analysis conducted to assess the prevalence of AUD among PLWHA. Therefore, this systematic review and meta-analysis aimed to summarize the existing evidence on the prevalence of AUD among PLWHA and to formulate possible suggestions for future clinical practice and research community.
Methods/design
Study design and search process
We performed an extensive search of literature as suggested by the guideline of reporting systematic review and meta-analysis (PRISMA) [24]. We have reviewed published literature conducted on the prevalence of AUD among PLWHA. The systematic literature search was conducted using electronic databases such as PubMed, EMBASE, Psych INFO, and SCOPUS. We performed our electronic search in PubMed using the following MeSH (Medical Subject Headings) terms: “(alcohol use OR alcohol use disorder OR hazardous drinking OR alcohol abuse OR alcohol dependence)) AND (prevalence OR magnitude OR epidemiology)) AND (HIV OR human immune deficiency virus OR AIDS OR acquired immune deficiency syndrome)”. The other databases such as EMBASE and SCOPUS were also comprehensively searched by applying the search terms used in PubMed for each database. In addition, we have manually searched the reference lists of eligible articles.
Eligibility criteria
In this systematic review and meta-analysis, appraisal of the identified studies was done using their title and abstract before the retrieval of full-text articles for further screening by the two reviewers (BD and GA). We adhered a predefined inclusion and exclusion criteria to screen the retrieved full articles and any discrepancies were solved by a discussion with a third reviewer (MA). We have included the studies in the review using the following inclusion criteria: First, cross-sectional and other observational studies; Second, conducted among PLWHA; Third, studies that were published in the English language; finally, studies that determined the prevalence of AUD among PLWHA. Therefore, we excluded duplicate studies, commentaries, reviews, letters, editorials, and short communications as they did not satisfy the eligibility criteria.
Methods for data extraction and quality assessment
Two reviewers (BD and MA) conducted the data extraction from the relevant articles. The following information was extracted: the name of the first author, the year of publication, study setting, and design, sample size, prevalence, and tools used to estimate the magnitude of AUD, and the reported magnitude by gender of the participants (See Table 1). Disagreements raised during data extraction were solved by discussion and consensus. A modified and adapted version of the Newcastle-Ottawa Scale (NOS) [47, 48] was used to assess the quality of included studies in the meta-analysis (See Additional file 1). The data collection tool used to measure AUD, sample size, statistical quality, sample representativeness and comparability between participants were the domains of the NOS scale to assess the quality of the eligible articles.
Data synthesis and analysis
We used a Comprehensive Meta-Analysis software version 3.0 to conduct a meta-analysis. The random effect model for meta-analysis was used to measure the overall pooled prevalence of AUD among PLWHA. The magnitude of statistical heterogeneity between the eligible articles was measured by using Q statistic and the I2 statistics [49] and values of 25, 50 and 75% were used to represent low, medium and high quality respectively [50]. Subgroup and sensitivity analysis was conducted to determine the potential source bias. The instruments used to assess the presence or absence of AUD, the location of the studies as well as the quality of the included studies were used as a moderator to assess the sensitivity as well as subgroup analysis. The funnel plot and Egger’s regression tests were used to assess potential publication bias [51].
Results
Identification of studies
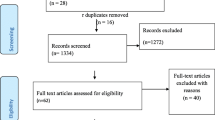
Our electronic database, as well as additional manual search, resulted in a total of 5505 documents. After a thorough screening, a full-text of 42 articles were retrieved for further appraisal and 17 of these were excluded (see Fig. 1).

Shows the PRISMA flowchart of systematic review search
Characteristics of included studies
In the current systematic review and meta-analysis, a total of 25 articles conducted in developing and developed countries including 25,154 participants were included in the final meta-analysis. The characteristics of the included studies was illustrated in Table 1. The studies included in this review were published between 2006 and 2019, with the sample size ranging between 108 participants in Brazil and 8567 participants in the USA. Among the 25 studies, five were from the USA, three from Brazil, one from Russia, one from India, one from Nepal and 11 from African countries. AUD among PLWHA was predominantly measured using AUDIT [52]. Thus, the AUDIT was used in 23 studies while the CIDI was used in only 2 studies.
Quality of included studies
Among the included articles, 19 articles were high quality (NOS score 8 and above), 5 articles were moderate quality (NOS score between 6 and 7 inclusive) and 1 article was low-quality studies (NOS score less than or equal to 5) (See Additional file 2).
The prevalence of AUD among PLWHA (meta-analysis)
In this review, twenty-five articles that reported the prevalence of AUD among PLWHA were included in the final analysis (Table 1). The pooled prevalence estimate of AUD among PLWHA was found to be 29.80% (95% CI; 24.10–35.76). We used a random-effect model due to the reported heterogeneity. We found an apparent heterogeneity for this analysis (I2 = 98.75%; p < 0.001) (See Fig. 2).

Shows the pooled prevalence of AUD among HIV patients: meta-analysis
Subgroup and sensitive analysis
The available epidemiologic evidence was diverse by the location of the study (the origin of the study), the instrument used to estimate AUD, the gender of participants as well as the methodologic quality.
The prevalence of AUD among PLWHA by developed and developing countries
In our subgroup analysis of developing and developed countries as a moderator, we found a significantly higher prevalence of AUD in developed countries 42.09% (95% CI 27.29–58.47) while comparably lower prevalence in the developing countries 24.52% (95% CI 19.66–30.14). The variation between the countries was statistically significant (P < 0.001) (See Table 2).
Subgroup analysis of the prevalence of AUD by the instrument used
We further performed a subgroup analysis using the type of instrument used to assess AUD as a moderator. The pooled prevalence of AUD was considerably higher when measured by AUDIT 31.52% (95%CI; 25.66–38.02) as compared to CIDI 13.51% (95%CI; 11.86–15.34%). The heterogeneity was significant for the studies performed by AUDIT (I2 = 98.75%, p < 0.0001), but not for CIDI (I2 = 2.13%, 0 = 0.312) (See Table 2).
Subgroup analysis of the prevalence of AUD among HIV patients by gender of participants
In this review, 15 studies reported the prevalence of AUD in male and female participants. Analysis of those previous studies which reported the prevalence of AUD by males and females revealed the higher prevalence in male 26.90% (95% CI, 19.72–35.53) than females 13.37% (95% CI, 8.79–19.80). A significant heterogeneity was found in both males (I2 = 97.92; p < 0.001) and females (I2 = 97.03; p < 0.001) (see Table 2).
Subgroup analysis of the prevalence of AUD among HIV patients by the quality of studies
Finally, we also performed the sensitivity analysis based on the quality of the included studies. The prevalence AUD for high quality was 28.50% and it was 33.19% for moderate and low-quality studies, even though the difference was not statistically significant (P = 0.586) (see Table 2).
Publication bias
For the overall meta-analysis of the prevalence of AUD among PLWHA, the funnel plot was symmetric and Egger’s regression tests provided no evidence of potential publication bias (B = 1.69, SE = 3.38, P = 0.621) (See Fig. 3).

Shows the funnel plot of publication bias of the included studies
Discussion
To our knowledge, this is the first systematic review and meta-analysis that explored the prevalence of AUD among PLWHA. The result of the pooled meta-analysis showed that the magnitude of AUD was remarkably high among PLWHA (29.80%). This finding indicates AUD is a significant public health issue among PLWHA.
In the present systematic review and meta-analysis, the available epidemiologic evidence was diverse by the location of the study (the origin of the study), the instrument used to estimate AUD, as well as the methodologic quality. Most of the studies used AUDIT while only 2 studies used CIDI to measure AUD. The majority of the included studies were of high quality (n = 19).
In this review, the pooled prevalence estimate of AUD among PLWHA (29.80%) was higher than the reported prevalence of AUD among the general population of the globe. For example, the studies conducted to assess the prevalence of AUD among the general population in the USA, Europe, and Australia reported 13.9, 11.1 and 11.8% respectively [53,54,55]. This variation might be due to people with the terminal illness such as HIV, may use alcohol as a coping mechanism for a way of dealing with psychological distress resulted due to the severity of the HIV illness and antiretroviral drugs side-effects [54, 55].
Contrarily, the pooled prevalence of AUD in our meta-analysis was lower than the prevalence of AUD among patients with schizophrenia, major depressive disorder and personality disorder which were 33.7, 28, and 50–70% respectively [56]. This may be due to the triggering effect of mental disorders. Thus, having mental disorders could result in alcohol use disorder in this group of population.
In our subgroup analysis, the pooled prevalence of alcohol use disorder was higher in men (26.90%) than women (13.37%). The difference in the prevalence of AUD among men and women may be due to the difference in the neurochemistry of the brain in the respective genders. For instance, a study conducted in the USA reported that regardless of the same level of alcohol drinking, a male has a higher dopamine release than a female [57]. The researchers of this study believe, the ability of alcohol to stimulate the release of dopamine may potentially contribute to its rewarding effect and this may be linked with a higher prevalence of AUD in males. Further, the difference in prevalence might be due to the variations in socio-cultural aspects of person’s life, for example, some cultures might not allow women to drink alcohol and also other environmental factors may play a role in this variation [58, 59].
The subgroup analysis using the instruments used to estimate AUD revealed a significant difference in the prevalence of AUD among PLWHA. The pooled prevalence of AUD was higher in studies conducted using AUDIT (31.50%) than CIDI (13.51%). The difference in instruments may contribute to the variation in the prevalence of AUD. For instance, AUDIT is a screening tool with aim of detecting early or risk factors of alcohol use disorder in a large number of asymptomatic whereas CIDI is a diagnostic tool which potentially depicts the presence or absence of AUD in symptomatic individuals to establish the diagnosis and arrange for clinical management [59].
Furthermore, the pooled prevalence estimates of AUD among PLWHIVA in developed countries (42.52%) was significantly higher than the pooled prevalence estimates of the developing countries (24.52%). This finding is in line with the other study conducted on alcohol abuse that revealed the prevalence of alcohol use in developed and developing nations which were 29.3 and 16.2% respectively [60]. In addition to this, the variation in the socio-economic status of the countries, cultural differences, the accessibility and availability of alcoholic beverages, variation in the number of studies in developed countries and the study setting capability of investigation might contribute to the difference in the prevalence of alcohol use among PLWHA.
Strength and limitations
The strengths are: (1) We employed our search based on a predefined search strategy designed to minimize reviewer’s bias; (2) data extraction and quality appraisal were done by two independent authors; (3) Execution of the sensitivity and subgroup analysis, countries of the study, the gender of the participants and the AUD assessment tool used. However, the review has the following limitations. The small number of articles that were included in the subgroup analysis could decrease the accuracy of the estimate. Furthermore, the AUDIT questionnaire has high sensitivity (94.1%). This could overestimate the prevalence of AUD in the studies that used AUDIT to assess AUD. In addition, few studies (two) used CIDI to measure AUD. This could also limit the sub-group analysis when using tools of AUD as a moderator. In addition, the review included articles only published in the English language. This also could underestimate the pooled prevalence of AUD.
Conclusion
The results of the current review revealed that the prevalence of AUD among PLWHA was high when compared to the prevalence of AUD in the general population. The pooled prevalence of AUD was higher as it was measured by the AUDIT as compared to CIDI. We also found that the prevalence of AUD was higher in men than in women. The prevalence estimates of AUD showed significant variation across developed and developing countries. Screening and appropriate management of AUD among PLWHA is recommended. Further strong studies with representative sample size across the globe were warranted to strengthen our findings. Furthermore, further studies focusing on the magnitude of AUD across different countries as well as gender were warranted.
Availability of data and materials
All data generated or analyzed data in study are included in this article.
Abbreviations
- AUD:
-
Alcohol use disorder
- AUDIT:
-
Alcohol used disorder identification test
- CIDI:
-
Composite International Diagnostic Interview
- PLWHA:
-
People living with HIV/AIDS
- QOL:
-
Quality of life
References
World Health Organization (WHO), Key Facts on HIV/AIDS. 2019. https://www.who.int/news-room/fact-sheets/detail/hiv-aids.
Galvan FH, Bing EG, Fleishman JA, London AS, Caetano R, Burnam MA, et al. The prevalence of alcohol consumption and heavy drinking among people with HIV in the United States: results from the HIV cost and services utilization study. J Stud Alcohol. 2002;63(2):179–86.
World Health Organazation (WHO), Substance abuse (2014), https://www.who.int/topics/substance_abuse/en/
Sadock BJ, Sadock VA. Alcohol related disorders in Kaplan & Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry (10th ed.)390–407. Philadelphia, PA, Lippincott, Williams & Wilkins; 2007.
Probst C, Parry CDH, Rehm J. HIV/AIDS mortality attributable to alcohol use in South Africa: a comparative risk assessment by socioeconomic status. BMJ Open. 2018;8:e017955.
Global Burden of Disease. Global Burden of Disease 2010: Understanding Disease, Injury, and Risk. Glob Burd Dis. 2012;2012:380.
Chander G, Lau BMR. Hazardous alcohol use: a risk factor for nonadherence and lack of suppression in HIV infection. J Acquir Immune Defic Syndr. 2006;43:411–7.
Segni MT, Teshome G, Demissie HF. AIDS & Clinical Research Substance use and associated factors among retro viral infected ( RVI ) patients on antiretroviral treatment (ART ) at Assela teaching hospital. J AIDS Clin Res. 2017;8(6):6–10.
Hahn JA, Bwana MB, Javors MA, Martin JN, Emenyonu NI, Bangsberg DR. Biomarker testing to estimate under-reported heavy alcohol consumption by persons with HIV initiating ART in Uganda. AIDS Behav. 2010;14(6):1265–8.
Park LS, Hernandez-Ramirez RU, Silverberg MJ, Crothers K, Dubrow R. Prevalence of non-HIV cancer risk factors in persons living with HIV/AIDS: a meta-analysis. AIDS. 2016;30(2):273–91.
Lefevre F, O’Leary B, Moran M, Mossar M, Yarnold PR, Martin GJ, et al. Alcohol consumption among HIV-infected patients. J Gen Intern Med. 1995;10:458–60.
Samet JH, Phillips SJ, Horton NJ, Traphagen ETFK. Detecting alcohol problems in HIV-infected patients: use of the CAGE questionnaire. AIDS Res Hum Retrovir. 2004;20:151–5.
Goar SG, Audu MD, Agbir MT, Dochalson E, Prevalence and Socio-demographic correlates of alcohol use disorders among HIV patients, African Journal of Drug & Alcohol Studies, (2011)10(1).
Orwat J, Saitz R, Tompkins CP, Cheng DM, Dentato MP, Samet JH. Substance abuse treatment utilization among adults living with HIV/AIDS and alcohol or drug problems. J Subst Abus Treat. 2011;41(3):233–42.
Williams EC, Hahn JA, Saitz R, Bryant K, Lira MC, Samet JH. Alcohol use and human immunodeficiency virus (HIV) infection: current knowledge, implications, and future directions. Alcohol Clin Exp Res. 2016;40(10):2056–72.
Amoakwa K, Martinson NA, Moulton LH, Barnes GL, Msandiwa R, Chaisson RE. Risk factors for developing active tuberculosis after the treatment of latent tuberculosis in adults infected with human immunodeficiency virus. Open Forum Infect Dis. 2015;2:ofu120.
Bonacini M. Alcohol use among patients with HIV infection. Ann Hepatol. 2011;10(4):502–7.
Benhamou Y, Bochet M, Di Martino V, Charlotte F, Azria F, Coutellier A, et al. Liver fibrosis progression in human immunodeficiency virus and hepatitis C virus coinfected patients. Multivirc Gr Hepatol. 1999;30:1054–8.
Parsons JT, Vicioso K, Kutnick A, Punzalan JC, Halkitis PNVM. Alcohol use and stigmatized sexual practices of HIV seropositive gay and bisexual men. Addict Behav. 2004;29:1045–51.
Suwa G. Goar, Moses D. Audu Mt A & Edward D, Suwa G. Goar, Moses D. Audu, Michael T. Agbir & Edward Dochalson. African J Drug Alcohol Stud. 2011;10(1).
Porges EC, Bryant VE, Woods AJ, et al. The effect of current alcohol consumption on cognitive impairment varies as a function of HIV status and age. Alcohol Clin Exp Res. 2015;39:268a.
Jia H, Uphold CR, Wu S, Chen GJ, Duncan PW. Predictors of changes in health-related quality of life among men with HIV infection in the HAART era. AIDS Patient Care STDs. 2005;19(6):395–405.
Moak ZBAA. The association between perceived interpersonal social support and physical and mental health: results from the National Epidemiological Survey on Alcohol and Related Conditions. J Public Heal (Oxf). 2010;32:191–201.
Reviews UoYCf, Dissemination. Systematic reviews: CRD's guidance for undertaking reviews in health care: University of York, Centre for Reviews & Dissemination; 2009.
Silverberg MJ, Leyden WA, Leibowitz A, Hare CB, Jang HJ, Sterling S, et al. Factors associated with hazardous alcohol use and motivation to reduce drinking among HIV primary care patients: Baseline findings from the Health & Motivation study. Addict Behav. 2018;84:110–7.
da Silva CM, Mendoza-Sassi RA, da Mota LD, Nader MM, de Martinez AM. Alcohol use disorders among people living with HIV/AIDS in southern Brazil: prevalence, risk factors and biological markers outcomes. BMC Infect Dis. 2017;17(1):263.
Crane HM, McCaul ME, Chander G, et al. Prevalence and factors associated with hazardous alcohol use among persons living with HIV across the US in the current era of antiretroviral treatment. AIDS Behav. 2017;21(7):1914–25.
Nouaman MN, Vinikoor M, Seydi M, et al. High prevalence of binge drinking among people living with HIV in four African countries. J Int AIDS Soc. 2018;21(12):e25202.
Pokhrel KN, Pokhrel KG, Neupane SR, Sharma VD. Harmful alcohol drinking among HIV-positive people in Nepal: an overlooked threat to anti-retroviral therapy adherence and health-related quality of life. Glob Health Action. 2018;11(1):1441783.
Egbe CO, Dakum PS, Ekong E, Kohrt BA, Minto JG, Ticao CJ. Depression, suicidality, and alcohol use disorder among people living with HIV/AIDS in Nigeria. BMC Public Health. 2017;17(1):542.
Rosemary WK. The prevalence of alcohol and substance use disorders among HIV infected youth aged between 15-25 years old at Mbagathi Hospital, Kenya (dissertation). http://erepository.uonbi.ac.ke/bitstream/handle/11295/94741/Kiunyu_Prevelance%20Of%20Alcohol%20&%20Substance%20Use%20Disorders%20Among%20Hiv%20Infected%20Youth%20Aged%20Between%201525%20Yrs%20Old%20At%20Mbagathi%20Hospital.pdf?sequence=3.
Kibera AW, Kuria MW, Kokonya DA. Alcohol Use Disorders Among HIV and AIDS Patients at Kenyatta National Hospital (KNH) Comprehensive Care Centre, Nairobi, Kenya. International Journal of Research Studies in Medical and Health Sciences. 2017;2(7):21–30.
Mayston R, Patel V, Abas M, Korgaonkar P, Paranjape R, Rodrigues S, et al. Determinants of common mental disorder, alcohol use disorder and cognitive morbidity among people coming for HIV testing in Goa, India. Trop Med Int Health. 2015;20:397–406.
Belayneh Z, Mekuriaw B, Abebe Z, Alcohol use disorders and associated factors among adults attending art clinics in Gedeo Zone health centers, Southern Ethiopia: a cross sectional study, Journal of Virology & Antiviral Research, 2018, Volume: 7.
de Oliveira LC, Dos Anjos MG, Macedo Mustafe R, Sebastiao BA. Alcohol consumption and associated factors among HIV/AIDS patients. Braz J Infect Dis. 2016;20(3):320–1.
Soboka M, Tesfaye M, Feyissa GT, Hanlon C. Alcohol use disorders and associated factors among people living with HIV who are attending services in south West Ethiopia. BMC Res Notes. 2014;7:828.
Parsons JT, Starks TJ, Millar BM, Boonrai K, Marcotte D. Patterns of substance use among HIV-positive adults over 50: implications for treatment and medication adherence. Drug Alcohol Depend. 2014;139:33–40.
Simon D, Michita R, Béria J, Tietzmann D, Stein A, Lunge V. Alcohol misuse and illicit drug use are associated with HCV/HIV co-infection. Epidemiol Infect. 2014;142(12):2616–23.
Medley A, Seth P, Pathak S, Howard AA, DeLuca N, Matiko E, et al. Alcohol use and its association with HIV risk behaviors among a cohort of patients attending HIV clinical care in Tanzania, Kenya, and Namibia. AIDS Care. 2014;26(10):1288–97.
Scott-Sheldon LA, Carey KB, Carey MP, Cain D, Simbayi LC, Kalichman SC. Alcohol use disorder, contexts of alcohol use, and the risk of HIV transmission among south African male patrons of shebeens. Drug Alcohol Depend. 2014;140:198–204.
Jolley SE, Alkhafaf Q, Hough C, Welsh DA. Presence of an alcohol use disorder is associated with greater pneumonia severity in hospitalized HIV-infected patients. Lung. 2016;194(5):755–62.
Idrisov B, Lunze K, Cheng DM, Blokhina E, Gnatienko N, Quinn E, et al. Role of substance use in HIV care cascade outcomes among people who inject drugs in Russia. Addict Sci Clin Pract. 2017;12(1):30.
Bultum JA, Yigzaw N, Demeke W, Alemayehu M. Alcohol use disorder and associated factors among human immunodeficiency virus infected patients attending antiretroviral therapy clinic at Bishoftu general hospital, Oromiya region, Ethiopia. PLoS ONE. 2018;13(3):e0189312.
Wandera B, Tumwesigye NM, Nankabirwa JI, Kambugu AD, Parkes-Ratanshi R, Mafigiri DK, et al. Alcohol Consumption among HIV-Infected Persons in a Large Urban HIV Clinic in Kampala Uganda: A Constellation of Harmful Behaviors. PLoS One. 2015;10(5):e0126236. https://doi.org/10.1371/journal.
Farley J, Miller E, Zamani A, Tepper V, Morris C, Oyegunle M, et al. Screening for hazardous alcohol use and depressive symptomatology among HIV-infected patients in Nigeria: prevalence, predictors, and association with adherence. J Int Assoc Phys AIDS Care (Chicago, Ill : 2002). 2010;9(4):218–226.
Duko B, Toma A, Abraham Y. Alcohol use disorder and associated factors among individuals living with HIV in Hawassa City, Ethiopia: a facility based cross- sectional study. Subst Abuse Treat Prev Policy. 2019;14:22.
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–5.
Modesti PA, Reboldi G, Cappuccio FP, Agyemang C, Remuzzi G, Rapi S, et al. Panethnic differences in blood pressure in Europe: a systematic review and meta-analysis. PLoS One. 2016;11(1):e0147601.
Borenstein M, Hedges LV, Higgins J, Rothstein HR. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res Synth Methods. 2010;1(2):97–111.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ: British Medical Journal. 2003;327(7414):557.
Sterne JAC, Gavaghan D, Egger M. Publication and related bias in meta-analysis: power of statistical tests and prevalence in the literature. J Clin Epidemiol. 2000;53(11):1119–29.
Reinert DF, Allen JP. The alcohol use disorders identification test (AUDIT): areview of recent research. Alcohol Clin Exp Res. 2002;26(2):272.
Grant BF, Goldstein RB, Saha TD, Chou P, Jung J, Zhang H, et al. Epidemiology of DSM-5 alcohol use disorder: results from the National Epidemiologic Survey on alcohol and related conditions III. JAMA Psychiatry. 2015;72(8):757–66.
Manthey J, Gual A, Jakubczyk A, Pieper L, Probst C, Struzzo P, et al. Alcohol use disorders in Europe: A comparison of general population and primary health care prevalence rates. J Subst Abus. 2016;21(5):478–84.
Louise Mewton, Maree Teesson, Tim Slade, Rachel Grove, The epidemiology of DSM-IV alcohol use disorders amongst young adults in the Australian population, Alcohol Alcohol, Volume 46, Issue 2, March-April 2011, Pages 185–191.
Plant M. The role of alcohol in women’s lives: a review of issues and responses. J Subst Abus. 2008;13(3):155–91.
Urban NB, Kegeles LS, Slifstein M, Xu X, Martinez D, Sakr E, Abi-Dargham A. Sex differences in striatal dopamine release in young adults after oral alcohol challenge: a positron emission tomography imaging study with [11C]raclopride. Biol Psychiatry. 2010;68(8):689–96.
Peralta R. ‘Alcohol allows you to not be yourself’: toward a structured understanding of alcohol use and gender difference among gay and lesbian, and heterosexual youth. The Journal of Drug Issues. 2008;38:373–400.
Mackenzie K, Differences between screening and diagnostic tests and case finding. 2017. https://www.healthknowledge.org.uk/public-health-textbook/disease-causation-diagnostic/2c-diagnosis-screening/screening-diagnostic-case-finding.
Glantz MD, Medina-Mora ME, Petukhova M, Andrade LH, Anthony JC, de Girolamo G, et al. Alcohol abuse in developed and developing countries in the world mental health surveys: socially defined consequences or psychiatric disorder? Am J Addict. 2014;23:145–55.
Acknowledgements
No acknowledgements at this stage.
Funding
The authors declare that there is no funding.
Author information
Authors and Affiliations
Contributions
BD performed the database search, data extraction, quality assessment, analysis, and write-up and drafted the manuscript. MA performed the database search and data extraction. GA performed the database search, conducted analyses, and write-up. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
N/A
Consent for publication
N/A
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
Adapted NOS for Cross-sectional studies.
Additional file 2.
Qualities of included studies in meta-analysis.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Duko, B., Ayalew, M. & Ayano, G. The prevalence of alcohol use disorders among people living with HIV/AIDS: a systematic review and meta-analysis. Subst Abuse Treat Prev Policy 14, 52 (2019). https://doi.org/10.1186/s13011-019-0240-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13011-019-0240-3