
Abstract
Background
The pharmacoepidemiology of the long-term benefits and harms of medicines in pregnancy and breastfeeding has received little attention. The impact of maternal medicines on children is increasingly recognised as a source of avoidable harm. The focus of attention has expanded from congenital anomalies to include less visible, but equally important, outcomes, including cognition, neurodevelopmental disorders, educational performance, and childhood ill-health. Breastfeeding, whether as a source of medicine exposure, a mitigator of adverse effects or as an outcome, has been all but ignored in pharmacoepidemiology and pharmacovigilance: a significant ‘blind spot’.
Whole-population data on breastfeeding: why we need them
Optimal child development and maternal health necessitate breastfeeding, yet little information exists to guide families regarding the safety of medicine use during lactation. Breastfeeding initiation or success may be altered by medicine use, and breastfeeding may obscure the true relationship between medicine exposure during pregnancy and developmental outcomes. Absent or poorly standardised recording of breastfeeding in most population databases hampers analysis and understanding of the complex relationships between medicine, pregnancy, breastfeeding and infant and maternal health. The purpose of this paper is to present the arguments for breastfeeding to be included alongside medicine use and neurodevelopmental outcomes in whole-population database investigations of the harms and benefits of medicines during pregnancy, the puerperium and postnatal period. We review: 1) the current situation, 2) how these complexities might be accommodated in pharmacoepidemiological models, using antidepressants and antiepileptics as examples; 3) the challenges in obtaining comprehensive data.
Conclusions
The scarcity of whole-population data and the complexities of the inter-relationships between breastfeeding, medicines, co-exposures and infant outcomes are significant barriers to full characterisation of the benefits and harms of medicines during pregnancy and breastfeeding. This makes it difficult to answer the questions: ‘is it safe to breastfeed whilst taking this medicine’, and ‘will this medicine interfere with breastfeeding and/ or infants’ development’?
Similar content being viewed by others
Background
Pharmacoepidemiology, pharmacovigilance and the reproductive years
After a medicinal product has been marketed, patient safety depends on accurate population surveillance, pharmacovigilanceglossary—detecting, assessing, and preventing adverse effects, and pharmacoepidemiologyglossary – describing the use and effects of drugs in large numbers of people (Table 1 Glossary has definitions). Pregnant and breastfeeding individuals and their infants should not be excluded from the protection afforded by pharmacovigilance [1]. Neither continuation nor discontinuation of medicines is without risk, but harm can be minimised by effective pharmacovigilance. This depends on comprehensive characterisation of drug-related benefits and harms, and any imbalance. For people of childbearing age, this should include information across the full reproductive life cycle: fertility rates; pregnancy loss; terminations, for all reasons; congenital anomalies; preterm birth; growth centiles; complications of pregnancy; complications of childbirth and the puerperium (e.g. haemorrhage); neonatal complications (pulmonary hypertension, hypoglycaemia, discontinuation syndromes); breastfeeding rates at different ages; infant and childhood outcomes, including cognitive functioning, neurodevelopmental disorders, education performance, long-term conditions, survival and reproductive success [2].
This paper aims to present the arguments for breastfeeding to be included alongside medicines use and neurodevelopmental outcomes in population databases and studies investigating the benefits and harms of medicines during pregnancy, the puerperium and postnatal period. We review:
-
1) the current situation.
-
2) how breastfeeding might be accommodated in pharmacoepidemiological models exploring the impact of medicines on breastfeeding as an outcome and on infants exposed to medicines in utero and via breastmilk.
-
3) the challenges in obtaining comprehensive data.
Breastfeeding and medicines: locating the data and why we need them
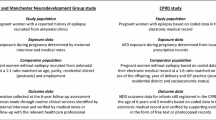
To research the impact of medicine exposure during and after pregnancy on infant development, we shall need population databases linking data on medicine exposure plus breastfeeding plus infant development. Across Europe, few population databases hold data on all three together, and there is little uniformity in outcomes, definitions, methods and timing of assessments, as illustrated in Table 2.
It took 30 years for the dose–response associations between in utero exposure to valproic acid derivatives and altered neurodevelopment trajectories [26], and congenital anomalies [27] to be incorporated into regulatory measures to curtail prescribing during pregnancy [28]. Valproate prescribing to women of childbearing age is declining [29], but, in England, it was prescribed to 247 pregnant women between April 2018 and September 2021 [30]. Subsequently, pharmacoepidemiologists have considered the effects of exposure to other medicines during pregnancy, particularly, antidepressants [31], and opioids [32]. However, although suboptimal breastfeeding is one of the main threats to global health [33], it appears to be a ‘blind spot’ in healthcare databases and pharmacovigilance.
It is rarely possible to obtain the population-wide picture of short- and long-term transgenerational outcomes from clinical trials, case series, spontaneous reports, and cohort studies, due to (largely unavoidable) selection biasglossary [21, 34]. Prospective observational birth cohort studies collect information on infant feeding, but they represent a self-selected sample of the population. For example, cohorts in Norway and Denmark recruited 41% and ~ 30% of the eligible populations [35, 36], whilst other cohorts lack linked prescription [37] or child development data [38]. Pharmacokinetic studies usually involve small numbers of participants, and, like animal studies, may not predict developmental or clinical outcomes [39]. Manufacturers’ medicine-related pregnancy registries capture insufficient data on pregnancy, infant follow-up, and breastfeeding: median (interquartile range) enrolment is reported as 36 (5–258) pregnancies and 12 (2–119) infants [40]. Patient safety researchers are, therefore, examining population databases; however, data quality and validity are not always completely evaluated [41, 42], and most have no data on breastfeeding and neurodevelopment [43, 44].
Breastfeeding
Breastfeeding requires an optimal biopsychosocial milieu [45]. Socioeconomic status (SES) glossary, cultural norms, availability of infant formula, and maternal intention are important, but the impact of prescribed medicines on breastfeeding should not be overlooked [46]. Exposure to some prescription medicines in pregnancy, labour and postpartum, may reduce breastfeeding initiation or continuation [24, 46, 47]. The complex physiology of lactation is vulnerable to disruption, particularly by medicines that affect serotoninergic pathways (including antidepressants) [48, 49], antagonise prolactin (amphetamines, oestrogens, ergotamine derivatives, aripiprazole, promethazine, possibly diuretics, injected corticosteroids), or reduce oxytocin release (alcohol, opioids, possibly sympathomimetics, anticholinergics, antidepressants) [50,51,52,53]. However, we do not know all the reasons underlying the lower breastfeeding rates amongst those using prescription medicines. People may be reluctant to breastfeed if the impact of the medicine on the infant is unknown [54]: doubts, hesitancies, and anxieties may compound physiological difficulties.
Neurodevelopment
Medicine exposure through breastfeeding is an important consideration in analyses of neurodevelopmental outcomes (neurodevelopmental disorders, cognitive performance, educational performance) [55,56,57,58], particularly if prolonged and exclusive [59, 60]. The effect of breastfeeding is demonstrated in many observational studies and a cluster randomised controlled trial of assistance with breastfeeding [61]. Similarly, a meta-analysis of observational studies reports that children with autism are less likely to have been breastfed (OR = 0.61, 95% CI 0.45, 0.83) [57].
Causation is not easily established: infants may be exposed to medicines in utero and/ or via breastmilk, and observational studies cannot discount the possibility that difficulties with breastfeeding, and early discontinuation, are due to neonatal irritability associated with early signs of neurodevelopmental problems [62]. Also, some prescribed medicines (antidepressants, valproic acid derivatives) and high dose alcohol may simultaneously predispose to neonatal irritability [63], and disruption of breastfeeding physiology [48, 64, 65]. Accordingly:
-
Breastfeeding warrants consideration as a health outcome measure, indicating a healthy mother-infant dyad.
-
Those concerned with medicines’ safety in pregnancy and breastfeeding should account for infant feeding when modelling both long- and short-term outcomes.
-
Inter-dependence between medicines and breastfeeding warrants scrutiny, alongside the full range of putative aetiologies of adverse outcomes. Currently, the optimum strategy is uncertain.
How should breastfeeding be accommodated in pharmacoepidemiology?
Without information on breastfeeding, it will be impossible to separate the effect of exposure to medicines in utero and/or during breastfeeding from the effect of ‘not breastfeeding’ for some medicines. Although prescribed medicines and breastfeeding may affect infant development in different ways, information on breastfeeding is needed to understand and minimise adverse outcomes in childhood. With definitions (Table 1 Glossary), examples and explanation of implications, we explore breastfeeding in relation to confounding, mediating, moderating, and colliding [9], and offer diagrammatic illustrations as tentative directed acyclic graphs (DAGs) for discussion [66, 67]. Breastfeeding may be:
-
a)
A confounder, when exploring whether exposure both during and after pregnancy affects the infant, assuming medicines reach the infant in utero and then via breastmilk.
-
b)
A mediator, when exploring how in utero exposure affects neurodevelopment, when medicines may affect initiation or duration of breastfeeding.
-
c)
A moderator, by countering any adverse effects of medicines on neurodevelopment.
-
d)
Vulnerable to colliding and volunteer bias when exploring the effects of medicines on breastfeeding success.
-
e)
Incorporated into a range of statistical models.
Confounding
Definition
The concept of ‘confounding’glossary, based on differences (or non-comparability) between exposed and non-exposed subjects, distinct from ‘selection bias’ glossary, has developed in the last half-century [68]. The definition of confounderglossary most widely adopted is: “a factor associated with both the exposure and the outcome, and not part of the causal pathway from exposure to outcome” [8], blurring effects [7, 69, 70] (Table 1).
All observational studies are vulnerable to confounding [67], including those considering the impact of maternal medicines on infant development. Some confounders are well known e.g., socioeconomic status (SES) glossary; others are known, but accurate information is almost impossible to obtain in fieldwork and routine care e.g., doses of recreational drugs consumed. However, there remain ‘unknown unknowns’ or ‘lurking or latent variablesglossary’ [71], such as local environmental pollution and cultural norms. Without randomisation, researchers can only speculate as to the effects of these unmeasured or unmeasurable confounders [13] on breastfeeding and childhood outcomes, based on knowledge of the data and their own milltir sgwar (communities, where they have lived for generations).
Example
Breastfeeding would be considered a confounder in the analysis of the effect of medicines used both during and after pregnancy on neurodevelopmental outcomes when prescribed medicines do not greatly affect breastfeeding physiology and reach the infant in utero and via breastmilk. Most medicines enter breastmilk in small quantities [39]; therefore, breastfeeding affects both:
-
a)
neurodevelopment directly [57, 61], probably via biological processes and
-
b)
infants’ total medicine exposure during both prenatal and postnatal periods of brain development (Fig. 1).

How does total medicine exposure affect infants’ neurodevelopment? Breastfeeding as a confounder.
In this example, breastfeeding affects both neurodevelopmental outcomes and total exposure to medicines (via the placenta + breastmilk). This relates to postnatal exposure, following prenatal exposure
Implications: infants’ total exposure, including via breastmilk
Identifying associations between infant outcomes and medicine exposure via breastmilk is complicated by variations in medicine transfer from breastmilk to infant, depending on dose, timing of administration and breastfeeding, and supplementary formula feeding. Concentrations of medicines in infant blood samples, as proportions of maternal blood concentrations, vary widely, for example: 28.9% (0.6–90.3%), 17.2% (12.4–22.0%), 21.4% (17.9–24.9%), and 44.2% (35.2–125.3%) (median and full range) for lamotrigine, topiramate, valproic acid, and zonasamide respectively [72]. Similarly, appreciable but variable and unpredictable concentrations of citalopram, sertraline, venlafaxine and metabolites pass into breastmilk [73]. This variation in infant exposure may relate to infants’ ability to metabolise and eliminate medicines. Elimination is compromised in premature or sick infants [39] or if maternal or infant metaboliser or transporter status is unusual [74], suggesting a need for close infant monitoring [75, 76]. Although prenatal antidepressant exposure is reported to adversely affect cognitive development [77,78,79], there are few data on long-term outcomes of exposure via breastmilk [65]. Short-term effects of exposure to psychotropic medicines via breastmilk include sedation, irritability, restlessness, diarrhoea and suboptimal weight gain [80, 81], but how these relate to long-term neurodevelopment is unknown. Current practice recommendations rest on case series, indicating that opioids, clozapine, amisulpride, combinations of central nervous system depressants, amiodarone, oral retinoids, radio-iodine, topical and systemic free iodine, and chemotherapy pass into breastmilk, risking (at least) short-term transgenerational (mother to child) adverse drug reactions (ADRs) glossary following breastmilk exposure [39, 82]. Including breastfeeding in analyses of infant outcomes informs families as to whether the benefits of breastfeeding outweigh the risks of increasing infants’ total dose. Analysis of IQ in children followed to age 6 suggests that there are no disbenefits of breastfeeding for children of mothers using sodium valproate (n = 35), but more data are needed regarding breastfeeding when prescribed phenytoin (n = 36) [83], particularly for rare ADRs, such as methaemoglobinaemia and combination regimens [65]. Larger studies are needed to resolve the dilemma “should those prescribed medicines breastfeed?” (see moderating, below).
Mediating
Definition
Mediation occurs when the exposure is associated with an intermediate variable (the mediator), which is then associated with the outcome [84]. Mediatorsglossary, unlike confounders, lie on the causal pathway between exposure and outcome, and describe how, or even why, an association occurs [85, 86]. Breastfeeding is a mediator when:
-
a) medicines reduce breastfeeding, and then.
-
b) reduction or absence of breastfeeding affects neurodevelopment and health (Fig. 2).

How do medicines in pregnancy affect infants’ neurodevelopment? Breastfeeding as a mediator.
Breastfeeding as a mediator relates largely to prenatal exposure
Mediator effects can be tested by exploring the relationship between exposure and outcome with and without the mediator [13], which is particularly important for breastfeeding after in utero exposure [87].
example
SSRI antidepressant exposure in late pregnancy is associated with reduced breastfeeding rates [88] at birth [89], discharge [90], two [91], and 6–8 weeks [47], and, in some studies, with delayed neurodevelopment, including motor control [92], social behaviours [77], and autistic spectrum disorders [78, 79]. Neurodevelopmental delay following prenatal and perinatal antidepressant use may be due, in part, to the medicines’ effect on breastfeeding, i.e., delay may be mediated (or caused) by reduced breastfeeding caused by medicines.
Implications: infant development
Antidepressants may disrupt the physiology of lactation by delaying alveolar secretary activation from 69 to 86 hours, due to serotonin-dependent changes in tight (inter-cellular) junctions [48] and disruption of local production of serotonin [49, 64]. In addition to direct effects on lactogenesis, SSRI exposure in trimester 3 affects monoamine metabolism and serotonin availability in infants, associated with a dose–response increase in restlessness, tremor, and incoordination [93]. These symptoms, and any neonatal withdrawal symptoms of irritability, may impede latching, making breastfeeding painful and difficult, promoting discontinuation. The same disturbances that increase difficulties with breastfeeding may underlie delays in fine motor development at three years [92] or autistic-like behaviours [77]. Adult insomnia [94] and sleep disorders associated with SSRIs [95] and their effects on mother-infant bonding [96] and breastfeeding may compound any direct effects on lactogenesis.
If absence of breastfeeding contributes to any suboptimal neurodevelopmental outcomes associated with antidepressant exposure, breastfeeding partly mediates the association. Any mediator effects of breastfeeding on development can only be explored where a database collects data on children’s neurodevelopment and medicines and breastfeeding.
Moderating
Definition
Moderatorsglossary affect the strength or direction of the relation between exposure and outcome [13]. Moderators explain when, and under which circumstances, associations occur, and are sometimes used to identify subgroups at risk, e.g., age bands or co-morbidities, where exposure and outcome may be more closely linked than in the full population [84, 97]. Breastfeeding is a moderator if it affects:
-
a) neurodevelopment directly via changes in neuronal architecture, and
-
b) the extent of the impact of prenatal and postnatal medicine use on neurodevelopment.
In regressionglossary analyses, moderating effects are usually tested with interaction variables: if these explain a statistically significant amount of model varianceglossary, moderator (or modification) effects are likely, i.e. associations identified depend on the value of the moderator [84], in this case, breastfeeding.
Example
If breastfeeding is a moderator, the impact of in utero exposure to medicines will depend on whether the infant is breastfed. In cohorts of infants exposed to antiepileptics (AEDs) (valproate, carbamazepine and lamotrigine) in utero, the prevalence of neurodevelopmental difficulties is lower in breastfed than formula-fed infants, despite the additional postnatal exposure [83, 98].
Implications: mitigating in utero exposure
This suggests that breastfeeding might mitigate harm emanating from AEDs or other medicines, and exposures should be explored separately in breastfed and formula-fed infants (Fig. 3). This would inform families regarding the benefits of breastfeeding while using medicines.

Does breastfeeding affect developmental outcomes for infants exposed to maternal medicines? Breastfeeding as a moderator.
Breastfeeding may affect developmental outcomes if infants have been exposed to AEDs prenatally. This relates to prenatal exposure, followed by postnatal use of medicines
Genetic variations might be considered as moderators, defining sub-groups at risk of exposure via breastmilk [72]. Transgenerational adverse outcomes may be confined to genotypes vulnerable to changes in serotoninergic and corticosteroid substrates [99]. Also, CNS depression or sedation in breastfed infants mainly occurs in infants with low activity in blood–brain barrier efflux transporters (P-gp) [74]. Allelic variations in transporter proteins [100], and maternal or infant single nucleotide polymorphisms [101] are rarely recorded at population level, but may define subgroups at risk of ADRs, and should be considered as moderators in a priori subgroup analyses.
Colliding and Volunteer Bias: the case for whole population databases
Colliderglossary and volunteer biasglossary are examples of selection biasglossary, defined as systematic differences between participants and non-participants (Table 1).
Definition
Collider bias is the distorted (induced) association between two or more variables that both affect the likelihood of an individual being included in the dataset (sampled) [102]. A collider is a variable influenced by other variables: for example, when an exposure or risk factorglossary (such as medicines use) and an outcome (such as breastfeeding) both affect the likelihood of being sampled, they “collide”. Similarly, both being a ‘healthcare worker’ (exposure) and having a ‘severe COVID-19 infection’ (outcome) increase the chances of being tested for COVID, and thereby joining the dataset being analysed [102].
Volunteer samples may not represent the less affluent, smokers [21], or people with obesity [5]. Selective or volunteer recruitment and any deficit in representativeness risks collider bias [102]. This occurs when both exposure and outcome (or an antecedent of the outcome) influence recruitment or retention by their relation to volunteering, which then defines the sample [103,104,105]. The resulting collider bias can distort their relationships [102].
Example
Associations between variables may be vulnerable to collider bias [66, 106] if:
-
a)
Breastfeeding and medicine use both affect the selection of study participants, and
-
b)
the study sample over-represents these characteristics, (Fig. 4).

Does volunteer recruitment affect investigation of breastfeeding? Illustration of Collider Bias.
In this example, the outcome is breastfeeding. Its relationship with maternal medicines is influenced by the composition of the sample of women studied. In this example, both breastfeeding and using prescription medicines affected recruitment to the study
Implications: breastfeeding as a study outcome
When exploring the impact of medicines on initiation or duration of breastfeeding, if recruitment were to favour participants who a) were not using medicines, and b) breastfed, these characteristics would be over-represented. This over-representation would distort the sample and generate associations between breastfeeding and ‘no medicines’ that may not appear in the wider (non-volunteer) population [102]. An analogy might be drawn between volunteer bias and the “streetlight effect”: looking for lost items under a lamp-post, because that is the only place where anything can conveniently be seen [107]. Any associations found under the light may be due to colliding and co-existence in the illuminated patch: whilst they are valid in the sample examined, they may not be true in the wider population [102].
Capturing the whole population of a country or region removes volunteer bias, and hence collider bias, because neither exposure nor outcome nor covariatesglossary drive study inclusion. Attempts to account for colliding in the statistical analysis involve untestable assumptions, and it is better to avoid this problem by capturing data on the unselected regional or national population [102]. However, many databases are vulnerable to ‘live birth bias’, as they fail to record miscarriages [108], and infants dying within their first few days may not be linked to population databases [109], which means they do not capture all pregnancies, risking collider bias.
Approaches to analysis
Regressionglossary models can identify associations, for example, between prescription medicines and exclusive formula feeding, but there are more complex questions, such as the inter-relationships between breastfeeding, maternal medicines, and infant development. Multilevel modellingglossary extends regression analysis to account for clustering of individuals, for example by hospital, primary care provider, region, or country. This allows for the possibility that, in any one cluster, exposures may differ, for example, each primary care provider may have an individualised prescribing pattern. Further analytic techniques move beyond regression models to explore causation:
-
Marginal Structural Modelsglossary were designed to accommodate:
-
◦ time-dependent exposure (e.g., one-off medicine administration, changes in treatment or drug absorption throughout pregnancy) and
-
◦ time-varying covariates, such as breastfeeding, that may be both confounders (prenatal plus postnatal exposure) and mediators (prenatal exposure) (above) [110]
-
Where prescription regimens change frequently, analysis depends on modelling assumptions [111]. This approach has, for example, been used to explore associations between breastfeeding, SES and adult health [112], and between breastfeeding, infant deaths and self-reported ethnic group [113].
-
Structural Equation Modelling.glossary offers a framework for theory-driven hypotheses to be tested (or falsified) in a single cohesive model, using large datasets [14, 114, 115]. For example, this approach has been used to explore: the effects of maternal and infant characteristics on breastfeeding techniques and breastfeeding, [116] associations between attention-deficit-hyperactivity disorder (ADHD), obesity and breastfeeding [117], and predictors of infants’ neurodevelopment, including breastfeeding [115]
These’ causal models’ are used where trials would be considered unethical (pregnancy, breastfeeding) or impractical (rare outcomes), and are scarce [118]. However, models cannot accommodate the possibility that omitted variablesglossary may bias associations of interest [112]. In contrast, large trials account for known and unknown confounding variables by randomisation, albeit within the recruited population. Return on investment in analytic techniques will be insufficient without comprehensive data collection.
Getting the full picture: challenges of comprehensive characterisation
Depending on how neurodevelopment is investigated, breastfeeding may be a confounder (when medicines are taken during pregnancy and whilst breastfeeding) or a mediator (when in utero exposure is considered) or a moderator (when defining ‘at risk’ subgroups) or a casualty of volunteer bias (in recruited cohorts). Many investigators consider breastfeeding sufficiently important to be an outcome itself [38], but it may be a casualty of volunteer bias in recruited cohorts [102].
Effective pharmacoepidemiology and pharmacovigilance need not only an understanding of causal pathways and unselected whole-population databases, but also comprehensive characterisation of the full range of variables affecting childhood outcomes [2, 119]. In addition to data on pregnancy dates, outcomes, and exposures to medicines and disease [2], regulators [1] recommend including data on: maternal age; obstetric and medical history; disease status and management; prescription of known teratogenic or foetotoxic medicines; folic acid and multivitamin use; smoking; alcohol intake; illicit drug use (with duration); lifestyle factors (exercise and nutrition); body mass index; and full family history of conditions possibly related to adverse perinatal and neurodevelopmental outcomes [2]. Breastfeeding is included as ‘follow up’ information [1]. Other parametersglossary may be important in determining perinatal and childhood outcomes, for example: SES; parental educational outcomes; infections or inflammation in pregnancy; healthcare contacts (including, but not limited to, antenatal monitoring); vaccinations; rurality [120]; distance from environmental pollutants [121,122,123]; and genetic/ epigenetic influences [101].
Environmental pollutants, including lead, mercury, and dioxins, pass into breastmilk [124] and may increase the risk of sub-optimal growth [125], allergy [126] and neurodevelopmental delay [79, 127]; however, breastfeeding mitigates the impact of prenatal exposure [128]. Organochlorides may reduce lactation [129]. As with medicines, long-term effects of exposure via breastmilk are under-investigated, and databases contain little information.
Inter-relationships between these myriad variables determining childhood outcomes complicate evaluation of co-exposures, and may converge on SESglossary. SES is associated with: breastfeeding status [24, 38, 46]; environmental pollution [130]; health, perinatal, developmental and educational outcomes [131]; morbidity [132]; depression [133]; smoking; substance misuse; and prescription medicines [25, 47], including antidepressant prescribing [24, 38, 46, 134]. Combining these diverse variables into a propensity score risks overlooking individual modifiable risk factors and targets for change, such as prescribing practices or breastfeeding support. Subsuming the impact of ‘not breastfeeding’ under SES allows it to be ‘drowned out’, obscured, and lost to pharmacovigilance.
Deprivationglossary [24, 38, 46], depression pre-pregnancy [47, 135] and antidepressants [47, 89,90,91] all lower breastfeeding rates [88, 136]. Both depression and antidepressants stimulate the hypothalamic–pituitary–adrenal axis, transfer of cortisol to the foetus, and epigenetic changes [137, 138] and their biological effects on neurodevelopment are difficult to disentangle [77]. Exactly how breastfeeding lies on the causal chain between deprivation (low SES) and poor school performance likely varies between individuals. Any impact of prescribed medicines on breastfeeding is of crucial importance, and any disruption of breastfeeding may have far-reaching consequences, as illustrated in Fig. 5.

How is deprivation linked to school performance? A putative causal chain.
School performance is affected by too many inter-related factors to be depicted in a single illustration. This figure illustrates just one scenario: we have prioritised clarity over complexity [103]
The impact of prescribed medicines on reproductive health, childbirth and breastfeeding is not confined to transgenerational ADRs: other adverse effects, such as maternal weight gain, may affect breastfeeding directly or indirectly. For example, weight gain is associated with some antipsychotics, AEDs, antidepressants, and lithium; in turn, obesity complicates monitoring of pregnancy, glycaemic control, and childbirth [139, 140], and increases the risk of preterm birth, congenital anomalies and reduced breastfeeding [141,142,143].
How did we get here? Controlling the databases
The Cumberlege Report states that pharmacovigilance systems failed and are failing pregnant individuals prescribed valproic acid derivatives, due to inability to monitor adverse outcomes [144]( p.4). Congenital anomalies following in utero valproate exposure were reported in 1982 [145] and 1985 [27], but were regarded as isolated cases or attributed to co-prescribing. After accumulation of twenty years’ data from large databases demonstrated an association between in utero sodium valproate exposure and lower IQ, [26] UK authorities issued unequivocal prescribing instructions, in 2018 [28]. A similar argument might be made to address the absence of breastfeeding data. In 1994 and 2001, the American Academy of Paediatrics [146] recommended codeine for short term cough suppression whilst breastfeeding [147]. Codeine had been noted to cause apnoea [148] or sedation [149] in breastfed infants a decade earlier, but was not contra-indicated whilst breastfeeding, until the death of a breastfed infant from codeine exposure was reported in 2005 [150]. This case is controversial [151], but other case series are reported [65], and several opioids are probably harmful via breastmilk [23, 81]. Only one large database study is available [152], and assessment of codeine exposure is complicated by its availability (in low doses) without prescription. Until databases include breastfeeding, risks remain that either some transgenerational ADRs will escape detection or decisions on medicines approvals will be based on case series, with inherent risks of mis-interpretation [151].
To monitor adverse effects, maternal prescription records should be linked to all childhood outcomes and modifiable risk factors [144], and analyses defined explicitly a priori [153]. The usefulness of databases depends on comprehensive coverage, and the nature and detail of their data, including ‘women’s problems’ of miscarriage, pregnancy termination, breastfeeding (extent and duration), and all infections (including those sexually transmitted). Database studies, unlike large clinical trials, cannot rely on randomisation to account for unrecorded variables. Omission or redaction of data constrains examination of potential associations and renders hypotheses unfalsifiable [154] (p.44). Hence, ‘facts’ uncovered by research are dependent on and limited by the processes of inquiry and the zeitgeist of investigators and those establishing and controlling the databases [155, 156]. Any discrimination in data collection may lead to omission of key variables, ‘blind spots’, and obfuscation of transgenerational ADRs. We can only speculate as to reasons for the apparently selective exclusions of crucial variables [144]. Without full transparency, these decisions may be heard as echoes of patriarchal power and its ability to control resources [157], with multi-generational consequences [144].
Limitations of this paper
To our knowledge, this is the first paper to address the complex questions surrounding incorporation of infant feeding data into healthcare databases used to report patient safety. Other research approaches, such as case series, recruited cohorts and randomised trials, and analytical methods are detailed in guidelines [119], and are outside the scope of this discussion; however, concerns over external generalisation remain [21]. For simplicity, our tentative directed acyclic graphs do not offer comprehensive characterisation of the full range of variables affecting childhood outcomes and breastfeeding, listed above [1, 120, 122, 124, 129].
Conclusions
Families need to know whether prescribed medicines will make breastfeeding more difficult and if breastfeeding will leave infants vulnerable to ADRs from maternal medicines or confer benefits, as in the wider population [55,56,57,58,59,60,61]. Current data are inconclusive [44, 158]. Existing regression analyses may offer sufficient evidence to target low-risk interventions to those in most need: for example, records of antidepressant prescriptions in pregnancy should trigger additional breastfeeding support [24, 88, 89]. However, answering complex questions on transgenerational ADRs and how to avoid, monitor and mitigate them, will involve juxtaposition of high-quality linked data on medicines, childhood outcomes and modifiable risk factors, including breastfeeding, in whole-population databases. Comprehensive characterisation and robust analyses of drug-related benefits and harms necessitate information across the life cycle, from miscarriage to fertility of the next generations: breastfeeding should not be a ‘blind spot’.
Abbreviations
- ADR:
-
Adverse drug reaction
- AED:
-
Anti-epileptic drugs
- DAG:
-
Directed acyclic graph
- MeSH:
-
Medical Subject Headings (in PubMed)
- OED:
-
Oxford English Dictionary
- PV:
-
Pharmacovigilance
- SES:
-
Socioeconomic status
- SSRI:
-
Selective serotonin inhibitors (a class of antidepressants)
References
EMA. Guideline on good pharmacovigilance practices (GVP) 3 Product- or Population-Specific Considerations III: Pregnant and 4 breastfeeding women. EMA/653036/2019 DRAFT FOR PUBLIC CONSULTATION EMA, Heads of Medicines agencies 4.12.19, Amsterdam. Available: https://www.ema.europa.eu/en/documents/scientific-guideline/draft-guideline-good-pharmacovigilance-practices-product-population-specific-considerations-iii_en.pdf. Accessed 2 Nov 2020.
Damase-Michel C, Wurst K, et al . Core evidence elements for generating medication safety evidence for pregnancy using population-based data Core data elements, design and analytical foundations ConcePTION-D1.2.pdf (imi-conception.eu). 2021. available: https://www.imi-conception.eu/news-details/?news_id=693].
European Medicines Agency (EMA). Guideline on good pharmacovigilance (GVP) . Module vi – collection, management and submission of reports of suspected adverse reactions to medicinal products. rev 2. 2017.
Sackett D. Bias in analytic research. J Chronic Dis. 1979;32(1–2):51–63.
Munafo MR, Tilling K, Taylor AE, Evans DM, Davey Smith G. Collider scope: When selection bias can substantially influence observed associations. Int J Epidemiol. 2018;47(1):226–35.
Field A. Discovering statistics using SPSS, 4th. edition. London: Sage; 2013.
VanderWeele TJ, Shpitser I. On the definition of a confounder. Ann Stat. 2013;41(1):196–220.
Kahlert J, Gribsholt SB, Gammelager H, Dekkers OM, Luta G. Control of confounding in the analysis phase - an overview for clinicians. Clin Epidemiol. 2017;9:195–204.
Salkind N. Encyclopedia of Research Design. Thousand Oaks, CA: SAGE Publications, Inc.; 2010.
Townsend P, Phillimore P, Beattie A. Health and Deprivation: Inequality and the north. London: Routledge; 1988.
Oxford English Dictionary (OED) Online.
Robins JM, Hernán MA, Brumback B. Marginal structural models and causal inference in epidemiology. Epidemiology. 2000;11(5):550–60. https://doi.org/10.1097/00001648-200009000-00011.
Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–82.
Miles JSM. Applying Regression & Correlation : A guide for students and researchers. Thousand Oaks, Calif: Sage Publications; 2001.
World Health Organization. The importance of pharmacovigilance, safety monitoring of medicinal products. Geneva: World Health Organisation; 2002.
Offord D, Kraemer H. Risk factors and prevention. Evid Based Ment Health. 2000;3:70–1.
PubMed MeSH database: Selection bias. 1990.
Krieger N, Williams D, Moss N. Measuring social class in us public health research: Concepts, methodologies, and guidelines. Annu Rev Public Health. 1997;18:341–18378.
Galobardes B, Shaw M, Lawlor DA, Lynch JW, Davey Smith G. Indicators of socioeconomic position (part 1). J Epidemiol Community Health. 2006;60(1):7–12. https://doi.org/10.1136/jech.2004.023531.
Altman D. Practical Statistics for Medical Research. London: Chapman & Hall; 1991.
Jordan S, Watkins A, Storey M, Allen SJ, Brooks CJ, Garaiova I, et al. Volunteer bias in recruitment, retention, and blood sample donation in a randomised controlled trial involving mothers and their children at six months and two years: A longitudinal analysis. PLoS ONE. 2013;8(7):e67912.
Lacroix I, Hurault C, Sarramon M, Guitard C, Berrebi A, Grau M, et al. Prescription of drugs during pregnancy: A study using EFEMERIS, the new french database. Eur J Clin Pharmacol. 2009;65(8):839–46.
Soussan C, Gouraud A, Portolan G, Jean-Pastor MJ, Pecriaux C, Montastruc JL, et al. Drug-induced adverse reactions via breastfeeding: A descriptive study in the French pharmacovigilance database. Eur J Clin Pharmacol. 2014;70(11):1361–6.
Jordan S, Emery S, Watkins A, Evans JD, Storey M, Morgan G. Associations of drugs routinely given in labour with breastfeeding at 48 hours: Analysis of the cardiff births survey. BJOG. 2009;116(12):1622–9.
Davies G, Jordan S, Thayer D, Tucker D, Humphreys I. Medicines prescribed for asthma, discontinuation and perinatal outcomes, including breastfeeding: A population cohort analysis. PLoS ONE. 2020;15(12):e0242489.
Bromley R, Weston J, Adab N, Greenhalgh J, Sanniti A, McKay AJ, et al. Treatment for epilepsy in pregnancy: Neurodevelopmental outcomes in the child. Cochrane Database Syst Rev. 2014;2014(10):CD010236.
Garden AS, Benzie RJ, Hutton EM, Gare DJ. Valproic acid therapy and neural tube defects. Can Med Assoc J. 1985;132(8):933, 936.
Drug Safety Update 2018[https://www.gov.uk/drug-safety-update/valproate-pregnancy-prevention-programme-actions-required-now-from-gps-specialists-and-dispensers ]
Hurault-Delarue C, Morris JK, Charlton R, Gini R, Loane M, Pierini A, et al. Prescription of antiepileptic medicines including valproate in pregnant women: A study in three european countries. Pharmacoepidemiol Drug Saf. 2019;28(11):1510–8.
Medicines and pregnancy registry: Antiepileptic use in females aged 0 to 54 in england: April 2018 to September 2021 NHS Digital 2022[https://digital.nhs.uk/data-and-information/publications/statistical/mi-medicines-and-pregnancy-registry/antiepileptic-use-in-females-aged-0-to-54-in-england-april-2018-to-september-2021]
Morales DR, Slattery J, Evans S, Kurz X. Antidepressant use during pregnancy and risk of autism spectrum disorder and attention deficit hyperactivity disorder: Systematic review of observational studies and methodological considerations. BMC Med. 2018;16:6.
Cook MN, Olshan AF, Guess HA, Savitz DA, Poole C, Blatt J, et al. Maternal medication use and neuroblastoma in offspring. Am J Epidemiol. 2004;159(8):721–31.
Lawn JE, Blencowe H, Oza S, You D, Lee AC, Waiswa P, et al. Every newborn: Progress, priorities, and potential beyond survival. Lancet. 2014;384(9938):189–205.
Sackett D. Bias in analytical research. J Chronic Dis. 1979;32:51–63.
Lund-Blix NA, Dydensborg Sander S, Stordal K, Nybo Andersen AM, Ronningen KS, Joner G, et al. Infant feeding and risk of type 1 diabetes in two large scandinavian birth cohorts. Diabetes Care. 2017;40(7):920–7.
Olsen J, Melbye M, Olsen SF, Sørensen TI, Aaby P, Nybo Andersen A-M, et al. The danish national birth cohort-its background, structure and aim. Scand J Public Health. 2001;29(4):300–7.
Fraser A, Macdonald-Wallis C, Tilling K, Boyd A, Golding J, Davey Smith G, et al. Cohort profile: The Avon Longitudinal Study of Parents and Children: ALSPAC mothers cohort. Int J Epidemiol. 2013;42(1):97–110.
McAndrew F, Thompson J, Fellows L, Large A, Speed M, Renfrew M. The infant feeding survey 2010. In. Edited by NHS Information Centre for Health and Social Care. London: Office of National Statistics; 2012.
Verstegen RHJ, Anderson PO, Ito S. Infant drug exposure via breast milk. Br J Clin Pharmacol. 2020;1–17. https://doi.org/10.1111/bcp.14538.
Bird ST, Gelperin K, Taylor L, Sahin L, Hammad H, Andrade SE, et al. Enrollment and retention in 34 united states pregnancy registries contrasted with the manufacturer’s capture of spontaneous reports for exposed pregnancies. Drug Saf. 2018;41(1):87–94.
Rawson NSB, D’Arcy C. Healthcare databases for drug safety research: Data validity assessment remains crucial. Drug Saf. 2018;41(9):829–33.
Pacurariu A, Plueschke K, McGettigan P, Morales DR, Slattery J, Vogl D, et al. Electronic healthcare databases in europe: Descriptive analysis of characteristics and potential for use in medicines regulation. BMJ Open. 2018;8(9):e023090.
Coathup V, Boyle E, Carson C, Johnson S, Kurinzcuk JJ, Macfarlane A, et al. Gestational age and hospital admissions during childhood: Population based, record linkage study in england (tigar study). BMJ. 2020;371:m4075.
Roque Pereira L, Durán CE, Layton D, Poulentzas G, Lalagkas P-N, Kontogiorgis C, et al. A landscape analysis of post-marketing studies registered in the eu pas register and clinicaltrials. Gov focusing on pregnancy outcomes or breastfeeding effects: A contribution from the conception project. Drug Safety. 2022;45(4):333–44.
Llorente-Pulido S, Custodio E, Lopez-Gimenez MR, Sanz-Barbero B, Otero-Garcia L. Barriers and facilitators for exclusive breastfeeding in women’s biopsychosocial spheres according to primary care midwives in tenerife (canary islands, spain). Int J Environ Res Public Health. 2021;18(7):3819.
Jordan S, Emery S, Bradshaw C, Watkins A, Friswell W. The impact of intrapartum analgesia on infant feeding. BJOG. 2005;112(7):927–34.
Jordan S, Davies GI, Thayer DS, Tucker D, Humphreys I. Antidepressant prescriptions, discontinuation, depression and perinatal outcomes, including breastfeeding: A population cohort analysis. PLos One. 2019;14(11):e0225133.
Marshall AM, Nommsen-Rivers LA, Hernandez LL, Dewey KG, Chantry CJ, Gregerson KA, et al. Serotonin transport and metabolism in the mammary gland modulates secretory activation and involution. J Clin Endocrinol Metab. 2010;95(2):837–46.
Nyarady K, Turai R, Funke S, Gyorgyi E, Makai A, Premusz V, et al. Effects of perinatal factors on sirtuin 3, 8-hydroxy-2’- deoxyguanosine, brain-derived neurotrophic factor and serotonin in cord blood and early breast milk: An observational study. Int Breastfeed J. 2020;15:57.
Whitley J, Wouk K, Bauer AE, Grewen K, Gottfredson NC, Meltzer-Brody S, et al. Oxytocin during breastfeeding and maternal mood symptoms. Psychoneuroendocrinology. 2020;113:104581.
Lawrence R, Schaefer C, et al. General commentary on drug therapy and drug risk during lactation. In: Schefer C, et al., editors. Drugs during Pregnancy and Lactation. 3rd ed. Amsterdam: Elsevier; 2015. p. 637–48.
Anderson P. Drugs that suppress lactation, part 1. Breastfeed Med. 2017;12:128–30.
Anderson P. Drugs that suppress lactation, part 2. Breastfeed Med. 2017;12:199–201.
Saha M, Ryan K, Amir L. Postpartum women’s use of medicines and breastfeeding practices: A systematic review. Int Breastfeed J. 2015;10:28.
Victora C, Bahl R, Barros A, França G, Horton S, Krasevec J, et al. Breastfeeding series group. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387:475–90.
Ghozy S, Tran L, Naveed S, Quynh TTH, Helmy Zayan A, Waqas A, et al. Association of breastfeeding status with risk of autism spectrum disorder: A systematic review, dose-response analysis and meta-analysis. Asian J Psychiatr. 2020;48:101916101916.
Tseng PT, Chen YW, Stubbs B, Carvalho AF, Whiteley P, Tang CH, et al. Maternal breastfeeding and autism spectrum disorder in children: A systematic review and meta-analysis. Nutr Neurosci. 2019;22(5):354–62.
Boucher O, Julvez J, Guxens M, Arranz E, Ibarluzea J, Sanchez de Miguel M, et al. Association between breastfeeding duration and cognitive development, autistic traits and adhd symptoms: A multicenter study in spain. Pediatr Res. 2017;81(3):434–42.
Belfort MB, Rifas-Shiman SL, Kleinman KP, Guthrie LB, Bellinger DC, Taveras EM, et al. Infant feeding and childhood cognition at ages 3 and 7 years: Effects of breastfeeding duration and exclusivity. JAMA Pediatr. 2013;167(9):836–44.
Blomkvist EAM, Hillesund ER, Helland SH, Simhan I, Overby NC. Diet and neurodevelopmental score in a sample of one-year-old children-a cross-sectional study. Nutrients. 2019;11(7):1676.
Kramer MS, Aboud F, Mironova E, Vanilovich I, Platt RW, Matush L, et al. Breastfeeding and child cognitive development: New evidence from a large randomized trial. Arch Gen Psychiatry. 2008;65(5):578–84.
Miike T, Toyoura M, Tonooka S, Konishi Y, Oniki K, Saruwatari J, et al. Neonatal irritable sleep-wake rhythm as a predictor of autism spectrum disorders. Neurobiol Sleep Circadian Rhythms. 2020;9:100053.
Rotem-Kohavi N, Oberlander TF. Variations in neurodevelopmental outcomes in children with prenatal ssri antidepressant exposure. Birth Defects Res. 2017;109(12):909–23.
Weaver SR, Fricke HP, Xie C, Lipinski RJ, Vezina CM, Charles JF, et al. Peripartum fluoxetine reduces maternal trabecular bone after weaning and elevates mammary gland serotonin and pthrp. Endocrinology. 2018;159(8):2850–62.
LACTMED. Drugs and lactation database (Lactmed). In.: Bethesda (MD): National Library of Medicine (US); 2006.
Kincaid H. Causal modeling, mechanism, and probability in epidemiology. In: McKay Illari P, Russo F, Williamson J, editors. Causality in the Sciences. Oxford: Oxford University Press; 2011. p. 170–90.
Suzuki E, Shinozaki T, Yamamoto E. Causal diagrams: Pitfalls and tips. J Epidemiol. 2020;30(4):153–62.
Morabia A. History of the modern epidemiological concept of confounding. J Epidemiol Community Health. 2011;65(4):297–300.
Rothman K, Greenland S. Modern Epidemiology. 2nd ed. Philadelphi: Lippincott-Raven; 1998.
Schulz K, Grimes D. The Lancet Handbook of Essential Concepts in Clinical Research. Edinburgh: Elsevier; 2006.
Draper N, Smith H. Applied Regression Analysis, 3rd ed. Chichester: Wiley; 1998.
Birnbaum AK, Meador KJ, Karanam A, Brown C, May RC, Gerard EE, et al. Antiepileptic drug exposure in infants of breastfeeding mothers with epilepsy. JAMA Neurol. 2020;77(4):441–50.
Schoretsanitis G, Westin AA, Stingl JC, Deligiannidis KM, Paulzen M, Spigset O. Antidepressant transfer into amniotic fluid, umbilical cord blood & breast milk: A systematic review & combined analysis. Prog Neuropsychopharmacol Biol Psychiatry. 2021;107:110228.
Sistonen J, Madadi P, Ross CJ, Yazdanpanah M, Lee JW, Landsmeer ML, et al. Prediction of codeine toxicity in infants and their mothers using a novel combination of maternal genetic markers. Clin Pharmacol Ther. 2012;91(4):692–9.
Sprague J, Wisner KL, Bogen DL. Pharmacotherapy for depression and bipolar disorder during lactation: A framework to aid decision making. Semin Perinatol. 2020;44(3):151224.
Amir LH, Ryan KM, Jordan SE. Avoiding risk at what cost? Putting use of medicines for breastfeeding women into perspective. Int Breastfeed J. 2012;7(1):14.
Gemmel M, Bogi E, Ragan C, Hazlett M, Dubovicky M, van den Hove DL, et al. Perinatal selective serotonin reuptake inhibitor medication (SSRI) effects on social behaviors, neurodevelopment and the epigenome. Neurosci Biobehav Rev. 2018;85:102–16.
Sujan AC, Rickert ME, Oberg AS, Quinn PD, Hernandez-Diaz S, Almqvist C, et al. Associations of maternal antidepressant use during the first trimester of pregnancy with preterm birth, small for gestational age, autism spectrum disorder, and attention-deficit/hyperactivity disorder in offspring. JAMA. 2017;317(15):1553–62.
Emberti Gialloreti L, Mazzone L, Benvenuto A, Fasano A, Alcon AG, Kraneveld A, et al. Risk and protective environmental factors associated with autism spectrum disorder: Evidence-based principles and recommendations. J Clin Med. 2019;8(2):217.
Merlob P, Schaefer C. Psychotropic drugs. In: Schaefer C, Peters P, Miller R, editors. Drugs during Pregnancy and. Lactation. London: Academic Press/ Elsevier; 2015. p. 743–74.
Anderson PO, Sauberan JB. Modeling drug passage into human milk. Clin Pharmacol Ther. 2016;100(1):42–52.
Anderson PO, Manoguerra AS, Valdes V. A review of adverse reactions in infants from medications in breastmilk. Clin Pediatr (Phila). 2016;55(3):236–44.
Meador KJ, Baker GA, Browning N, Cohen MJ, Bromley RL, Clayton-Smith J, et al. Breastfeeding in children of women taking antiepileptic drugs: Cognitive outcomes at age 6 years. JAMA Pediatr. 2014;168(8):729–36.
Bennett JA. Mediator and moderator variables in nursing research: Conceptual and statistical differences. Res Nurs Health. 2000;23(5):415–20.
Hernan MA. The c-word: Scientific euphemisms do not improve causal inference from observational data. Am J Public Health. 2018;108(5):616–9.
Petersen ML, van der Laan MJ. Causal models and learning from data: Integrating causal modeling and statistical estimation. Epidemiology. 2014;25(3):418–26.
Groenwold RHH, Palmer TM, Tilling K. To adjust or not to adjust? When a “confounder” is only measured after exposure. Epidemiology. 2021;32(2):194–201.
Anderson PO. Antidepressants and breastfeeding. Breastfeed Med. 2021;16(1):5–7.
Grzeskowiak LE, Saha MR, Nordeng H, Ystrom E, Amir LH. Perinatal antidepressant use and breastfeeding outcomes: Findings from the Norwegian mother, father and child cohort study. Acta Obstet Gynecol Scand. 2022;101(3):344–54.
Venkatesh K, Castro V, Perlis R. Impact of antidepressant treatment during pregnancy on obstetric outcomes among women previously treated for depression: An observational cohort study. J Perinatol. 2017;37:1003–9.
Gorman J, Kao K, Chambers C. Breastfeeding among women exposed to antidepressants during pregnancy. J Hum Lact. 2012;28:181–8.
Handal M, Skurtveit S, Furu K, Hernandez-Diaz S, Skovlund E, Nystad W, et al. Motor development in children prenatally exposed to selective serotonin reuptake inhibitors: A large population-based pregnancy cohort study. BJOG. 2016;123(12):1908–17.
Laine K, Heikkinen T, Ekblad U, Kero P. Effects of exposure to selective serotonin reuptake inhibitors during pregnancy on serotonergic symptoms in newborns and cord blood monoamine and prolactin concentrations. Arch Gen Psychiatry. 2003;60(7):720–6.
Quagliato LA, Cosci F, Shader RI, Silberman EK, Starcevic V, Balon R, et al. Selective serotonin reuptake inhibitors and benzodiazepines in panic disorder: A meta-analysis of common side effects in acute treatment. J Psychopharmacol. 2019;33(11):1340–51.
Joint Formulary Committee. Bnf 80: September 2020-march 2021. London: Pharmaceutical Press; 2020.
Tikotzky L. Postpartum maternal sleep, maternal depressive symptoms and self-perceived mother-infant emotional relationship. Behav Sleep Med. 2016;14(1):5–22.
Mackinnon DP. Integrating mediators and moderators in research design. Res Soc Work Pract. 2011;21(6):675–81.
Veiby G, Engelsen BA, Gilhus NE. Early child development and exposure to antiepileptic drugs prenatally and through breastfeeding: A prospective cohort study on children of women with epilepsy. JAMA Neurol. 2013;70(11):1367–74.
Hilli J, Heikkinen T, Rontu R, Lehtimaki T, Kishida I, Aklillu E, et al. Mao-a and comt genotypes as possible regulators of perinatal serotonergic symptoms after in utero exposure to ssris. Eur Neuropsychopharmacol. 2009;19(5):363–70.
Daud AN, Bergman JE, Bakker MK, Wang H, de Walle HE, Plosch T, et al. Pharmacogenetics of drug-induced birth defects: The role of polymorphisms of placental transporter proteins. Pharmacogenomics. 2014;15(7):1029–41.
Nembhard W, Tang X, Hu Z, MacLeod S, Stowe Z, Webber D. Maternal and infant genetic variants, maternal periconceptional use of selective serotonin reuptake inhibitors, and risk of congenital heart defects in offspring: Population based study. BMJ. 2017;356:j832.
Griffith GJ, Morris TT, Tudball MJ, Herbert A, Mancano G, Pike L, et al. Collider bias undermines our understanding of covid-19 disease risk and severity. Nat Commun. 2020;11(1):5749.
Cole SR, Platt RW, Schisterman EF, Chu H, Westreich D, Richardson D, et al. Illustrating bias due to conditioning on a collider. Int J Epidemiol. 2010;39(2):417–20.
Lee H, Aronson JK, Nunan D. Collider bias. In: Catalogue of bias collaboration. 2019. https://catalogofbias.org/biases/collider-bias/.
Yan R, Liu T, Peng Y, Peng X. Can statistical adjustment guided by causal inference improve the accuracy of effect estimation? A simulation and empirical research based on meta-analyses of case-control studies. BMC Med Inform Decis Mak. 2020;20:333.
Elwert F, Winship C. Endogenous selection bias: The problem of conditioning on a collider variable. Annu Rev Sociol. 2014;40:31–53.
Battaglia M, Atkinson MA. The streetlight effect in type 1 diabetes. Diabetes. 2015;64(4):1081–90.
Huybrechts KF, Bateman BT, Hernández-Díaz S. Use of real-world evidence from healthcare utilization data to evaluate drug safety during pregnancy. Pharmacoepidemiol Drug Saf. 2019;28(7):906–22.
Loane M, Given JE, Tan J, Reid A, Akhmedzhanova D, Astolfi G, et al. Linking a european cohort of children born with congenital anomalies to vital statistics and mortality records: A Eurolinkcat study. PLoS ONE. 2021;16(8):e0256535.
Pazzagli L, Linder M, Zhang M, Vago E, Stang P, Myers D, et al. Methods for time-varying exposure related problems in pharmacoepidemiology: An overview. Pharmacoepidemiol Drug Saf. 2018;27(2):148–60.
Shinozaki T, Suzuki E. Understanding marginal structural models for time-varying exposures: Pitfalls and tips. J Epidemiol. 2020;30(9):377–89.
McDade TW, Koning SM. Early origins of socioeconomic inequalities in chronic inflammation: Evaluating the contributions of low birth weight and short breastfeeding. Soc Sci Med. 2021;269:113592.
Naimi AI, Schnitzer ME, Moodie EE, Bodnar LM. Mediation analysis for health disparities research. Am J Epidemiol. 2016;184(4):315–24.
Rappaport LM, Amstadter AB, Neale MC. Model fit estimation for multilevel structural equation models. Struct Equ Modeling. 2020;27(2):318–29.
Park S, Bellinger DC, Adamo M, Bennett B, Choi NK, Baltazar PI, et al. Mechanistic pathways from early gestation through infancy and neurodevelopment. Pediatrics. 2016;138(6):e20161843.
Lau Y, Htun TP, Lim PI, Ho-Lim S, Klainin-Yobas P. Maternal, infant characteristics, breastfeeding techniques, and initiation: Structural equation modeling approaches. PLoS ONE. 2015;10(11):e0142861.
Turkoglu S, Bilgic A, Akca OF. ADHD symptoms, breast-feeding and obesity in children and adolescents. Pediatr Int. 2015;57(4):546–51.
Middleton JC, Stuebe A, Berkman N, Goulding AN, McLaurin-Jiang S, et al. Maternal, fetal, and child outcomes of mental health treatments in women: A systematic review of perinatal pharmacologic interventions. 2021.
The European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (ENCePP). Guide on Methodological Standards in Pharmacoepidemiology (Revision 10). EMA/95098/2010. Available at http://www.encepp.eu/standards_and_guidance.
Blakey K, Feltbower RG, James PW, Libby G, Stiller C, Norman P, et al. Socio-economic patterning in early mortality of patients aged 0–49 years diagnosed with primary bone cancer in great britain, 1985–2008. Cancer Epidemiol. 2018;53:49–55.
Dolk H, Vrijheid M, Armstrong B, Abramsky L, Bianchi F, Garne E, et al. Risk of congenital anomalies near hazardous-waste landfill sites in europe: The eurohazcon study. Lancet. 1998;352(9126):423–7.
Kihal-Talantikite W, Zmirou-Navier D, Padilla C, Deguen S. Systematic literature review of reproductive outcome associated with residential proximity to polluted sites. Int J Health Geogr. 2017;16(1):20.
Cheng J, Eskenazi B, Widjaja F, Cordero JF, Hendren RL. Improving autism perinatal risk factors: A systematic review. Med Hypotheses. 2019;127:26–33.
Pajewska-Szmyt M, Sinkiewicz-Darol E, Gadzala-Kopciuch R. The impact of environmental pollution on the quality of mother’s milk. Environ Sci Pollut Res Int. 2019;26(8):7405–27.
Grandjean P, Budtz-Jorgensen E, Steuerwald U, Heinzow B, Needham LL, Jorgensen PJ, et al. Attenuated growth of breast-fed children exposed to increased concentrations of methylmercury and polychlorinated biphenyls. FASEB J. 2003;17(6):699–701.
Grandjean P, Poulsen LK, Heilmann C, Steuerwald U, Weihe P. Allergy and sensitization during childhood associated with prenatal and lactational exposure to marine pollutants. Environ Health Perspect. 2010;118(10):1429–33.
Kao CC, Que DE, Bongo SJ, Tayo LL, Lin YH, Lin CW, et al. Residue levels of organochlorine pesticides in breast milk and its associations with cord blood thyroid hormones and the offspring’s neurodevelopment. Int J Environ Res Public Health. 2019;16(8):1438.
Dorea JG. Exposure to environmental neurotoxic substances and neurodevelopment in children from Latin America and the Caribbean. Environ Res. 2021;192:110199.
Rogan WJ, Gladen BC, McKinney JD, Carreras N, Hardy P, Thullen J, et al. Polychlorinated biphenyls (PCBs) and dichlorodiphenyl dichloroethene (DDE) in human milk: Effects on growth, morbidity, and duration of lactation. Am J Public Health. 1987;77(10):1294–7.
Appleton AA, Holdsworth EA, Kubzansky LD. A systematic review of the interplay between social determinants and environmental exposures for early-life outcomes. Curr Environ Health Rep. 2016;3(3):287–301.
Ruiz M, Goldblatt P, Morrison J, Kukla L, Svancara J, Riitta-Jarvelin M, et al. Mother’s education and the risk of preterm and small for gestational age birth: A drivers meta-analysis of 12 european cohorts. J Epidemiol Community Health. 2015;69(9):826–33.
Lewis KM, Ruiz M, Goldblatt P, Morrison J, Porta D, Forastiere F, et al. Mother’s education and offspring asthma risk in 10 european cohort studies. Eur J Epidemiol. 2017;32(9):797–805.
Hein A, Rauh C, Engel A, Haberle L, Dammer U, Voigt F, et al. Socioeconomic status and depression during and after pregnancy in the franconian maternal health evaluation studies (frames). Arch Gynecol Obstet. 2014;289(4):755–63.
Jordan S, Charlton R, Tingay K, Thayer D, Davies G, Morgan M et al. Ssri use in pregnancy: A study in 6 European databases. Abstracts from the Marce society conference. Arch womens ment health. In: The International Marcé Society For Perinatal Mental Health Biennial Scientific Conference: 2015. vol. 8. Swansea: Swansea University; 2015;18:269–408.
Wallenborn JT, Joseph AC, Graves WC, Masho SW. Prepregnancy depression and breastfeeding duration: A look at maternal age. J Pregnancy. 2018;2018:4825727.
Galbally M, Watson SJ, Boyce P, Nguyen T, Lewis AJ. The mother, the infant and the mother-infant relationship: What is the impact of antidepressant medication in pregnancy. J Affect Disord. 2020;272:363–70.
Gentile S, Fusco ML. Placental and fetal effects of antenatal exposure to antidepressants or untreated maternal depression. J Matern Fetal Neonatal Med. 2017;30(10):1189–99.
Kendall-Tackett K, Hale TW. The use of antidepressants in pregnant and breastfeeding women: A review of recent studies. J Hum Lact. 2010;26(2):187–95.
Petersen I, Sammon CJ, McCrea RL, Osborn DPJ, Evans SJ, Cowen PJ, et al. Risks associated with antipsychotic treatment in pregnancy: Comparative cohort studies based on electronic health records. Schizophr Res. 2016;176(2–3):349–56.
Ellfolk M, Leinonen MK, Gissler M, Lahesmaa-Korpinen AM, Saastamoinen L, Nurminen ML, et al. Second-generation antipsychotics and pregnancy complications. Eur J Clin Pharmacol. 2020;76(1):107–15.
Rankin J, Tennant PW, Stothard KJ, Bythell M, Summerbell CD, Bell R. Maternal body mass index and congenital anomaly risk: A cohort study. Int J Obes (Lond). 2010;34(9):1371–80.
Marchi J, Berg M, Dencker A, Olander EK, Begley C. Risks associated with obesity in pregnancy, for the mother and baby: A systematic review of reviews. Obes Rev. 2015;16(8):621–38.
Ballesta-Castillejos A, Gomez-Salgado J, Rodriguez-Almagro J, Ortiz-Esquinas I, Hernandez-Martinez A. Relationship between maternal body mass index with the onset of breastfeeding and its associated problems: An online survey. Int Breastfeed J. 2020;15:55.
IMMDS, Cumberlege J. First do no harm – the report of the independent medicines and medical devices safety review. 2020. ISBN 978-1-5272-6567-7. https://www.immdsreview.org.uk/Report.html.
Robert E, Guibaud P. Maternal valproic acid and congenital neural tube defects. Lancet. 1982;2(8304):937.
American Academy of Pediatrics Committee on Drugs. Transfer of drugs and other chemicals into human milk. Pediatrics. 1994;93:137–50.
Mitchell J. Use of cough and cold preparations during breastfeeding. J Hum Lact. 1999;15(4):347–9.
Davis J, Bhutani V. Neonatal apnea and maternal codeine use. Develop Pharma. 1985;170A:389.
Ito S, Blajchman A, Stephenson M, Eliopoulos C, Koren G. Prospective follow-up of adverse reactions in breast-fed infants exposed to maternal medication. Am J Obstet Gynecol. 1993;168(5):1393–9.
Koren G, Cairns J, Chitayat D, Gaedigk A, Leeder SJ. Pharmacogenetics of morphine poisoning in a breastfed neonate of a codeine-prescribed mother. Lancet. 2006;368(9536):704.
Zipursky J, Juurlink DN. The implausibility of neonatal opioid toxicity from breastfeeding. Clin Pharmacol Ther. 2020;108(5):964–70.
Juurlink DN, Gomes T, Guttmann A, Hellings C, Sivilotti ML, Harvey MA, et al. Postpartum maternal codeine therapy and the risk of adverse neonatal outcomes: A retrospective cohort study. Clin Toxicol (Phila). 2012;50(5):390–5.
Luijken K, Dekkers OM, Rosendaal FR, Groenwold RHH. Exploratory analyses in aetiologic research and considerations for assessment of credibility: Mini-review of literature. BMJ. 2022;377:e070113.
Popper K. The Logic of Scientific Discovery. London: Hutchinson; 1959.
Dewey J. How We Think. Boston: Heath and Co; 1909.
Russell B. History of Western Philosophy. 2nd ed. New York: Allen and Unwin; 1961.
Suliman N. The intertwined relationship between power and patriarchy: Examples from resource extractive industries. Societies. 2019;9:14.
Pacchiarotti I, Leon-Caballero J, Murru A, Verdolini N, Furio MA, Pancheri C, et al. Mood stabilizers and antipsychotics during breastfeeding: Focus on bipolar disorder. Eur Neuropsychopharmacol. 2016;26(10):1562–78.
Acknowledgements
We should like to thank the representatives of the registries and databases in Finland, Scotland and Tuscany for supplying information on the availability of key data in their organisations.
Funding
This work has been undertaken under the auspices of the ConcePTION project. The ConcePTION project has received funding from the Innovative Medicines Initiative 2 Joint Undertaking under grant agreement No 821520. This Joint Undertaking receives support from the European Union’s Horizon 2020 research and innovation programme and EFPIA. Funding was awarded to SJ, HD, ML, GJ, RB, CDM. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors have declared that no competing interests exist.

Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jordan, S., Bromley, R., Damase-Michel, C. et al. Breastfeeding, pregnancy, medicines, neurodevelopment, and population databases: the information desert. Int Breastfeed J 17, 55 (2022). https://doi.org/10.1186/s13006-022-00494-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13006-022-00494-5