
Abstract
Background
Bimaxillary surgery is often performed for class III malocclusion, and its complex influence on the upper airway has been well considered. The aim of this research was to provide a scaled formula between upper airway volume changes and bone movements in Class III patients after orthognathic surgery.
Materials and methods
Using a retrospective study design, the investigators enrolled a total of 30 class III malocclusion patients who were undergoing bimaxillary surgery as the study subjects. The subjects included 15 males and 15 females, and their average age was 23.3 ± 3.4 years. CBCT (cone beam tomography) was performed both before and one year after the surgery for each patient. The changes in the soft palate, tongue and upper airway were measured by using CBCT data that was collected before and after surgery. 3D superimposition of CBCT was performed to calculate three-dimensional jaw movements. A multiple regression analysis was used to calculate the quantitative relationship between airway volume changes and jaw movements.
Results
The nasopharynx airway volume was observed to be increased by 1064.0 ± 1336.2 mm3, whereas the retropalatal and retroglossal airway volumes were observed to be decreased by 1399.0 ± 2881.6 mm3 and 1433.8 ± 3043.4 mm3, respectively, after the surgery. One millimetre forward and downward movements of the PNS resulted in increases of 626.90 mm3 and 392.18 mm3 in nasopharynx airway volume, respectively. Moreover, one millimetre retrogression of the B point caused decreases of 314.6 mm3 and 656.6 mm3 in the retropalatal and retroglossal airway volume, respectively. The changes in the soft palate contributed to the decrease in the retropalatal airway volume, whereas the tongue compensated for the decrease in the retroglossal airway volume.
Conclusion
The movements of the PNS and B points could be used to predict upper airway volumetric changes in Class III patients after maxillary advancement and mandibular setback.
Similar content being viewed by others

Background
Orthognathic surgery is well accepted for patients with skeletal Class III deformities, due to its improvements in facial appearance, mastication function and long-term stability [1]. However, it was recently found that large-scale backwards movement of the mandible may have a negative impact on the airway space [2,3,4,5]. The volume reduction of the pharyngeal airway causes increasing concerns because it is considered to be one of the aetiologies of OSA (obstructive sleep apnea) [6]. Additionally, postoperative airway changes are especially considered by oral surgeons when developing the surgery plan.
The complexity of Class III orthognathic surgery involves the fact that maxillary advancement leads to the widening of the upper airway [7, 8], whereas mandible setback results in the narrowing of the upper airway [9,10,11]. In the real world, the amount of jaw movement and airway changes can vary greatly among different patients. Many previous studies have described airway changes after specific operation methods, but little research has been conducted on the relationship between airway changes and the amount of bone movement [12]. In fact, the quantitative relationship between airway changes and bone movements may be more helpful for surgeons in deciding the surgery design.
In reports about long-term postoperative airway changes, postoperative airway remodelling has been observed to be a gradual process that changes with time [13]. This is supported by evidence that the airway space decreases in the first few months but recovers after a period of time [11]. The reasons for this effect include the postoperative physiological adaptation of soft tissue to the new environment and the location shift of the hyoid bone, as evidenced by some studies [14, 15]. In his study, Saitoh theorized that the connecting soft tissues and the musculature that anchor and stabilize the airway explain how skeletal movements can influence the upper airway [16]. The adaptive changes in soft tissue should be considered an important factor when evaluating airway changes.
Thus, the purpose of this retrospective study focused on the quantitative relationship between hard and soft tissue movements and airway changes in Class III patients at one year after bimaxillary surgery.
Materials and methods
Subjects
The protocols were approved by the Medical Ethics Committee of the Peking University School and Hospital of Stomatology (No. 202053015). Due to the retrospective nature of the present study, informed consent was not needed. The sample size of this research was calculated by using PASS (Power Analysis and Sample Size, Utah, USA.) software. The desired value and standard deviation were δ = 724.71 and SD = 1098.38, respectively, which was calculated based on a pre-experiment of ten patients. The other statistical settings were α = 0.05 and β = 0.1. At least 27 samples were needed for this study.
The patients were recruited from the Department of Radiology, Peking University School of Stomatology from January 2017 to December 2019. The inclusion criteria included skeletal Class III deformities (ANB < 0°; overjet<− 2 mm), performance of maxillary advancement and mandibular setback and genioplasty procedures and sufficient visual fields of images. The exclusion criteria included congenital syndromes, diagnoses of temporomandibular joint disorders, BMI > 35 kg/m2, records with respiratory disease or a history of facial trauma. Patients were also excluded if the change in cranio-cervical inclination was greater than 5° between the T1 (one week before surgery) and T2 (an average of 1 year after surgery) scans, which was done to avoid significant influences of neck extension on airway measurements [7, 17].
In total, thirty patients, including 15 males and 15 females, were selected. All of the patients were aged from 18 to 29 years, and the average age was 23.3 ± 3.4 years. Moreover, the average BMI of the patients was 21.49 ± 3.92 kg/m2.
Cone beam computed tomography (CBCT) scanning
CBCT scans were obtained at 2 time points: T1 (one week before surgery) and T2 (an average of 1 year after surgery). All of the subjects were scanned with the same machine (DCT PRO; Vatech Co, Seoul, South Korea) in routine processes. For each patient, CBCT was performed according to the international guidelines. The CBCT settings were as follows: tube voltage, 90 kVp; scan time, 24 s; tube current, 4.0 mA and voxel size, 0.3 mm. The data were imported into Dolphin software version 11.0 (Dolphin Imaging and Management Solutions, Chatsworth, California USA) for data processing [18].
Three-dimensional coordinate system and image superimposition
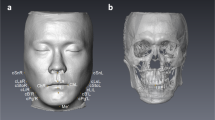
A three-dimensional coordinate system was set up for each CBCT image (Fig. 1A). The Frankfort horizontal plane was set as the x-coordinate, and the left side direction was recorded as being positive. A plane perpendicular to the x-axis and passing through Nasion was defined as the y-coordinate, and the upwards direction was recorded as being positive. The plane perpendicular to the other planes that went through Nasion was defined as the Z plane, and the forward direction was recorded as being positive.

Three-dimensional coordinate system and image superimposition of the CBCT. A. Three-dimensional coordinate system. B. Superimposition of preoperative and postoperative CBCT. The red box stood for the reference region. The definition landmarks were given in Table 2. C. Linear measurements of soft palate and tongue. D Area measurements of soft palate and tongue
Quantifications of jaw movements were performed via the superimposition of preoperative and postoperative CBCT images. Via the Dolphin software, voxel-based superimposition was performed as previously described by Bazina, Mohamed and Hernando [19, 20]. The anterior cranial base was selected as the reference region, which is shown in Fig. 1B.
Five landmarks, including PNS, A, B, Gn and H, were digitized on the CBCT images to represent the posterior maxilla, anterior maxilla, anterior mandible, chin and hyoid bone, respectively. We digitized the landmarks in the sagittal, coronal and axial planes according to the method previously described by Ludlow JB [21]. The definitions of the landmarks are provided in Table 1, and a diagrammatic sketch is shown in Fig. 1B. The coordinates of the landmarks were exported by the software. The movements of the jaws were calculated by subtracting the coordinates both before and after the surgery.
Soft tissue and airway measurements
All soft tissue measurements were measured in the middle sagittal plane under the same threshold settings, including the length, area and angle of the soft palate, as well as the horizontal length and vertical height of the tongue (Fig. 1C). To describe the relationship between the soft palate and tongue, their contact distance was recorded. The tongue was divided into the velopharyngeal tongue and oropharyngeal tongue, according to the plane that passed through the tip point of the soft palate, and the area of the two parts was calculated (Fig. 1D).
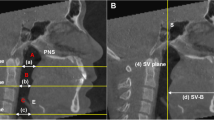
The total airway was defined as the sum of the nasopharynx, retropalatal and retroglossal airways, which are illustrated by diagrammatic sketches in Fig. 2 A and B. The nasopharynx airway was defined as the area between a plane parallel to the Frankfort horizontal through the PNS and a plane perpendicular to the Frankfort horizontal through the PNS [22]. The retropalatal airway was defined as the airway that was superiorly bounded by the plane parallel to the Frankfort horizontal passing through PNS and inferiorly bounded by a plane parallel to the Frankfort horizontal passing through the top of the soft palate [22]. The retroglossal airway was defined as the airway that was superiorly bounded by the lower border of the retropalatal airway and inferiorly bounded by a plane parallel to the Frankfort horizontal passing through the top of the epiglottis.

The three-dimensional diagrammatic sketch of upper airway division and their illustrations. A. Division of the pharyngeal airway in the midsagittal plane. NP: Nasopharynx airway, RP: Retropalatal airway, RG: Retroglossal airway. B. Four planes at the levels of the hard palatal, soft palate, tongue, and epiglottis. C. Anteroposterior length and transversal width, cross-sectional area at each plane
The airway was 3-dimensionally scanned to ensure that every aspect was included. The volume was calculated via Dolphin software under the same threshold settings. To evaluate the airway changes at different levels, we measured the anteroposterior length (APL), largest transverse width (LTW) and cross-sectional area (CSA) at 4 axial planes (palatal plane, soft palate, tongue and epiglottis) (Fig. 2C) [23]. The definitions of the airway measurements are provided in Table 1.
The operator reliabilities of landmarks and airway measurements were evaluated by using intraclass correlation coefficients. Ten subjects were randomly selected from all of the subjects to test for intraoperator and interoperator reliabilities. Intraoperator reliability was performed by the same operator (HZ. L.), who defined the landmarks twice in one week. Interoperator reliability was assessed by 2 operators (HZ. L and YL. C) at the same time. The intraoperator reliability coefficients varied between 0.77 and 0.99. The interoperator reliability coefficients ranged from 0.79 to 0.99.
Statistical analyses
SPSS software (Windows version 17.0; SPSS Inc. Chicago, IL, USA) was used to perform the data analysis. The data were described as the mean and standard deviation after using the Shapiro–Wilk test to identify a normal distribution. Paired t tests were used to verify significant differences in the airway measurements and in hard and soft tissue changes. A single-factor linear regression analysis was conducted to screen the variables (included if p < 0.1). Subsequently, stepwise multiple linear regression analyses were performed to identify the factors that affected the airway volume.
Results
Maxillary and mandibular movements
Three-dimensional movements of landmarks are provided in Table 2. The main changes occurred in the sagittal dimension, with the A point and PNS point moving forward and the B point and Gn point moved backwards.
Soft tissue and hyoid bone changes
The soft tissue and hyoid changes after orthognathic surgery was shown in Table 3. The length of the soft palate was observed to be larger than that before the operation. The included angle between the soft palate and hard palate was also found to be larger than that before the operation. The tongue arched up from the horizontal into the vertical planes due to mandible compression, with the horizontal length decreasing and vertical length increasing. The contact distance of the soft palate and tongue were also observed to be significantly increased. Moreover, the three-dimensional positions of the hyoid bone did not significantly change.
Airway measurements
An increase in the nasopharynx airway space and a decrease in the retropalatal and retroglossal airway spaces were observed (Table 4). A significant decrease was also observed in the cross-sectional area at the levels of the soft palate, tongue, and epiglottis. The exception was the cross section at the level of the hard palate plane, with an increase in the APL (p < 0.05); however, the area and LTW of this section did not significantly change.
Multiple linear regression analysis
The scatter plots of the included factors are shown in Fig. 3. The results of the multivariate linear regression analysis are provided in Table 5. The nasopharynx airway volume was shown to be affected by PNS movement; one millimetre of forward movement of the PNS point increased the airway volume by 626.90 mm3, whereas one millimetre of upwards movement decreased the airway volume by 392.18 mm3. Furthermore, retro-palatal airway volume was observed to be affected by B sagittal backwards movement and the soft palate, with 314.6 mm3 and 204.9 mm3 volume reductions observed per unit, respectively. The retroglossal airway was shown to be affected by B sagittal movement and tongue horizontal length; one millimetre setback of the former factor reduced airway volume by 656.6 mm3, whereas one millimetre reduction of the latter factor offset airway volume by 356.4 mm3. To better explain the effects of jaw movement on the airway, the quantitative relationship between jaw movement and the percentage change of airway was also calculated, and the results are provided in Table 5.

Single linear analysis of the variables bone movements and volume variation. A. PNS horizontal movement and nasopharynx airway volume (r = 0.451). B. PNS vertical movement and nasopharynx airway volume (r = 0.378). C. B horizontal movement and retropalatal airway volume (r = 0.574). D. Soft palate angle and retropalatal airway volume (r = 0.643). E. B horizontal movement and retroglossal airway volume (r = 0.548). F. Tongue horizontal length and retroglossal airway volume (r = 0.261)
Discussion
This study aimed to provide a mathematical calculation to predict the volumetric changes in the upper airway after orthoganthic surgery in Class III patients, which will benefit the estimation and prediction of potential sleep-disordered breathing risks in the preoperative planning stage. The risk has been previously described by a systematic review that showed that reduction of the upper airway should be considered for patients who have undergone large mandible setback surgery [24]. However, two-jaw surgery is more common than single-jaw surgery for Class III patients in the real world for the sake of a better profile. Some scholars believe that two-jaw surgery is beneficial to the airway [25,26,27,28], whereas other scholars hold the opposite view [3, 29,30,31]. The divergence among the studies not only resulted from different surgical designs but was also due to the degrees of bone movement of each surgery [32]. Therefore, a formula established by using regular movement of landmarks of the maxilla and mandible could be significant for evaluating airway changes.
Wiedemeyer used a mathematical method to predict airway changes in Class II patients [33], which was a valuable attempt at practicing precision medicine. However, his research focused on single jaw surgery, and the lateral cephalometric radiograph that was used in his study could not reflect the actual 3D airway structures. Three-dimensional digital technology based on CBCT was used in this study to observe airway, jaw and soft tissue changes from a three-dimensional perspective. Additionally, one year was set as the observation window in consideration of time, in order to avoid the recurrence stage and to obtain more stable results. According to previous studies, more than 6 months was considered the stable stage for Class III organathic surgery patients [11, 30].
From the current study, it could be observed that one millimetre forward and downwards movements of PNS resulted in an increase of 626.90 mm3 and 392.18 mm3 of the nasopharynx airway volume, respectively. Subsequently, for one millimetre retrogression of point B, a 314.6 mm3 decrease in the retropalatal airway and a 656.6 mm3 decrease in the retroglossal airway could be seen. There have been some similar reports that have proven the relationship between upper airway changes and the amount of bone movement. For example, Mohammed found that nasopharynx airway changes were related to the A point [7]. Additionally, Hart demonstrated the quantitative relationship that one millimetre of forward or backwards movements of the D point could account for a 403.6 mm3 increase in the total airway or a 383.9 mm3 decrease in the oropharyngeal airway volume [34]. However, Brunetto suggested the use of percentage values instead of absolute values [35]. The experimental results may vary among studies because of different surgical designs, sample characteristics, measurement indices and follow-up times.
According to the present study, the main disadvantage factor for upper airway changes was mandible setback, which not only caused an encroachment of the pharynx but also pushed the soft palate back to the retropalatal airway space, which ultimately decreased the airway volume. Moreover, the advantageous factors for upper airway changes included maxilla movement and tongue adaptation changes. The forward and downwards movements of the maxilla acted as a favourable factor for the postoperative airway changes due to its positive correlation with the nasopharynx airway volume. In addition to this, adaptive tongue changes (arched dorsum) were also observed to be helpful for the upper airway. A multivariate linear regression analysis showed that the decrease in tongue horizontal length could offset retroglossal airway volume reduction. The tongue played a compensatory role in mandible retraction if given a relatively long time to adapt to the new jaw position.
In addition, the changes in the hyoid bone did not significantly change in this study, which was consistent with the studies by Aydemir [36].
As a retrospective study, the present study had limitations due to several missing data details. The reference data provided in the present study may only be used in Asian Class III patients undergoing bimaxillary surgery. Furthermore, the conclusion of this study was drawn from young and thin patients, which may not act as guidelines for patients with larger BMIs, older ages or populations from other races. In addition, a one-year period was set as the observation window, which could not reflect even longer changes in the airway. Finally, this study was based on sitting CBCT images and a lack of a polysomnography (PSG) index, which could provide neither sleep functional data nor direct evidence of OSA risks.
Conclusion
This was a pilot study to provide a quantitative relationship between airway volume changes and bone movements. The upper airway volume was comprehensively affected by both maxilla advancement and mandible recession. The compensatory performance of the tongue also played an advantageous role in one-year airway changes.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- CBCT:
-
Come beam tomography
- OSA:
-
Obstructive sleep apnea
References
Naran S, Steinbacher DM, Taylor JA. Current Concepts in Orthognathic Surgery. Plast Reconstr Surg. 2018;141:925e–36e.
Chen F, Terada K, Hua Y, Saito I. Effects of bimaxillary surgery and mandibular setback surgery on pharyngeal airway measurements in patients with class III skeletal deformities. Am J Orthod Dentofac Orthop. 2007;131(3):372–7. https://doi.org/10.1016/j.ajodo.2005.06.028.
Irani SK, Oliver DR, Movahed R, Kim YI, Thiesen G, Kim KB. Pharyngeal airway evaluation after isolated mandibular setback surgery using cone-beam computed tomography. Am J Orthod Dentofac Orthop. 2018;153(1):46–53. https://doi.org/10.1016/j.ajodo.2017.05.031.
Muto T, Yamazaki A, Takeda S, Sato Y. Effect of bilateral sagittal split ramus osteotomy setback on the soft palate and pharyngeal airway space. Int J Oral Maxillofac Surg. 2008;37(5):419–23. https://doi.org/10.1016/j.ijom.2007.12.012.
Chen F, Terada K, Hanada K, Saito I. Predicting the pharyngeal airway space after mandibular setback surgery. J Oral Maxillofac Surg. 2005;63(10):1509–14. https://doi.org/10.1016/j.joms.2005.06.007.
Neelapu BC, Kharbanda OP, Sardana HK, Balachandran R, Sardana V, Kapoor P, et al. Craniofacial and upper airway morphology in adult obstructive sleep apnea patients: a systematic review and meta-analysis of cephalometric studies. Sleep Med Rev. 2017;31:79–90. https://doi.org/10.1016/j.smrv.2016.01.007.
Almuzian M, Almukhtar A, Ju X, Al-Hiyali A, Benington P, Ayoub A. Effects of Le fort I osteotomy on the nasopharyngeal airway—6-month follow-up. J Oral Maxillofac Surg. 2016;74(2):380–91. https://doi.org/10.1016/j.joms.2015.06.172.
Souza Pinto GNd, Iwaki Filho L, Previdelli ITdS, Ramos AL, Yamashita AL, Stabile GAV et al. Three-dimensional alterations in pharyngeal airspace, soft palate, and hyoid bone of class II and class III patients submitted to bimaxillary orthognathic surgery: a retrospective study. J Cranio-Maxillofac Surg 2019;47(6):883–894. DOI: https://doi.org/10.1016/j.jcms.2019.03.015.
Kitahara T, Hoshino Y, Maruyama K, In E, Takahashi I. Changes in the pharyngeal airway space and hyoid bone position after mandibular setback surgery for skeletal Class III jaw deformity in Japanese women. Am J Orthod Dentofacial Orthop 2010;138:708.e701–710; discussion 708-709.
Mattos CT, Vilani GNL, Sant’Anna EF, Ruellas ACO, Maia LC. Effects of orthognathic surgery on oropharyngeal airway: a meta-analysis. Int J Oral Maxillofac Surg. 2011;40(12):1347–56. https://doi.org/10.1016/j.ijom.2011.06.020.
An JH, Park S-B, Choi Y-K, Lee SH, Kim KB, Kim Y-I. Cone-beam computed tomography evaluation of pharyngeal airway space changes after Bimaxillary orthognathic surgery in patients with class III skeletal deformities: a 6-year follow-up study. J Oral Maxillofac Surg. 2019;77(12):2534–44. https://doi.org/10.1016/j.joms.2019.07.013.
Giralt-Hernando M, Valls-Ontañón A, Haas Junior OL, Masià-Gridilla J, Hernández-Alfaro F. What are the surgical movements in orthognathic surgery that Most affect the upper airways? A three-dimensional analysis. J Oral Maxillofac Surg. 2021;79(2):450–62. https://doi.org/10.1016/j.joms.2020.10.017.
Saitoh K. Long-term changes in pharyngeal airway morphology after mandibular setback surgery. Am J Orthod Dentofac Orthop. 2004;125(5):556–61. https://doi.org/10.1016/j.ajodo.2003.04.017.
Li YM, Liu JL, Zhao JL, Dai J, Wang L, Chen JW. Morphological changes in the pharyngeal airway of female skeletal class III patients following bimaxillary surgery: a cone beam computed tomography evaluation. Int J Oral Maxillofac Surg. 2014;43(7):862–7. https://doi.org/10.1016/j.ijom.2014.03.009.
Burkhard JP, Dietrich AD, Jacobsen C, Roos M, Lübbers HT, Obwegeser JA. Cephalometric and three-dimensional assessment of the posterior airway space and imaging software reliability analysis before and after orthognathic surgery. J Craniomaxillofac Surg. 2014;42(7):1428–36. https://doi.org/10.1016/j.jcms.2014.04.005.
Saitoh K. Long-term changes in pharyngeal airway morphology after mandibular setback surgery. Am J Orthod Dentofac Orthop. 2004;125(5):556–61. https://doi.org/10.1016/j.ajodo.2003.04.017.
Muto T, Takeda S, Kanazawa M, Yamazaki A, Fujiwara Y, Mizoguchi I. The effect of head posture on the pharyngeal airway space (PAS). Int J Oral Maxillofac Surg. 2002;31(6):579–83. https://doi.org/10.1054/ijom.2002.0279.
Weissheimer A, Menezes LMd, Sameshima GT, Enciso R, Pham J, Grauer D. Imaging software accuracy for 3-dimensional analysis of the upper airway. Am J Orthod Dentofac Orthop 2012;142(6):801–813. DOI: https://doi.org/10.1016/j.ajodo.2012.07.015.
Bazina M, Cevidanes L, Ruellas A, Valiathan M, Quereshy F, Syed A, et al. Precision and reliability of dolphin 3-dimensional voxel-based superimposition. Am J Orthod Dentofac Orthop. 2018;153(4):599–606. https://doi.org/10.1016/j.ajodo.2017.07.025.
Haas Junior OL, Guijarro-Martínez R, Sousa Gil AP, Méndez-Manjón I, Valls-Otañón A, de Oliveira RB, et al. Cranial Base superimposition of cone-beam computed tomography images: a voxel-based protocol validation. J Craniofac Surg. 2019;30(6):1809–14. https://doi.org/10.1097/SCS.0000000000005503.
Ludlow JB, Gubler M, Cevidanes L, Mol A. Precision of cephalometric landmark identification: Cone-beam computed tomography vs conventional cephalometric views. Am J Orthod Dentofacial Orthop. 2009;136:312.e311-312.e310.
Kim Y-J, Hong J-S, Hwang Y-I, Park Y-H. Three-dimensional analysis of pharyngeal airway in preadolescent children with different anteroposterior skeletal patterns. Am J Orthod Dentofacial Orthop. 2010;137:306.e301-306.e311.
Mattos CT, Cruz CV, da Matta TCS, Pereira LdA, Solon-de-Mello PdA, Ruellas ACdO et al. Reliability of upper airway linear, area, and volumetric measurements in cone-beam computed tomography. Am J Orthod Dentofac Orthop. 2014;145(2):188–197. DOI: https://doi.org/10.1016/j.ajodo.2013.10.013.
Canellas JV, Barros HL, Medeiros PJ, Ritto FG. Sleep-disordered breathing following mandibular setback: a systematic review of the literature. Sleep Breath. 2016;20(1):387–94. https://doi.org/10.1007/s11325-015-1274-z.
Christovam IO, Lisboa CO, Ferreira DM, Cury-Saramago AA, Mattos CT. Upper airway dimensions in patients undergoing orthognathic surgery: a systematic review and meta-analysis. Int J Oral Maxillofac Surg. 2016;45(4):460–71. https://doi.org/10.1016/j.ijom.2015.10.018.
He J, Wang Y, Hu H, Liao Q, Zhang W, Xiang X, et al. Impact on the upper airway space of different types of orthognathic surgery for the correction of skeletal class III malocclusion: a systematic review and meta-analysis. Int J Surg. 2017;38:31–40. https://doi.org/10.1016/j.ijsu.2016.12.033.
Hong JS, Park YH, Kim YJ, Hong SM, Oh KM. Three-dimensional changes in pharyngeal airway in skeletal class III patients undergoing orthognathic surgery. J Oral Maxillofac Surg. 2011;69(11):e401–8. https://doi.org/10.1016/j.joms.2011.02.011.
Uslu-Akcam O, Gokalp H. Tongue size and posterior airway space changes in class III malocclusion after Maxillomandibular surgery: a retrospective study. Int J Orthod Milwaukee. 2015;26(4):37–43.
He L, He S, Wu X, Huang Y. Three-dimensional morphological changes of the upper airway in patients with skeletal class III malocclusion after orthognathic surgery. J Craniofac Surg. 2019;30(8):2451–5. https://doi.org/10.1097/SCS.0000000000005738.
Tan SK, Tang ATH, Leung WK, Zwahlen RA. Three-dimensional pharyngeal airway changes after 2-jaw orthognathic surgery with segmentation in Dento-skeletal class III patients. J Craniofac Surg. 2019;30(5):1533–8. https://doi.org/10.1097/SCS.0000000000005351.
Park JE, Bae SH, Choi YJ, Choi WC, Kim HW, Lee UL. The structural changes of pharyngeal airway contributing to snoring after orthognathic surgery in skeletal class III patients. Maxillofac Plast Reconstr Surg. 2017;39(1):22. https://doi.org/10.1186/s40902-017-0120-6.
Guimarães TM, Bariani RC, Iafigliola SG, Guimarães CM, Chaves Junior CM, Ferraz O, et al. Cone beam computed tomography in assessment on pharynx effects of orthopedic-surgical treatment - a review of the literature. Sleep Sci. 2019;12(2):106–9. https://doi.org/10.5935/1984-0063.20190066.
Wiedemeyer V, Berger M, Martini M, Kramer F-J, Heim N. Predictability of pharyngeal airway space dimension changes after orthognathic surgery in class II patients: a mathematical approach. J Cranio-Maxillofac Surg. 2019;47(10):1504–9. https://doi.org/10.1016/j.jcms.2019.07.024.
Hart PS, McIntyre BP, Kadioglu O, Currier GF, Sullivan SM, Li J, et al. Postsurgical volumetric airway changes in 2-jaw orthognathic surgery patients. Am J Orthod Dentofac Orthop. 2015;147(5):536–46. https://doi.org/10.1016/j.ajodo.2014.12.023.
Brunetto DP, Velasco L, Koerich L, Araujo MT. Prediction of 3-dimensional pharyngeal airway changes after orthognathic surgery: a preliminary study. Am J Orthod Dentofac Orthop. 2014;146(3):299–309. https://doi.org/10.1016/j.ajodo.2014.05.024.
Aydemir H, Memikoğlu U, Karasu H. Pharyngeal airway space, hyoid bone position and head posture after orthognathic surgery in class III patients. Angle Orthod. 2012;82(6):993–1000. https://doi.org/10.2319/091911-597.1.
Acknowledgements
Not applicable.
Funding
The study was supported by National Natural Science Foundation of China [81470272] and Beijing Municipal Natural Science Foundation[L192068].
Author information
Authors and Affiliations
Contributions
Hai-Zhen Li reviewed medical records, analyzed data, and wrote draft manuscripts. Chong-Ke Sun and Yan-Long Chen helped to collect the medical records and participated in their follow-up. Xue-Mei Gao and Zhi-Peng Sun designed this research together and Xue-Mei Gao was the main writer of manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The protocol for the research project has been approved by the Medical Ethics Committee of PKUSSIRB (No. 202053015) of Peking University School and Hospital of Stomatology, and that it conforms to the provisions of the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, H., Sun, C., Chen, Y. et al. Quantitative changes of upper airway in class III patients undergoing bimaxillary surgery after one-year follow-up: a retrospective study. Head Face Med 18, 14 (2022). https://doi.org/10.1186/s13005-022-00317-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13005-022-00317-2