
Abstract
Background
The elaboration of a precise pre-surgical plan is essential during surgical treatment of dentofacial deformities. The aim of this study was to evaluate the accuracy of computer-aided simulation compared with the actual surgical outcome, following orthognathic surgery reported in clinical trials.
Methods
Our search was performed in PubMed, EMBASE, Cochrane Library and SciELO for articles published in the last decade. A total of 392 articles identified were assessed independently and in a blinded manner using eligibility criteria, out of which only twelve articles were selected for inclusion in our research. Data were presented using intra-class correlation coefficient, and linear and angular differences in three planes.
Results
The comparison of the accuracy analyses of the examined method has shown an average translation (< 2 mm) in the maxilla and also in the mandible (in three planes). The accuracy values for pitch, yaw, and roll (°) were (< 2.75, < 1.7 and < 1.1) for the maxilla, respectively, and (< 2.75, < 1.8, < 1.1) for the mandible. Cone-beam computed tomography (CBCT) with intra-oral scans of the dental casts is the most used imaging protocols for virtual orthognathic planning. Furthermore, calculation of the linear and angular differences between the virtual plan and postoperative outcomes was the most frequented method used for accuracy assessment (10 out of 12 studies) and a difference less than 2 mm/° was considered acceptable and accurate.
When comparing this technique with the classical planning, virtual planning appears to be more accurate, especially in terms of frontal symmetry.
Conclusion
Virtual planning seems to be an accurate and reproducible method for orthognathic treatment planning. However, more clinical trials are needed to clearly determine the accuracy and validation of the virtual planning in orthognathic surgery.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
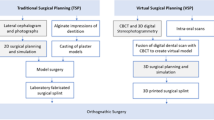
Two-dimensional (2D) radiographs and manual model surgery are essential parts of the preoperative planning for orthognathic surgery. However, this approach has its limitations, especially in the case of patients with major facial deformity or asymmetry [1], as 2D cephalometric images cannot provide full information about the 3D structures.
When conventional 2D surgical plans are executed, unexpected problems, such as a bony collision in the ramus area, the discrepancy in pitch, roll and yaw rotation, midline difference and chin inadequacy may occur [2].
When two-jaw surgery is performed, an inter-occlusal splint is fabricated to work as an intermediate guide for repositioning the maxilla relative to the intact mandible [3]. Any variation between the plan and the plaster model surgery could lead to a poorly fabricated wafer, which in turn could lead to unexpected (and often undesirable) results, regardless of how skillfully and carefully the surgery is performed [3].
These examples illustrate that the elaboration of a precise pre-surgical plan is of utmost importance when it comes to correcting dentofacial deformities.
Computer-aided surgical simulations using cone beam computed tomography (CBCT) images have revolutionized orthodontics and have been adapted for orthognathic surgery (OGS) to facilitate cephalometric analysis, surgical simulation and splint fabrication [4,5,6,7,8,9].
In particular, the visualization of skeletal complexities within an asymmetric dentofacial deformity has been greatly enhanced through three dimensional (3D) modeling, which can demonstrate the extent of yaw rotation in the maxilla and mandible, occlusal plane canting and differential length of a mandibular body or the ramus [1, 10, 11]. The 3D simulation method has been accepted for planning in orthognathic surgery and led to significant improvements in surgical outcomes [1, 9, 12]. Intraoperative efficiency has also improved with the fabrication of the templates and jigs to reproduce gaps or spacing between the osteotomies depicted in the virtual plan. These jigs may reinforce intraoperative accuracy of the clinical movement of the virtual plan and aid in orienting and positioning bony segments [10, 13,14,15,16,17,18]. Thus, the aim of this systematic review is to assess the accuracy of computer-aided planning in orthognathic surgery.
Methods
A systematic search was conducted of electronic and printed articles that have been published in the period (2007–2017) on virtual planning for orthognathic surgery and in the English language. The databases used were PubMed, EMBASE, Cochrane Library and SciELO. Keywords and Boolean operators (‘OR’ and ‘AND’) were used to join the terms related to orthognathic surgery and virtual planning.
Search strategy
Main search
The systematic search was done by one of the authors (A.A.). The search of PubMed was conducted using the following medical subject heading (MeSH) terms: [(‘Orthognathic Surgery’ OR ‘Surgery, Orthognathic’ OR ‘Maxillofacial Orthognathic Surgery’ OR ‘Orthognathic Surgeries, Maxillofacial’ OR ‘Orthognathic Surgery, Maxillofacial’ OR ‘Surgery, Maxillofacial Orthognathic’ OR ‘Orthognathic Surgical Procedures’ OR ‘Procedure, Orthognathic Surgical’ OR ‘Surgical Procedure, Orthognathic’ AND (‘Surgery, virtual planning’ OR ‘virtual planning Surgery’ OR ‘Computer Assisted Surgery’ OR ‘virtual planning ,Surgery’ OR ‘Surgery, virtual planning’ OR ‘virtual planning Design’ OR ‘virtual planning Designs’ OR ‘Design, virtual planning’ OR ‘virtual planning Manufacturing’ OR ‘Manufacturing, virtual planning’)].
The same search strategy was applied to the Cochrane Library since this also uses MeSH terms.
For the search of EMBASE, the entry terms ‘orthognathic surgery’ AND ‘virtual planning surgery’ were used to carry out a specific search.
Health sciences descriptors were used to search the SciELO databases, ‘orthognathic surgery’ AND ‘virtual planning’ were performed.
Eligibility of the studies
The eligibility of the studies was determined by the author (A.A.), observing the following criteria: (1) the main theme of the paper had to focus on virtual planning for orthognathic surgery; (2) the study had to be original and interventional; (3) the surgical procedure had to be virtually planned with a virtual surgical splint; (4) accuracy measures had to be presented for the surgical procedure; (5) the sample size of the trial had to be ≥10. The latter criterion was determined somewhat arbitrarily, as a reasonable minimum, given the small sample sizes of these studies in general.
Main search
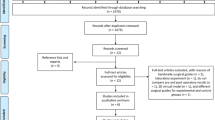
Three hundred and sixty-seven articles were found in PubMed, 84 in EMBASE, 7 in Cochrane Library and 16 in SciELO. Duplicate papers were removed, leaving a total of 392 possible studies, that have been read and 31 of these were chosen for full-text reading (Fig. 1).

Flowchart of the review process
Eligibility assessment
As part of the eligibility assessment, 31 studies were read in full. At the end of this analysis, only twelve papers were included in the sample for our systematic review. The other 19 studies were excluded for the following reasons: virtual surgical planning for orthognathic surgery was not the main focus of the paper [19],the paper was not an intervention study [17], or it was not original [5, 20, 21], the surgical procedure did not involve a computer-assisted virtual surgical splint [22,23,24], the accuracy measurements for the surgical procedure were not provided [25,26,27,28,29] and the sample size was less than 10 [16, 22, 30,31,32,33].
Quality assessment of the included articles
The quality of the papers was assessed using an adaptation of the bias analysis proposed by Clementini and colleagues [34]. The criteria were the presence or absence of the following: sample randomization, blind assessment, statistical analysis, defined inclusion and exclusion criteria and reporting of follow-up. With respect to the risk of bias for each analyzed study, papers containing all the above items were considered low risk, studies lacking one or two items were missing were deemed medium risk, and investigations that lacked three or more items were considered high risk.
Results
Descriptive data of the included studies (sample size, age, gender and type of facial deformity) are presented in (Table 1).
The imaging protocols and the software used for surgical planning varied substantially among the studies, These variations are shown in (Table 2).
The included studies also varied in the type of surgical plan and virtual splints, as well as in the method used for the assessment of accuracy. These variations we summarized in (Table 3).
The actual accuracy values are presented in detail in Additional file 1 (Table S1).
Finally, the papers included in this review were assessed as being medium quality, since the risk of bias was considered medium in ten studies of the twelve. The risk of bias assessement for the included studies are presented in (Table 4).
Discussion
The use of computerized methods for diagnosis and treatment planning in orthodontics and orthognathic surgery has evolved substantially [42], which is confirmed by the 392 papers on this topic that have appeared in the major databases in the period (2007–2017).
Hsu and colleagues reported that computer-aided techniques enable the accurate correction of maxillary malformations with yaw deviation, alignment of proximal and distal segments and restoration of mandibular symmetry [6].
Lin and co-workers concluded that virtual orthognathic planning yields aesthetically favorable results, a high level of patient satisfaction, accurate translation of the treatment plan and thus making the operation itself easier and safer [20, 44].
The analyzed studies used both the CT and CBCT imaging modalities (two of them worked with both). Better identification of soft tissue and less image distortion where metallic elements are present are obvious advantages of CT over CBCT, while disadvantages include image quality, the supine position of the patient during the test (especially because of mandibular retrusion) and larger radiation doses [45,46,47]. Mandibular retrusion in the supine position during CT image capture was attenuated using central occlusal registry [6, 42]. The major disadvantage of CBCT is the occasional appearance of metal artifacts, but this is diminished by scanning the plaster casts [37, 40, 42], intraoral scanning of the dental arches [30, 37], scanning occlusion with reference points [6, 7] or by a triple scan procedure [39, 41].
Thus, the fusion of facial CT images and dental arch scans is important in computer-aided planning and it is more accurate when reference points are reproducible for both modalities [8].
Evaluation of the accuracy of the virtual planning methods used in Orthognathic surgery
One of the most frequently used methods to evaluate the accuracy of virtual planning is the use of the mean error differences in superimposition between the virtual plan and the postoperative outcomes. Baan and colleagues used this technique to assess the degree of correspondence between the planned and performed positions. They also assessed the repeatability of the surgical procedure performed by different surgeons, and noticed that the discrepancy between the 3D planning and the postoperative results was the greatest regarding the vertical positioning of the maxilla and mandible, suggesting a less accurate intra-operative vertical control of virtual planning [39].
On the other hand, Franz and co-workers suggested that the use of the mean error as an only endpoint to measure the degree of accuracy can limit the generalizability of the studies. They also suggested that the confidence interval does not describe the real range of the method error but defines only the range of values that the mean error can assume from a statistical perspective [23].
Ho and colleagues calculated the accuracy of computer-aided orthognathic planning by evaluating the root-mean square difference (RMSD) of the 3D simulation and postsurgical CBCT images and found that the errors were acceptable, with RMSD (0.63 ± 0.25) mm for the maxilla and (0.85 ± 0.41) mm for the mandible [1].
De Riu and co-workers also suggested that the simple superimposition of the simulation and the cephalometric results is an unsatisfactory method, as it fails to consider the magnitude of the surgical manipulation leading to an error of a given magnitude. For instance, a slight positional error can be completely acceptable for large manipulations, but would be unacceptable when the manipulation takes place at a small scale and thus needs to be extremely precise [35].
The accuracy of the translation of the maxilla with computer-assisted planning for orthognathic surgery was < 1 mm in the study of Hsu and colleagues, indicating that this type of planning is accurate for the maxilla [6].
The Stokbro group found that the mean linear differences for the maxilla, mandible and the chin segment in all three planes were within 0.5 mm, while the mean precision, measured as the standard deviation, had the smallest deviation superoinferiorly, followed closely by mediolateral deviation, and finally the largest deviation was found anteroposteriorly [38].
De Riu and co-workers found that virtual surgical planning presented a high degree of accuracy for most of the parameters assessed, with an average error of 1.98 mm for linear measurements and 1.19° for angular measurements. At the same time, they observed significant differences between planned and achieved anterior facial height (p = 0.033). Without genioplasty, no significant difference was observed (U test; p = 0.45). The authors concluded that the problem was caused by the virtual model of the soft tissues, which made it difficult to manage the vertical dimension [35].
It has been also shown in the study of Baan and colleagues that the right /left translation has the lowest absolute mean difference between the 3D planning and the surgical results for both the maxilla and mandible (0.49 mm and 0.71 mm, respectively). Furthermore, they noticed that in 7 out of 10 cases, the maxilla was positioned more posteriorly than in the 3D plan, with an absolute mean difference of 1.41 mm. The same tendency was found in the sagittal position of the mandible,where in 8 out of 10 cases the mandible was positioned more posteriorly than planned with absolute mean difference of 1.17 mm [39]. Lee and colleagues suggested that the condylar position might have been changed during surgery by muscle tone and gravity as the patient was placed in the supine position, which affects the optimal condylar seating [48]. Stokbro et al. (2016) are of the same opinion about this issue.
The clinical analysis of Sun and colleagues, of the twenty three patients, using the OrthoGnathic Analyser, showed an adequate position of the maxilla and mandible in the left/right direction with a deviation of 0.32 mm and 0.75 mm, respectively. It was found that the maxilla had a lower RMSD (0.6 mm) than did the mandible (0.85 mm) [19].
Zhang et al. showed that the overall mean linear difference was (0.81 mm), and the overall mean angular difference was (0.95°) [40], which was an improvement as compared with their previous study, as a result of surgical experience, 3D printing technology, and improvement of the elasticity modulus of 3D-printed surgical templates [49].
On the other hand, Baan et al. observed that the accuracy of the pitch of the maxilla (2.72°) and the mandible (2.75°) showed the highest discrepancy between the 3D plans and the actual postoperative status. This variance could be the result of bone conflict between the pterygoid plate and the osteotimized maxilla [39]. Stokbro et al. came to similar conclusions [38].
Comparison of the accuracy between classical and virtual planning methods
A lot of studies compared computer-assisted planning with classical planning and found favorable accuracy results in all bony segments for computer-aided planning [36, 41, 42, 50]. Ziesner and colleagues reported that the mandibular condyle maintained a central position in the temporomandibular joint, which did not occur when classic planning was used [42].
Hsu et al. compared the two types of interventions in the chin and found highly favorable accuracy results for computer-aided planning in this bone segment, with the largest difference recorded for translation in the sagittal plane (2.5 mm) and rotation pitch (3.68°). They explained these differences by the fact that classical planning does not use surgical splints; surgeons are guided by their experience, some internal reference points and the chin plate [6].
Ritto and colleagues reported on a similar level of precision in all evaluated regions when assessing the vertical positioning of the maxilla, but virtual surgical planning (VSP) was more accurate for the anteroposterior position of the maxilla. As for transverse positioning, conventional model surgery (CMS) yielded higher precision only for the upper midline position. However, there was no statistically significant difference between the groups, and the mean imprecision was also < 2 mm for all regions evaluated [36].
Risk of Bias assessment
The papers included in this systematic review were classified as medium quality, since the risk of bias was considered medium in ten studies [1, 6, 7, 35,36,37, 39, 41,42,43], that is, the majority.
These studies [1, 7, 35,36,37, 42, 43] did not report on sample randomization and blinding. Baan et al. (2016) failed to report on blinding and follow-up.
Conclusions
In conclusion, the results of this systematic review suggest that computer-aided planning is an accurate method for orthognathic surgery of the maxilla and the mandible.
We found that CBCT with intraoral scan of the dental cast is the most frequently used method for virtual orthognathic planning, and SimPlant (Materialise, Leuven, Belgium) and Dolphin (Dolphin Imaging, USA) are the most widely used software.
Despite its limitations, the calculation of the linear and angular differences between the virtual plan and the postoperative status is still the most frequently used method for accuracy assessment, and differences < 2 mm/° are considered acceptable.
Availability of data and materials
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CT:
-
Computed tomography
- CBCT:
-
Cone-beam computed tomography
- 2D:
-
Two-dimensional
- 3D:
-
Three dimensional
- OGS:
-
Orthognathic surgery
- MeSH:
-
Medical subject heading
- SD:
-
Standard deviation
- NA:
-
No information provided by the authors
- CMS:
-
Conventional model surgery
- VSP:
-
Vitual surgical planning
- M:
-
Male
- F:
-
Female
- FHP:
-
Frankfort horizontal plane
- CP:
-
Coronal plane
- MFP:
-
Midfacial plane
- OcPl:
-
Occlusal plane
- MdPl:
-
Mandibular plane
- N:
-
Nasion point
- ICC:
-
Intra-class correlation coefficient
- VS:
-
Virtual splint
- CS:
-
Classic splint
- NS:
-
No splint
- ANB:
-
A relationship of maxilla and mandible
- UAFH:
-
Change of upper anterior facial height
- LAFH:
-
Change of lower anterior facial height
- UAFH/LAFH:
-
Change of vertical portion of facial height
- RMSD:
-
Root-mean square difference
References
Ho CT, Lin HH, Liou EJ, Lo LJ. Three-dimensional surgical simulation improves the planning for correction of facial prognathism and asymmetry: a qualitative and quantitative study. Sci Rep. 2017;7:40423.
Xia JJ, Gateno J, Teichgraeber JF. New clinical protocol to evaluate craniomaxillofacial deformity and plan surgical correction. J Oral Maxillofac Surg. 2009;67:2093–106.
Seres L, Varga EJ, Kocsis A, Rasko Z, Bago B, Varga E, et al. Correction of a severe facial asymmetry with computerized planning and with the use of a rapid prototyped surgical template a case reporttechnique article. Head Face Med. 2014;10:27.
Adolphs N, Haberl EJ, Liu W, Keeve E, Menneking H, Hoffmeister B. Virtual planning for craniomaxillofacial surgery--7 years of experience. J Craniomaxillofac Surg. 2014;42:e289–95.
Haas OL Jr, Becker OE, de Oliveira RB. Computer-aided planning in orthognathic surgery-systematic review. Int J Oral Maxillofac Surg. 2015;44:329-42.
Hsu SS, Gateno J, Bell RB, Hirsch DL, Markiewicz MR, Teichgraeber JF, et al. Accuracy of a computer-aided surgical simulation protocol for orthognathic surgery: a prospective multicenter study. J Oral Maxillofac Surg. 2013;71:128–42.
Sun Y, Luebbers HT, Agbaje JO, Schepers S, Vrielinck L, Lambrichts I, et al. Accuracy of upper jaw positioning with intermediate splint fabrication after virtual planning in bimaxillary orthognathic surgery. J Craniofac Surg. 2013;24:1871–6.
Swennen GR, Mollemans W, De Clercq C, Abeloos J, Lamoral P, Lippens F, et al. A cone-beam computed tomography triple scan procedure to obtain a three-dimensional augmented virtual skull model appropriate for orthognathic surgery planning. J Craniofac Surg. 2009;20:297–307.
Zinser MJ, Mischkowski RA, Dreiseidler T, Thamm OC, Rothamel D, Zoller JE. Computer-assisted orthognathic surgery: waferless maxillary positioning, versatility, and accuracy of an image-guided visualisation display. Br J Oral Maxillofac Surg. 2013;51:827–33.
Farrell BB, Franco PB, Tucker MR. Virtual surgical planning in orthognathic surgery. Oral Maxillofac Surg Clin North Am. 2014;26:459–73.
Wu TY, Lin HH, Lo LJ, Ho CT. Postoperative outcomes of two- and three-dimensional planning in orthognathic surgery: a comparative study. J Plast Reconstr Aesthet Surg. 2017;70:1101–11.
Baker SB, Goldstein JA, Seruya M. Outcomes in computer-assisted surgical simulation for orthognathic surgery. J Craniofac Surg. 2012;23:509–13.
Bai S, Bo B, Bi Y, Wang B, Zhao J, Liu Y, et al. CAD/CAM surface templates as an alternative to the intermediate wafer in orthognathic surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110:e1–7.
Bai S, Shang H, Liu Y, Zhao J, Zhao Y. Computer-aided design and computer-aided manufacturing locating guides accompanied with prebent titanium plates in orthognathic surgery. J Oral Maxillofac Surg. 2012;70:2419–26.
Levine JP, Patel A, Saadeh PB, Hirsch DL. Computer-aided design and manufacturing in craniomaxillofacial surgery: the new state of the art. J Craniofac Surg. 2012;23:288–93.
Li B, Zhang L, Sun H, Yuan J, Shen SG, Wang X. A novel method of computer aided orthognathic surgery using individual CAD/CAM templates: a combination of osteotomy and repositioning guides. Br J Oral Maxillofac Surg. 2013;51:e239–44.
Polley JW, Figueroa AA. Orthognathic positioning system: intraoperative system to transfer virtual surgical plan to operating field during orthognathic surgery. J Oral Maxillofac Surg. 2013;71:911–20.
Zinser MJ, Mischkowski RA, Sailer HF, Zoller JE. Computer-assisted orthognathic surgery: feasibility study using multiple CAD/CAM surgical splints. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;113:673–87.
Sun Y, Luebbers HT, Agbaje JO, Schepers S, Vrielinck L, Lambrichts I, et al. Evaluation of 3 different registration techniques in image-guided bimaxillary surgery. J Craniofac Surg. 2013;24:1095–9.
Lin HH, Lo LJ. Three-dimensional computer-assisted surgical simulation and intraoperative navigation in orthognathic surgery: a literature review. J Formos Med Assoc. 2015;114:300–7.
Stokbro K, Aagaard E, Torkov P, Bell RB, Thygesen T. Virtual planning in orthognathic surgery. Int J Oral Maxillofac Surg. 2014;43:957–65.
de Waard O, Baan F, Verhamme L, Breuning H, Kuijpers-Jagtman AM, Maal T. A novel method for fusion of intra-oral scans and cone-beam computed tomography scans for orthognathic surgery planning. J Craniomaxillofac Surg. 2016;44:160–6.
Franz L, Isola M, Bagatto D, Calzolari F, Travan L, Robiony M. A novel protocol for planning and navigation in craniofacial surgery: a preclinical surgical study. J Oral Maxillofac Surg. 2017;75:1971–9.
Lu C, He D, Yang C, Huang D, Ellis E 3rd. Computer-assisted surgical planning and simulation for unilateral condylar benign lesions causing facial asymmetry. Oral Surg Oral Med Oral Pathol Oral Radiol. 2017;123:453–8.
Grybauskas S, Saiki C, Cintra O, Razukevičius D. A “forced symmetry”: surgical planning protocol for the treatment of posterior facial asymmetries. EJCO. 2016;4:e53–9.
Shaheen E, Sun Y, Jacobs R, Politis C. Three-dimensional printed final occlusal splint for orthognathic surgery: design and validation. Int J Oral Maxillofac Surg. 2017;46:67–71.
Steinhuber T, Brunold S, Gartner C, Offermanns V, Ulmer H, Ploder O. Is virtual surgical planning in Orthognathic surgery faster than conventional planning? A time and workflow analysis of an office-based workflow for single- and double-jaw surgery. J Oral Maxillofac Surg. 2018;76:397–407.
Wrzosek MK, Peacock ZS, Laviv A, Goldwaser BR, Ortiz R, Resnick CM, et al. Comparison of time required for traditional versus virtual orthognathic surgery treatment planning. Int J Oral Maxillofac Surg. 2016;45:1065–9.
Ying B, Ye N, Jiang Y, Liu Y, Hu J, Zhu S. Correction of facial asymmetry associated with vertical maxillary excess and mandibular prognathism by combined orthognathic surgery and guiding templates and splints fabricated by rapid prototyping technique. Int J Oral Maxillofac Surg. 2015;44:1330–6.
Hernandez-Alfaro F, Guijarro-Martinez R. New protocol for three-dimensional surgical planning and CAD/CAM splint generation in orthognathic surgery: an in vitro and in vivo study. Int J Oral Maxillofac Surg. 2013;42:1547–56.
Shehab MF, Barakat AA, AbdElghany K, Mostafa Y, Baur DA. A novel design of a computer-generated splint for vertical repositioning of the maxilla after Le fort I osteotomy. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;115:e16–25.
Uribe F, Janakiraman N, Shafer D, Nanda R. Three-dimensional cone-beam computed tomography-based virtual treatment planning and fabrication of a surgical splint for asymmetric patients: surgery first approach. Am J Orthod Dentofac Orthop. 2013;144:748–58.
Xia JJ, Gateno J, Teichgraeber JF, Christensen AM, Lasky RE, Lemoine JJ, et al. Accuracy of the computer-aided surgical simulation (CASS) system in the treatment of patients with complex craniomaxillofacial deformity: a pilot study. J Oral Maxillofac Surg. 2007;65:248–54.
Clementini M, Morlupi A, Canullo L, Agrestini C, Barlattani A. Success rate of dental implants inserted in horizontal and vertical guided bone regenerated areas: a systematic review. Int J Oral Maxillofac Surg. 2012;41:847–52.
De Riu G, Virdis PI, Meloni SM, Lumbau A, Vaira LA. Accuracy of computer-assisted orthognathic surgery. J Craniomaxillofac Surg. 2017;46:293–8.
Ritto FG, Schmitt ARM, Pimentel T, Canellas JV, Medeiros PJ. Comparison of the accuracy of maxillary position between conventional model surgery and virtual surgical planning. Int J Oral Maxillofac Surg. 2017;47:160–6.
Chin SJ, Wilde F, Neuhaus M, Schramm A, Gellrich NC, Rana M. Accuracy of virtual surgical planning of orthognathic surgery with aid of CAD/CAM fabricated surgical splint-a novel 3D analyzing algorithm. J Craniomaxillofac Surg. 2017;45:1962–70.
Stokbro K, Aagaard E, Torkov P, Bell RB, Thygesen T. Surgical accuracy of three-dimensional virtual planning: a pilot study of bimaxillary orthognathic procedures including maxillary segmentation. Int J Oral Maxillofac Surg. 2016;45:8–18.
Baan F, Liebregts J, Xi T, Schreurs R, de Koning M, Berge S, et al. A new 3D tool for assessing the accuracy of Bimaxillary surgery: the OrthoGnathicAnalyser. PLoS One. 2016;11:e0149625.
Zhang N, Liu S, Hu Z, Hu J, Zhu S, Li Y. Accuracy of virtual surgical planning in two-jaw orthognathic surgery: comparison of planned and actual results. Oral Surg Oral Med Oral Pathol Oral Radiol. 2016;122:143–51.
De Riu G, Meloni SM, Baj A, Corda A, Soma D, Tullio A. Computer-assisted orthognathic surgery for correction of facial asymmetry: results of a randomised controlled clinical trial. Br J Oral Maxillofac Surg. 2014;52:251–7.
Zinser MJ, Sailer HF, Ritter L, Braumann B, Maegele M, Zoller JE. A paradigm shift in orthognathic surgery? A comparison of navigation, computer-aided designed/computer-aided manufactured splints, and "classic" intermaxillary splints to surgical transfer of virtual orthognathic planning. J Oral Maxillofac Surg. 2013;71(2151):e1–21.
Aboul-Hosn Centenero S, Hernandez-Alfaro F. 3D planning in orthognathic surgery: CAD/CAM surgical splints and prediction of the soft and hard tissues results - our experience in 16 cases. J Craniomaxillofac Surg. 2012;40:162–8.
Lin HH, Chang HW, Lo LJ. Development of customized positioning guides using computer-aided design and manufacturing technology for orthognathic surgery. Int J Comput Assist Radiol Surg. 2015;10:2021–33.
De Vos W, Casselman J, Swennen GR. Cone-beam computerized tomography (CBCT) imaging of the oral and maxillofacial region: a systematic review of the literature. Int J Oral Maxillofac Surg. 2009;38:609–25.
Guijarro-Martinez R, Swennen GR. Cone-beam computerized tomography imaging and analysis of the upper airway: a systematic review of the literature. Int J Oral Maxillofac Surg. 2011;40:1227–37.
Lechuga L, Weidlich GA, vs CBCT, Fan Beam CT. A Comparison of Image Quality and Dose Delivered Between Two Differing CT Imaging Modalities. Cureus. 2016;8:e778.
Lee CY, Jang CS, Kim JW, Kim JY, Yang BE. Condylar repositioning using centric relation bite in bimaxillary surgery. Korean J Orthod. 2013;43:74–82.
Li Y, Jiang Y, Zhang N, Xu R, Hu J, Zhu S. Clinical feasibility and efficacy of using virtual surgical planning in bimaxillary orthognathic surgery without intermediate splint. J Craniofac Surg. 2015;26:501–5.
Griffitts TM, Tandon R, Herford AS, Dean J. Computer assisted surgical simulation versus model surgery in Orthognathic surgery: a postoperative comparison of surgical outcomes. J Oral Maxillofac Surg. 2013;71:e18.
Acknowledgements
Not applicable.
Funding
Dr. Alkhayer was supported by Stipendium Hungaricum Scholarship. Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
A.A. collected, analyzed and interpreted the data for this publication. J.P., C.L. and E.S. helped in study design and data interpretation. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1
. Virtual planning accuracy of the included studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Alkhayer, A., Piffkó, J., Lippold, C. et al. Accuracy of virtual planning in orthognathic surgery: a systematic review. Head Face Med 16, 34 (2020). https://doi.org/10.1186/s13005-020-00250-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13005-020-00250-2