
Abstract
Background
Thymofibrolipoma has been described as a variant of thymolipoma. To date, 3 cases have been reported, and the lesion have been described to consist of extensive areas of collagenous tissue interspersed with islands of mature adipose tissue and strands of thymic tissue.
Case presentation
A 43-year-old woman had an anterior mediastinal tumor. Macroscopically, the cut surface of the tumor was composed of a yellowish lipomatous component and a uniform whitish fibrous component with elastic stiffness. Microscopically, the tumor was composed of collagenous fibrous tissue with sparse spindle cells, mature adipocytes and strands or islands of thymic tissue. The spindle cells in the fibrous tissue had monoallelic deletion of the 13q14 region and corresponding loss of RB1 and FOXO1A protein expression.
Conclusions
This case report may strengthen the hypothesis that thymofibrolipoma is a neoplastic lesion and a variant of thymolipoma and that thymofibrolipoma and lipofibroadenoma are different names for the same lesion. The name “lipofibroadenoma” was given to the lesion because of its histological resemblance to fibroadenoma of the mammary gland. However, this name does not reflect the pathogenesis of this lesion, and the name “thymofibrolipoma” would be preferable. It will be necessary to discuss whether lipofibroadenoma should be listed as an independent entity in the WHO classification.
Similar content being viewed by others


Background
Thymofibrolipoma has been described as a variant of thymolipoma. It was first reported in 2001 by Moran et al., who revealed that thymofibrolipoma was composed of extensive areas of collagenous tissue interspersed with islands of mature adipose tissue and strands of thymic tissue.[1].
Case presentation
We encountered a case of thymofibrolipoma for which immunohistochemical and cytogenetic analyses were performed.
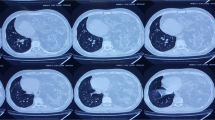
A 43-year-old woman had an anterior mediastinal tumor, and chest contrast-enhanced computed tomography was performed at a periodic health check-up for observation of a suspected thymic cyst. (Fig. 1 A) During follow-up, the tumor continued to grow slowly, and thoracoscopy-assisted mediastinal tumor resection was performed because a neoplastic lesion could not be ruled out.

Clinical images: (A) Chest computed tomography revealed a non-contrast-enhanced mass lesion in the anterior mediastinum. (White arrowhead)
Macroscopic images: (B) The cut surface of the material in the anterior mediastinal tumor showed a yellowish lipomatous component and a uniform whitish fibrous component
Macroscopically, the tumor was a mass-like lesion that had a relatively clear border with the surrounding thymus. The cut surface of the tumor was composed of a yellowish lipomatous component and a uniform whitish fibrous component with elastic stiffness. (Fig. 1B) Microscopically, the whitish fibrous component was mainly composed of fibrous tissue with sparse spindle cells against a background of collagenous fibers. The fibrous tissue was accompanied by strands of thymic tissue, islands of adipocytes and scattered area of calcifications. (Figs. 2 A, 2B) In the yellowish lipomatous component, mature adipocytes and strands or islands of thymic tissue with small lymphocytes were observed. (Fig. 2 C) As a minor component, fibrous tissue was also observed in the lipomatous component. (Fig. 2D) Age-appropriate atrophic thymic tissue was found in the partially resected nontumor area. No neoplastic or hyperplastic lesions were found.

Microscopic images: Collagenous tissue accompanied by strands or islands of thymic tissue and scattered mature adipose tissue, (A) A low-magnification image (B) A high-magnification image
Microscopic images: (C) Adipose tissue accompanied by strands or islands of thymic tissue. (D) Adipose tissue accompanied by collagenous tissue and scattered calcifications
The strands or islands of thymic tissue were composed of CK19(+) thymic epithelial cells and small lymphocytes, which were predominantly immature T lymphocytes showing the following profile: CD20(-), CD3(+), CD99(+), and TdT(+). Hassall bodies were also observed in some thymic tissue. The spindle cells in the fibrous tissue showed SMA and CD34 expression and had lost RB1 and FOXO1A expression. (Figs. 3 A, 3B, 3 C) Fluorescence in situ hybridization (FISH) analysis using a probe specific for chromosome 13q14 (Vysis LSI D13s319/13q34 FISH Probe Kit, Abbott, Abbott Park, IL) detected a single signal in the tumor cells and two signals in the nuclei of normal cells, demonstrating monoallelic deletion of the 13q14 region in the tumor cells. (Fig. 3D) Based on the morphological and immunohistochemical analyses, we diagnosed the tumor as a thymofibrolipoma. The patient was discharged uneventfully. During the 8-month follow-up period, the patient did not show any evidence of recurrence or metastasis.

Immunohistochemical images: Spindle cells stained positive for CD34 (A) and negative for RB1 (B) and FOXOA1 (C)
Fluorescence in situ hybridization assay: (D) Monoallelic loss of the 13q14 region was found. (White arrow: D13S319 probe red signal, white arrowhead: 13q34 probe green signal)
Discussion and conclusions
Thymolipoma is classified in the current WHO classification as a mesenchymal tumor of the mediastinum.[2] It is a benign tumor composed of a mixture of mature adipose tissue and nonneoplastic thymic tissue. Thymofibrolipoma has been reported as a variant of thymolipoma, and to date, 3 cases have been reported.[1, 3] Thymofibrolipoma was first described in 2001 by Moran et al., who revealed that it was composed of extensive areas of collagenous tissue interspersed with islands of mature adipose tissue and strands of thymic tissue.[1] One report described chromosomal abnormalities, suggesting that thymolipoma may be a neoplastic lesion.[4] In our case, monoallelic 13q14 deletion and the corresponding loss of RB1 and FOXO1A protein expression were found. Monoallelic 13q14 deletion has been found in certain neoplasms, including spindle cell/pleomorphic lipoma, cellular angiofibroma and myofibroblastoma.[5, 6] Whether this finding is a coincidence or a recurrent feature will require further investigation, but if it is a recurrent feature, it may strengthen the hypothesis that thymofibrolipoma is a neoplastic lesion and a variant of thymolipoma.
Variants of lipoma (angiolipoma, chondroid lipoma, myolipoma, myelolipoma, etc.) differ from conventional lipoma in terms of their characteristic microscopic features.[6] One variant of lipoma, called sclerotic lipoma, was characterized as having a prominent fibrosclerotic stromal matrix.[7] As there are many variants of soft tissue lipoma, it is not surprising that there would be many variants of thymolipoma if thymolipoma is a neoplastic lipomatous lesion. Just as sclerotic lipoma is a variant of soft tissue lipoma, thymofibrolipoma may be a variant of thymolipoma.
The current WHO classification lists lipofibroadenoma as a rare form of thymoma.[2] To date, 12 cases have been reported.[8,9,10,11,12,13,14,15,16,17,18,19] Lipofibroadenoma was first described in 2001 by Kuo et al., who revealed a histology similar to that of fibroadenoma of the mammary gland, namely, that lipofibroadenoma was composed of fibrotic and hyaline stroma interspersed with narrow strands of thymic tissue and mature adipose tissue.[8].
To date, 12 cases of lipofibroadenoma and 3 cases of thymofibrolipoma have been reported. In all reported cases, extensive areas of collagenous tissue interspersed with islands of mature adipose tissue and strands of thymic tissue are the main microscopic features. (Supplementary Tables 1, 2) Based on the descriptions of the histopathological features and microscopic figures of lipofibroadenoma and thymofibrolipoma in previous reports, it is possible that they are different names for the same lesion.
The name “lipofibroadenoma” was given to the lesion because of its histological resemblance to fibroadenoma of the mammary gland.[8] However, the thymic epithelial cells in this lesion had morphological and immunohistochemical features consistent with normal thymic components; thus, its name does not reflect the pathogenesis of this lesion. If our hypothesis that thymofibrolipoma is a neoplastic lesion and a variant of thymolipoma, described in the previous paragraph, is correct, the name “thymofibrolipoma” may be preferable.
The current WHO classification lists lipofibroadenoma as an independent entity of thymoma; however, as we have suggested in our report, if thymofibrolipoma, as a subtype of thymolipoma, and lipofibroadenoma refer to the same lesion by different names, it would be necessary to discuss whether it is appropriate to describe lipofibroadenoma as an independent entity.
Data Availability
All data generated or analyzed during this study are included in this published article.
Abbreviations
- FISH:
-
Fluorescence in situ hybridization
References:
Moran CA, Zeren H, Koss MN. Thymofibrolipoma. A histologic variant of thymolipoma. Arch Pathol Lab Med. 1994;118:281–2.
WHO Classification of Tumours Editorial Board. Thoracic Tumours. International Agency for Research on Cancer.; 2021.
Kang G-H, Han J, Kim TS, Choi YS, Um S-W. Thymofibrolipoma - A brief case report -. Korean J Pathol. The Korean Society of Pathologists and The Korean Society for Cytopathology; 2010;44:338.
Hudacko R, Aviv H, Langenfeld J, Fyfe B. Thymolipoma: clues to pathogenesis revealed by cytogenetics. Ann Diagn Pathol. 2009;13:185–8.
Flucke U, van Krieken JHJM, Mentzel T. Cellular angiofibroma: analysis of 25 cases emphasizing its relationship to spindle cell lipoma and mammary-type myofibroblastoma. Mod Pathol. 2011;24:82–9.
WHO Classification of Tumours Editorial Board. Soft Tissue and Bone Tumours. International Agency for Research on Cancer; 2020.
Laskin WB, Fetsch JF, Michal M, Miettinen M. Sclerotic (fibroma-like) lipoma: a distinctive lipoma variant with a predilection for the distal extremities. Am J Dermatopathol. 2006;28:308–16.
Kuo T, Shih LY. Histologic types of thymoma associated with pure red cell aplasia: a study of five cases including a composite tumor of organoid thymoma associated with an unusual lipofibroadenoma. Int J Surg Pathol. 2001;9:29–35.
Onuki T, Iguchi K, Inagaki M, Suzuki K. [Lipofibroadenoma of the thymus]. Kyobu Geka. 2009;62:395–8.
Wang Y-L, Yi X-H, Chen G, Wu C-Y. [Thymoma associated with an lipofibroadenoma: report of a case]. Zhonghua Bing Li Xue Za Zhi. 2009;38:556–7.
Aydin Y, Sipal S, Celik M, Araz O, Ulas AB, Alper F, et al. A rare thymoma type presenting as a giant intrathoracic tumor: lipofibroadenoma. Eurasian J Med. 2012;44:176–8.
Qu G, Yu G, Zhang Q, Ma J, Wang X. Lipofibroadenoma of the thymus: a case report. Diagn Pathol. 2013;8:117.
Makdisi G, Roden AC, Shen KR. Successful Resection of Giant Mediastinal Lipofibroadenoma of the Thymus by Video-Assisted Thoracoscopic Surgery. Ann Thorac Surg. 2015;100:698–700.
Hamada K, Kaseda K, Omura S, Suzuki M, Tanaka H, Suzuki Y, et al. A Case of Lipofibroadenoma of the Thymus. Japanese J Lung Cancer Japan Lung Cancer Soc. 2018;58:237–8.
Kojima I, Matsuyama T, Tateyama H, Horibe Y. A case of lipofibroadenoma of the thymus. Pathol and Clin Med. 2018;36:265–9.
Akkaya B, Yilmaz DB, Ozbudak IH, Sarper A. Lipofibroadenoma of the thymus: a case report. Virchows Arch. 2018;473:272.
Hui M, Paul TR, Uppin SG, Jyothi N. Lipofibroadenoma with B1 thymoma: A case report of a rare thymic tumor. Indian J Pathol Microbiol. 2018;61:630–2.
Hakiri S, Kawaguchi K, Tateyama H, Fukui T, Nakamura S, Ozeki N, et al. Thymic lipofibroadenoma accompanied with largish calcifications. Gen Thorac Cardiovasc Surg. 2021;69:394–7.
Bolca C, Has A, Bobocea A, Afetelor A, Stoica R, Strambu I, et al. A Rare Thymic Tumor - Lipofibroadenoma - Always a Postoperative Surprise. Vivo. 2021;35:3623–6.
Acknowledgements
The authors thank Makoto Tamagaki and Kumiko Hayashi, Department of Gene Analysis, LSI Medience Corporation, for FISH analysis.
Funding
The authors declare that they have no financial support.
Authors’ contributions.
RJ was responsible for the histological and cytogenetic studies, review of the literature, writing the manuscript and processing digital images. ET performed surgery and provided clinical information. All authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jokoji, R., Tomita, E. Thymofibrolipoma: a case report and review of the literature. Diagn Pathol 17, 77 (2022). https://doi.org/10.1186/s13000-022-01260-1
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13000-022-01260-1