
Abstract
The occurrence of endocrine cell micronests in ovarian tumors is rarely reported. To our knowledge, there are only three prior cases reported to date: one occurring in an ovarian mucinous cystadenoma, one in an ovarian mucinous cystadenofibroma, and another in an ovarian mucinous carcinoma with a predominant borderline component. This is a 27-year-old woman that presented with a one-month history of abdominal pain and fullness. Imaging studies revealed a large multiloculated cystic and solid mass measuring 23 cm occupying the majority of the pelvis and abdomen concerning for a primary ovarian malignancy. The patient underwent a right salpingo-oophorectomy with appendectomy. Histologic sections from the ovary showed a multiloculated, cystic and focally solid mass lined by gastrointestinal-type mucinous epithelium with variable degrees of proliferation accounting for greater than 10% of the tumor. In addition to the mucinous epithelial component, there were several foci of bland, monotonous epithelioid cells arranged in solid nests with focal tubular/acinar formation within the fibrous septa and mucinous epithelium. Immunohistochemical studies showed that these cells were positive for cytokeratin, EMA, and synaptophysin, while negative for inhibin. The Ki-67 proliferation index was low (<1%). The presence of endocrine cell nests associated with an ovarian mucinous neoplasm is a rare phenomenon. Whether this represents preservation of endocrine cells in the context of epithelial degeneration or an independent neoplastic component is unclear. Progression related to this endocrine cell proliferation is unlikely and the recognition of this phenomenon holds more diagnostic value than prognostic significance, as it could be confused with microinvasion or sex cord stromal elements.
Similar content being viewed by others


Introduction
Mucinous tumors represent 10-15% of primary ovarian neoplasms and can be divided into three groups based on malignant behavior: benign, borderline, or malignant histologic variants [1]. Among benign ovarian tumors, mucinous cystadenomas and mucinous adenofibromas account for approximately 75% of cases. The second most common, borderline ovarian tumors or atypical proliferative ovarian tumors, account for approximately 15-20%. The remaining 5% of cases represent invasive primary ovarian mucinous carcinomas [1, 2]. In addition to gastrointestinal-type mucinous epithelium, the presence of endocrine cells in ovarian mucinous neoplasms has been recognized for decades [3,4,5,6]. The endocrine cells are frequently inconspicuous when they are distributed as scattered single cells in the mucinous glands on routine hematoxylin and eosin-stained (H&E) sections, but can be highlighted by use of special stains or immunohistochemistry. Though infrequent, endocrine cell proliferation can be found within the epithelium and stroma and can give rise to rare cases of mixed ovarian tumors composed of a combination of epithelial and endocrine elements [7,8,9,10].
Herein, we describe a case of ovarian mucinous borderline tumor with foci of microscopic endocrine cell nests in the stroma and adjacent mucinous epithelium. The endocrine cells are predominantly distributed in reactive stroma adjacent to glandular elements in various stages of degeneration. This histologic observation lends support to the theory that endocrine cell micronests are preserved endocrine cells in the context of glandular degeneration [8, 10]. The awareness of this phenomenon is helpful in diagnosis as endocrine cell micronests may show overlapping morphologic features with microinvasion or sex cord-stromal elements.
Case report
The patient is a 27-year-old woman with no significant past medical history that presented with a one-month history of abdominal pain and fullness. Computed tomography (CT) scan revealed a complex, cystic right ovarian mass with internal septations and solid component occupying a majority of the pelvis and abdomen with prominent pelvic sidewall adenopathy. Preoperative serum CA- 125 was elevated at 174.9 U/mL (reference range: 0-35 U/mL). The patient underwent right salpingo-oophorectomy with appendectomy. The ovarian tumor measured 23 cm and weighed 2,890 g with a smooth and glistening intact capsule and an attached fimbriated fallopian tube. Sectioning of the mass revealed a multiloculated, cystic mass containing clear, watery serous fluid and thin mucoid material. The cysts were thin-walled with predominantly a smooth lining and focal solid growth (accounting for approximately 15-20%). On histologic examination, the cysts were lined by gastrointestinal-type mucinous epithelium with variable degrees of proliferation accounting for greater than 10% of the tumor (Fig. 1A and B). In addition to the mucinous epithelial component, there were several foci of bland, monotonous epithelioid cells arranged in solid nests with focal tubular/acinar arrangement scattered within the stroma and adjacent to and intermingled with mucinous epithelium (Fig. 1C and D). These epithelioid cells were generally uniform with bland, round nuclei, fine chromatin, and arranged in linear or micronodular clusters of at least 5 cells. No cytologic atypia or mitotic activity was identified. No teratomatous elements were identified despite extensive sampling of the tumor. Immunohistochemical studies showed that the epithelioid cells were positive for cytokeratin and EMA, while negative for inhibin (Fig. 1E and F). Synaptophysin highlighted individual cells and small nests of endocrine cells in adjacent mucinous glands. The Ki-67 proliferation index was low (<1%). The endocrine cell proliferations were focally present and often associated with outpouchings from large mucinous cysts (Fig. 2A), frequently noted adjacent to mucinous glands with degeneration (Fig. 2B and C), and associated with foamy histiocytes in areas with completely obliterated mucinous glands were occasionally seen (Fig. 2D).

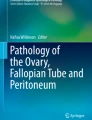
A, The cysts are lined by gastrointestinal-type mucinous epithelium with variable degrees of epithelial proliferation. B, Higher magnification demonstrating mucinous epithelium with goblet cells and nuclear atypia. C, There are several foci of bland, monotonous epithelioid cells arranged in solid nests or tubular/acinar architecture in reactive stroma adjacent to mucinous epithelium. The bland epithelioid cells can also be seen in adjacent mucinous glands (arrow). D, Florid stromal micronests are seen focally and cells emanating from a mucinous gland are present (arrow). E, Pancytokeratin (AE1/AE3) immunostaining highlights both mucinous epithelium and the stromal micronests. F, Synaptophysin immunostaining highlights the endocrine cell micronests in the stroma as well as intraepithelial neuroendocrine cells in adjacent mucinous glands

A, Endocrine cell micronests are seen in stroma adjacent to the mucinous cysts and their outpouching glands (arrow). B, Mucinous glands in early stage of degeneration with intraluminal neutrophils and stroma with reactive changes, histiocytes, and endocrine cell micronests. C, Round to ovoid shaped histiocytic infiltrates with endocrine cell micronests at the periphery, representing the late-stage glandular degeneration with preserved endocrine cells. D. Synaptophysin immunostaining highlights stromal endocrine cell micronests and intraepithelial neuroendocrine cells. A completely degenerated mucinous cyst with preserved neuroendocrine cells (arrow) is seen adjacent to a relatively intact mucinous cyst demonstrating intraepithelial neuroendocrine cells with variable degrees of proliferation (arrowhead)
Discussion
Endocrine cells can be found in multiple organs throughout the body, but largely in the lungs, pancreas, and gastrointestinal tract. They may be seen as an inconsequential (minor) component of epithelial tumors or as a larger proportion of epithelial, germ cell, or sex cord stromal cell tumors. The presence of endocrine cell micronests associated with an ovarian mucinous neoplasm is a rare phenomenon that might cause diagnostic confusion when encountered. Whether this represents preservation of endocrine cells in the context of epithelial degeneration or an independent neoplastic component is unclear. Progression related to this endocrine cell proliferation is unlikely and the recognition of this phenomenon holds more diagnostic value than prognostic significance.
To our knowledge only 4 cases, including the present case, have been previously reported in mucinous neoplasia of the ovary (Table 1). In the first report, in addition to increased intraglandular endocrine cells, multiple foci of isolated endocrine cells and small nests were observed in fibrous stroma surrounding mucinous glands. This was thought to represent diffuse endocrine cell hyperplasia within a mucinous cystadenofibroma [7]. Similarly, in the second report, multifocal stromal endocrine cell nests were associated with increased intraglandular endocrine cells in the borderline component of mucinous carcinoma [8]. In the third report, the stroma showed multiple nests of endocrine cells with occasional follicle-like structures and was suggested to represent preservation of endocrine cells in the context of a degenerative phenomenon rather than true endocrine cell hyperplasia [10]. The mucinous epithelium often demonstrates morphologic features and immunophenotype suggestive of intestinal differentiation [11, 12]. As in our current case, the stromal endocrine cell micronests in previously reported cases demonstrated bland cytological features without atypia or mitotic activity. The endocrine cell micronests were immunoreactive for CK7, chromogranin, synaptophysin, and CD56 with negative reactions for CK20. The differential diagnosis in our case initially included sex cord stromal elements or microinvasion of the mucinous neoplasm [10, 13]. The focal continuity of endocrine cell clusters with adjacent mucinous glands and the presence of intraglandular endocrine cell proliferation provided useful diagnostic clues. Given the periglandular location with patchy distribution of endocrine cell micronests, the diagnosis of tumor microinvasion in the setting of a mucinous borderline tumor may be entertained; however, unlike microinvasion, endocrine cell micronests show classic neuroendocrine cytomorphology and are morphologically distinct from adjacent mucinous epithelium. Immunohistochemical studies with antibodies directed against neuroendocrine markers can aid in recognizing these endocrine cells when arranged in small solid nests with limited cell quantity and distinction from tumor microinvasion is not straightforward.
Interestingly, the presence of stromal endocrine cell micronests and endocrine cell hyperplasia in adjacent mucinous glands, as in our case, are similar to those seen in autoimmune gastritis/chronic atrophic gastritis [14,15,16]. The majority of ovarian carcinoid tumors are associated with teratomatous components or by themselves, considered to be of germ cell origin. Cases of ovarian carcinoid tumors arising in the setting of ovarian mucinous neoplasms have been reported [17, 18]. The distinction between endocrine cell micronests and carcinoid/well-differentiated neuroendocrine tumor is somewhat subjective, but neuroendocrine tumors tend to be large, often with an expansile rather than infiltrative growth pattern and the tumor cells are arranged in insular, trabecular, or solid patterns with associated hyalinized, fibrotic stroma which are lacking with benign endocrine cell micronests [15].
An observation that is worth mentioning is the close spatial relationship between stromal endocrine cell micronests and mucinous glands with degeneration. As in our case, it is not uncommon to see neuroendocrine cells within reactive stroma with foamy histiocytic infiltration adjacent to degenerated mucinous epithelium. Our morphologic findings offer convincing evidence in support of preservation of endocrine cells in the setting of mucinous glandular degeneration as the most plausible underlying pathogenesis of stromal endocrine cell micronests [10]. The intraglandular endocrine cells are not evenly distributed in the mucinous epithelium and when present they may be arranged in single-cell fashion as well as aggregates that are clearly evident on routine H&E stain. These findings suggest that a background endocrine cell hyperplasia does exist and is similar to two previous reported cases [7, 8]. As mentioned earlier, the distinction between endocrine cell micronests and a neuroendocrine tumor can be difficult and sometimes arbitrary. There is no clear evidence of using Ki-67 labeling index as a prognostic marker in the setting of primary ovarian carcinoid tumors. However, Ki-67 labeling index may provide some useful information when metastatic neuroendocrine tumors from other organs are considered. These tumors often exhibit a higher Ki-67 labeling index compared to primary ovarian carcinoid tumors and portend a worse prognosis [19].
In summary, we report a mucinous borderline tumor with endocrine cell micronests that most likely represents preservation of endocrine cells in the setting of mucinous gland degeneration. Careful consideration of the histological and immunohistochemical features will help to avoid misinterpretation as microinvasion or sex cord stromal elements. Extensive sampling and a diligent search for any teratomatous components will exclude ovarian teratoma as a diagnostic consideration. We conclude that the presence of endocrine cell micronests are likely a benign morphological finding and although rarely reported, is a more common occurrence that is under-reported and should be interpreted as clinically insignificant when encountered.
Availability of data and materials
Not applicable.
References
Prat J, D’Angelo E, Espinosa I. Ovarian carcinomas: at least five different diseases with distinct histological features and molecular genetics. Hum Pathol. 2018;80:11–27.
Vang R, Longacre TA, Köbel M, Ramalingam P, Khunamornpong S. Mucinous carcinoma of the ovary. In: WHO Classification of Tumours Editorial Board. Female Genital Tumours, vol 4. 5th ed. Lyon: International Agency for Research on Cancer; 2020.
Klemi PJ. Pathology of mucinous ovarian cystadenomas. I. Argyrophil and argentaffin cells and epithelial mucosubstances. Acta Pathol Microbiol Scand A. 1978;86A(6):465–70.
Louwerens JK, Schaberg A, Bosman FT. Neuroendocrine cells in cystic mucinous tumours of the ovary. Histopathology. 1983;7(3):389–98.
Aguirre P, Scully RE, Dayal Y, DeLellis RA. Mucinous tumors of the ovary with argyrophil cells. Am J Surg Pathol. 1984;8(5):345–56.
Fox H, Kazzaz B, Langley FA. Argyrophil and argentaffin cells in the female genital tract and in ovarian mucinous cysts. J Pathol Bacteriol. 1964;88:479–88.
Ishikura H, Shibata M, Yoshiki T. Endocrine cell micronests in an ovarian mucinous cystadenofibroma: a mimic of microinvasion. Int J Gynecol Pathol. 1999;18(4):392–5.
Stewart CJR, Leung YC. Ovarian mucinous tumour with multifocal endocrine cell micronests. Pathology. 2008;40(1):91–3.
Eichhorn JH, Young RH. Neuroendocrine tumors of the genital tract. Am J Clin Pathol. 2001;115(suppl 1):S94-112.
Stewart CJR, Harding S. Stromal endocrine cell micronests associated with an ovarian mucinous cystadenoma: endocrine cell preservation (pseudohyperplasia) potentially mimicking stromal sex cord proliferation or tumor microinvasion. Int J Gynecol Pathol. 2021;40(1):56–9.
Jaffee IM, Rahmani M, Singhal MG, Younes M. Expression of the intestinal transcription factor CDX2 in carcinoid tumors is a marker of midgut origin. Arch Pathol Lab Med. 2006;130(10):1522–6.
Sangoi AR, Ohgami RS, Pai RK, Beck AH, McKenney JK, Pai RK. PAX8 expression reliably distinguishes pancreatic well-differentiated neuroendocrine tumors from ileal and pulmonary well-differentiated neuroendocrine tumors and pancreatic acinar cell carcinoma. Mod Pathol. 2011;24(3):412–24.
Clement PB, Young RH, Scully RE. Ovarian granulosa cell proliferations of pregnancy: a report of nine cases. Hum Pathol. 1988;19(6):657–62.
Iwai K, Yao T, Nakamura S, et al. Multiple gastric carcinoids and endocrine cell micronests in type A gastritis: nuclear morphometric and immunohistochemical analysis. Oncol Rep. 2005;13(3):397–404.
Itsuno M, Watanabe H, Iwafuchi M, et al. Multiple carcinoids and endocrine cell micronests in type A gastritis. Their morphology, histogenesis and natural history. Cancer. 1989;63(5):881–90.
Solcia E, Fiocca R, Villani L, Luinetti O, Capella C. Hyperplastic, dysplastic, and neoplastic enterochromaffin-like-cell proliferations of the gastric mucosa. Classification and histogenesis. Am J Surg Pathol. 1995;19(Suppl 1):S1–7.
Robboy SJ, Norris HJ, Scully RE. Insular carcinoid primary in the ovary. A clinicopathologic analysis of 48 cases. Cancer. 1975;36(2):404–18.
Robboy SJ. Insular carcinoid of ovary associated with malignant mucinous tumors. Cancer. 1984;54(10):2273–6.
Zhang X, Jones A, Jenkins SM, Huang Y. Ki67 proliferative index in carcinoid tumors involving ovary. Endocr Pathol. 2018;29(1):43–8.
Acknowledgements
The skillful photographic assistance of Fredrik Skarstedt is gratefully acknowledged.
Funding
The authors do not have a conflict of interest associated with this publication, and there has been no significant financial support for this work that could have influenced its outcome.
Author information
Authors and Affiliations
Contributions
KC, SS, and MH performed the histological examination of the case. KC and MH wrote the manuscript and reviewed the scientific literature and were major contributors in writing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We confirm all relevant ethical guidelines have been followed. We consulted with the Institutional Review Board/Research Ethic Committee of Indiana University who determined that ethical approval was not applicable because this article does not contain any studies with human or animal subjects.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Collins, K., Segura, S. & Hwang, M. Endocrine cell micronests in an ovarian mucinous borderline tumor: a potential diagnostic pitfall for microinvasion. Diagn Pathol 17, 37 (2022). https://doi.org/10.1186/s13000-022-01217-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13000-022-01217-4