
Abstract
Background
While morphological changes to the cervical spine have been observed for over 40 years in response to contact sport participation, little is known about the secondary effects of the cervical impairment on future musculoskeletal injury and disability.
Objectives and design
A scoping review was performed to discuss the relationship between contact sport participation and morphological changes to the cervical spine. Moreover, the correlation between morphological changes in the musculoskeletal structures of the cervical spine and resultant deficits in cervical sensorimotor and neuromotor function are discussed. Lastly, how alterations in cervical sensorimotor function may affect overall risk of musculoskeletal injury is discussed.
Methods
The scientific literature was searched in PubMed, Sport Discus, and Web of Science pertaining to contact-sport athletes and/or cervical pathology and the cervicocephalic network. The Asksey and O’Malley’s framework and PRISMA for Scoping Reviews were used to conduct and report the following review. Included articles were grouped into three categories: (1) Morphological changes to the cervical spine in contact sport athletes. (2) The role of the neuromotor pathways of the cervical spine in maintenance of postural tone and coordination of the extremities. (3) The correlation between altered cervical sensorimotor function and a resultant increase in musculoskeletal injury risk.
Results
Our search identified 566 documents, of which 405 underwent full-text screening, resulting in 54 eligible studies for the review. Widespread cervical sensorimotor dysfunction was observed in contact sport athletes. Independently, cervical sensorimotor function was demonstrated to play a critical role in postural control and limb coordination. However, limited research exists exploring the interaction between contact sport participation and altered cervical sensorimotor function, as well as an associated increase in musculoskeletal injury risk.
Conclusions
Limited evidence exists linking cervical injury and/or observed deficits in cervical sensorimotor and neuromotor function to musculoskeletal injury risk. Longitudinal studies combining imaging measures (e.g., MRI, DEXA), cervical functional test, and prospective injury risk are needed to further explore the correlation between resultant cervical sensorimotor deficits following contact sport impacts and future musculoskeletal injury risk.
Similar content being viewed by others


Background
For over 40 years, morphological changes to the musculoskeletal structures of cervical spine have been observed in contact sport athletes [1,2,3,4]. These changes are thought to be a result of mechanical loads to the musculoskeletal structures of the cervical spine, which modulate up to 80% of the mechanical forces applied to the body following sports-related repetitive head impacts (RHI) [5]. RHI are thought to play a catalytic role in early degeneration of the cervical spine, including cervical stenosis, degenerative disk disease, osteoarthritis, and spondylosis/spondylolisthesis [3, 6,7,8,9]. Moreover, acute musculoskeletal injuries to the cervical spine, such as cervical strains, fractures, and sprains, frequently develop into more chronic disability lasting up to 24 months and beyond [10, 11]. Understanding the relationship between RHI and degeneration of the musculoskeletal components of the cervical spine is critical to weigh the risks and benefits of contact sport participation [12].
In addition to the morphological changes to the musculoskeletal structures of the cervical spine, alterations in the neuromotor and sensory pathways of the cervical spine have been identified in contact sport athletes. For example, alterations in cervical joint position error, cervical strength, and cervical range of motion have been observed in individuals with a history of contact sport participation as well as following exposure to instrumented RHI [13,14,15,16]. Preliminary studies have subsequently linked decreased cervical joint position error, cervical weakness, decreased static posture, and inhibited trunk activation to an increased risk of suffering future injury (e.g., lateral ankle sprain, anterior cruciate ligament tear, concussion) [17,18,19]. These studies highlight preliminary evidence of a relationship between RHI and future injury through alterations in the neuromotor pathways and decreased functional capacities of the cervical spine. The neuromuscular and sensory pathways of the cervical spine and brain form the cervicocephalic connection, which serves as a vital component of postural tone and neuromuscular coordination [20,21,22,23]. Cervical afferent signals work synergistically with efferent motor signals to coordinate the position of limbs throughout sports-related task [20,21,22, 24].
Despite frequent observations of cervical deficits in contact sport athletes, little research has focused on how those morphological changes impact the complex neurological connections between the brain and the cervical spine, which form the cervicocephalic connection. Moreover, limited research has investigated the connection between cervical deficits and prospective musculoskeletal injury risk, despite the strong documented relationships between the cervicocephalic pathways and neuromotor coordination of the limbs [20, 21, 25].
Due to the paucity of research in understanding the direct causal relationship between RHI and subsequent increased cervical dyskinesia, we established the following purposes for this scoping review: (1) Summarize evidence detailing acute and chronic morphological changes to the cervical spine in response to exposure to contact sport participation. (2) Briefly describe the cervicocephalic network and its role in proper maintenance of head position, postural tone, and coordination of the extremities. (3) Summarize existing research pertaining to a theoretical likelihood of an increase in injury risk due to altered cervical sensorimotor function in a useful way for practitioners and other relevant stakeholders. (4) Identify gaps in existing literature detailing the connection between contact sport participation, cervical disability, decreased cervical sensorimotor function, and consequential resultant changes in musculoskeletal injury risk.
Methods
We conducted a scoping review, as this approach is superior in addressing an exploratory research question [26,27,28]. Working within the preferred reporting items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR), we followed the framework of Arksey and O’malley [26], incorporating adaptations from Levac et al. and Joanna Briggs Institute [28, 29]. At the initiation of this review, there were no databases for registering a priori scoping review strategies.
Stage 1: Identify the research question(s)
Research Questions:
-
1.
What is known about damage to the cervical spine and neuropathways in response to contact sport participation?
-
2.
What is the role of cervical sensorimotor function in posture maintenance and neuromuscular control of the extremities?
-
3.
What is the relationship between changes in cervical sensorimotor, neuromuscular control deficits, and increased risk of injury?
Stage 2: Identify relevant studies
Inclusion Criteria
-
Articles of any study design or source (peer-reviewed, grey literature, reviews)
-
All age groups and sexes
-
Contact sport athletes (e.g., hockey, lacrosse, American football, soccer, rugby, Australian football, wrestling)
-
Musculoskeletal injury, head impacts, and or degenerative condition affecting the cervical spine
Exclusion Criteria
-
Abstracts where no full-text was available
-
Case reports
-
Not published in the English language
-
Step 1 Initial limited search
An initial limited search (May 2021) was conducted. The search terms used were “contact sport” AND “cervical spine”. A total of 122 articles were reviewed. Twenty-two studies were included, with the references from those studies being reviewed for further relevant papers. The entire search strategy is detailed in Additional file 1: Appendix A.
-
Step 2 Identify key words and index terms
The title, abstract, and index terms used to describe the articles identified in step 1 were analyzed. The first search focused on prevalence of cervical pathology in contact sport athletes. Separately, articles that demonstrated the connections between cervical kinesthesia and postural control unrelated to contact sport participation were searched. Lastly, a search for studies that combined these two concepts was performed.
For the preliminary search ‘Cervical Spine’ and ‘Sport’ were set as the primary research terms. Secondary search terms (Additional file 1: Appendix A) were then added along with Boolean terms AND and OR. This process was then repeated with search terms ‘cervical kinesthesia’ and ‘posture’ to stratify evidence related to cervicocephalic connection. Lastly, ProQuest database as well as google scholar were searched to explore potential grey literature.
-
Step 3 Further Searching of references and citations
A final search of the reference list of identified articles was performed. A completed final search strategy is shown in Additional file 1: Appendix A.
Stage 3: Study selection
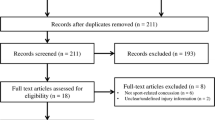
Titles and abstracts were evaluated by two reviewers (KC and KK). A third reviewer (JK) completed a random sample of 20% of the titles and abstracts as a quality check and achieved concordance > 97% regarding the decision of each article [28,29,30]. Additional file 1: Appendix B details the selection and screening criteria. All titles and abstracts were reviewed independently, and any disagreement was discussed and the full-text was reviewed. A Prisma flow diagram (Fig. 1) details articles excluded at each step.

Scoping review flow chart
Stage 4: Charting the data
KC and KK independently trialed the data extraction form which included: author(s), year of publication, aims/purpose, participants, methodology, outcomes, intervention type, and key findings on 10 selected studies. Following this step, KC extracted data from 90% of included studies, and KK extracted data from 10% of the studies. Following data extraction, KC reviewed those studies extracted by KK while KK reviewed 10% of the studies that KC extracted. Ninety-five percent overall concordance was established, in agreement with previously published scoping reviews thus, no further cross-checking was performed [28, 29]. Table 1 presents a summary of each article identified in the scoping review.
Stage 5: Collating, summarizing, and reporting the results
The methods employed throughout this protocol enabled us to collate existing knowledge and summarize the data in the following ways
-
1.
A numerical and descriptive analysis, mapping of data within a scoping review flow chart.
-
2.
An inductive thematic summary and analysis describing to the research questions and aims, based on the analysis on Braum and Clarke’s six-phase framework.
Results
Descriptive analysis
Our initial search identified 564 documents. Of these, 519 were within databases/search platforms and 45 from grey literature (Fig. 1). After duplicates were excluded, 378 records remained. An additional 28 potential studies were identified during step 3. In total, 406 articles underwent screening, and 315 records were excluded following abstract screening. An additional 37 were removed after reading full text. As a result, the scoping review identified 54 eligible studies (Fig. 1).
Included studies by year of publication
As consistent across the wider bibliometric trends, a substantial chronological increase in the number of relevant papers was identified over the previous 50 years (Fig. 2).

Included studies by year of publication
Type of study
Study design
The studies varied in terms of study design and primary focus. No formal quality assessment of included studies was performed, as scoping reviews are intended to provide a map of what evidence has been produced as opposed to seeking only the best available evidence to create policy or answer evidence-based practice questions [26, 30]. A taxonomy of research designs included in this scoping review is shown in Fig. 3.

Taxonomy of research designs for included literature
Theme of the study
Each included study fit into one of 3 themes which were further divided up into subthemes to accomplish the 4 purposes outlined in the introduction.
Theme 1: Cervical spine and contact sport participation
Thirty-three articles detailed the relationship between contact sport participation and the cervical spine. These articles present the evidence relating to the effects of contact sport participation on the cervical spine congruent with our first purpose. These studies provided consistent evidence of damage to the structures of the cervical spine responsible for maintaining the cervicocepahlic connection. Three secondary themes, including: (1) epidemiology of cervical injuries; (2) morphological changes to the cervical spine; and (3) return to play considerations emerged.
Epidemiology of cervical injuries in contact sport athletes
Three studies identified 223 catastrophic cervical injuries [31,32,33]. Representing an incidence rate of 0.52 in high school, 1.55 in college, and 14.00 in professional football for every 100,000 participants [31, 33]. Five epidemiological studies explored the prevalence of acute head and neck injuries in contact sport athletes [34,35,36,37,38]. Among the collegiate population, an estimated 7496 total cervical spine injuries between 2009–2010 to 2013–2014 were extrapolated from a smaller observed population, creating an estimated injury rate of 2.91 per 10,000 athlete exposure (AE) [34]. Stinger was the most common cervical injury (1.8/10,000 AE), followed by cervical strains (0.8/10,000 AEs) [34]. Among high school students, time loss cervical spine injuries were estimated at 3.04 per 100,000 AEs [36]. The most frequent mechanism of a cervical injury was contact with another player (70–85%) followed by contact with the ground (15–20%) [35, 36].
Two prospective studies explored head and neck injuries in professional soccer athletes [39, 40]. The incidence rate was 0.17–12.5/1000 player hours (men 12.8, women 11.5) and 3.7/1000 player hours for lost-time injuries (men 3.5, women 4.1) [39]. Mechanisms of injury involved aerial challenges (55%) and the use of the upper extremity (33%) or head (30%). [39]
Morphological changes to the cervical spine
Ten studies identified degenerative changes such as cervical spinal stenosis, degenerative disk disease, temporary paralysis, spondylolisthesis, and neck pain 10–20 years prior to aged-matched controls among contact sport athletes [3, 8, 41,42,43,44,45,46,47]. Lastly, three studies reviewed the experimental biomechanical stresses placed on the cervical spine in response to mechanical head loads during contact sport participation [9, 48, 49]. In these studies, multidirectional instability in the upper cervical spine was observed following simulated head impacts.
Return to play considerations
Ten studies explained principles guiding returning to play which included: asymptomatic, pain-free, neurologically intact, full strength and full cervical range of motion [50,51,52,53,54,55,56,57,58,59]. The primary concerns included reticulating pain, damage to C1 or C2, and instability [59, 60]. However, observations of increased risk of musculoskeletal injury following a concussion, portend the importance of caring for surrounding structures [19, 27].
The two most frequent concerns for disqualification were spinal stenosis and brachial plexus injury. Brachial plexus injury has an estimated 87% reoccurrence rate and caution should be taken to return those athletes with reoccurring radicular pain [53].
Theme 2: Cervical afferents and postural control
A total of twelve studies demonstrated the role cervical afferents play in upright posture and control of locomotion [11, 20, 23, 61,62,63,64,65,66,67,68,69]. These articles describe the cervicocephalic network and the role it plays in proper maintenance of head position, postural tone and coordination of the extremities congruent with the 2nd purpose of this review. Cervical afferents such as mechanoreceptors and nociceptive nerve endings are prevalent in cervical facet capsular tissue [23]. High densities up to 200 muscle spindles per gram compared to the first lumbrical in the thumb which has a mere 16 muscle spindles per gram [67].
Artificially induced afferent cervical dysfunction alters neuromotor control and posture maintenance
Three studies demonstrated how vibration and/or using anesthetic injections to simulate cervical dysfunction could cause severe ataxia and disequilibrium [64, 67, 69]. Malmstrom et al. [64] demonstrated significant increases in error during walking task. Moreover, Wannaprom et al. [69] reported increased postural sway and slower gait speeds under a vibration condition. Allum et al. [20] compared healthy controls to individuals with labyrinthine deficiency to isolate the contributions of the vestibular and cervical afferents in head control revealing head velocities during balance corrections were highly dependent on the movements of the head-neck mass-viscoelastic system. The cervico-collic reflex was also found to modulate the amplitude of functionally stabilizing responses and dampen mechanically induced instability of the head and neck.
Cervical pathology is linked to altered neuromotor control and poor posture maintenance
In addition to experiments in healthy controls, alterations in postural maintenance and locomotion, as well as cervical afferent processing following cervical pathology have been observed [11, 61,62,63,64,65,66,67,68, 70]. Patients with neck pain and dizziness demonstrate decreased postural stability [11, 63], as well as decreases in cervical sensorimotor function [62]. Specifically, cervical joint position error was significantly correlated with greater levels of neck pain and extent of cervical degeneration [62]. These findings have been replicated several times [11, 62, 65]. Separately, changes in cervical joint position error have also been correlated with altered postural stability [71].
Theme 3: Damage to cervical afferents and increased risk of injury
In considering the 3rd aim of the present review 4 studies demonstrate preliminary evidence of a connection between head impacts and altered cervical sensorimotor function [13, 14, 16, 72]. Cheever et al. [14] reported amateur sport athletes with a history of contact sport exposure exhibit 25% more total neck reposition error than controls. A follow up study utilized an acute bout of instrumented head impacts and observed a 65% acute increase in cervical joint position error following soccer heading compared to a 6% decrease among controls who did not complete the heading [13]. A decrease in trunk and head positioning following head impacts has also been observed, suggesting altered balance strategies and trunk muscle activation as regulated by the cervicocephalic network may also manifest following RHI. [72]
Further exploring the 3rd aim two preliminary prospective studies explored the correlation between decreased cervical sensorimotor function and a corresponding increase in musculoskeletal injury risk [13, 19]. In a prospective cohort study performed by Hides et al. [19], five risk factors were identified (cervical joint position error, history of concussion, and 3 measures of trunk muscle function). Athletes with 3 or more risk factors were 14 times more likely to suffer a neck/head injury (sensitivity 75% and specificity 82%) than players with 2 or fewer risk factors. Significantly decreased sway velocity and increased size/contraction of trunk muscles were also correlated with head position sense [19]. A similar study by Cheever et al. [13] found that a combination of sign and symptom severity scores and neck reposition error had robust predictive capability of individual’s future musculoskeletal injury status (AUC = 0.80, p = 0.003).
Discussion
The objective of this scoping review was to present the available evidence of morphological changes to the cervical spine following contact sport participation and to describe a theorized increased risk of musculoskeletal injury due to alterations in cervical sensorimotor function resulting from those morphological changes. Morphological changes to the cervical spine were observed throughout the literature, and associated decreased cervical sensorimotor function were observed in a few instances [13, 14]. Furthermore, preliminary evidence of a correlation between cervical sensorimotor function and secondary musculoskeletal injury was observed. [13, 19]
Decreased cervical sensorimotor function following morphological changes to the cervical spine and exposure to RHI
A preponderance of studies have demonstrated a relationship contact sport athletes who have a history of scrumming, tackling, and/or head contact with a ball and early development of chronic degeneration of the cervical spine [3, 6, 9, 73]. Separately, acute bouts of soccer heading and a history of contact sport history have been correlated with decreased cervical sensorimotor function [13, 14, 16]. However, while observations of accelerated degeneration and acute damage to the cervical spine have been corroborated in different sports (e.g., soccer, rugby, American football), all studies employed a cross-sectional design, failing to demonstrate a longitudinal correlation [7, 44, 46].
Preliminary findings from a series of instrumented heading studies serve as a potential foundation of a direct link between exposure to RHI and decreased cervical sensorimotor function and posture [13, 74]. Cheever et al. demonstrated a 65% increase in cervical joint reposition error in response to controlled soccer headers [13]. Similarly, decreased balance following instrumented soccer headers has been observed [74]. Both cervical sensorimotor function and balance deficits have been identified independently in patients suffering from chronic cervical pathology and athletes following an acute bout of soccer headers [75,76,77].
Cervical sensorimotor dysfunction and increased musculoskeletal injury risk
Previous research studies have demonstrated correlations between decreases in cervical joint position and postural control deficits Independent of contact sport exposure [70,71,72,73,74,75,76,77,78,79]. Both patients suffering from persistent cervical symptoms and persistent post-concussive symptoms have demonstrated altered postural control, as well as decreased cervical sensorimotor function [61, 66, 68, 70].
A large body of existing literature demonstrates an observed increase in musculoskeletal injury risk in the year after sustaining a concussion [80]. The mechanism for this relationship remains highly contested [27]. However, one leading hypothesis points to observations of lingering neuromuscular control deficits [79]. While not fully explored, altered cervical afferent processing may play a role in this heightened risk. Sensorimotor control of both stable upright position and locomotion relies heavily on cervical afferent information that play a critical role in three reflexes that influence head, eye and postural stability: the cervico-collic reflex, the cervico-ocular reflex, and the tonic neck reflex [67]. These reflexes work alongside the vestibular and visual systems throughout the central nervous system to maintain proper postural control [80]. These connections have been further mapped in Fig. 4 to visually demonstrate the potential connection of morphological and neurological changes to the cervical spine and increased risk of secondary injury.

Mapping of potential implications for altered cervical afferent input
While findings of impaired sensorimotor function and balance in contact sport athletes are an important step, these movements were all performed at slow speeds, which don’t mirror the pace of sports-related task. Previous experiments exploring the integration of deficient cervical afferent information into the cerviocephalic network were performed in either a static position or walking at a relatively slow steady state (< 2–3 mph) [64, 69]. Athletes frequently travel in excess of 15–20 mph during sprints with individual spikes in limb movement exceeding 8000 degrees/s [81]. No research has been performed in a high velocity movement state to test how variations in postural control and cervical sensorimotor function may be magnified by the high velocity demands of contact sport movement patterns (e.g., dodging a potential tackler, sprinting after an advancing player, or adjusting to a rapid change of direction).
Knowledge gaps and future research
In line with the 4th aim of the present scoping review several gaps in the available literature were identified (Box 1). Future research should explore the dose dependent effect of RHI on structures of the cervical spine and the causative affect those changes have on musculoskeletal injury risk. Moreover, it would be important to explore potential interventional therapies to reduce the increased risk of injury.
Limitations
While scoping reviews are comprehensive, they fall short of exhaustively identifying all relevant literature by balancing the breadth and depth of the desired analysis. Our search was subject to a limited number of contact sports rather than all physical activity involving RHI. Contact sport athletes are different from controls for many reasons such as exercise history, exposure to other impacts to the head or body, making it difficult to have true controls matched across all demographical and extraneous factors. Scoping reviews are broad in nature and allow for the development of theoretically connections regardless of quality, which allows for a broader and more contextual overview than a systematic review but may be more subject to individual bias. Rigorous and reproducible methods were employed to demonstrate the authors commitment to publish all findings whether findings were positive, negative or not significant to the theoretical argument presented in the introduction.
Conclusions
While preliminary work exploring the role the cervicocepahlic network plays in control of both static posture and locomotion demonstrates clear connections between deficit cervical afferent input and erroneous motor output. Moreover, morphological changes to the cervical spine and associated sensorimotor deficits were observed throughout the literature in response to contact sport participation. However, while both deficit cervical afferent and erroneous motor output have been observed in response to contact sport participation little research has explored a potential causal relationship between those deficits and future musculoskeletal injury risk. Further research is necessary to elucidate the relationship between cervical pathology and alterations in cervical sensorimotor function in recreational and amateur athletes.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
References
Bailes JE. Management of cervical spine sports injuries. Athl Train. 1990;25(2):156–9.
Legault EP, Descarreaux M, Cantin V. Musculoskeletal symptoms in an adolescent athlete population: a comparative study. BMC Musculoskelet Disord. 2015;16(210):1–9.
Sortland O, Tysvaer AT, Storli OV. Changes in the cervical spine in association football players. Br J Sports Med. 1982;16(2):80–4.
Torg JS, Ramsey-Emrhein JA. Suggested management guidelines for participation in collision activities with congenital, developmental, or postinjury lesions involving the cervical spine. Med Sci Sports Exer. 1997;29(7 Suppl):S256-s272.
Panjabi MM, Cholewicki J, Nibu K, Grauer J, Babat LB, Dvorak J. Critical load of the human cervical spine: an in vitro experimental study. Clin Biomech. 1998;13(1):11–7.
Berge JRM, Marque B, Vital JM, Sénégas J, Caillã JM. Age-related changes in the cervical spines of front-line rugby players. Am J Sports Med. 1999;27(4):422–9.
Castinel BH, Adam P, Milburn PD, Castinel A, Quarrie KL, Peyrin JC, Yeo JD. Epidemiology of cervical spine abnormalities in asymptomatic adult professional rugby union players using static and dynamic MRI protocols: 2002 to 2006. Br J Sports Med. 2010;44(3):194–9.
Kartal A, ıldıran I, Şenköylü A, Korkusuz F. Soccer causes degenerative changes in the cervical spine. Euro Spine J. 2004;13(1):76–82.
Mehnert MJ, Agesen T, Malanga GA. “Heading” and neck injuries in soccer: a review of biomechanics and potential long-term effects. Pain Phys. 2005;8(4):391–7.
Service NH. Whiplash/symptoms of whiplash 2015. 2015. http://www.nhsinform.com/health-library/articles/w/whiplash/symptoms.
Treleaven J, Peterson G, Ludvigsson ML, Kammerlind AS, Peolsson A. Balance, dizziness and proprioception in patients with chronic whiplash associated disorders complaining of dizziness: a prospective randomized study comparing three exercise programs. Man Ther. 2016;22:122–30.
Cantu RC. Cervical spinal stenosis. Challenging an established detection method. Phys Sportsmed. 1993;21(9):57–58;62–63.
Cheever KM, Howard JT, Kawata K. Clinical changes in cervical neuromuscular control following subconcussive impacts. J Sport Rehabil. 2021;30(3):467–74.
Cheever K, Mcdevit J, Wright WG, Tierney R. Differences in cervical kinesthesia between amateur athletes with and without a history of contact sport participation. Brain Inj. 2021;35(4):404–10.
Lark SD, Mccarthy P. The effects of a rugby playing season on cervical range of motion. J Sports Sci. 2010;28(6):649–55.
Lark SD, Mccarthy PW. Cervical range of motion and proprioception in rugby players versus non-rugby players. J Sports Sci. 2007;25(8):887–94.
Cheever K. Exploring the relationship between musculoskeletal injury and clinical outcome measures of cervical sensorimotor function. Int J Athl Ther Train. 2021;26:262–8.
Collins CL, Fletcher EN, Fields SK, Kluchurosky L, Rohrkemper MK, Comstock RD, Cantu RC. Neck strength: a protective factor reducing risk for concussion in high school sports. J Prim Prevent. 2014;35(5):309–19.
Hides JA, Smith MMF, Mendis MD, Treleaven J, Rotstein AH, Sexton CT, Choy NL, Mccrory P. Self-reported concussion history and sensorimotor tests predict head/neck injuries. Med Sci Sports Exer. 2017;49(12):2385–93.
Allum JH, Gresty M, Keshner E, Shupert C. The control of head movements during human balance corrections. J Vestib Res Equil Orient. 1997;7(2–3):189.
Boyle R. Vestibulospinal control of reflex and voluntary head movement. Ann New York Acad Sci. 2001;942(1):364–80.
Kulkarni V, Chandy MJ, Babu KS. Quantitative study of muscle spindles in suboccipital muscles of human foetuses. Neurol India. 2001;49(4):355–9.
Mclain RF. Mechanoreceptor endings in human cervical facet joints. Spine. 1994;19(5):495–501.
Marshall CM, Vernon H, Leddy JJ, Baldwin BB. The role of the cervical spine in post-concussion syndrome. Phys Sports Med Phys Sportsmed. 2015;43(3):274–84.
Schneider KJ, Meeuwisse WH, Nettel-Aguirre A, Barlow K, Boyd L, Kang J, Emery CA. Cervicovestibular rehabilitation in sport-related concussion: a randomised controlled trial. Br J Sports Med. 2014;48(17):1294-U55.
Arskey HL, O’Malley K. Scoping studies, towards a methodological fraemwork. Int J Soc Res Methodol. 2005;5(8):19–32.
Howell DR, Lynall RC, Buckley TA, Herman DC. Neuromuscular control deficits and the risk of subsequent injury after a concussion: a scoping review. Sports Med. 2018;48(5):097–1115.
Murray AD, Daines L, Archibald D, Hawkes RA, Schiphorst C, Kelly P, Grant L, Mutrie N. The relationships between golf and health: a scoping review. Br J Sports Med. 2017;51(1):12.
Griffin SA, Perera NKP, Murray A, Hartley C, Brooks JHM, Kemp SPT, Stokes KA. The relationships between rugby union and health: a scoping review protocol. BMJ Open Sport Exer Med. 2019;5(1):11–7.
Caron JG, Bloom GA, Falcao WR, Sweet SN. An examination of concussion education programmes: a scoping review methodology. Inj Prev. 2015;21(5):301–8.
Cantu RC, Mueller FM. Catastrophic spine injuries in American football. 1977–2001. Neurosurgery. 2003;53(2):358–62.
Hutton MJ, Mcguire RA, Dunn R, Williams R, Robertson P, Twaddle B, Kiely P, Clarke A, Mazda K, Davies P, Pagarigan KT, Dettori JR. Catastrophic cervical spine injuries in contact sports. Global Spine J. 2016;6(7):721–33.
Mueller FO. Fatalities from head and cervical spine injuries occurring in tackle football: 50 years’ experience. Clin Sports Med. 1998;17(1):169–82.
Chung AS, Makovicka JL, Hassebrock JD, Patel KA, Tummala SV, Deckey DG, Hydrick TC, Rubel NC, Chhabra A. Epidemiology of cervical injuries in NCAA football players. Spine. 2019;44(12):848–54.
Lee KM, Kay MC, Kucera KL, Prentice WE, Kerr ZY. Epidemiology of cervical muscle strains in collegiate and high school football athletes, 2011–2012 through 2013–2014 academic years. J Athl Train. 2019;54(7):780–6.
Meron A, Mcmullen C, Laker SR, Currie D, Comstock RD. Epidemiology of cervical spine injuries in high school athletes over a ten-year period. PM & R. 2018;10(4):365–72.
Simmons MM, Swedler DI, Kerr ZY. Injury surveillance of head, neck, and facial injuries in collegiate ice hockey players, 2009–2010 through 2013–2014 academic years. J Athl Train. 2017;52(8):776–84.
Williams JZ, Singichetti B, Li HM, Xiang H, Klingele KE, Yang JZ. Epidemiological patterns of initial and subsequent injuries in collegiate football athletes. Am J Sports Med. 2017;45(5):1171–8.
Fuller CW, Junge A, Dvorak J. A six year prospective study of the incidence and causes of head and neck injuries in international football. Br J Sports Med. 2005;39:I3–9.
Nilsson M, Hagglund M, Ekstrand J, Walden M. Head and neck injuries in professional soccer. Clin J Sport Med. 2013;23(4):255–60.
Bailes JE. Experience with cervical stenosis and temporary paralysis in athletes. J Neurosurg-Spine. 2005;2(1):11–6.
Brauge D, Delpierre C, Adam P, Sol JC, Bernard P, Roux FE. Clinical and radiological cervical spine evaluation in retired professional rugby players. J Neurosurg-Spine. 2015;23(5):551–7.
Kuman K, Umeyama T. Cervical disk injuries in athletes. Arch Orthopaed Trauma Surg. 1986;105(4):223–6.
Ndubuisi CA, Ohaegbulam SC, Mezue WC. Impact of active leisure (noncompetitive) contact sports activities on the space available for the cord of the subaxial cervical spine of asymptomatic adults. World Neurosurg. 2017;108:705–10.
Quarrie KL, Cantu RC, Chalmers DJ. Rugby union injuries to the cervical spine and spinal cord. Sports Med. 2002;32(10):633–53.
Torg JS, Naranja RJ, Pavlov H, Galinat BJ, Warren R, Stine RA. The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players—an epidemiological study. J Bone Joint Surg-Am Volume. 1996;78A(9):1308–14.
Tysvaer AT. Head and neck injuries in soccer—impact of minor trauma. Sports Med. 1992;14(3):200–13.
Ivancic PC. Cervical spine instability following axial compression injury: a biomechanical study. Orthopaed Traumatol Surg Res. 2014;100(1):127–33.
Trewartha G, Preatoni E, England ME, Stokes KA. Injury and biomechanical perspectives on the rugby scrum: a review of the literature. Br J Sports Med. 2015;49(7):425-U25.
Cantu RC. Functional cervical spinal stenosis—a contraindication to participation in contact sports. Med Sci Sports Exer. 1993;25(3):316–7.
Cantu RC. The cervical spinal stenosis controversy. Clin Sports Med. 1998;17(1):121–6.
Chao S, Pacella MJ, Torg JS. The pathomechanics, pathophysiology and prevention of cervical spinal cord and brachial plexus injuries in athletics. Sports Med. 2010;40(1):59–75.
Dailey A, Harrop JS, France JC. High-energy contact sports and cervical spine neuropraxia injuries what are the criteria for return to participation? Spine. 2010;35(21):S193–201.
Joaquim AF, Hsu WK, Patel AA. Cervical spine surgery in professional athletes: a systematic review. Neurosurg Focus. 2016;40(4):143–8.
Kepler CK, Vaccaro AR. Injuries and abnormalities of the cervical spine and return to play criteria. Clinics Sports Med. 2012;31(3):499–508.
Mcana S, Cho S, Qureshi S, Hecht AC. A commentary on cervical spondylolysis in the contact athlete. Spine. 2014;14(6):E7–8.
Mcana S, Cho S, Qureshi S, Hecht AC. A commentary on cervical spondylolysis in the contact athlete. Spine. 2014;14(6):E7–8.
Okonkwo DO, Stone JR. Basic science of closed head injuries and spinal cord injuries. Clin Sports Med. 2003;22(3):467–81.
Torg JS. Cervical spine injuries and the return to football. Sports Health. 2009;1(5):376–83.
Torg JS, Ramsey-Emrhein JA. Cervical spine and brachial plexus injuries: return-to-play recommendations. Phys Sportsmed. 1997;25(7):60–62;64;66–67;72;81–82;85–88.
Carrick FR, Pagnacco G, Hunfalvay M, Azzolino S, Oggero E. Head position and posturography: a novel biomarker to identify concussion sufferers. Brain Sci. 2020;10(12):1003.
Freppel S, Bisdorff A, Colnat-Coulbois S, Ceyte H, Cian C, Gauchard G, Auque J, Perrin P. Visuo-proprioceptive interactions in degenerative cervical spine diseases requiring surgery. Neuroscience. 2013;25(5):226–32.
Karlberg M, Magnusson M, Malmstrom ME, Melander A, Moritz U. Postural and symptomatic improvement after physiotherapy in patients with dizziness of suspected cervical origin. Arch Phys Med Rehabil. 1996;77(9):874–82.
Malmstrom EM, Fransson PA, Bruinen TJ, Facic S, Tjernstrom F. Disturbed cervical proprioception affects perception of spatial orientation while in motion. Exp Brain Res. 2017;235(9):2755–66.
Reddy RS, Tedla JS, Dixit S, Abohashrh M. Cervical proprioception and its relationship with neck pain intensity in subjects with cervical spondylosis. BMC Musculoskelet Disord. 2019;20(1):1–7.
Sjostrom H, Allum JFJ, Carpenter MG, Adkin AL, Honegger F, Ettlin T. Trunk sway measures of postural stability during clinical balance tests in patients with chronic whiplash injury symptoms. Spine. 2003;28(15):1725–34.
Treleaven J. Sensorimotor disturbances in neck disorders affecting postural stability, head and eye movement control. Man Ther. 2008;13(1):2–11.
Treleaven J, Jull G, Lowchoy N. Standing balance in persistent whiplash: a comparison between subjects with and without dizziness. J Rehabil Med. 2005;37(4):224–9.
Wannaprom NJ, Treleaven J, Jull G, Uthaikhup S. Neck muscle vibration produces diverse responses in balance and gait speed between individuals with and without neck pain. Musculoskelet Sci Pract. 2018;35:25–9.
Treleaven J, Jull G, Lowchoy N. Lowchoy N The relationship of cervical joint position error to balance and eye movement disturbances in persistent whiplash. Man Ther. 2006;11(2):99–106.
Abdelkader NA, Mahmoud AY, Fayaz NA, Mahmoud LS. Decreased neck proprioception and posturalstability after induced cervical flexor muscles fatigue. J Musculoskelet Neur Interact. 2020;20(3):421–8.
Hides JA, Smith MMF, Mendis MD, Smith NA, Cooper AJ, Treleaven J, Leung F, Gardner AJ, Mccrory P, Choy NL. A prospective investigation of changes in the sensorimotor system following sports concussion. An exploratory study. Musculoskelet Sci Pract. 2017;29:7–19.
Svaldi DO, Joshi C, Mccuen EC, Music JP, Hannemann R, Leverenz LJ, Nauman EA, Talavage TM. Accumulation of high magnitude acceleration events predicts cerebrovascular reactivity changes in female high school soccer athletes. Brain Imag Behavior. 2020;14(1):164–74.
Haran FJ, Tierney R, Wright WG, Keshner E, Silter M. Acute changes in postural control after soccer heading. Int J Sports Med. 2013;34(4):350–4.
Hwang S, Ma L, Kawata K, Tierney R, Jeka JJ. Vestibular dysfunction after subconcussive head impact. J Neurotrauma. 2017;34(1):8–15.
Mcpartland JM, Brodeur RR, Hallgren RC. Chronic neck pain, standing balance, and suboccipital muscle atrophy—a pilot study. J Manipul Physiol Therapeut. 1997;20(1):24–9.
Rix GD, Bagust J. Cervicocephalic kinesthetic sensibility in patients with chronic, nontraumatic cervical spine pain. Arch Phys Med Rehabil. 2001;82(7):911–9.
Kristjansson K, Treleaven EJ. Sensorimotor function and dizziness in neck pain: implications for assessment and management. J Orthop Sports Phys Ther. 2009;39(5):364–77.
Alsalaheen BA, Mucha A, Morris LO, Whitney SL, Furman JL, Camiolo-Reddy CE, Collins MW, Lovell PJ, Sparto M. Vestibular rehabilitation for dizziness and balance disorders after concussion. J Neurol Phys Ther. 2010;34(2):87–93.
Sjolander P, Michaelson P, Jaric S, Djupsjobacka M. Sensorimotor disturbances in chronic neck pain–range of motion, peak velocity, smoothness of movement, and repositioning acuity. Man Ther. 2008;13(2):122–31.
Bourdon PC, Cardinale M, Murray A, Gastin P, Kellmann M, Varley MC, Gabbett TJ, Coutts AJ, Burgess DJ, Gregson W, Cable NT. Monitoring athlete training loads: consensus statement. Int J Sports Physiol Perform. 2017;12(1):161–70.
Acknowledgements
We would like to acknowledge Leslie Rosas, Clarissa Garcia, and Ivanna Peralta who all work as undergraduate research assistants for Dr. Cheever and May Hayward who is a research librarian who all provided valuable assistance in helping to identify and categorize the articles for this scoping review.
Funding
The authors report no funding associated with the scoping review.
Author information
Authors and Affiliations
Contributions
KC was primarily responsible for the conception and framework of the scoping review. Additionally, Dr. KC lead the scoping review process. JK assisted in the development and critically reviewed the manuscript while adding much needed content expertise as skilled clinician in the diagnosis and treatment of cervical spine pathology. KK assisted in the process of the scoping review while also providing meaningful structure development and writing expertise. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors report no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Search strategy.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cheever, K., King, J. & Kawata, K. The association between contact sport exposure and cervical sensorimotor dysfunction: a scoping review of implications for future musculoskeletal injury risk. Chiropr Man Therap 30, 50 (2022). https://doi.org/10.1186/s12998-022-00458-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12998-022-00458-w