
Abstract
Background
Studies suggest a correlation between excessive sedentary behavior, insufficient physical activity, and an elevated likelihood of experiencing psychiatric disorder. Nonetheless, the precise influence of sedentary behavior and physical activity on psychiatric disorder remains uncertain. Hence, the objective of this research was to investigate the possible causal relationship between sedentary behavior, physical activity, and the susceptibility to psychiatric disorder (depression, schizophrenia and bipolar disorder), utilizing a two-sample Mendelian randomization (MR) approach.
Methods
Potential genetic instruments related to sedentary leisure behaviors were identified from the UK Biobank database, specifically a summary-level genome-wide association study (GWAS) involving 422,218 individuals of European descent. The UK Biobank database also provided the GWAS data for physical activity. Primary analysis was performed using inverse variance weighting (IVW) to assess the causal relationship between sedentary behavior, physical activity, and the risk of psychiatric disorder (depression, schizophrenia and bipolar disorder). Sensitivity analysis was conducted using Cochran’s Q test, the MR–Egger intercept test, the MR-pleiotropy RESidual sum and outlier test, leave-one-out analysis, and funnel plot analysis.
Results
According to the IVW analysis, there was a significant association between genetically predicted leisure television watching and an increased risk of depression (odds ratio [OR] = 1.027, 95% confidence interval [CI]: 1.001–1.053; P = 0.04). The IVW analysis also indicated that there was a decreased risk of depression associated with fraction accelerations of > 425 milligravities, as measured by accelerometers (OR = 0.951, 95%CI: 0.914–0.989; P = 0.013). The other MR methods obtained consistent but non-significant results in the same direction. However, there was no evidence of a causal association between genetic liability for moderate-to-vigorous physical activity, accelerometer-assessed physical activity, computer use, or driving and the risk of depression. Furthermore, IVW analysis has also found that driving has a slight effect in reducing the risk of schizophrenia (OR = 0.092, 95%CI: 0.010–0.827; P = 0.033), while leisure television viewing has a significant protective effect against the onset of bipolar disorder (OR = 0.719, 95%CI: 0.567–0.912; P = 0.006).
Conclusion
The study provides compelling evidence of a link between depression, bipolar disorder, and excessive TV watching. Furthermore, it suggests that higher accelerometer-assessed fraction accelerations of > 425 milligravities can serve as a genetic protective factor against depression. To mitigate the risk of developing depression, it is advisable to reduce sedentary activities, particularly television watching, and prioritize engaging in vigorous physical exercise.
Similar content being viewed by others
Background
Psychiatric disorders are widespread mental health problems that affect a significant proportion of the global population. It is estimated that these disorders impact approximately 22.1% of the world’s population [1]. The origins of psychiatric disorders are complex, involving a combination of genetic, environmental, and neurobiological factors.
Recent research has also explored the role of leisure sedentary behavior and physical activity in the development of psychiatric disorders. Evidence indicates that excessive leisure sedentary behavior is associated with an increased risk of developing depression [2]. In fact, leisure sedentary behavior can lead to physiological changes, decreased exposure to natural light, and reduced social interaction, all of which may contribute to the severity and development of depressive symptoms [3]. Observational studies have also found a link between sedentary behavior and schizophrenia and bipolar disorder [4, 5]. Regular physical activity has been proven to have positive effects on mental health, including the alleviation of depressive symptoms [6]. Exercise boosts the levels of endorphins, serotonin, and other neurochemicals linked to improved mood and overall well-being [7, 8]. Nevertheless, there is still a lack of direct evidence regarding the causal influence of leisure sedentary behavior and physical activity on psychiatric disorders.
Mendelian randomization (MR) analysis is a powerful tool for examining the causal connections between risk factors and diseases. By using genetic variations as the instrumental variables (IVs), MR provides more reliable evidence of causality compared with traditional observational studies [9]. A notable advantage of MR is its ability to overcome the common limitations encountered in observational studies, such as confounding and reverse causality. By utilizing genetically determined variations at conception, MR can provide stronger evidence of causality since these variations are less influenced by external factors that may be linked to both the risk factors and the disease outcomes. The impact of MR in investigating causality has been extensively explored across a range of diseases, including prostate cancer [10], inflammatory bowel disease [11], cardiovascular diseases [12], and gastrointestinal diseases [13], as well as their association with depression. Nonetheless, the connection between psychiatric disorder and leisure sedentary behavior and physical activity has not been thoroughly explored. Consequently, a comprehensive analysis was undertaken using a two-sample MR approach and incorporated data from genome-wide association studies (GWAS) to delve deeper into the causal associations between leisure sedentary behavior, physical activity, and psychiatric disorders (depression, schizophrenia and bipolar disorder).
Materials and methods
Study design
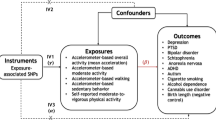
A MR study was carried out utilizing two samples to assess the causal relationship between leisure sedentary behavior, physical activity, and psychiatric disorders (depression, schizophrenia and bipolar disorder) (as depicted in Fig. 1). Psychiatric disorders mainly include depression, schizophrenia and bipolar disorder. To accomplish this, the MR method relied on three critical assumptions: [1] the genetic instrumental variables employed in the analysis exhibited a robust association with sedentary behavior and physical activity; [2] the genetic instrumental variables remained unaffected by any confounding variables; and [3] the genetic instrumental variables were solely connected to the outcomes through sedentary behavior and physical activity, without any involvement of other causal pathways [14]. The data primarily originated from independent GWAS data sources.

Study design and workflow. Note: Outcomes including depression, schizophrenia, and bipolar disorder
Data sources and instrumental variables selection
Exposures in genome-wide association studies: leisure sedentary behaviors and physical activity
The genetic instruments considered for leisure sedentary behavior were determined by analyzing data from the most recent summary-level GWAS. This research involved 422,218 individuals of European descent who were part of the UK Biobank [15]. Within this GWAS, three main categories of sedentary behaviors linked to participation in leisure activities were considered: watching TV, using a computer, and driving. The participants were asked to provide information regarding their daily time allocation to different activities through responding to the following inquiries: “What is the typical duration of time you spend per day watching television?” “How many hours do you usually use a computer within a day? (excluding computer use at work)”, and “On average, how much time do you spend driving in a day?”. According to the gathered responses, the participants dedicated a daily average of 2.8 h to watching television, with a standard deviation (SD) of 1.5 h. Similarly, computer usage accounted for approximately 1.0 h per day, with a SD of 1.2 h, while driving averaged 0.9 h per day, with a SD of 1.0 h. Considering multiple variables, including age, gender, smoking habits, hypertension, diabetes, body mass index (BMI), Townsend deprivation index, levels of physical activity, weekly alcohol intake, and educational background, the study identified a total of 209 single nucleotide polymorphisms (SNPs) associated with watching television, 35 SNPs associated with computer usage, and four SNPs associated with driving (P < 1 × 10–8) [15].
To ensure the quality of the SNP data for the MR analysis, rigorous filtering procedures were implemented. Initially, we combined SNPs that were in linkage disequilibrium within a 10-mb range, with an R2 value of > 0.001. To evaluate the effectiveness of the genetic instruments, SNPs with an F statistic of < 10 were excluded in the subsequent analysis. Additionally, SNPs were associated with the corresponding exposure using a genome-wide significance threshold of P < 5 × 10− 8. To eliminate any ambiguity, palindromic SNPs were also removed through harmonizing processes. Furthermore, any potential pleiotropy was addressed by employing the MR-pleiotropy RESidual sum and outlier method to remove any SNPs before MR analysis was re-performed to ensure robustness. Ultimately, 78 SNPs were employed as IVs for television viewing, 15 SNPs for computer usage, and one SNP for driving. For more comprehensive details regarding the SNPs utilized as IVs, refer to Additional file 1: Tables S1–S3.
The GWAS data for physical activity were provided by the UK Biobank [16, 17]. Adjustments in the data included age, sex, the first 10 genomic principal components from the genotyping chip, the center, the season (month) of the center visit, and the use of an accelerometer. Physical activity was measured using three different measures: self-reported levels of moderate-to-vigorous physical activity (MVPA), objectively measured physical activity using accelerometers, and accelerometer-based percentage accelerations exceeding 425 milligravities. Comprehensive details of these physical activity measures can be found in the original study [16]. To identify IVs for physical activity, the following criteria were applied [18]: [1] SNPs with genome-wide significance (P < 5 × 10–8); [2] SNP clustering using the PLINK algorithm (r2 threshold = 0.001 and window size = 10 MB); and [3] exclusion of SNPs that may have pleiotropic effects. Consequently, the investigation employed 14 SNPs for MVPA, seven SNPs for accelerometer-measured physical activity, and seven SNPs for accelerations exceeding 425 milligravities as the IVs (Additional file 1: Tables S4–S6).
Outcomes in genome-wide association studies
Summary statistics were obtained from publicly available large-scale GWAS on depression [19]. Depression was based on self-reported help-seeking behaviour for mental health difficulties from either a general practitioner or psychiatrist. To ensure the exclusion of individuals potentially impacted by conditions such as schizophrenia, a thorough screening procedure was implemented. This procedure involved the utilization of self-reported information, responses generated by the touchscreen, or ICD codes obtained from medical facility admission records. In addition, information was obtained from individuals who disclosed the usage of antipsychotic medication during a spoken interview. Conversely, control participants were excluded if they reported taking antidepressant medication, had a documented diagnosis of a mood disorder with depressive symptoms in their medical facility admission records, or self-reported experiencing depressive feelings. This study was carried out with the explicit endorsement of the NHS National Research Ethics Service, and all participants voluntarily provided informed written consent. To ascertain statistical significance, the threshold was established at P < 5 × 10− 8, adhering to the customary convention [19].
GWAS data for schizophrenia [20] and bipolar disorder [21] were obtained from the Psychiatric Genomics Consortium.
Statistical analysis
Mendelian randomization analysis
In this two-sample MR study, the inverse-variance weighted (IVW) method was used as the primary analytical method to assess the causality between leisure sedentary behavior, physical activity, and depression. The IVW method involves the use of the Wald ratio method to calculate the exposure outcome effect for each SNP and weighted linear regression with a forced intercept equal to zero. If the IVs satisfy three fundamental assumptions, this method offers more precise estimation and testing capabilities. Various sensitivity analyses were conducted to tackle issues related to unknown and unmeasured confounding factors, including MR-Egger regression [22], weighted median estimator (WME) analysis [23], and simple mode [24], weighted mode, and outlier methods. Among these methods, WME provides consistent causal relationship estimates, even if up to 50% of genetic variation is invalid. Unlike other techniques, WME considers both potential linkage imbalances and sampling errors among SNPs when estimating the impact of IVs on exposure [24].
Sensitivity analyses
The F statistic technique was utilized to gauge the potency of the IVs for the selected SNPs in this study. A threshold F-value of > 10, which is commonly recommended in MR analytical studies, was used. The strength of each genetic tool was estimated using the F statistic: F = R2(N − 2)/(1 − R2), where R2 is equal to the proportion of the variance explained by the genetic instrument and N is the effective sample size of the SNP-micronutrient associated GWAS [25]. As an additional measure, Cochran’s Q test was employed to examine the heterogeneity among the SNPs, which was derived from IVW evaluations. Sensitivity analysis was performed using leave-one-out (LOO) analysis by removing one SNP to ensure that no single SNP had an escalating impact on the analysis. This was combined with IVW to assess the total impact of the remaining SNPS. The analysis was conducted using R software (version 4.3.0) and R software package two-sample MR. The results are presented as the mean effect of a 1-SD-increase in BMI, along with the corresponding 95% confidence interval (CI). A two-sided P-value of < 0.05 was regarded as statistically significant.
Risk factors
To explore the genetic associations between leisure sedentary behavior and physical activity in relation to depression, an investigation was conducted on various potential mediators. These mediators encompassed factors such as BMI, lipid levels (triglycerides and total cholesterol), type 2 diabetes (T2D), and fasting insulin levels. The genetic basis for BMI was determined using data from the UK Biobank, which included a cohort of 461,460 individuals of European ancestry. The dataset utilized for this analysis is publicly accessible through the MRC IEU OpenGWAS database and MR-Base project, with the GWAS-ID, ukb-b-19,953. To process this dataset, PHESANT-derived variables from the UK Biobank were employed.
Varied GWAS data from the UK Biobank [26] was employed to analyze the lipid profile. Information on genetic factors related to T2D was obtained from the Diabetes Genetics Replication and Meta-analysis (DIAGRAM) consortium [27]. Additionally, the Meta-Analyses of Glucose and Insulin-related traits Consortium (MAGIC) provided the GWAS data on fasting insulin [28]. Refer to Table 1 for comprehensive details on each data source.
In this investigation, leisure sedentary behavior and physical activity were regarded as the exposures, while the aforementioned potential risk factors were employed as outcomes for the purpose of conducting MR. The primary findings were evaluated utilizing IVW estimates, with the significance level established at P ≤ 0.05.
Results
Mendelian randomization estimates
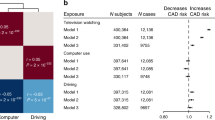
The IVW analysis revealed a significant link between the anticipated genetic influence on leisure television viewing and an increased likelihood of experiencing depression (OR = 1.027, 95%CI: 1.001–1.053; P = 0.04) (Fig. 2a). Conversely, when evaluating the accelerometer data, it was observed that higher fraction accelerations exceeding 425 milligravities were associated with a reduced risk of depression (OR = 0.951, 95%CI: 0.914–0.989; P = 0.013) (Fig. 2b). However, no evidence of causation was found between genetic predisposition for MVPA, accelerometer-measured physical activity, computer utilization, or driving and the risk of depression (Fig. 2). Furthermore, while the results obtained through the other MR methods consistently aligned with the above findings, they failed to achieve statistical significance (Additional file 1: Table S7 and Fig. 2).

Causal effects of leisure sedentary behaviors and physical activity on depression. (a, b) Summary of the Mendelian randomization (MR) estimates derived from the inverse-variance weighted (IVW), weighted median (WM), and MR-Egger methods. MVPA: self-reported moderate-to-vigorous physical activity
Furthermore, IVW analysis has also found that driving has a slight effect in reducing the risk of schizophrenia (OR = 0.092, 95%CI: 0.010–0.827; P = 0.033), while leisure television viewing has a significant protective effect against the onset of bipolar disorder (OR = 0.719, 95%CI: 0.567–0.912; P = 0.006). On the other hand, there is no apparent association between physical activity, computer use, and the onset of schizophrenia or bipolar disorder (Additional file 1: Table S8 and Table S9).
Sensitivity analyses
To assess the robustness and reliability of the above findings, a variety of sensitivity analyses were conducted. These analyses included the use of different statistical tests, including Cochran’s Q test, the MR-Egger intercept test, and the MR-PRESSO global test (Table 2). The results of the MR-Egger intercept tests indicated that there was no evidence of horizontal pleiotropy, as all P values were > 0.05. However, when examining the Q test analysis for the relationship between television watching and depression (Q = 161.853, P = 5.53 × 10− 8), some heterogeneity was observed. It is important to note that this heterogeneity did not affect the validity of the MR estimates, as the random-effects IVW method used in this study helps to account for pooled heterogeneity. Furthermore, the absence of pleiotropy was confirmed by the Egger intercepts, which indicated that the MR estimates were not influenced by pleiotropic bias, even in the presence of heterogeneity (Figs. 3a and c and 4a and c). In the remaining analyses, no heterogeneity was observed. Moreover, the LOO analysis indicated that none of the SNPs had a significant impact on the results, while the funnel plots displayed a symmetrical distribution (Figs. 3b and d and 4b and d), suggesting that the estimates were not compromised (Additional file 2: Figures S1-S4).

Scatter plots and funnel plots depicting the relationship between genetically predicted television watching and depression, and the relationship between genetically predicted accelerometer fraction accelerations of > 425 milligravities and depression. (a, b) Genetically predicted impact of television watching on depression; (c, d) genetically predicted impact of accelerometer fraction accelerations of > 425 milligravities on depression

Scatter plots and funnel plots depicting the relationship between genetically predicted driving and schizophrenia, and the relationship between genetically predicted television watching and bipolar disorder. (a, b) Genetically predicted impact of driving on schizophrenia; (c, d) genetically predicted impact of television watching on bipolar disorder
Risk factor analysis
To examine the possible factors connecting an increased risk of depression with television watching, MR methods were utilized to analyze the attendant impact on various common risk factors associated with depression. As shown in Table 3, the results demonstrate the following findings. In the case of leisure sedentary behavior, a significant association was observed between a 1-SD-h increase (2.8 h) in television watching and a 0.479 higher BMI, a 99% increased risk of T2D, and a 0.168-pmol/L rise in fasting insulin levels.
Regarding accelerometer-assessed fraction accelerations of > 425 milligravities, a significant association was found between a 1-SD-increase in such accelerations and a 0.22-lower BMI, a 0.154-mmol/L decrease in serum triglycerides, and a 50% reduced risk of T2D.
To summarize, the research findings indicate that metabolic disorders potentially contribute to the vulnerability to depression associated with leisure sedentary behavior, as evidenced by the risk factor analyses conducted.
Discussion
This study utilized public psychiatric disorder GWAS data on a large scale to investigate the potential causal connection between depression, schizophrenia, bipolar disorder and leisure sedentary behavior/physical activity. Various MR methods were employed to analyze this relationship. The findings indicate that physical activity, as measured by accelerometer-assessed fraction accelerations of > 425 milligravities, can lower the likelihood of depression, while casual TV watching can increase the risk. Considering the substantial prevalence and detrimental consequences of depression, it is imperative to explore strategies for improving lifestyles in view of preventing this condition.
With the development of the social economy, people’s lifestyles have changed a great deal, with many including a reduction in sports time and an increase in leisure sedentary behavior time. These unhealthy lifestyles seriously affect people’s physical health, as well as their spiritual world. It is crucial to acknowledge that a persistent lack of physical activity and increased sedentary behavior are frequently linked to adverse physical and mental health outcomes, along with an elevated susceptibility to various chronic diseases, such as obesity, T2D, cardiovascular disease, and cancer [29,30,31,32]. Importantly, studies have indicated that detrimental lifestyle choices, insufficient physical activity, and obesity are associated with an elevated likelihood of developing depression [33,34,35]. Notwithstanding the findings from limited observational studies, there is currently insufficient direct evidence to establish a causal relationship between sedentary behavior and depression. In contrast to unrealistic large-scale prospective clinical trials, due to the need for long-term observation, MR studies have revealed the fact that leisure sedentary behavior/physical activity is associated with responding to depression in a time- and cost-effective manner.
The present study further confirms that, from a causal perspective, the risk of depression is increased by sedentary behavior. Several factors can be attributed to the possible causes of depression resulting from this type of behavior. Sedentary behavior often involves prolonged periods of sitting or lying down, which leads to reduced physical activity. Studies have shown that regular exercise and physical activity can improve mental health and decrease the risk of depression [36, 37]. Decreased social interaction and increased isolation can be associated with sedentary behavior. Devoting an excessive amount of time to sedentary activities, such as watching television or engaging in video game activities, can potentially restrict the opportunities for social interaction, thereby contributing to emotions of loneliness and isolation [38, 39]. Sedentary behavior, especially late-night use of electronic devices, can also disrupt sleep patterns, with insufficient or poor-quality sleep closely linked to an increased risk of depression [40]. Such activities can negatively affect sleep by disrupting the circadian rhythm, leading to mood disturbances and depressive symptoms [40]. Additionally, many sedentary activities are indoor-based, resulting in limited exposure to natural light. Sunlight exposure has a positive impact on mental health and is associated with the production of serotonin, a neurotransmitter that regulates mood. Reduced access to natural light due to sedentary behavior may contribute to the development or worsening of depression [41, 42]. The present study also found that there was a decrease in the risk of depression when fraction accelerations of > 425 milligravities were assessed using an accelerometer. A previous study found that accelerometer-based activity reduces the risk of major depressive disorder [43]. Growing evidence suggests that lifestyle behaviors influence disease development by altering epigenetic processes [44, 45]. It has been found that 6 months of exercise intervention can change the methylation of DNA associated with obesity and diabetes [46]. Therefore, exercise may also reduce the risk of depression through epigenetic effects, and the specific mechanism needs to be further studied. Therefore, reducing sedentary behavior, especially the time spent watching TV, while increasing physical activity (fraction accelerations of > 425 milligravities) is crucial to the prevention and treatment of depression.
Furthermore, our comprehensive analyses revealed numerous potential reasons for this causal link between depression and watching television. Initially, various indicators related to obesity were identified, such as BMI, triglycerides, fasting insulin, and T2D, which could potentially function as mediators linking television viewing and the occurrence of depression. Substantial evidence suggests that chronic low-grade inflammation in the body is correlated with metabolic disorders such as obesity and diabetes. Inflammation has the capability to impact the brain and neurotransmitter levels, potentially contributing to the development of depression. The overproduction of pro-inflammatory cytokines, such as tumor necrosis factor-alpha and interleukin-6, has been observed in cases of depression [47, 48]. Additionally, metabolic diseases have the potential to disrupt the hypothalamic-pituitary-adrenal (HPA) axis, resulting in the dysregulation of stress response and cortisol production. The chronic activation of the HPA axis and abnormal cortisol levels have been linked to depression [49]. When compared with computer usage and driving, watching television is a form of leisure entertainment that is more immersive and less reflective, with a limited scope for communication. Consistently, prolonged television viewing has been associated with poor physical and mental health, which could also partly contribute to depression. It should be emphasized that additional research is imperative for establishing the exact degree to which sedentary behavior mediation is implicated in depression. Without specific mediation analysis, it is not possible to determine the direct impact of television watching on depression.
In addition, our study also found that driving has a slight effect in reducing the risk of schizophrenia, while leisure television viewing has a significant protective effect against the onset of bipolar disorder. This is an interesting finding, although observational studies have not yet reported this phenomenon. This also suggests that the effects of watching TV on different psychiatric disorders are different, and different situations need to be treated differently. On the other hand, there is no apparent association between physical activity, computer use, and the onset of schizophrenia or bipolar disorder.
The two-sample MR analysis method has several merits. First, in contrast to conventional observational studies, employing MR methods permits the estimation of effects with greater reliability and minimizes the potential for confounding and reverse causation. Second, the inclusion of individuals with European ancestry in the data analysis greatly reduces the potential impact of population stratification. Finally, the implementation of rigorous procedures effectively curtails the deviation attributable to instrumental variables.
Nevertheless, this study has certain limitations. First, there is insufficient personal information in the stratified secondary data to analyze gender and age. Second, the MR analysis postulates a linear correlation between exposure and outcome effects. However, such an assumption impedes the assessment of the non-linear correlation between depression risk and sedentary behavior and physical activity. Third, since the study was limited to individuals of European descent, the generalizability of the present findings to other ethnic populations is unfeasible. Fourth, subgroup analysis of different depression types was not feasible due to a lack of relevant information.
In summary, the present study involving two-sample MR presents compelling findings supporting the genetic underpinnings of the association between heightened sedentary behavior, reduced physical activity, and depression. As a result, these novel findings underscore the importance of reducing television watching time and increasing physical activity as preventive measures for depression. In addition, our study also found that leisure television viewing has a significant protective effect against the onset of bipolar disorder. This suggests that the effects of watching TV on different psychiatric disorders are different, and different situations need to be treated differently.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Charlson F, van Ommeren M, Flaxman A, Cornett J, Whiteford H, Saxena S. New WHO prevalence estimates of mental disorders in conflict settings: a systematic review and meta-analysis. Lancet. 2019;394(10194):240–8. https://doi.org/10.1016/S0140-6736(19)30934-1
Davy Vancampfort M, Hallgren F, Schuch B, Stubbs L, Smith S, Rosenbaum, et al. Sedentary behavior and depression among community-dwelling adults aged ≥ 50 years: results from the Irish longitudinal study on ageing. J Affect Disord. 2020;262:389–96. https://doi.org/10.1016/j.jad.2019.11.066
Megan Teychenne K, Ball J, Salmon. Sedentary behavior and depression among adults: a review. Int J Behav Med. 2010;17(4):246–54. https://doi.org/10.1007/s12529-010-9075-z
Davy Vancampfort J, Firth FB, Schuch S, Rosenbaum J, Mugisha M, Hallgren, et al. Sedentary behavior and physical activity levels in people with schizophrenia, bipolar disorder and major depressive disorder: a global systematic review and meta-analysis. World Psychiatry. 2017;16(3):308–15. https://doi.org/10.1002/wps.20458
Kevin Dang P, Ritvo J, Katz D, Gratzer Y, Knyahnytska A, Ortiz, et al. The role of daily steps in the treatment of major depressive disorder: secondary analysis of a randomized controlled trial of a 6-month internet-based, mindfulness-based cognitive behavioral therapy intervention for youth. Interact J Med Res. 2023;8:12e46419. https://doi.org/10.2196/46419
Schuch FB, Vasconcelos-Moreno MP, Borowsky C, Zimmermann AB, Rocha NS, Fleck MP. Exercise and severe major depression: effect on symptom severity and quality of life at discharge in an inpatient cohort. J Psychiatr Res. 2015;61:25–32. https://doi.org/10.1016/j.jpsychires.2014.11.005
Loretta Garvey AC, Benson D, Benger T, Short H, Banyard K-L, Edward. The perceptions of mental health clinicians integrating exercise as an adjunct to routine treatment of depression and anxiety. Int J Ment Health Nurs. 2023;32(2):502–12. https://doi.org/10.1111/inm.13089
Peter J, Carek SE, Laibstain SM, Carek. Exercise for the treatment of depression and anxiety. Int J Psychiatry Med. 2011;41(1):15–28. https://doi.org/10.2190/PM.41.1.c
Widding-Havneraas T, Zachrisson HD. A gentle introduction to instrumental variables. J Clin Epidemiol. 2022;149:203–5. https://doi.org/10.1016/j.jclinepi.2022.06.022
Chen X, Kong J, Diao X, Cai J, Zheng J, Xie W, et al. Depression and prostate cancer risk: a Mendelian randomization study. Cancer Med. 2020;9(23):9160–7. https://doi.org/10.1002/cam4.3493
Luo J, Xu Z, Noordam R, van Heemst D, Li-Gao R. Depression and inflammatory bowel disease: a bidirectional two-sample Mendelian randomization study. J Crohns Colitis. 2022;16(4):633–42. https://doi.org/10.1093/ecco-jcc/jjab191
Li GH, Cheung CL, Chung AK, Cheung BM, Wong IC, Fok MLY, et al. Evaluation of bi-directional causal association between depression and cardiovascular diseases: a Mendelian randomization study. Psychol Med. 2022;52(9):1765–76. https://doi.org/10.1017/S0033291720003566
Ruan X, Chen J, Sun Y, Zhang Y, Zhao J, Wang X, et al. Depression and 24 gastrointestinal diseases: a Mendelian randomization study. Transl Psychiatry. 2023;13(1):146. https://doi.org/10.1038/s41398-023-02459-6
Sekula P, Del GMF, Pattaro C, Köttgen A. Mendelian randomization as an approach to assess causality using observational data. J Am Soc Nephrol. 2016;27(11):3253–65. https://doi.org/10.1681/ASN.2016010098
Yordi J, van de Vegte MA, Said M, Rienstra, Pim van der Harst Niek Verweij. Genome-wide association studies and Mendelian randomization analyses for leisure sedentary behaviours. Nat Commun. 2020;11(1):1770. https://doi.org/10.1038/s41467-020-15553-w
Aiden Doherty K, Smith-Byrne T, Ferreira MV, Holmes C, Holmes, et al. GWAS identifes 14 loci for device-measured physical activity and sleep duration. Nat Commun. 2018;9(1):5257. https://doi.org/10.1038/s41467-018-07743-4
Yann C, Klimentidis DA, Raichlen J, Bea DO, Garcia NE, Wineinger LJ, Mandarino, et al. Genome-wide association study of habitual physical activity in over 377,000 UK Biobank participants identifes multiple variants including CADM2 and APOE. Int J Obes (Lond). 2018;42(6):1161–76. https://doi.org/10.1038/s41366-018-0120-3
Bahls M, Leitzmann MF, Karch André, Teumer A, Dörr M, Stephan B, Felix, et al. Physical activity, sedentary behavior and risk of coronary artery disease, myocardial infarction and ischemic stroke: a two-sample Mendelian randomization study. Clin Res Cardiol. 2021;110(10):1564–73. https://doi.org/10.1007/s00392-021-01846-7
Howard DM, Adams MJ, Shirali M, Clarke TK, Marioni RE, Davies G, et al. Genome-wide association study of depression phenotypes in UK Biobank identifies variants in excitatory synaptic pathways. Nat Commun. 2018;9(1):1470. https://doi.org/10.1038/s41467-018-03819-3
Vassily Trubetskoy, Antonio F, Pardiñas T, Qi G, Panagiotaropoulou S, Awasthi, Tim B, Bigdeli, et al. Mapping genomic loci implicates genes and synaptic biology in schizophrenia. Nature. 2022;604(7906):502–8. https://doi.org/10.1038/s41586-022-04434-5
Niamh Mullins AJ, Forstner, Kevin S, O’Connell B, Coombes, Jonathan RI, Coleman Z, Qiao, et al. Genome-wide association study of more than 40,000 bipolar disorder cases provides new insights into the underlying biology. Nat Genet. 2021;53(6):817–29. https://doi.org/10.1038/s41588-021-00857-4
Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44(2):512–25. https://doi.org/10.1093/ije/dyv080
Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. 2016;40(4):304–14. https://doi.org/10.1002/gepi.21965
Zhu Z, Zheng Z, Zhang F, Wu Y, Trzaskowski M, Maier R, et al. Causal associations between risk factors and common diseases inferred from GWAS summary data. Nat Commun. 2018;9(1):224. https://doi.org/10.1038/s41467-017-02317-2
Mandrekar J, Petitti DB. Overlooked shortcomings of observational studies of interventions in coronavirus disease 2019: an illustrated review for the clinician. Open Forum Infect Dis. 2021;8(8):ofab317. https://doi.org/10.1093/ofid/ofab317
Tom G, Richardson E, Sanderson, Tom M, Palmer M, Ala-Korpela, Brian A, Ference GD, Smith, et al. Evaluating the relationship between circulating lipoprotein lipids and apolipoproteins with risk of coronary heart disease: a multivariable Mendelian randomisation analysis. PLoS Med. 2020;17(3):e1003062. https://doi.org/10.1371/journal.pmed.1003062
Morris AP, Voight BF, Teslovich TM, Ferreira T, Segrè AV, Steinthorsdottir V, et al. Large-scale association analysis provides insights into the genetic architecture and pathophysiology of type 2 diabetes. Nat Genet. 2012;44(9):981–90. https://doi.org/10.1038/ng.2383
Manning AK, Hivert MF, Scott RA, Grimsby JL, Bouatia-Naji N, Chen H, et al. A genome-wide approach accounting for body mass index identifes genetic variants infuencing fasting glycemic traits and insulin resistance. Nat Genet. 2012;44(6):659–69. https://doi.org/10.1038/ng.2274
Gortmaker SL, Must A, Sobol AM, Peterson K, Colditz GA, Dietz WH. Television viewing as a cause of increasing obesity among children in the United States, 1986–1990. Arch Pediatr Adolesc Med. 1996;150(4):356–62. https://doi.org/10.1001/archpedi.1996.02170290022003
Wilmot EG, Edwardson CL, Achana FA, Davies MJ, Gorely T, Gray LJ, et al. Sedentary time in adults and the association with diabetes, cardiovascular disease and death: systematic review and meta-analysis. Diabetologia. 2012;55(11):2895–905. https://doi.org/10.1007/s00125-012-2677-z
Schmid D, Leitzmann MF. Television viewing and time spent sedentary in relation to cancer risk: a meta-analysis. J Natl Cancer Inst. 2014;106(7):dju098. https://doi.org/10.1093/jnci/dju098
Patterson R, McNamara E, Tainio M, de Sá TH, Smith AD, Sharp SJ, et al. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: a systematic review and dose response meta-analysis. Eur J Epidemiol. 2018;33(9):811–29. https://doi.org/10.1007/s10654-018-0380-1
Chae WR, Nübel J, Baumert J, Gold SM, Otte C. Association of depression and obesity with C-reactive protein in Germany: a large nationally representative study. Brain Behav Immun. 2022;103:223–31. https://doi.org/10.1016/j.bbi.2022.04.024
Wang R, Snieder H, Hartman CA. Familial co-aggregation and shared heritability between depression, anxiety, obesity and substance use. Transl Psychiatry. 2022;16;12(1):108. https://doi.org/10.1038/s41398-022-01868-3
Sander C, Ueck P, Mergl R, Gordon G, Hegerl U, Himmerich H. Physical activity in depressed and non-depressed patients with obesity. Eat Weight Disord. 2018;23(2):195–203. https://doi.org/10.1007/s40519-016-0347-8
Gujral S, Aizenstein H, Reynolds CF 3rd, Butters MA, Erickson KI. Exercise effects on depression: possible neural mechanisms. Gen Hosp Psychiatry. 2017;49:2–10. https://doi.org/10.1016/j.genhosppsych.2017.04.012
López-Torres Hidalgo J, DEP-EXERCISE Group. Effectiveness of physical exercise in the treatment of depression in older adults as an alternative to antidepressant drugs in primary care. BMC Psychiatry. 2019;19(1):21. https://doi.org/10.1186/s12888-018-1982-6
Santini ZI, Jose PE, York Cornwell E, Koyanagi A, Nielsen L, Hinrichsen C, et al. Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older americans (NSHAP): a longitudinal mediation analysis. Lancet Public Health. 2020;5(1):e62–e70. https://doi.org/10.1016/S2468-2667(19)30230-0
Noguchi T, Saito M, Aida J, Cable N, Tsuji T, Koyama S, et al. Association between social isolation and depression onset among older adults: a cross-national longitudinal study in England and Japan. BMJ Open. 2021;11(3):e045834. https://doi.org/10.1136/bmjopen-2020-045834
Difrancesco S, Lamers F, Riese H, Merikangas KR, Beekman ATF, van Hemert AM, et al. Sleep, circadian rhythm, and physical activity patterns in depressive and anxiety disorders: a 2-week ambulatory assessment study. Depress Anxiety. 2019;36(10):975–86. https://doi.org/10.1002/da.22949
Wirz-Justice A, Skene DJ, Münch M. The relevance of daylight for humans. Biochem Pharmacol. 2021;191:114304. https://doi.org/10.1016/j.bcp.2020.114304
Burns AC, Saxena R, Vetter C, Phillips AJK, Lane JM, Cain SW. Time spent in outdoor light is associated with mood, sleep, and circadian rhythm-related outcomes: a cross-sectional and longitudinal study in over 400,000 UK Biobank participants. J Affect Disord. 2021;295:347–52. https://doi.org/10.1016/j.jad.2021.08.056
Karmel W, Choi C-Y, Chen MB, Stein YC, Klimentidis M-J, Wang, Karestan C, Koenen, et al. Assessment of bidirectional relationships between physical activity and depression among adults: a 2-sample Mendelian randomization study. JAMA Psychiatry. 2019;76(4):399–408. https://doi.org/10.1001/jamapsychiatry.2018.4175
Lisa M, McEwen EG, Gatev MJ, Jones, Julia L, MacIsaac, Megan M, McAllister RE, Goulding, et al. DNA methylation signatures in peripheral blood mononuclear cells from a lifestyle intervention for women at midlife: a pilot randomized controlled trial. Appl Physiol Nutr Metab. 2018;43(3):233–9. https://doi.org/10.1139/apnm-2017-0436
Mahmood Rasool A, Malik MI, Naseer A, Manan S, Ansari I, Begum, et al. The role of epigenetics in personalized medicine: challenges and opportunities. BMC Med Genomics. 2015;8(Suppl 1):5. https://doi.org/10.1186/1755-8794-8-S1-S5
Tina Rönn P, Volkov C, Davegårdh T, Dayeh E, Hall, Anders H, Olsson, et al. A six months exercise intervention influences the genome-wide DNA methylation pattern in human adipose tissue. PLoS Genet. 2013;9(6):e1003572. https://doi.org/10.1371/journal.pgen.1003572
Richard C, Shelton AH, Miller. Inflammation in depression: is adiposity a cause? Dialogues Clin Neurosci. 2011;13(1):41–53. https://doi.org/10.31887/DCNS.2011.13.1/rshelton
Dona AC, DeLouize AM, Eick G, Thiele E, Salinas Rodríguez A, Manrique Espinoza BS, et al. Inflammation and central adiposity as mediators of depression and uncontrolled diabetes in the study on global AGEing and adult health (SAGE). Am J Hum Biol. 2020;32(6):e23413. https://doi.org/10.1002/ajhb.23413
Vreeburg SA, Hoogendijk WJ, van Pelt J, Derijk RH, Verhagen JC, van Dyck R, et al. Major depressive disorder and hypothalamic-pituitary-adrenal axis activity: results from a large cohort study. Arch Gen Psychiatry. 2009;66(6):617–26. https://doi.org/10.1001/archgenpsychiatry.2009.50
Funding
No funding.
Author information
Authors and Affiliations
Contributions
HJB and YW conceived and designed the research. HJB and LLZ managed the data and performed the bioinformatics analyses. The manuscript was rewritten and modified by HJB, LLZ, HMP, XFH, and YW. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Human ethics and consent to participate declarations
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ba, H., Zhang, L., Peng, H. et al. Causal links between sedentary behavior, physical activity, and psychiatric disorders: a Mendelian randomization study. Ann Gen Psychiatry 23, 9 (2024). https://doi.org/10.1186/s12991-024-00495-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12991-024-00495-0