
Abstract
Purpose
The COVID-19 pandemic increased psychiatric distress and impacts differed by family structure. We aimed to identify mechanisms contributing to these inequalities.
Methods
Survey data were from the UK Household Longitudinal Study. Psychiatric distress (GHQ-12) was measured in April 2020 (first UK lockdown; n = 10,516), and January 2021 (lockdown re-introduced following eased restrictions; n = 6,893). Pre-lockdown family structure comprised partner status and presence of children (< 16 years). Mediating mechanisms included: active employment, financial strain, childcare/home-schooling, caring, and loneliness. Monte Carlo g-computation simulations were used to adjust for confounding and estimate total effects and decompositions into: controlled direct effects (effects if the mediator was absent), and portions eliminated (PE; representing differential exposure and vulnerability to the mediator).
Results
In January 2021, after adjustment, we estimated increased risk of distress among couples with children compared to couples with no children (RR: 1.48; 95% CI 1.15–1.82), largely because of childcare/home-schooling (PE RR: 1.32; 95% CI 1.00–1.64). Single respondents without children also had increased risk of distress compared to couples with no children (RR: 1.55; 95% CI 1.27–1.83), and the largest PE was for loneliness (RR: 1.16; 95% CI 1.05–1.27), though financial strain contributed (RR: 1.05; 95% CI 0.99–1.12). Single parents demonstrated the highest levels of distress, but confounder adjustment suggested uncertain effects with wide confidence intervals. Findings were similar in April 2020 and when stratified by sex.
Conclusion
Access to childcare/schooling, financial security and social connection are important mechanisms that need addressing to avoid widening mental health inequalities during public health crises.
Similar content being viewed by others


Introduction
Psychiatric distress increased globally during the COVID-19 pandemic, especially in countries with higher infection rates and stricter lockdowns [1]. Findings on mental health in the early pandemic [2,3,4,5,6,7,8,9,10] differ, with some reporting early growth in anxiety and depression followed by decreases as people adapted, but a pooled analysis of 11 longitudinal population surveys in the UK found increases in psychiatric distress that persisted from March 2020–March 2021 [11]. Psychiatric distress increased more among: women than men; highly educated than less well-educated people; and adults aged 25–44 than younger and older adults [11]. Unequal impacts may reflect differing exposure to aspects of pandemic management that cause distress, such as: job loss, financial strain, social isolation or caring responsibilities for children or elderly relatives [12]. Inequalities in outcomes may also reflect differing vulnerability to such mechanisms (i.e. being more or less affected by exposure to job loss, financial strain, etc.), or a combination of differential exposure and vulnerability [13]. Understanding how differential impacts develop can help address inequalities.
Family structure may also have been associated with inequalities in exposure and vulnerability to distressing aspects of the pandemic. Lone parents may have experienced greater financial strain than couple parents, for example, because they are more likely to live on a low income [14], and may have felt more isolated than couples during lockdowns. Working parents also had to balance childcare and home-schooling with work during school closures, and working lone parents had no partner to share these responsibilities.
We explore contributions of five potential mediating mechanisms to inequalities in psychiatric distress by family structure during UK lockdowns: active employment, financial strain, childcare and home-schooling, caring, and loneliness. In addition to testing for mediation/moderation in relation to these five factors, we test the hypothesis that findings from the 1st UK lockdown in April 2020 (where most existing research is focused), will differ compared to findings using data from January 2021 as lockdowns were re-introduced following eased restrictions. Given reports of women being disproportionally affected by increases in childcare and other caring burdens during the pandemic [15,16,17], we further test the hypothesis that the mediating and moderating effects of these five factors differ by gender.
Methods
Sample
Understanding Society (the UK Household Longitudinal Study) is a nationally representative longitudinal household panel study, based on a clustered-stratified probability sample of UK households, detailed elsewhere [18]. All adults aged 16 + years in chosen households are invited to participate annually in surveys spanning 24 months. We used pre-pandemic data from 2018 to 2019, with an individual response rate of 65.4%. Additional online surveys [19] were conducted during the pandemic and our main analyses use data from surveys in April, Sep and Nov 2020 and Jan 2021 (response rates: 40.3%, 29.2%, 27.3% and 27.2%). We also present descriptive data from surveys in 2017–2018 and in May, June and July 2020.
We defined two analytical samples relating to initial and later UK lockdowns. The analytical sample for April 2020 (1st lockdown) was based on participants aged 16 + from the 2018–2019 pre-pandemic survey who had complete data on all analysis variables from that and the April COVID survey (n = 10,516). The January 2021 sample (later lockdown) comprised those participating in the 2018–2019 pre-pandemic survey with complete data for analysis variables from that and from COVID surveys in September and November 2020 and January 2021 (n = 6,893; respondent inclusion flowchart in Additional file 1: Figure S1). Analyses were weighted for survey attrition and non-response.
Measures
For the April 2020 sample, baseline information was from the 2018–2019 survey, with mediators and outcomes measured in April 2020. For the January 2021 data, baseline information was from either the September 2020 survey (during the period of eased restrictions), or the 2018–2019 survey if not available there. Information for mediating variables was from surveys in November 2020 and January 2021 (see Table 1).
Exposure: pre-lockdown family structure
Family structure was coded for each individual based on presence of a spouse/partner and children (aged < 16 years), as follows: couple with no children; couple with children; single with no children; and single with children.
Outcome: psychiatric distress during lockdown
Symptoms of anxiety and depression were measured with the 12-item General Health Questionnaire (GHQ) [20], with scores of 4 + coded as psychiatric distress.
Mediators
Five mediating pathways reflecting material and psychosocial mechanisms were considered: active employment, financial strain, childcare/home-schooling, caring and loneliness.
Respondents reporting full-time, part-time or self-employment were coded as in active employment, while furloughed respondents and those economically inactive for other reasons were coded as not in active employment. We grouped furloughed and other economically inactive groups together such that this variable primarily relates to spending time working. We reasoned that at least some of the key differences between furloughed and other economically inactive respondents would be captured by the next mediating pathway: financial strain, which was measured with the question: How well would you say you yourself are managing financially these days? Answers were coded in two categories (living comfortably, doing alright, or just about getting by vs finding it quite or very difficult).
Childcare/home-schooling indicated reporting any time spent on childcare and home-schooling. This was not deterministically related to family structure as some with children aged < 16 years did not report spending time on childcare, and some reported spending time on childcare despite not living with a child aged < 16 years, for example, they could have been helping someone else or caring for a child aged 16 + years.
Caring indicated looking after or giving special help to someone who was sick, disabled or elderly, either within the same household or outside of the household.
Loneliness was measured with the question: In the last 4 weeks, how often did you feel lonely? Answer categories were: hardly ever or never, some of the time, and often; binary coded to indicate often feeling lonely.
Confounders
Pre-lockdown confounders included: sex (male vs female), race/ethnicity (White vs non-White ethnic minority), UK country (England, Scotland, Wales or Northern Ireland), age in years (16–34, 35–54, 55 +), education (degree-level vs less education), longstanding illness (any vs none); National Statistics Socioeconomic Classification (NS-SEC) codes for occupational class (four categories: professional/managerial; intermediate; routine/unskilled; or long-term non-employed); poverty (household income < 60% of the median); smoking status (current vs non-smoker); alcohol consumption measured using the AUDIT-C scale (coded with scores of 8 + indicating moderate–high risk drinking); loneliness (measured as described above); and psychiatric distress (GHQ as above).
Additional confounders measured during lockdown included indicators for: changes in family structure from pre-lockdown state; whether respondents had received a letter from the National Health Service advising them to shield/isolate; and whether respondents identified as a keyworker, i.e. their occupation was considered critical enough for them to continue working in their workplace during the lockdown.
Analysis
First, we provide descriptive data showing the characteristics of the analytic samples and proportions with high psychiatric distress by family structure over the course of the pandemic. Our main analyses used Monte Carlo g-computation simulations [21] to decompose inequalities in psychiatric distress by family structure into their mediating mechanisms (details in Additional file 1: Appendix S2 and Figure S3). Logistic and multinomial models were estimated for analysis variables using observed data on variables assumed to precede them in the causal pathway (Additional file 1: Figure S4). Models from observed data were then used to simulate hypothetical interventions on family structure and mediating pathways. Simulations were validated by comparing runs with no intervention against the observed data. Comparison of proportions with psychiatric distress across simulation arms with family structure set to different values enabled calculation of risk ratios representing total effects (TE) for each of the following (exposure vs reference) comparisons:
-
1.
Couple with children (exposure) compared against couple with no children (reference); i.e. the effect of children < 16 years within couples.
-
2.
Single with no children (exposure) compared against couple with no children (reference); i.e. the effect of being single among those without children < 16 years.
-
3.
Single with children (exposure) compared against couple with children (reference); i.e. the effect of being single among those with children < 16 years.
-
4.
Single with children (exposure) compared against single with no children (reference); i.e. the effect of children < 16 years among those who are single.
Total effects for 1–4 above were decomposed for each mediating mechanism into [22]:
-
A.
A controlled direct effect (CDE) representing the effect of the family structure, in the absence of the mediator.
-
B.
A pure indirect effect (PIE) representing the effect of the family structure, purely through differential exposure to the mediator of interest.
-
C.
A reference interaction (rINT) representing differential vulnerability to the effects of the mediator within the exposure group.
-
D.
A mediated interaction (mINT) representing the combination of differential vulnerability and differential exposure to the mediator.
For ease of presentation, we sum the latter three components (B-D) together into a Portion Eliminated (PE), representing the portion of the effect that would be eliminated in the absence of the mediator, i.e. the portion that is due to differential exposure and/or differential vulnerability to the mediator. Full decompositions are in Additional file 1, with relevant insights highlighted in the text. Where controlled direct effects (CDE) are similar to the total effect, this indicates a mediating mechanism does not make a strong contribution. Whereas, if the CDE differs from the total effect and the PE differs from the null, this indicates a contribution to the total effect.
For comparisons 1 and 2, we additionally estimated effects stratified by gender, while this was not possible for comparisons 3 and 4 where the family structure of interest (single with children < 16 years) was predominantly female. Additional analyses assessed sensitivity of findings to more conservative confounding assumptions (see Additional file 1: Figure S5).
Results
Descriptive statistics
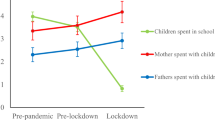
Figure 1 shows the prevalence of psychiatric distress by family structure, for two annual pre-pandemic surveys and from surveys at different stages of the pandemic. Mental health was patterned by family structure before the pandemic. Respondents who were single with children had the worst rates of psychiatric distress, followed by those who were single with no children, while those in couples with no children fared best. This patterning was accentuated during the first UK lockdown (covering the April–June 2020 surveys), returned close to previous levels as restrictions eased over summer, and was accentuated again during the further lockdowns.

Psychiatric distress by family structure during the COVID-19 pandemic in the UK Household Longitudinal Study
Additional file 1: Table S6 provides descriptive statistics for both samples, overall and by family structure. Single respondents with children were: predominantly female, younger than 55 years of age, more likely to be in household poverty and to be smokers. Single respondents (with or without children) were more likely to often feel lonely, experience psychiatric distress, and report financial difficulties. Respondents with children had higher proportions spending time on childcare and home-schooling, and caring for others in or out of the household.
Additional file 1: Figures S7–S8 show validation of our simulations comparing observed vs simulated prevalence of all variables (mean and 95% confidence intervals from 1000 simulations), with no manipulation of family structure or mediators. Additional file 1: Figures S9–S16 show further validation, sampling only from within each family structure category. Simulations generally returned proportions similar to those in the observed data.
Estimated effects of family structure on psychiatric distress and decomposition of effects via mediating pathways
For each comparison, figures display the estimated total effect and decomposition into CDE and PE for each mediating mechanisms in April 2020 and January 2021. Where the PE is closer to the TE and the CDE nearer to the null, the mediating pathway is more important. Additional file 1 details four-way decompositions, simulated proportions experiencing psychiatric distress in the comparison groups, analyses stratified by gender (where applicable), and sensitivity analyses with more conservative confounding assumptions. Key findings from Additional file 1 are highlighted below.
Couples with children vs. without children
Figure 2 shows the effect estimates (Total, CDE and PE) comparing the risk of psychiatric distress in couples with children against those without. With estimates adjusted for confounding factors, having children was associated with increased risk of psychiatric distress during lockdowns among couples (April 2020 RR: 1.15; 95% CI 0.98–1.33; Jan 2021 RR 1.48; 95% CI 1.15–1.82). In both samples childcare and home-schooling was associated with the largest contributions to the total (April 2020 PE RR 1.20; 95% CI 0.99–1.40; January 2021 PE RR 1.32; 95% CI 1.00–1.64). The four-way decomposition (Additional file 1 Table S17) indicated this was mainly due to differential exposure to childcare and home-schooling, but there was evidence of differential vulnerability too, especially in April 2020. In April 2020 couples with children were also less susceptible to remaining in active employment, and that this helped mitigate otherwise larger effects (rINT RR 0.84; 95% CI 0.65–1.06 with CDE RR 1.31; 95% CI 0.99–1.63), but no similar pattern was apparent in January 2021. When stratifying by gender (Additional file 1 Tables S18-S19) confidence intervals were wider, but estimates were largely consistent in magnitude with those above, except for females in April 2020 where females in couples with and without children had similarly high proportions with psychiatric distress (36–37%; RR 1.05; 95% CI 0.88–1.21). Even here though, there was a clear PE for childcare/home-schooling (RR 1.30; 95% CI 1.10–1.49). More conservative control for confounding gave similar findings (Additional file 1: Table S20).

Decompositions for psychiatric distress differences between couples with children vs without children
Singles vs. couples without children
Figure 3 shows estimates for being single compared to being in a couple among those with no children. The confounder-adjusted estimates indicated that being single was associated with increased risk of psychiatric distress during lockdowns (April 2020 RR 1.28; 95% CI 1.11–1.44; Jan 2021 RR 1.55; 95% CI 1.27–1.83). In both April 2020 and January 2021, the largest PEs were related to loneliness (April 2020 RR 1.18; 95% CI 1.12–1.24; January 2021 RR 1.16; 95% CI 1.05–1.27). Finer decomposition (Additional file 1: Table S21) indicated this was due to differential exposure to loneliness. There were also minor PEs related to financial strain (April 2020 RR: 1.07; 95% CI 1.02–1.12; January 2021 RR: 1.05; 95% CI 0.99–1.12), which in April 2020 were clearly related to differential exposure, while in January 2021 differential exposure may have been combined with differential vulnerability. Results were consistent for both genders (Additional file 1: Tables S22-S23), except that in January 2021, there was evidence that single compared to couple males experienced differential vulnerability to remaining in active employment (rINT RR 1.34; 95% CI 1.00–1.67). Effects were attenuated with more conservative confounding control but remained consistent (Additional file 1: Table S24).

Decompositions for psychiatric distress differences between singles vs. couples without children
Singles vs. couples with children
Estimates in Fig. 4 show effects of being single among those with children. An effect could be distinguished from confounding factors in April 2020 (RR 1.41; 95% CI 1.03–1.79) but not in January 2021 (RR 1.22; 95% CI 0.76–1.69). No mediators clearly contributed to higher rates of distress among single parents, though caring apparently mitigated an otherwise larger effect in January 2021 (RR 0.79; 95% CI 0.61–0.98). Detailed decompositions (Additional file 1: Table S25) suggested single parents were less vulnerable to caring than couple parents. There was evidence of differential exposure to loneliness, but this was mitigated by lower susceptibility such that there was no clear overall PE for loneliness. More conservative confounding control (Additional file 1: Table S26) still suggested a mitigating effect of lower susceptibility to caring (rINT RR 0.81; 95% CI 0.63–0.98), but all other effects were attenuated, including the total effect in April 2020 (RR 1.26; 95% CI 0.95–1.57). Thus, differential distress experienced in this group may have been largely due to characteristics established prior to the pandemic (even if these pre-pandemic differences were caused by the difference in family structure).

Decompositions for psychiatric distress differences between singles vs. couples with children
Singles with children vs. without children
Estimates in Fig. 5 show effects of having children among singles, which could not be confidently distinguished above the effects of confounding factors (April 2020 RR 1.24; 95% CI 0.91–1.58; January 2021 RR 1.10; 95% CI 0.68–1.52), nor was there clear evidence for contributions from any mediator (Additional file 1: S27). More conservative confounding control (Additional file 1: Table S28) also found no clear effects. Thus, differential distress between singles and couples with children appeared largely accounted for by confounding.

Decompositions for psychiatric distress differences between singles with children vs. without children
Discussion
During the UK’s first lockdown in April 2020, and then in January 2021, when lockdowns had been re-introduced after a summer of eased restrictions, we examined differences in psychiatric distress by family structure with representative UK survey data. With a novel simulation approach allowing us to distinguish differential exposure and differential vulnerability to mediating factors, we investigated contributions from active employment, financial difficulties, childcare/home-schooling, other caring, and loneliness. At both time-points, couples with children < 16 years had greater risk of psychiatric distress than those without, even after adjusting for confounders. Differential exposure and vulnerability to childcare and home-schooling were the clearest contributing mechanisms. Among respondents who did not have children < 16 years, being single rather than in a couple was also associated with increased risk for psychiatric distress at both time-points and after confounder adjustment. Differential exposure to loneliness contributed most clearly to this difference, but differential exposure to financial strain also made a minor contribution. These findings were consistent for both men and women. Single parents (predominantly women) had the highest levels of distress, but effects of single parenthood could not be confidently distinguished above those of confounding factors.
Childcare/home-schooling contributing to differences in mental health between couples with and without children in the home, concurs with previous analyses of working parents using the April–May 2020 data [23], and confirm this was still happening later in the pandemic (January 2021). While facing greater childcare burdens than men during the pandemic may have contributed to higher levels of distress among women [15,16,17], we did not find that childcare or caring made greater contributions to the mental health differences associated with having children in the home for women than it did for men. In at least some instances this was apparently because women were experiencing high levels of distress regardless of whether young children were at home.
Previous findings also suggest that single parents were especially vulnerable to increased distress during the pandemic [14], and while we confirmed this descriptively, there was insufficient evidence to support single parenthood as a cause of higher distress during the COVID-19 pandemic. This may be due to low statistical power as confidence intervals were wide and relative risk estimates (as well as absolute differences in the estimated proportions with distress) were of similar magnitude to other comparisons. Our estimates were also based on comparing single parents to others with similar background characteristics (i.e. average effects among the exposed), rather than population average effects. Considering that single parents represent a select minority of all families with higher rates of disadvantage, it is feasible that estimates based within this select population could differ from those in the general population, and that risk was raised enough based on other disadvantages that single parenthood had little additional effect. Interestingly, while single parents were more exposed to loneliness than couple parents, they were less vulnerable to it (resulting in no effect overall), suggesting they may have developed adaptive coping strategies for dealing with loneliness.
Causal interpretation of findings rests on assumptions regarding causal direction between variables (as detailed in Additional file 1: Appendix S3 and Figures S5, S6), perfectly measured confounders, and no unobserved confounders, either of the relationship between family structure and mental health, or of their relationships to mediators. Findings were robust to treating a set of mediator-outcome confounders more conservatively as exposure-outcome confounders. Nevertheless, reverse causation and unmeasured confounding remain possible. For example, we treated mental health during the pandemic as an outcome with confounding adjustment for pre-lockdown mental health, assuming mediators like loneliness and financial strain occupied intermediary positions in the causal pathway. Early changes in mental health during the pandemic could plausibly have influenced respondents’ perceptions of their loneliness or financial situation and this could be an alternative explanation for our findings. Analyses were weighted for response to COVID-19 surveys, but response rates were relatively low and residual selection bias could remain. Furthermore, estimated contributions of mediating mechanisms to total effects may reflect both differences in the actual strength of causal processes and differences in how well measures reflected any true causal processes.
Data sparsity presented some issues. We could only use a broad age categorisation because of few single parents at older ages. Single parent comparisons exhibited effects sizes of similar magnitude to other comparisons, but confidence intervals were wide, making it hard to distinguish noise from real effects. Additionally, while interactions between family structure and mediators were included, we were not able to examine interactions between mediating mechanisms, or moderation of mediating mechanisms by a wider range of factors other than gender and timing during the course of the pandemic. For example, childcare and home-schooling might have had more of an effect on distress when coupled with active employment, and other studies have indicated that having to adapt working patterns for such reasons during the pandemic was especially closely linked to distress [24]. Similarly, the role of childcare and home-schooling might have varied depending on factors such as housing, or parental education, and these could be important avenues for further study.
While financial concerns had a minor role in contributing to differences in mental health between singles and couples, neither they nor remaining actively employed, or caring for the sick, elderly or disabled appeared to be strong drivers of inequalities in mental health by family structure. The relative lack of contribution from economic mechanisms may be because the UK job retention scheme (furlough) was helping to ameliorate impacts of economic disruption on mental health [25].
Between the UK’s first lockdown in April 2020 and subsequent lockdowns in late 2020/early 2021 little progress had been made in mitigating key mechanisms leading to family structure-based differences in distress. Demands of childcare and home-schooling appeared to be leading to an excess mental health burden among those with young children in their household, while loneliness was apparently leading to poorer mental health among single people than those in couples. In managing future pandemics or other crises (e.g. involving isolation orders), or even considering on-going moves towards home working, a focus on measures that support financial security, social connections and continued access to childcare, early years’ education and learning, and schooling for young children may be important to avoid exacerbating adult mental health inequalities. This might include measures such as more generous parental leave entitlements, regulations that promote flexible working and/or job sharing, or investment in schools, childcare facilities, and community resources that promote social connection. Furthermore, showing who fares worst and why when such resources are curtailed also highlights the importance of these mechanisms for supporting equal population mental health more generally. Future research should compare different approaches to intervening on these mechanisms with respect to their effectiveness, cost-effectiveness and equity impact.
Data availability
Understanding Society data are available through the UK data service. Main surveys: https://beta.ukdataservice.ac.uk/datacatalogue/studies/study?id=6614. COVID surveys: https://beta.ukdataservice.ac.uk/datacatalogue/studies/study?id=8644
Code availability
Analytical code is available in Additional File 2.
References
Santomauro DF, Mantilla Herrera AM, Shadid J, Zheng P, Ashbaugh C, Pigott DM, Abbafati C, Adolph C, Amlag JO, Aravkin AY, Bang-Jensen BL, Bertolacci GJ, Bloom SS, Castellano R, Castro E, Chakrabarti S, Chattopadhyay J, Cogen RM, Collins JK, Dai X, Dangel WJ, Dapper C, Deen A, Erickson M, Ewald SB, Flaxman AD, Frostad JJ, Fullman N, Giles JR, Giref AZ, Guo G, He J, Helak M, Hulland EN, Idrisov B, Lindstrom A, Linebarger E, Lotufo PA, Lozano R, Magistro B, Malta DC, Månsson JC, Marinho F, Mokdad AH, Monasta L, Naik P, Nomura S, O’Halloran JK, Ostroff SM, Pasovic M, Penberthy L, Reiner RC Jr, Reinke G, Ribeiro ALP, Sholokhov A, Sorensen RJD, Varavikova E, Vo AT, Walcott R, Watson S, Wiysonge CS, Zigler B, Hay SI, Vos T, Murray CJL, Whiteford HA, Ferrari AJ. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. 2021;398(10312):1700–12. https://doi.org/10.1016/S0140-6736(21)02143-7.
Pierce M, Hope H, Ford T, Hatch S, Hotopf M, John A, Kontopantelis E, Webb R, Wessely S, McManus S, Abel KM. Mental health before and during the COVID-19 pandemic: a longitudinal probability sample survey of the UK population. Lancet Psychiatry. 2020;7(10):883–92. https://doi.org/10.1016/S2215-0366(20)30308-4.
Henderson M, Fitzsimons E, Ploubidis GB, Richards M, Patalay P. Mental health during lockdown: evidence from four generations—Initial findings from the COVID-19 Survey in Five National Longitudinal Studies. London: UCL Centre for Longitudinal Studies; 2020.
O’Connor RC, Wetherall K, Cleare S, McClelland H, Melson AJ, Niedzwiedz CL, O’Carroll RE, O’Connor DB, Platt S, Scowcroft E, Watson B, Zortea T, Ferguson E, Robb KA. Mental health and well-being during the COVID-19 pandemic: longitudinal analyses of adults in the UK COVID-19 Mental Health & Wellbeing study. Br J Psychiatry. 2021;218(6):326–33. https://doi.org/10.1192/bjp.2020.212.
Fancourt D, Steptoe A, Bu F. Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: a longitudinal observational study. Lancet Psychiatry. 2021;8(2):141–9. https://doi.org/10.1016/S2215-0366(20)30482-X.
Pierce M, McManus S, Hope H, Hotopf M, Ford T, Hatch SL, John A, Kontopantelis E, Webb RT, Wessely S, Abel KM. Mental health responses to the COVID-19 pandemic: a latent class trajectory analysis using longitudinal UK data. Lancet Psychiatry. 2021;8(7):610–9. https://doi.org/10.1016/s2215-0366(21)00151-6.
Kwong A, Pearson R, Smith D, Northstone K, Lawlor D, Timpson N. Longitudinal evidence for persistent anxiety in young adults through COVID-19 restrictions [version 1; peer review: 2 approved with reservations]. Wellcome Open Research. 2020;5:195. https://doi.org/10.12688/wellcomeopenres.16206.1.
Robinson E, Sutin AR, Daly M, Jones A. A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID-19 pandemic in 2020. J Affect Disord. 2022;296:567–76. https://doi.org/10.1016/j.jad.2021.09.098.
Bonati M, Campi R, Segre G. Psychological impact of the quarantine during the COVID-19 pandemic on the general European adult population: a systematic review of the evidence. Epidemiol Psychiatr Sci. 2022;31:e27. https://doi.org/10.1017/s2045796022000051.
Niedzwiedz CL, Green MJ, Benzeval M, Campbell D, Craig P, Demou E, Leyland A, Pearce A, Thomson R, Whitley E, Katikireddi SV. Mental health and health behaviours before and during the initial phase of the COVID-19 lockdown: longitudinal analyses of the UK Household Longitudinal Study. J Epidemiol Community Health. 2021;75(3):224–31. https://doi.org/10.1136/jech-2020-215060.
Patel K, Robertson E, Kwong ASF, Griffith GJ, Willan K, Green MJ, Di Gessa G, Huggins CF, McElroy E, Thompson EJ, Maddock J, Niedzwiedz CL, Henderson M, Richards M, Steptoe A, Ploubidis GB, Moltrecht B, Booth C, Fitzsimons E, Silverwood R, Patalay P, Porteous D, Katikireddi SV. Psychological distress before and during the COVID-19 pandemic among adults in the United Kingdom based on coordinated analyses of 11 longitudinal studies. JAMA Netw Open. 2022;5(4):e227629–e227629. https://doi.org/10.1001/jamanetworkopen.2022.7629.
Etheridge B, Spantig L (2020) The gender gap in mental well-being during the Covid-19 outbreak: evidence from the UK. ISER Working Paper Series: 2020–08. ISER, Colchester
Diderichsen F, Hallqvist J, Whitehead M. Differential vulnerability and susceptibility: how to make use of recent development in our understanding of mediation and interaction to tackle health inequalities. Int J Epidemiol. 2019;48(1):268–74. https://doi.org/10.1093/ije/dyy167.
Benzeval M, Burton J, Crossley TF, Fisher P, Jäckle A, Low H, Read B (2020) The idiosyncratic impact of an aggregate shock: the distributional consequences of COVID-19. Understanding Society Working Paper Series: 2020–09. ISER, Colchester
Seedat S, Rondon M. Women’s wellbeing and the burden of unpaid work. BMJ. 2021;374:n1972. https://doi.org/10.1136/bmj.n1972.
Xue B, McMunn A. Gender differences in unpaid care work and psychological distress in the UK Covid-19 lockdown. PLoS ONE. 2021;16(3):e0247959. https://doi.org/10.1371/journal.pone.0247959.
Almeida M, Shrestha AD, Stojanac D, Miller LJ. The impact of the COVID-19 pandemic on women’s mental health. Arch Womens Ment Health. 2020;23(6):741–8. https://doi.org/10.1007/s00737-020-01092-2.
University of Essex, Institute for Social and Economic Research, NatCen Social Research, Kantar Public (2020) Understanding Society: Waves 1–10, 2009–2017 and Harmonised BHPS: Waves 1–18, 1991–2009. 13th Edition. UK Data Service
University of Essex, Institute for Social and Economic Research (2021) Understanding Society: COVID-19 Study, 2020-2021. 11th Edition. UK Data Service
Goldberg D, Williams P (1988) A user's guide to the general health questionnaire. NFER-Nelson, Windsor
Wang A, Arah OA. G-computation demonstration in causal mediation analysis. Eur J Epidemiol. 2015;30(10):1119–27. https://doi.org/10.1007/s10654-015-0100-z.
VanderWeele TJ. A unification of mediation and interaction: a four-way decomposition. Epidemiology. 2014;25(5):749–61. https://doi.org/10.1097/EDE.0000000000000121.
Cheng Z, Mendolia S, Paloyo AR, Savage DA, Tani M. Working parents, financial insecurity, and childcare: mental health in the time of COVID-19 in the UK. Rev Econ Household. 2021;19(1):123–44. https://doi.org/10.1007/s11150-020-09538-3.
Xue B, McMunn A. Gender differences in the impact of the Covid-19 lockdown on unpaid care work and psychological distress in the UK. SocArXiv. 2020. https://doi.org/10.31235/osf.io/wzu4t.
Jacques W, Booth C, Wielgoszewska B, Green MJ, Di Gessa G, Huggins CF, Griffith GJ, Kwong ASF, Bowyer RCE, Maddock J, Patalay P, Silverwood RJ, Fitzsimons E, Shaw R, Thompson EJ, Steptoe A, Hughes A, Chaturvedi N, Steves CJ, Katikireddi SV, Ploubidis GB. Mental and social wellbeing and the UK coronavirus job retention scheme: evidence from nine longitudinal studies. Social Sci Med. 2022;308:115226. https://doi.org/10.1016/j.socscimed.2022.115226.
Funding
This work was supported by the Medical Research Council [MC_UU_00022/2] and the Scottish Government Chief Scientist Office [SPHSU17]. SVK was additionally supported by a NRS Senior Clinical Fellowship [SCAF/15/02], and AP was additionally supported by a Wellcome Trust University Award [205412/Z/16/Z]. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
MJG, PC, ED, SVK, AHL and AP contributed to the research questions and conceptual design of the study. MG conducted all data management, designed and conducted the analysis, and drafted the Methods, Results and Discussion. MJG, PC, ED, and AP reviewed literature and PC drafted the Introduction. MJG, PC, ED, SVK, AHL and AP contributed to revision of the manuscript for critical content.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
In accordance with the Declaration of Helsinki the University of Essex Ethics Committee approved all data collection for the study, including verbal consent to participate. No additional ethical approval was necessary for this study. For further details see: https://www.understandingsociety.ac.uk/documentation/mainstage/user-guides/main-survey-user-guide/ethics
Competing interests
SVK was a member of the UK Scientific Advisory Group on Emergencies (SAGE) subgroup on ethnicity and co-chair of the Scottish Government Expert Reference Group on Ethnicity and COVID-19. There were no other competing interests for any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Supplementary figures, tables and appendices.
Additional file 2.
R code for analysis
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Green, M.J., Craig, P., Demou, E. et al. Understanding inequalities in mental health by family structure during COVID-19 lockdowns: evidence from the UK Household Longitudinal Study. Ann Gen Psychiatry 22, 24 (2023). https://doi.org/10.1186/s12991-023-00454-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12991-023-00454-1