
Abstract
Background
Tardive dystonia associated with antidepressant use is rare and often under-recognized. We had an experience with trazodone, which is used for delirium and insomnia prescribed in general hospital, inducing tardive dystonia.
Case presentation
A 61-year-old Japanese woman had been treated for schizophrenia. She was moved to general hospital because of consciousness disturbance. She was prescribed trazodone (25 mg/day) for delirium and insomnia. After she was discharged, she returned to the psychiatric hospital with tardive dystonia. Her dystonia symptoms improved with 3 days of discontinuing trazodone.
Conclusion
In the present case, long-term use of trazodone induced tardive dystonia. Discontinuing trazodone rapidly improved tardive dystonia.
Similar content being viewed by others

Background
Antipsychotics, which are dopamine antagonists and sometimes antidepressants, cause tardive dystonia [1]. However, tardive dystonia associated with antidepressant use is rare and often under-recognized [2].
Despite the lack of relevant and reliable safety data, trazodone continues to be widely used for treating delirium and insomnia [3,4,5,6]. Some clinicians have been noted to unnecessarily prescribe trazodone to patients with tardive dystonia.
Here, we describe the case of a Japanese woman with schizophrenia who was treated with risperidone and developed tardive dystonia after the addition of trazodone to her regimen.
Case presentation
A 61-year-old, right-handed, Japanese woman had been treated for schizophrenia since her mid-20s. She had no family history of head trauma, seizures, or substance abuse and received haloperidol, risperidone, and olanzapine for the treatment of her psychotic symptoms, such as excitement, hallucination, and difficulty in controlling emotions. Her schizophrenia symptoms indicated partial response to treatment; however, she complained of decreased motivation, delusions, and convulsive symptoms and was therefore admitted to a psychiatric ward 5 years ago. One year ago, she was moved from our psychiatric ward to a general hospital because of water intoxication-induced consciousness disturbance. At this point she was treated with risperidone 6 mg/day and chlorpromazine 75 mg/day.
The patient was discharged from the general hospital after the treatment of water intoxication and consciousness disturbance. She was prescribed trazodone (25 mg/day) for delirium and insomnia at the time of discharge. According to her chart, she had not received calcium channel blockers, such as flunarizine or cinnarizine, or lithium over the past 2 years. Within a week of discharge, she returned to the psychiatric ward with complaints of general slowness and excessive fatigue. She exhibited dysphagia, and the nurses had to regularly monitor her during her meals. The abovementioned symptoms gradually progressed and caused considerable distress in her communication, impairing her social and occupational functions.
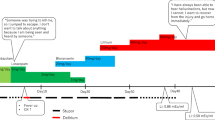
Her hematological and biochemical examinations as well as thyroid function (free total thyroxine and thyroid-stimulating hormone) were normal. Regarding the psychiatric history and diagnostic check, neither conversion nor malingering disorder was relevant for the patient. Secondary tardive dystonia caused by trazodone was diagnosed. Her dystonia symptoms, including cervical extension and dysphagia, improved within 3 days of discontinuing trazodone (Fig. 1).

Clinical course of trazodone-associated tardive dystonia
Discussion
Here, we report a case of tardive dystonia caused by administering trazodone along with the antipsychotic risperidone (4 mg/day). Few studies on trazodone-induced extrapyramidal symptoms, such as dystonia, have been reported to date [7,8,9,10].
Trazodone is widely used for treating delirium and insomnia, particularly in the elderly. Trazodone is a potent antagonist of the 5-HT2A and 5-HT2c receptors, a weak inhibitor of serotonin reuptake, a moderately to highly potent α-adrenoceptor antagonist (particularly to α1), and a moderate histaminergic (H1) antagonist.
The pathophysiology of dystonia remains unclear owing to lack of data supporting any particular mechanism. Because tardive dystonia is most commonly caused by antipsychotics, postsynaptic supersensitivity induced by sustained inhibition of dopaminergic neurotransmission was speculated to be the major mechanism underlying its clinical presentation. However, the contrast between the benefits of anticholinergics for tardive dystonia and the deterioration of patients with tardive dyskinesia following treatment with such drugs indicates a difference in their pathophysiology. Other mechanisms have also been suggested; increased serotonin transmission may inhibit dopaminergic neurons in the ventral tegmental. In addition, Remington reported a possible role of serotonergic and noradrenergic modulation of the cholinergic pathway in tardive dystonia and Pisa syndrome [11]. Another theory involves calcium channel blockers, which reportedly cause tardive blepharospasm [12] and Parkinsonism [13]; however, a review reported that the effects of calcium channel blockers on antipsychotic-induced tardive dystonia are unknown [14]. Trazodone was recently demonstrated to inhibit T-type calcium channels [15]; however, the mechanism underlying how this effect contributes to tardive dystonia remains to be elucidated.
Clinicians have been sometimes known to unnecessarily prescribe trazodone for insomnia and delirium. In the present case, long-term use of trazodone induced tardive dystonia. Discontinuing trazodone rapidly improved tardive dystonia.
Conclusion
Using trazodone as a hypnotic can cause tardive dystonia in elderly patients with schizophrenia. All healthcare providers should be informed of this serious but seemingly completely reversible adverse effect.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
References
Jankovic J, Schwartz K. Response and immunoresistance to botulinum toxin injections. Neurology. 1995;45(9):1743–6.
Lee Y, et al. Antidepressant-induced tardive syndrome: a retrospective epidemiological study. Pharmacopsychiatry. 2013;46(7):281–5.
Walsh JK, Schweitzer PK. Ten-year trends in the pharmacological treatment of insomnia. Sleep. 1999;22(3):371–5.
Okamoto Y, et al. Trazodone in the treatment of delirium. J Clin Psychopharmacol. 1999;19(3):280–2.
Mort JR, Aparasu RR. Prescribing potentially inappropriate psychotropic medications to the ambulatory elderly. Arch Intern Med. 2000;160(18):2825–31.
James SP, Mendelson WB. The use of trazodone as a hypnotic: a critical review. J Clin Psychiatry. 2004;65(6):752–5.
Sarwar AI. Trazodone and parkinsonism: the link strengthens. Clin Neuropharmacol. 2018;41(3):106–8.
Lin CC, et al. Tardive dystonia and tardive sensory syndrome related to trazodone: a case report. Prog Neuropsychopharmacol Biol Psychiatry. 2008;32(6):1609–10.
Lewis CF, DeQuardo JR, Tandon R. Dystonia associated with trazodone and sertraline. J Clin Psychopharmacol. 1997;17(1):64–5.
Kramer MS, et al. Atypical acute dystonia associated with trazodone treatment. J Clin Psychopharmacol. 1986;6(2):117–8.
Remington GJ. The Pisa syndrome: possible role for serotonin and noradrenaline. J Clin Psychopharmacol. 1988;8(3):228–9.
Alonso-Navarro H, Jimenez-Jimenez FJ. Tardive blepharospasm associated with cinnarizine use. Clin Neuropharmacol. 2006;29(4):187–9.
Terland O, Flatmark T. Drug-induced parkinsonism: cinnarizine and flunarizine are potent uncouplers of the vacuolar H + -ATPase in catecholamine storage vesicles. Neuropharmacology. 1999;38(6):879–82.
Soares-Weiser, K. and J. Rathbone, Calcium channel blockers for neuroleptic-induced tardive dyskinesia. Cochrane Database Syst Rev, 2004(1): p. Cd000206.
Kraus RL, et al. Trazodone inhibits T-type calcium channels. Neuropharmacology. 2007;53(2):308–17.
Acknowledgements
Thanks to the Minamigaoka hospital shin-3 ward drug discussion team members.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
HH, YK, MT and CO were involved in clinical investigations. YK and HH wrote the first manuscript. NO and HH were involved in the literature review and corrections. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report.
Competing of interest
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kadota, Y., Hori, H., Takayama, M. et al. Tardive dystonia improved with discontinuation of trazodone in an elderly schizophrenia patient: a case report. Ann Gen Psychiatry 19, 23 (2020). https://doi.org/10.1186/s12991-020-00273-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12991-020-00273-8