
Abstract
Background
Leptin is a peptide hormone secreted by adipose tissue and is an important determinant of obesity and its complications. The purpose of this study was to establish sex- and body mass index (BMI)-specific reference intervals for serum leptin in a Chinese population and investigate the factors influencing leptin concentrations.
Methods
Fasting serum leptin levels were assayed in 469 men and 773 women from randomly sampled Chinese residents. Blood glucose, insulin, hemoglobin A1c (HbA1c), liver enzymes, blood lipid profiles, creatinine, and uric acid (UA) levels were measured. Pearson’s correlation coefficient and multiple linear regression analyses were used to estimate the relationship between serum leptin level and other variables. The reference intervals were determined by the 2.5th and 97.5th percentiles.
Results
The mean ± standard deviation serum leptin level was much higher in women (20.92 ± 12.96 ng/mL) than in men (6.45 ± 5.53 ng/mL). The reference interval of serum leptin was 0.33–19.85 ng/mL in men and 3.60–54.86 ng/mL in women. The specific reference intervals of serum leptin in men with BMI of 20 to < 25 and 25 to < 27.5 kg/m2 were 0.42–12.32 and 2.17–20.22 ng/ml, respectively. The specific reference intervals of serum leptin in women with BMI of 20 to < 25 and 25 to < 27.5 kg/m2 were 4.11–38.09 and 8.27–48.66 ng/ml, respectively. BMI was significantly correlated with Ln (leptin) both in men (r = 0.698, P < 0.001) and women (r = 0.626, P < 0.001). In multivariate linear regression analysis, serum leptin was correlated with BMI, homeostasis model assessment of insulin resistance (HOMA-IR), UA in women, and plus triglyceride (TG) in men. The variance in serum leptin levels could be partially explained by these variables in both women (adjusted R2 = 0.447) and men (adjusted R2 = 0.552). In participants with leptin levels higher than the reference intervals, significantly higher levels of HOMA-IR, low-density lipoprotein cholesterol (LDL-C), UA, a higher proportion of central obesity (waist circumference [WC] > 90 cm), and metabolic syndrome were found in men, and significantly higher levels of HOMA-IR, UA and a higher proportion of central obesity (WC > 85 cm) were found in women.
Conclusion
This is the first study to establish sex- and BMI-specific reference intervals of leptin for both sexes in a large Chinese population. Serum concentration of leptin was predicted by BMI, HOMA-IR, UA in women, and TG in men.
Similar content being viewed by others

Introduction
Obesity and its’ comorbidities remain critical global public health issues. Over the past several decades, the number of obese women and men has increased to 390 (363–418) and 281 (257–307) million worldwide [1]. Leptin, with a size of 16 kDa, is a product of the obese (ob) gene [2]. This peptide hormone is mainly secreted by adipose tissue, and can cross the blood–brain barrier and act on neurons in the hypothalamus and elsewhere in the brain, thereby modulating food intake and body weight [3]. Under physiological conditions, the level of leptin increases when the mass of fat increases, thereby inhibiting food intake and forming a negative feedback loop [4]. In addition, leptin can regulate bone mass, reproductive function, and immune homeostasis [5]. High leptin levels are associated with greater risks of diabetes [6], non-alcoholic fatty liver disease [7], congestive heart failure, and cardiovascular disease [8]. Due to the lack of reference intervals for leptin in Chinese populations, studies on the association between leptin and the diseases described above have used different leptin cut-off points, which may be one of the reasons for the inconsistent results of these studies. Moreover, the terms “type 1 obesity” and “type 2 obesity,” which mean leptin hyposecretion or leptin resistance [4], need to be distinguished by determining the reference intervals of leptin.
Only a few studies have paid attention to the reference intervals of leptin levels in Asian healthy adults [9, 10]. Moreover, serum concentrations of leptin reflect the amount of energy stored in adipose tissue and may vary in between sexes and individuals with different BMI [11]. Although a small-scale study proposed reference intervals for leptin in native Chinese women, it did not include male participants or determine the BMI-specific reference intervals for leptin [9].
In this study, we aimed to establish sex- and BMI-specific reference intervals for serum leptin in a randomly sampled cohort from residents of Pinggu District in Beijing, as well as to identify the factors correlated with serum leptin concentrations.
Materials and methods
Study population
This is a cross-sectional study. Details of participant selection have been published in our previous publication [12]. Briefly, from September 2013 to July 2014, 6,583 individuals aged 25 to 76 years old living in the Pinggu District of Beijing, China were invited to participate in the Pinggu metabolic disease study using two-stage cluster random sampling and 4,002 individuals participated in the study. In the current analysis, a healthy population was defined by excluding participants with the following conditions (Fig. 1): (a) a history of diabetes (n = 404); (b) newly diagnosed diabetes and prediabetes (fasting plasma glucose [FPG] ≥ 6.1 mmol/L, and/or 2-h postprandial plasma glucose (PPG) after a 75-g oral glucose tolerance test [2 h-PPG] ≥ 7.8 and/or hemoglobin A1c [HbA1c] ≥ 5.7%;n = 1921) [13]; (c) self-reported history of liver diseases, including positive hepatitis B virus surface antigen (HBsAg), positive hepatitis C virus (HCV) antibody, alanine aminotransferase (ALT) ≥ 100 U/L, aspartate aminotransferase (AST) ≥ 100 U/L, or significant alcohol consumption (men > 210 g/week or women > 140 g/week [13]) (n = 361). Finally, after excluding participants with missing data on leptin concentrations (n = 74), the data of 1,242 healthy individuals were used to determine the reference intervals and correlated factors of leptin level. The study protocol was approved by the ethics committees of the Peking University Medical Center and the University of Michigan. Written informed consent was obtained from all the participants.

Flow diagram for the study population
Variables collection
Participant characteristics and medical histories were recorded through personal interviews with trained doctors and nurses. Weight and height were measured in light clothing, and BMI was calculated as weight divided by height in meters squared (kg/m2). Waist circumference (WC) was measured at the midpoint of the line between the lower edge of the ribs and iliac crest, and hip circumference (HC) at the level of the greater trochanter. After 10 min of rest, blood pressure was measured three times, and the mean systolic blood pressure (SBP) and diastolic blood pressure (DBP) were used. Participants reported their alcohol intake frequency and volume of drinks to determine alcohol consumption (g/week).
Venous blood samples were collected after 10–12 h of fasting. A standard 75-g glucose tolerance test was performed in individuals without previously diagnosed diabetes. Plasma glucose, total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), ALT, AST, serum creatinine (Cr), and uric acid (UA) levels were measured using an automated routine laboratory analyzer (UnicelDxC 800; Beckman Coulter, USA). HbA1c levels were measured by high-performance liquid chromatography (Adams A1c HA-8160; Arkray, Japan). Insulin was assayed by electrochemiluminescence (Roche E411; Roche Diagnostics). The severity of insulin resistance was evaluated by the homeostasis model assessment of insulin resistance (HOMA-IR), which was calculated as follows: HOMA-IR = FPG (mmol/L) × fasting insulin (μU/mL)/22.5 [14]. Serum leptin level was measured using a commercial ELISA kit (EMDMilipol, Billerica, MA, USA). The intra-assay coefficient variation of the ELISA method is < 5%, and the inter-assay coefficient variation is < 8.6%. HBsAg and HCV antibodies were measured by enhanced chemiluminescence assays (Ortho-Clinical Diagnostics, NJ, USA). According to the international diabetes federation (IDF) criteria, metabolic syndrome (MetS) is diagnosed if there is central obesity (WC > 90 cm for men, and > 85 cm for women, respectively), in addition to any two of the following four criteria: (1) TG level ≥ 1.7 mmol/L; (2) HDL-C < 1.0 mmol/L for men or < 1.3 mmol/L for women; (3) BP ≥ 130/85 mmHg or treatment of previously diagnosed hypertension; and (4) FPG ≥ 5.6 mmol/L or previously diagnosed as type 2 diabetes [15].
Statistical analysis
Separate analyses were conducted for men and women due to sex differences in serum leptin levels. Continuous variables with normal distribution are expressed as mean ± standard deviation (SD), and t test was used to compare differences between men and women. Continuous variables with skewed distribution were expressed as median (25th and 75th percentiles) and compared using the Mann–Whitney test. Leptin level was logarithmically transformed to Ln (leptin), because of the skewed distribution of serum leptin concentrations. Multiple linear regression analysis was used to estimate the association between the participant characteristics and serum leptin levels. Based on the Pearson’s correlation coefficients, variables with statistical significance and clinical significance were put into the multivariate linear regression model. In the multivariate linear regression analysis, variables were screened out stepwise to reach the largest adjusted R2. The adjusted R2 reflected the proportion of variation in leptin levels explained by participants’ characteristics. The sex- and BMI-specific reference intervals of serum leptin concentrations were determined using the 2.5th and 97.5th percentiles. In the supplementary files, Pearson’s correlation coefficients were used to assess the correlation between Ln (leptin) and the other variables. Participants were divided into three groups based on the 2.5th and 97.5th percentiles, and the tertiles of serum leptin levels, respectively. In addition, the differences in continuous variables among groups were compared using the analysis of variance or the Kruskal–Wallis test, and the differences in categorical variables among groups were compared using the Chi-square or Fisher’s exact tests. Receiver operating characteristic (ROC) analysis was performed for determining cut-off point of serum leptin levels, and the cut-off point was used to distinguish the participants with BMI < 25 kg/m2 (normal weight) and the participants with BMI ≥ 25 kg/m2 (overweight or obesity). Statistical significance was set at P < 0.05. The IBM SPSS Statistics software (version 21.0) was used for the statistical analysis.
Results
A total of 1242 participants were included in the study (Table 1). The mean age of the 1242 participants was 44.8 ± 11.6 years, and 37.8% (469) were men. The average BMI of the participants was 24.8 ± 3.6 kg/m2. The male participants were older than the female participants (46.1 ± 12.6 vs. 43.9 ± 10.8 years). Men were likely to be more frequent smokers, and have a higher proportion of metabolic syndrome, higher levels of BMI, WC, HC, blood pressure, FPG, TG, and serum UA than women. In contrast, women showed higher 2 h-PPG, HDL-C, and serum leptin levels than men. There were no significant differences in HOMA-IR, HbA1c, TC concentration, and LDL-C concentration between the two sexes. The median (25th and 75th percentiles) serum leptin was 12.95 (5.96 and 21.40) ng/mL in the overall population. Women had higher leptin levels (17.90 ng/mL) than men (5.20 ng/mL).
Additional file 1: Table S1 shows the correlation between Ln (leptin) and the different factors in men and women. HOMA-IR was positively correlated with Ln (leptin), whereas age and HDL-C were negatively correlated with Ln (leptin) in both sexes. Notably, the correlation coefficients of TG and UA in men were likely to be higher than those in women. BMI was the strongest factor correlated with Ln (leptin) in both men (r = 0.698) and women (r = 0.626) (Additional file 1: Table S1).
Multivariate linear regression analysis identified the most relevant factors that may affect leptin concentration. In men, BMI, HOMA-IR, TG, and UA were the variables that strongly predicted Ln (leptin), and the calculation of predicted serum leptin concentration in men was as follows: Ln (leptin) = -3.039 + 0.142 × (BMI) + 0.189 × (HOMA-IR) + 0.074 (TG) + 0.002 × (UA) (Table 2). In contrast, BMI, HOMA-IR, and UA were the variables that strongly predicted Ln (leptin) in women, with the calculation for predicted serum leptin concentration being as follows: Ln (leptin) = 0.066 + 0.092 × (BMI) + 0.157 × (HOMA-IR) + 0.001 × (UA) (Table 2).
Table 3 shows the serum leptin concentrations in each sex according to age, WC, HOMA-IR, and UA subgroups. The serum leptin levels of participants with HOMA-IR ≥ 1.00 were significantly higher than that of participants with HOMA-IR < 1.00 in both women and men (P < 0.001). Besides, serum leptin levels were significantly higher in the high-UA subgroup than in the low-UA subgroup in both women (P = 0.004) and men (P < 0.001).
Based on BMI levels, all participants were further divided into five subgroups: < 20, 20 to < 25, 25 to < 27.5, 27.5 to < 30, and ≥ 30 kg/m2. Table 4 shows the mean ± SD and reference intervals (2.5th and 97.5th percentiles) of the different BMI subgroups in each sex. Generally, the serum leptin levels of each BMI subgroup in women were much higher than those in men.
After determining the 2.5th and 97.5th percentiles for the serum leptin levels, we divided men and women with BMI of 20 to < 25 into three groups: leptin < 2.5th, 2.5th to ≤ 97.5th, and > 97.5th percentiles, respectively (Additional file 1: Table S2 and Additional file 1: Table S3). In men with a BMI of 20 to < 25, participants with leptin > 97.5th group had significantly higher levels of HOMA-IR, LDL-C, UA, a higher proportion of central obesity (WC > 90 cm), metabolic syndrome, and lower levels of HDL-C than participants with leptin of 2.5th to ≤ 97.5th group (Additional file 1: Table S2). Among women with a BMI of 20 to < 25, participants with leptin > 97.5th had significantly higher levels of HOMA-IR, UA and a higher proportion of central obesity (WC > 85 cm) compared to participants with leptin levels of 2.5th to ≤ 97.5th (Additional file 1: Table S3). In addition, as shown in Additional file 1: Table S3, participants with leptin levels > 97.5th seemed to have higher levels of LDL-C, and lower levels of HDL-C.
The clinical characteristics of men with BMI between 20 and 25 by tertiles of leptin levels are shown in Additional file 1: Table S4, and the clinical characteristics of women with BMI between 20 and 25 by tertiles of leptin levels are shown in Additional file 1: Table S5. ROC analysis for determining cut-off point of serum leptin levels is shown in Additional file 1: Table S6, along with the sensitivity, specificity, and the area under curve (AUC).
Discussion
In this large population-based study, we analyzed the correlation of leptin with other clinical characteristics and biochemical factors, including age, BMI, WC, blood glucose, HOMA-IR, blood lipid profiles, and UA. Furthermore, we proposed formulas for serum leptin concentrations using multivariate linear regression analysis in both men and women. We established sex- and BMI-specific reference intervals for serum leptin levels in both sexes, based on a healthy Chinese population.
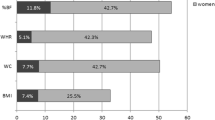
Previous studies have demonstrated a relationship between leptin levels and body fat distribution in various ethnic populations. A cross-sectional study found high correlations between leptin levels and BMI (r = 0.80 in men, 0.79 in women), and concluded that leptin production was proportional to adipose tissue mass [16]. Furthermore, another study indicated that leptin concentrations were significantly correlated with BMI (r = 0.741 in men, r = 0.814 in women) and WC (r = 0.840 in men, r = 0.718 in women) in Mexican Americans, and concluded a high association between leptin levels and overall adipose tissue depots rather than with a specific fat depot [17]. Our study found a similar correlation between serum leptin concentrations with both BMI (r = 0.698 in men and r = 0.626 in women) and WC (r = 0.712 in men and r = 0.554 in women) for both sexes. However, some studies have reported a significant correlation between leptin with other variables of body adiposity, such as skinfold thickness [18], percentage body fat [19] and truncal body fat [20].
In addition to physical measures, we investigated the association between leptin and biochemical variables. Our study showed a correlation between serum leptin concentrations and HOMA-IR in a Chinese population, which is consistent with the data of a previous study, indicating that leptin levels were positively associated with HOMA-IR (P < 0.001) in South Asian, Chinese, Aboriginal, and European Canadians [21]. Interestingly, a previous study showed a genetic correlation (r = 0.4785) and a shared genetic locus between circulating leptin concentrations and HOMA-IR [22]. Obesity leads to increased leptin levels and insulin resistance [23], and an experimental study indicated that leptin regulates the development of insulin resistance through its effects on the liver [24]. Elevated serum TG levels may lead to the expansion of adipose tissue, which may further increase serum leptin concentrations. In this study, we found that serum leptin levels were positively correlated with TG concentrations. This finding is consistent with the data of a large population-based study in Caucasian individuals, showing a significant correlation between leptin and TG:0.32 in women (P < 0.001) and 0.28 in men (P < 0.001) [25]. In addition, animal studies have suggested that leptin may influence serum triglyceride levels indirectly [26, 27].
Based on the significant correlation of leptin with BMI, HOMA-IR, TG, and UA, we proposed the predicted formulas for serum leptin levels for each sex, and the adjusted R2 of the formula was 0.552 and 0.447 for men and women, respectively. The multiple linear regression models in our study explained the degree of variance in serum leptin levels, as high as that explained by other models, including percentage body fat (R2 = 0.523 for men; R2 = 0.551 for women) estimated by the bioimpedance method [28] or total abdominal fat (R2 = 0.493 for men) assessed by abdominal CT [29].
To the best of our knowledge, our study is the first to establish sex- and BMI-specific reference intervals for leptin for both sexes in the largest Chinese cohort. In addition, this cohort was a random sampling population instead of the hospital population. A previous Chinese study investigating the reference values of serum leptin in women indicated that the mean ± SD value of serum leptin concentrations was 10.5 ± 1.99 ng/ml [9], which was significantly lower than the serum levels of leptin (20.92 ± 12.96 ng/mL) in women in our study [9]. The lower BMI levels (22.69 ± 3.26 kg/m2) observed in the above study [9] compared to that of our study (24.6 ± 3.5 kg/m2) may account for the variance of leptin concentrations. In addition, we established sex- and BMI-specific reference intervals for serum leptin concentrations in both sexes. A study of the data from the third National Health and Nutrition Examination Survey (NHANES III) showed the serum leptin concentrations by ethnicity and BMI in both genders [18], which had similar levels of leptin in men of all BMI groups (6.0 ± 0.16 ng/mL) as observed in our study. However, the serum leptin levels of all BMIs, < 20, 20 to < 25, 25 to < 27.5, 27.5 to < 30, and > 30 groups in women in our study seemed to be higher than that in the NHANES III study [18]. Another study in multiple ethnicities also found that compared with European women, South Asian women had strikingly high leptin concentrations, which could not be explained by fat distribution and hyperinsulinism [21]. However, there is evidence that hypertrophy of subcutaneous adipocytes may contribute to high leptin concentrations in South Asians [30].
After determining the reference interval of leptin levels, our further analysis showed that, in the normal BMI participants, individuals with leptin levels higher than the 97.5th percentile may have a higher risk of prevalent metabolic syndrome and abdominal obesity. This finding contributes to the clinical application of serum leptin measurement, but future studies with larger sample sizes are needed to support this finding.
The established reference intervals in our study provide reliable evidence for the clinical analysis and understanding of leptin, as well as a theoretical basis for the clinical application of leptin. However, our study had some limitations. First, the reference intervals for serum leptin concentrations can only reflect healthy individuals in the Han population. Second, we did not assess other specific fat distributions, such as skinfold thickness and visceral fat. Third, after excluding the participants who meet the exclusion criteria, there are differences in the number of participants with different age and sex. We excluded the participants with diabetes, so the higher prevalence of diabetes in men than in women may contribute to the differences. Of note, the sample size in our study is larger than previous study [9]. In addition, the median (25th, 75th) of serum leptin absolute levels with different ages are similar (Table 3).
Conclusion
In conclusion, we established sex- and BMI-specific reference intervals for serum leptin concentrations for both sexes in a large Chinese cohort living in Pinggu area and examined the possible factors correlated with leptin.
Availability of data and materials
All data generated or analyzed during this study are included in the article. Further inquiries can be directed to the corresponding author.
Abbreviations
- BMI:
-
Body mass index
- WC:
-
Waist circumference
- HC:
-
Hip circumference
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- FPG:
-
Fasting plasma glucose
- HOMA-IR:
-
Homeostasis model assessment of insulin resistance
- 2 h-PPG:
-
2-Hour postprandial plasma glucose
- HbA1c:
-
Hemoglobin A1c
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- HDL-C:
-
High density lipoprotein cholesterol
- LDL-C:
-
Low density lipoprotein cholesterol
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate aminotransferase
- Cr:
-
Creatinine
- UA:
-
Uric acid
- MetS:
-
Metabolic syndrome
References
Collaboration NCDRF. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet. 2017; 390:2627–2642. https://doi.org/10.1016/S0140-6736(17)32129-3
Zhang Y, Proenca R, Maffei M, et al. Positional cloning of the mouse obese gene and its human homologue. Nature. 1994;372:425–32. https://doi.org/10.1038/372425a0.
Munzberg H, Morrison CD. Structure, production and signaling of leptin. Metabolism. 2015;64:13–23. https://doi.org/10.1016/j.metabol.2014.09.010.
Friedman JM. Leptin and the endocrine control of energy balance. Nat Metab. 2019;1:754–64. https://doi.org/10.1038/s42255-019-0095-y.
Abella V, Scotece M, Conde J, et al. Leptin in the interplay of inflammation, metabolism and immune system disorders. Nat Rev Rheumatol. 2017;13:100–9. https://doi.org/10.1038/nrrheum.2016.209.
Schmidt MI, Duncan BB, Vigo A, et al. Leptin and incident type 2 diabetes: risk or protection? Diabetologia. 2006;49:2086–96. https://doi.org/10.1007/s00125-006-0351-z.
Polyzos SA, Aronis KN, Kountouras J, et al. Circulating leptin in non-alcoholic fatty liver disease: a systematic review and meta-analysis. Diabetologia. 2016;59:30–43. https://doi.org/10.1007/s00125-015-3769-3.
Lieb W, Sullivan LM, Harris TB, et al. Plasma leptin levels and incidence of heart failure, cardiovascular disease, and total mortality in elderly individuals. Diabetes Care. 2009;32:612–6. https://doi.org/10.2337/dc08-1596.
Wu XY, Wu XP, Xie H, et al. Relationship between age-related reference values of serum osteoprotegerin and leptin in native Chinese women and compared with those in women of other races. Clin Chim Acta. 2008;389:72–8. https://doi.org/10.1016/j.cca.2007.11.024.
Wu XY, Wu XP, Luo XH, et al. The relationship between the levels of gonadotropic hormones and OPG, leptin, TGF-beta1 and TGF-beta2 in Chinese adult women. Clin Chim Acta. 2010;411:1296–305. https://doi.org/10.1016/j.cca.2010.05.006.
Considine RV, Sinha MK, Heiman ML, et al. Serum immunoreactive-leptin concentrations in normal-weight and obese humans. N Engl J Med. 1996;334:292–5. https://doi.org/10.1056/NEJM199602013340503.
Zhou X, Li Y, Zhang X, et al. Independent markers of nonalcoholic fatty liver disease in a gentrifying population-based Chinese cohort. Diabetes Metab Res Rev. 2019;35: e3156. https://doi.org/10.1002/dmrr.3156.
Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology. 2012;142:1592–609. https://doi.org/10.1053/j.gastro.2012.04.001.
Matthews DR, Hosker JP, Rudenski AS, et al. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28:412–9. https://doi.org/10.1007/BF00280883.
Alberti KG, Zimmet P, Shaw J, Group IDFETFC. The metabolic syndrome—a new worldwide definition. Lancet. 2005; 366:1059–1062. https://doi.org/10.1016/S0140-6736(05)67402-8
Zimmet P, Hodge A, Nicolson M, et al. Serum leptin concentration, obesity, and insulin resistance in Western Samoans: cross sectional study. BMJ. 1996;313:965–9. https://doi.org/10.1136/bmj.313.7063.965.
Haffner SM, Gingerich RL, Miettinen H, Stern MP. Leptin concentrations in relation to overall adiposity and regional body fat distribution in Mexican Americans. Int J Obes Relat Metab Disord. 1996;20:904–8.
Ruhl CE, Everhart JE. Leptin concentrations in the United States: relations with demographic and anthropometric measures. Am J Clin Nutr. 2001;74:295–301. https://doi.org/10.1093/ajcn/74.3.295.
Luke AH, Rotimi CN, Cooper RS, et al. Leptin and body composition of Nigerians, Jamaicans, and US blacks. Am J Clin Nutr. 1998;67:391–6. https://doi.org/10.1093/ajcn/67.3.391.
Solin MS, Ball MJ, Robertson I, et al. Relationship of serum leptin to total and truncal body fat. Clin Sci (Lond). 1997;93:581–4. https://doi.org/10.1042/cs0930581.
Mente A, Razak F, Blankenberg S, et al. Ethnic variation in adiponectin and leptin levels and their association with adiposity and insulin resistance. Diabetes Care. 2010;33:1629–34. https://doi.org/10.2337/dc09-1392.
Wang X, Jia J, Huang T. Shared genetic architecture and casual relationship between leptin levels and type 2 diabetes: large-scale cross-trait meta-analysis and Mendelian randomization analysis. BMJ Open Diabetes Res Care. 2020. https://doi.org/10.1136/bmjdrc-2019-001140.
Das P, Bhattacharjee D, Bandyopadhyay SK, Bhattacharya G, Singh R. Association of obesity and leptin with insulin resistance in type 2 diabetes mellitus in Indian population. Indian J Physiol Pharmacol. 2013;57:45–50.
Tanida M, Yamamoto N, Morgan DA, et al. Leptin receptor signaling in the hypothalamus regulates hepatic autonomic nerve activity via phosphatidylinositol 3-kinase and AMP-activated protein kinase. J Neurosci. 2015;35:474–84. https://doi.org/10.1523/JNEUROSCI.1828-14.2015.
Ruige JB, Dekker JM, Blum WF, et al. Leptin and variables of body adiposity, energy balance, and insulin resistance in a population-based study. The Hoorn Study. Diabetes Care. 1999;22:1097–104. https://doi.org/10.2337/diacare.22.7.1097.
Shimabukuro M, Koyama K, Chen G, et al. Direct antidiabetic effect of leptin through triglyceride depletion of tissues. Proc Natl Acad Sci U S A. 1997;94:4637–41. https://doi.org/10.1073/pnas.94.9.4637.
Muoio DM, Dohm GL, Fiedorek FT Jr, Tapscott EB, Coleman RA. Leptin directly alters lipid partitioning in skeletal muscle. Diabetes. 1997;46:1360–3. https://doi.org/10.2337/diab.46.8.1360.
Echwald SM, Clausen JO, Hansen T, et al. Analysis of the relationship between fasting serum leptin levels and estimates of beta-cell function and insulin sensitivity in a population sample of 380 healthy young Caucasians. Eur J Endocrinol. 1999;140:180–5. https://doi.org/10.1530/eje.0.1400180.
Ramachandran A, Snehalatha C, Vijay V, et al. Plasma leptin in non-diabetic Asian Indians: association with abdominal adiposity. Diabet Med. 1997;14:937–41. https://doi.org/10.1002/(SICI)1096-9136(199711)14:11%3c937::AID-DIA502%3e3.0.CO;2-S.
Sniderman AD, Bhopal R, Prabhakaran D, Sarrafzadegan N, Tchernof A. Why might South Asians be so susceptible to central obesity and its atherogenic consequences? The adipose tissue overflow hypothesis. Int J Epidemiol. 2007;36:220–5. https://doi.org/10.1093/ije/dyl245.
Acknowledgements
The authors thank all the research staff, physicians and nurses in Peking University People’s Hospital and Capital Medical University Pinggu Teaching Hospital who participated in this work.
Funding
This work was supported by Science and Technology Department of Tibet Autonomous Region (XZ2017ZR-ZYZ151).
Author information
Authors and Affiliations
Contributions
XZ and LJ contributed to the study concept and design. YL, FZ, and XZ contributed to the acquisition of data. JC performed the statistical analysis. JC and YL were involved in interpretation of the data. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the ethics committee of Peking University Medical Center and University of Michigan. Written informed consent was provided by all participants.
Consent for publication
Not applicable.
Competing interests
The authors have no conflicts of interest to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
: Table S1. Correlation between Ln (leptin) and different variables in each gender. Table S2. Clinical characteristics of men with BMI of 20 to <25. Table S3. Clinical characteristics of women with BMI of 20 to <25. Table S4. Clinical characteristics of men with BMI of 20 to <25 by tertiles of leptin levels. Table S5. Clinical characteristics of women with BMI of 20 to <25 by tertiles of leptin levels. Table S6. ROC analysis for determining cut-off point of serum leptin levels (ng/ml) to distinguish the participants with BMI <25 kg/m2 (normal weight) and BMI ≥25 kg/m2 (overweight or obesity).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cheng, J., Luo, Y., Li, Y. et al. Sex- and body mass index-specific reference intervals for serum leptin: a population based study in China. Nutr Metab (Lond) 19, 54 (2022). https://doi.org/10.1186/s12986-022-00689-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12986-022-00689-x