
Abstract
Background
An essential aspect of human well-being is positive sexual health outcomes. However, the issue of adverse sexual health outcomes continues to be a major public health concern, particularly for women with disabilities in sub-Saharan Africa (SSA). Therefore, this current scoping review mapped studies conducted in the last twenty-nine years on the sexual health of women with disabilities from these five dimensions: sexual activity, contraceptive use, sexual autonomy, sexual violence and risky sexual behaviour, whilst seeking to identify the current state of knowledge and address the study gaps in SSA.
Methods
This current scoping review was informed by the methodological framework proposed by Arksey and O’Malley. Exploratory searches were conducted in PubMed, Web of Science, African Journals Online, etc., to identify studies conducted in SSA that focus on sexual activity, contraceptive use, sexual autonomy, sexual violence and risky sexual behaviour among women with disabilities in SSA since the inception of the International Conference on Population and Development in 1994 to 30th of March 2024. This process resulted in the inclusion of seventeen (17) studies.
Results
Of the 1362 identified through various databases, 34 studies were included for the full-text retrieval and screening; only 17 studies met the inclusion criteria. The eligible studies were conducted across six countries in SSA and published between 2008 and 2023. Eight studies used quantitative study type, six utilised qualitative approach, and three employed mixed-methods analysis. Two studies were conducted on sexual activity, ten were conducted on contraceptive use, four were conducted on sexual violence, and one study was conducted on risky sexual behaviour, whilst no study on sexual autonomy met the inclusion criteria.
Conclusion
This review showed that there were few or scarce studies on sexual activity, contraceptive use, sexual autonomy, sexual violence and risky sexual behaviour among women with disabilities in SSA and even where the studies were substantial (contraceptive use), the majority of the studies were conducted in a country. Future studies should consider examining dimensions of sexual health, such as sexual autonomy, sexual activity and risky sexual behaviour of women with disabilities that were not available or were scarce in the literature.
Plain language summary
Sexual health is really important for people's overall well-being, and it includes aspects like how we feel socially, mentally, emotionally, and physically. In sub-Saharan Africa, especially for women with disabilities, sexual health is a big concern. So, this review looked at studies done over the last 29 years about the sexual health of women with disabilities in sub-Saharan Africa. It focused on five areas: sexual activity, contraceptive use, sexual autonomy, sexual violence, and risky sexual behaviour. Databases were searched for relevant studies and found 17 that fit the set criteria. These studies were from six countries in sub-Saharan Africa and were published between 2008 and 2023. Most of the studies were about contraceptive use, with fewer focusing on sexual activity, sexual violence, and risky behaviour. There weren't any eligible studies on sexual autonomy. The review concluded that there's not enough research on these sexual health dimensions among women with disabilities in sub-Saharan Africa, especially on sexual autonomy, and future studies should explore this further.
Similar content being viewed by others


Background
An essential aspect of human well-being is sexual health, which has social, mental, emotional, and physical aspects [1, 2]. The issue of sexual health continues to be a major public health concern, particularly for women with disabilities in sub-Saharan Africa (SSA). Several studies have reported that achieving optimum sexual health and autonomy is often hindered by a myriad of barriers, including societal stigma, discrimination, and systemic neglect [3,4,5]. Women with disabilities still face numerous obstacles that obstruct the improvement of their sexual health despite the increased awareness of the significance of sexual health and rights [6]. It is imperative to comprehend and tackle these obstacles to advance gender parity, social justice, and inclusive growth within the region.
Research and advocacy focused on meeting the needs of women with disabilities globally in terms of their sexual health have gained significant traction in recent years [7, 8]. However, much of this attention has been concentrated in high-income countries, leaving behind the unique experiences and concerns of women with disabilities in SSA [9,10,11,12]. In the studies conducted by Rugoho and Maphose [13] and Ganle et al. [14] argued that the intersectionality of gender and disability compounds the obstacles faced by women in SSA, where patriarchal norms and cultural taboos further restrict their sexual agency and access to essential healthcare services. This oversight is particularly concerning given the intersecting layers of discrimination and marginalisation faced by women with disabilities in this region, including barriers to healthcare access, limited educational opportunities, and entrenched social stigma [15, 16]. Limited research and scarce data exacerbate the invisibility of this issue, hindering efforts to develop targeted interventions and policies that address the specific needs of women with disabilities.
This current scoping review could serve as a crucial starting point for discussions aimed at improving the sexual health of women with disabilities in SSA. Similar studies conducted in Sweden and Australia led to policy roundtable discussions with stakeholders and policymakers. These discussions resulted in the launch of sexual health initiatives that helped bridge gaps in sexual health services and promoted strong community ties and inclusiveness for women with disabilities in those countries [17, 18].
A scoping review offers a comprehensive approach to mapping the existing literature, identifying gaps, and synthesising evidence on a particular topic [19]. This study presents a scoping review of the sexual health of women with disabilities in SSA. By systematically examining the available literature, the research aims to highlight the gaps in knowledge needed to improve the sexual health of these women since the International Conference on Population and Development (ICPD) in Cairo, Egypt, in 1994, which initiated the concept of sexual and reproductive health and rights (SRHR) [20]. This type of review has been used in many latent studies on improving other specific populations’ sexual health and well-being [21, 22].
The study seeks to accomplish these objectives by presenting a thorough synopsis of the current state of research in relation to sexual health dimensions being considered. Moreover, the study aims to identify areas where evidence is limited, highlighting gaps in knowledge that warrant further investigations or examination with the purpose of improving the sexual health outcomes of women with disabilities in SSA whilst appraising the current state of knowledge to ensure that no one is left behind [23]. It's also pertinent to know that many international agendas, goals and targets might remain unachievable or challenging if the adverse sexual health of women with disabilities is not adequately addressed [24,25,26].
The study will review and consider a range of sexual health research dimensions that determine the sexual health outcomes of women with disabilities in SSA through sexual activity, sexual autonomy, contraception use, risky sexual behaviour and sexual violence. Through a comprehensive examination of the existing literature, this scoping review seeks to contribute to a deeper understanding of the sexual health current and future research needs for women with disabilities in SSA.
By highlighting neglected gaps and areas that require further investigation, this scoping review aims to catalyse efforts towards the development of inclusive and rights-based approaches to sexual health for all women, regardless of disability status and ultimately achieving sustainable development goals targets 3.7 and 5.6, which, respectively aim to ensure universal access to sexual and reproductive health care services and to achieve gender equality and empower all women and girls [24]. Therefore, the research question for this review is: What is the volume and coverage of current studies on improving the sexual health of women with disabilities in SSA, including aspects such as sexual activity, contraceptive use, sexual autonomy, sexual violence, and risky sexual behaviour?
Methods
Our scoping review design was guided by the methodological frameworks proposed by Arksey and O’Malley [27]. The two objectives of conducting a scoping review, as outlined by Arksey and O’Malley [27], were achieved by providing a comprehensive summary of existing research on sexual health with a focus on sexual health operationalised from the dimensions of sexual activity, contraceptive use, sexual autonomy, sexual violence and risky sexual behaviour of women with disabilities in SSA also by identifying any gaps present in the current literature. A protocol to guide the scoping review process was developed using the format prescribed by the International Prospective Register of Systematic Reviews (PROSPERO) [28]. However, we did not register the protocol due to PROSPERO's current exclusion of scoping review protocols for registration. We report the process and findings of the scoping review in accordance with the established Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines [29].
Literature search strategy
Before conducting the full searches for this scoping review, we conducted a preliminary exploratory search of the literature on improving the sexual health of women with disabilities with a focus on sexual activity, contraceptive use, sexual autonomy, sexual violence and risky sexual behaviour in SSA. Searches were performed in Cochrane Library and Joanna Briggs Institute (JBI) databases. Our search revealed that no reviews of this nature had been previously conducted nor were ongoing. However, JBI and Cochrane Library were not considered in the final databases considered. Additionally, exploratory searches were conducted on two general social and behavioural science databases, PubMed and Web of Science, to ensure a comprehensive search. The exploratory review also informed the development of the keyword list for our search strategy, helped refine the research question, and aided in the development of inclusion criteria. More information about the development of the keyword list is available in supplementary appendix I.
We conducted the search using all identified Medical Subject Headings (MeSH) terms found during the exploratory search (Supplementary appendix II). To ensure the inclusion of all relevant studies, particularly those published in African journals, we searched a variety of databases, including PubMed, Web of Science, African Journals Online, JSTOR, and PsycInfo. Additionally, we searched non-database websites such as Google Scholar and Guttmacher to complement or identify any missing study from those included in the databases. Finally, we examined the reference lists of all review studies identified in the search to identify additional relevant literature/eligible study.
Inclusion and exclusion criteria
Population
We included studies conducted among women with any form of disability between the ages of 15 and above. This limits the review to studies conducted on sexual health with a focus on sexual activity, contraceptive use, sexual autonomy, sexual violence and risky sexual behaviour among women with disabilities. We excluded studies that exclusively focus on young girls with disability and studies that compared women with disabilities with women without disability. We excluded studies focusing solely on young girls with disabilities to maintain the focus on adult women. Additionally, studies comparing women with disabilities to those without were excluded to avoid comparative bias and concentrate on the unique challenges faced by women aged 15–49 with disabilities. This ensures a clearer understanding of their specific sexual health needs.
Concept
Studies that discussed or assessed sexual health dimensions such as sexual activity, contraceptive use, sexual autonomy, sexual violence and risky sexual behaviour [30, 31] were included in this study, whilst other studies without the stated focus were excluded. The definition of sexual health dimensions considered are in Table 1 below;
Context
This scoping review covers studies conducted in SSA from January 1st 1995 to 30th March 2024. The 1995 start date was selected as it coincides with the ICPD held in Cairo, Egypt, in September 1994, which marked the inception of the doctrine of SRHR [20].
Types of studies
The study types included in this review were qualitative, quantitative, and mixed-methods. Only peer-reviewed studies published in English with the listed study types were considered. Technical reports, thesis, research protocols, book reviews, quasi-experiments, randomised control trials, conference proceedings, commentaries, blog posts and other kinds of grey were excluded. This approach helps maintain a high standard of evidence quality and relevance, focusing on established findings rather than preliminary or non-peer-reviewed work [27].
Eligible studies selection process
We employed EndNote X9 (Clarivate), a citation manager, to remove duplicate search results. Subsequently, we utilised the online systematic review software Covidence to conduct screening and data extraction for the remaining search results [32]. Two reviewers independently evaluated each search result. Initially, all titles and abstracts were screened for relevance. Following this, the full texts of all pertinent results were assessed against the inclusion and exclusion criteria. Disagreements at each stage were resolved through discussion until a consensus was reached. In cases where agreement could not be reached, a third reviewer (an independent reviewer) facilitated resolution. This process resulted in the inclusion of 17 studies.
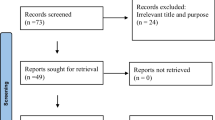
The elimination stages, the number of results eliminated at each stage, and the reasons for exclusion using the PRISMA flow diagram were displayed in Fig. 1 [29].

PRISMA 2020 Flow diagram [33]
Data extraction and charting
The included eligible articles were extracted independently from covidence using a standardised form in Microsoft Excel. Specifically, the following information was extracted: the first author's surname and year of publication, study country, and sexual health dimensions, including sexual activity, contraceptive use, sexual autonomy, sexual violence and risky sexual behaviour. Two authors conducted the data extraction, and the full information for all articles included in the review is available in Table 2.
Results
The initial search conducted by the authors had 1362 studies, and 1241 duplicates were removed as duplicates. One hundred twenty-one (121) were included for title and abstract sifting, and 87 studies were removed. Thirty-four studies (34) were included for the full-text retrieval and screening, and only 17 studies were included as eligible studies, whilst 17 studies were excluded due to not meeting the inclusion criteria (Fig. 1).
Geographical locations covered
The seventeen (17) included studies were conducted across 6 countries in SSA and published between 2008 and 2023. Eight out of the eligible studies were conducted in Ethiopia [34,35,36,37,38,39,40,41], three from South Africa [42,43,44], two from Uganda [45, 46], two from Ghana [47, 48] and one each from Kenya [49] and Malawi [50] (Table 2; Fig. 2).

Geographical distribution of studies included
Study type
Out of the seventeen eligible studies, 47% (8) were conducted using a quantitative study type, 35% utilised a qualitative approach, and 18% employed mixed-methods analysis. All the included studies focused on the sexual health dimensions of sexual activity, contraceptive use, sexual autonomy, sexual violence and risky sexual behaviour among women with disabilities in SSA (Fig. 3).

Study types of the eligible studies included
Sexual health focus and countries conducted across sub-Saharan Africa
The results on the sexual health focus show that two studies were conducted on sexual activity [42, 44], ten studies were conducted on contraceptive use [34,35,36,37,38,39,40, 45, 48, 49], none was found on sexual autonomy, four studies were conducted on sexual violence [41, 43, 47, 50] whilst one study was conducted on risky sexual behaviour [50] (Table 2).
Country and sexual health focus mix
Figure 4 shows the country mix and sexual health focus among women with disabilities in SSA. The graph shows that seven studies conducted in Ethiopia were on contraceptive use, whilst one study was conducted on sexual violence. Out of three studies conducted in South Africa, two were on sexual activity, whilst one was on sexual violence; in the same vein, the two studies conducted in Uganda were on contraceptive use and risky sexual behaviour. Ghana had two studies, one on contraceptive use and the other on sexual violence, whilst Malawi and Kenya had one study each, and the studies were on sexual violence and contraceptive use, respectively.

Sexual health focus across the eligible studies countries
Main findings from the sexual health dimensions included in the study.
Sexual activity
The findings on the eligible included studies suggest that disability stigma may hinder the attainment of normative womanhood and sexual relationships among women with disabilities in South Africa [44], while the persistent gap in access to prevention and treatment for people with disabilities highlights sexual abuse and exploitation as substantial threats to HIV/AIDS prevention efforts within this population [42].
Contraceptive use
In Ethiopia, the unmet need for family planning among women with disabilities stands at 24.3% [34]. Only 18% of women have ever used modern contraceptives, with a prevalence rate of 20.2% among currently married women [35]. Family planning utilisation among reproductive-age women with disabilities was 33.7% [36], and among women aged 35 and above, the rate was 27.2%, with injectable contraceptives being the most commonly used method (93.2%) [37]. High awareness of family planning methods was noted at 97.2%, but comprehensive knowledge was low at 32.5% in Ethiopia and Ghana [38, 48]. In rural Ethiopia, the overall unmet need for family planning was 24.08%, with 14.79% for spacing and 9.29% for limiting purposes [39]. In Uganda, 26.1% of women have utilised contraception, with increased uptake linked to access to health facilities and family planning information broadcast on the radio [45]. In Kajiado County, Kenya, 32.0% of women with disabilities use family planning, and 61.2% have negative attitudes towards it, which significantly affects utilisation rates [49]. Among reproductive-age women with disabilities in Ethiopia, 27.3% were current contraceptive users, with 48.5% preferring implants [40].
Several factors influence contraceptive use among women with disabilities. These include age, education level, desired number of children, employment status, and marital status. Attitudes towards family planning also play a significant role, particularly in Kenya, where negative perceptions were prevalent [49]. Access to health facilities and information dissemination, such as radio broadcasts in Uganda, was also crucial for increasing contraceptive uptake [45].
A qualitative response from one of the respondents in a study conducted by Nketsia et al. [48] stated, “I wish healthcare workers were more patient. I often experience misunderstandings when discussing modern contraceptive issues because they don't know sign language, which is our main form of communication”.
Sexual violence
In South Africa, learners with intellectual disabilities face school-based sexual violence, with frequent occurrences of inappropriate touching, threats, and intimidation [43]. In Ghana, women with disabilities experience a high prevalence of sexual violence, influenced by factors such as poverty, family rejection, isolation, and unemployment, which lead to unwanted pregnancies, divorce, rejection, and psychological trauma [47]. In Malawi, although none of the informants reported childhood sexual abuse, many women described experiencing sexual abuse in adulthood, often involving men who pretended to want to "marry" them but abandoned them once they became pregnant [50]. In Ethiopia, a notably high prevalence of sexual violence was reported among reproductive-age females with disabilities, at 59.8% [41].
Several factors contribute to the risk of sexual violence among women with disabilities. Demographic factors such as urban residence and specific age groups (25–34 and 35–49 years old) increase vulnerability, as seen in Ethiopia [41]. A lack of sexual information and specific disabilities, such as hearing impairments, further elevate the risk. In Malawi, societal attitudes and deceptive behaviours by men exacerbate the issue, leading to psychological trauma and social stigma for the affected women [50].
Risky sexual behaviour and sexual autonomy
The main key finding highlights was that risky sexual behaviour was prevalent among women with disabilities and often associated with HIV/AIDS, unwanted pregnancies due to sexual encounters with strangers [46]. Only a study was identified on sexual behaviour whilst no study was found for sexual autonomy based on this study’s selection criteria.
Discussion
To the best of our knowledge, this is the first scoping review conducted with the aim of understanding the research gap in improving the sexual health outcomes of women with disabilities in SSA with a focus on the following key dimensions of sexual health such as sexual activity, contraceptive use, sexual autonomy, sexual violence and risky sexual behaviour. This current scoping review provides a comprehensive summary of existing research and identifies areas that require further research in improving the sexual health of this population within SSA.
The distribution of previous research conducted across the included five dimensions of sexual health appears to be scanty among women with disabilities in SSA except for contraceptive use, in which case was majorly conducted in Ethiopia [34,35,36,37,38,39,40]. The review was unable to map any study on the sexual autonomy of women with disabilities in SSA, whilst few studies were conducted on sexual activity and risky sexual behaviour [42, 44, 46].
For sexual activity among women with disabilities in SSA, this current review found that disability stigma threatens normative womanhood and also that there were higher risk of sexual exploitations [44]. These findings align with a study conducted by Hubbard et al. [51], which concluded that there were higher sexual exploitations among women who were vulnerable compared to those who were not. This finding highlights the significant need for sex education programmes specifically targeting women with disabilities in SSA. These programmes should be customised for this group, as studies have shown that tailored sexual education empowers women with disabilities to make informed decisions, including choices about sexual activity [52, 53].
Regarding contraceptive use, the findings of this review show an unmet need for contraception among women with disabilities in SSA. These findings align with other studies conducted outside Africa regions, which ascertained that family planning services were less accessible to women with disabilities [54, 55]. The possible reasons for this may be due to lack of awareness or knowledge-gap and also limited access to disability-friendly services. The implication of this could result in women with disabilities facing increased chances of experiencing unwanted pregnancies and related adverse reproductive health outcomes [22]. Therefore, to ensure that the contraceptive needs of women with disabilities in SSA are met, it is crucial to draw the attention of key stakeholders and policymakers to the creation of awareness programmes targeting this population [56].
Furthermore, it is essential to provide accurate and timely information and to ensure that contraceptive services are accessible and disability-friendly. This approach aligns with the United Nations' principle of 'leaving no one behind' by promoting inclusivity [57,58,59]. If the use of contraceptives is low or not improved among this group, this may have a serious impact on the sexual and reproductive health of these women, which could lead to poor health outcomes [56].
The findings on sexual violence in this review revealed that women with disabilities were at risk of sexual violence in SSA. This is also in line with emerging studies that have documented that people with disabilities were at an increased risk of sexual violence [60, 61]. In the same vein, findings have also confirmed that women with a disability were at greater risk of experiencing rape than women without a disability [62, 63]. It has also been noted that suboptimal empowerment could also lead women with a disability to be more likely than women without a disability to report experiencing rape and sexual coercion, among other sexual abuses [64, 65]. Therefore, by understanding that women with disabilities are at greater risk of experiencing sexual violence, there is a need to take deliberate actions to stop the violence through targeted empowerment activities for this key population. In the same vein, there is a dire need to ensure self-protection skills such as consent to sex or sexual autonomy and also to develop a conducive environment and various channels for reporting sexual violence [64, 65].
Furthermore, the present study reveals a high prevalence of risky sexual behaviour among women with disabilities, correlating significantly with HIV/AIDS, unwanted pregnancies due to sexual encounters with strangers [46]. These findings align with previous findings on people with disabilities, which reported an elevated level of sexual risk-taking and its adverse sexual health outcomes [66]. It has been noted that this specific population group face significant barriers to sexual health education and services, which could mitigate these risks and improve overall sexual health outcomes [11].
Lastly, this study's findings were unable to map any study on sexual autonomy among women with disabilities in SSA based on the study’s inclusion and exclusion criteria. However, results from the studies conducted in other regions have indicated little or no sexual autonomy among women with disabilities, with emphasis on being surveilled or controlled by either their partner or family members to be involved in sexual acts [9, 10].
In general, the results of this review indicate the need for designing well-informed educational programmes that are need-based, which could influence behavioural change communication strategies to promote contraceptive use and sexual autonomy and prevent sexual violence and risky sexual behaviour among women with disabilities in SSA. The results reported in this study need to be taken seriously to improve the sexual health of women with disabilities and avert the consequence of adverse health outcomes [11, 17, 56, 57].
Limitations of the study
Our scoping review on improving sexual health outcomes among women with disabilities in SSA faces several limitations. Firstly, we excluded non-English language articles and grey literature, potentially missing valuable research and introducing bias. Secondly, the narrative synthesis approach was without meta-analysis, which prevented us from providing pooled prevalence rates of the sexual health dimensions considered in this study, affecting the precision of our conclusions. Also, the study heterogeneity in definitions, measurements, and populations may complicate comparisons and generalisability. Finally, potential publication bias and missing data may skew our findings. Future studies should aim to address and overcome these limitations.
Implications for research and policy
Our findings indicate a significant need for sexual empowerment programmes and targeted interventions to improve access to contraceptive services, increase sexual autonomy and prevent sexual violence and risky sexual behaviour among women with disabilities in SSA. Policies should ensure the provision of disability-friendly sexual health services and educational programmes tailored to women with disabilities are prioritised in SSA. Additionally, stakeholders and policymakers must ensure timely awareness campaigns and support systems for these women to enhance their sexual health and uphold the principle of inclusivity by ensuring that healthcare systems adapt to offer accessible and inclusive sexual health services, ensuring women with disabilities can effectively communicate their needs. This could close the adverse sexual health outcomes gaps among this population through well-informed policies and evidence-based strategies that are crucial to improving the sexual and reproductive health outcomes for women with disabilities in SSA.
Conclusion and recommendations for future research
This review showed that there were few or scarce studies on sexual activity, contraceptive use, sexual autonomy, sexual violence and risky sexual behaviour among women with disabilities in SSA and even where the studies were substantial (contraceptive use), the majority of the studies were conducted in Ethiopia. Furthermore, this current review shows that women with disabilities were less likely to use contraceptives and were at risk of sexual violence. Therefore, there is a need to pool all relevant stakeholders from the government, communities, and development partners to deliberately coin policies and programmes that empower access to contraceptives and prevent sexual violence among women with disabilities. Moreover, further studies should be conducted to explore the needs of women with disabilities regarding contraceptive use and also their perspectives regarding preventing and reporting sexual violence. In the same vein, future studies should consider examining other dimensions of sexual health, such as sexual autonomy, sexual activity and risky sexual behaviour of women with disabilities that were not available or were scarce in the literature.
Availability of data and materials
All data generated and analysed during this study are included in this manuscript as supplementary information.
Abbreviations
- SSA:
-
Sub-Saharan Africa
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PROSPERO:
-
International Prospective Register of Systematic Reviews
- MeSH:
-
Medical Subject Headings
- ICPD:
-
International Conference on Population and Development
- SRHR:
-
Sexual and reproductive health and rights
- MESH:
-
Medical Subject Headings
References
Mitchell KR, Lewis R, O’Sullivan LF, Fortenberry JD. What is sexual wellbeing and why does it matter for public health? The Lancet Public Health. 2021;6:e608–13.
Sexual Health. https://www.who.int/health-topics/sexual-health#tab=tab_1.
Schalet AT, Santelli JS, Russell ST, Halpern CT, Miller SA, Pickering SS, Goldberg SK, Hoenig JM. Invited commentary: broadening the evidence for adolescent sexual and reproductive health and education in the United States, vol. 43. NewYork: Springer; 2014. p. 1595–610.
Starrs AM, Ezeh AC, Barker G, Basu A, Bertrand JT, Blum R, Coll-Seck AM, Grover A, Laski L, Roa M. Accelerate progress—sexual and reproductive health and rights for all: report of the Guttmacher-Lancet Commission. The Lancet. 2018;391:2642–92.
Janighorban M, Boroumandfar Z, Pourkazemi R, Mostafavi F. Barriers to vulnerable adolescent girls’ access to sexual and reproductive health. BMC Public Health. 2022;22:2212.
Lottes IL. Sexual rights: meanings, controversies, and sexual health promotion. J Sex Res. 2013;50:367–91.
Sands T. A voice of our own: advocacy by women with disability in Australia and the Pacific. Gend Dev. 2005;13:51–62.
Good G, Hollis-English A, Attwell A, Dickson A, Gibbs A, Gordon J, Taylor J. Social-model mothers: disability, advocacy, and activism. Counterfutures. 2017;4:107–35.
Björnsdóttir K, Stefánsdóttir Á, Stefánsdóttir GV. People with intellectual disabilities negotiate autonomy, gender and sexuality. Sex Disabil. 2017;35:295–311.
Morales E, Gauthier V, Edwards G, Courtois F. Women with disabilities’ perceptions of sexuality, sexual abuse and masturbation. Sex Disabil. 2016;34:303–14.
Treacy AC, Taylor SS, Abernathy TV. Sexual health education for individuals with disabilities: a call to action. Am J Sexual Educ. 2018;13:65–93.
Kim EJ, Parish SL, Skinner T. The impact of gender and disability on the economic well-being of disabled women in the United Kingdom: a longitudinal study between 2009 and 2014. Soc Policy Admin. 2019;53:1064–80.
Rugoho T, Maphosa F. Challenges faced by women with disabilities in accessing sexual and reproductive health in Zimbabwe: the case of Chitungwiza town. Afr J Disabil. 2017;6:1–8.
Ganle JK, Baatiema L, Quansah R, Danso-Appiah A. Barriers facing persons with disability in accessing sexual and reproductive health services in sub-Saharan Africa: a systematic review. PLoS ONE. 2020;15: e0238585.
Matin BK, Williamson HJ, Karyani AK, Rezaei S, Soofi M, Soltani S. Barriers in access to healthcare for women with disabilities: a systematic review in qualitative studies. BMC Womens Health. 2021;21:1–23.
Chan XW, Hutchings K. Inequalities, barriers, intersectionality, and facilitators of careers of women with disabilities: themes and future research agenda from a scoping review. Front Psychol. 2023;14:1104784.
Löfgren-Mårtenson L. “I want to do it right!” A pilot study of Swedish sex education and young people with intellectual disabilities. Sex Disabil. 2012;30:209–25.
Inquiry talks about sexual expression in NDIS plans. https://www.sbs.com.au/news/podcast-episode/inquiry-talks-about-sexual-expression-in-ndis-plans/26o3vhepb.
Munn Z, Peters MD, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18:1–7.
Hempel M. Reproductive health and rights: origins of and challenges to the ICPD agenda. Health Transit Rev. 1996;6:73–85.
Moncayo-Quevedo JE, Pérez-Arizabaleta MDM, Rodríguez-Ortiz AR, Villegas-Trujillo LM. A contextualization of transgender women and condom use using the HIV syndemic framework: scoping review. Int J Sexual Health 2024:1–15.
Bolarinwa OA, Boikhutso T. Mapping evidence on predictors of adverse sexual and reproductive health outcomes among young women in South Africa: a scoping review. Afr J Primary Health Care Family Med. 2021; 13.
WHO. Joint United Nations statement on ending discrimination in health care settings. World Health Organization; 2017.
UN. Transforming our world: the 2030 Agenda for Sustainable Development. UN Doc A/RES/70/1 (September 25, 2015) 2015.
Convention on the Rights of Persons with Disabilities (CRPD). https://social.desa.un.org/issues/disability/crpd/convention-on-the-rights-of-persons-with-disabilities-crpd.
Cohen SA, Richards CL. The Cairo consensus: population, development and women. Fam Plann Perspect. 1994;26:272–7.
Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8:19–32.
Protocol registration. https://www.crd.york.ac.uk/prospero/.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10:1–11.
Giami A. Sexual health: the emergence, development, and diversity of a concept. Annu Rev Sex Res. 2002;13:1–35.
WHO. Developing sexual health programmes: a framework for action. World Health Organization; 2010.
Kellermeyer L, Harnke B, Knight S. Covidence and rayyan. J Med Lib Assoc JMLA. 2018;106:580.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372: n71.
Tessema AL, Bishaw MA, Bunare TS. Assessment of the magnitude and associated factors of unmet need for family planning among women of reproductive age group with disabilities in Bahir Dar City, Amhara Region, North West Ethiopia. Open J Epidemiol. 2015;5:51–8.
Beyene GA, Munea AM, Fekadu GA. Modern contraceptive use and associated factors among women with disabilities in Gondar City, Amhara Region, north west Ethiopia: a cross sectional study. Afr J Reprod Health. 2019;23:101–9.
Mesfin Yesgat Y, Gebremeskel F, Estifanous W, Gizachew Y, Jemal S, Atnafu N, Nuriye K. Utilization of family planning methods and associated factors among reproductive-age women with disability in Arba Minch Town, Southern Ethiopia. Open Access J Contracep. 2020;11:25–32.
Tsegay K, Gebremariam H, Haile F. Modern contraceptive methods utilization and associated factors among women with disabilities in Mekelle Town, Tigray, Ethiopia. Int J Pharm Biol Sci Fundam. 2017;13:1–8.
Yimer AS, Modiba LM. Modern contraceptive methods knowledge and practice among blind and deaf women in Ethiopia. A cross-sectional survey. BMC Women’s Health. 2019;19:1–13.
Alem AZ, Agegnehu CD. Magnitude and associated factors of unmet need for family planning among rural women in Ethiopia: a multilevel cross-sectional analysis. BMJ Open. 2021;11: e044060.
Tenaw Z, Gari T, Gebretsadik A. Contraceptive use among reproductive-age females with disabilities in central Sidama National Regional State, Ethiopia: a multilevel analysis. PeerJ. 2023;11: e15354.
Tenaw Z, Gari T, Gebretsadik A. Sexual violence and associated factors among reproductive-age females with disabilities in central Sidama National Regional State, Ethiopia: a multilevel analysis. BMC Womens Health. 2023;23:353.
Hanass-Hancock J. Interweaving conceptualizations of gender and disability in the context of vulnerability to HIV/AIDS in KwaZulu-Natal. S Afr Sexual Disabil. 2009;27:35–47.
Phasha TN, Nyokangi D. School-based sexual violence among female learners with mild intellectual disability in South Africa. Viol Against Women. 2012;18:309–21.
Van der Heijden I, Harries J, Abrahams N. In pursuit of intimacy: disability stigma, womanhood and intimate partnerships in South Africa. Cult Health Sex. 2019;21:338–51.
Ayiga N, Kigozi S. Access to and uptake of contraception by women with disabilities. J Soc Sci. 2016;12:171.
Birungi C, Ssebunnya J, Kiwanuka N, Nakasujja N, Kinyanda E. Factors contributing to vulnerability to risky sexual behaviour in severe mental illness in the Ugandan socio-cultural context. 2023.
Opoku MP, Huyser N, Mprah WK, Badu E, Alupo BA. Sexual violence against women with disabilities in Ghana: accounts of women with disabilities from Ashanti Region. Disabil CBR Inclusive Dev. 2016;27:91.
Nketsia W, Mprah WK, Opoku MP, Juventus D, Amponteng M. Achieving universal reproductive health coverage for deaf women in Ghana: an explanatory study of knowledge of contraceptive methods, pregnancy and safe abortion practices. BMC Health Serv Res. 2022;22:954.
Makau PM, Keraka MN, Kieru JN, Matoke VO, Geoffery O. Attitude towards utilization of family planning services among women of reproductive age living with disability in Kajiado County, Kenya. Int J Community Med Public Heal. 2021;8:3793.
Kvam MH, Braathen SH. “I thought… maybe this is my chance” sexual abuse against girls and women with disabilities in Malawi. Sexual Abuse. 2008;20:5–24.
Hubbard P, Scoular J. Making the vulnerable more vulnerable? The contradictions of British street prostitution policy. In: Safer sex in the city. London: Routledge; 2016. p. 135–54.
Ballan MS, Freyer MB. The sexuality of young women with intellectual and developmental disabilities: a neglected focus in the American foster care system. Disabil Health J. 2017;10:371–5.
Bruder C, Kroese B. The efficacy of interventions designed to prevent and protect people with intellectual disabilities from sexual abuse: a review of the literature. J Adult Protect. 2005;7:13–27.
Beyene GA, Abebe SM, Fekadu GA, Muche AA, Geremew BM. Contraceptive dynamics among women with disabilities in low-and middle-income countries: a scoping review protocol. Syst Rev. 2023;12:40.
Casebolt MT, Singh K, Speizer IS, Halpern CT. Use of modern contraceptives by women with disabilities in Rajasthan, India: an analysis of the annual health survey. Sexual Reprod Healthc. 2022;31: 100699.
Bolarinwa OA, Odimegwu C, Okeke SR, Ajayi KV, Sah RK. Barriers and facilitators to accessing and using sexual and reproductive health services during the COVID-19 pandemic outbreak in Africa: a protocol for a systematic review and meta-analysis. BMJ Open. 2023;13: e071753.
Bolarinwa OA, Odimegwu C, Adebisi YA. Leaving no one behind: addressing the sexuality of people with disabilities. Int J Equity Health. 2024;23:129.
Vision AC. Getting specific to leave no one behind on sustainable development. Leave no one behind: time for specifics on the sustainable development goals. 2019:1.
World Health Organization. Health in 2015: from MDGs, millennium development goals to SDGs, sustainable development goals. 2015.
Byrne G. Prevalence and psychological sequelae of sexual abuse among individuals with an intellectual disability: a review of the recent literature. J Intellect Disabil. 2018;22:294–310.
Stobbe KJ, Scheffers M, van Busschbach JT, Didden R. Prevention and intervention programs targeting sexual abuse in individuals with mild intellectual disability: a systematic review. J Mental Health Res Intellect Disabil. 2021;14:135–58.
Nannini A. Sexual assault patterns among women with and without disabilities seeking survivor services. Womens Health Issues. 2006;16:372–9.
Basile KC, Breiding MJ, Smith SG. Disability and risk of recent sexual violence in the United States. Am J Public Health. 2016;106:928–33.
Tang CS-K, Lee YK-S. Knowledge on sexual abuse and self-protection skills: a study on female Chinese adolescents with mild mental retardation. Child Abuse Neglect. 1999;23:269–79.
Liou W-Y. An illustrated scale measuring the sexual-abuse prevention knowledge of female high school students with intellectual disabilities in Taiwan. Sex Disabil. 2014;32:135–51.
Magaya L. Predictors of sexual risk behavior among Zimbabwean adolescents with and without disabilities: implications for HIV/AIDS prevention. Southern Illinois University at Carbondale. 2004.
Acknowledgements
Not applicable.
Funding
This study received no specific funding support.
Author information
Authors and Affiliations
Contributions
OAB and CO conceived and designed the study. OAB drafted the manuscript, conducted the methodology, and performed the narrative synthesis for the review. TT and OAB wrote the discussion and conclusion sections, whilst CO supervised the overall study development and critically reviewed the manuscript for methodological and intellectual content. All authors read and approved the final version of the manuscript before submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bolarinwa, O.A., Odimegwu, C. & Tapera, T. Improving the sexual health of women with disabilities in sub-Saharan Africa: a scoping review of published studies. Reprod Health 21, 116 (2024). https://doi.org/10.1186/s12978-024-01859-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12978-024-01859-1