
Abstract
Background
Unintended pregnancies can adversely affect maternal health, preventable through timely postpartum contraception. During the COVID-19 pandemic, family planning services were constrained by policies that curtailed outpatient visits. We investigated the prevalence of postpartum contraceptive initiation at King Chulalongkorn Memorial Hospital (KCMH) during January to June 2020, comparing with the same period in 2019, and identified factors associated with such initiation.
Methods
We reviewed the medical records of 4506 postpartum women who delivered at KCMH during the study period. Logistic regression was conducted to test the association between early COVID-19 phase deliveries and post-partum long acting reversible contraception (LARC) initiation including copper intrauterine devices, levonorgestrel intrauterine systems, contraceptive implants, and progestogen-only injectable contraceptives.
Results
A total of 3765 women (83.6%), of whom 1821 delivered during the pandemic and 1944 during the historical cohort period, were included in this study. The proportion of women who initiated non-permanent modern contraceptives at six weeks postpartum was comparable between the COVID-19 (73.4%) and historical cohort (75.3%) (p = 0.27) periods. The proportion of women who initiated LARC at six weeks postpartumwas comparable between the historical cohort period (22.5%) and the COVID-19 (19.7%) (p = 0.05) period. Accessing a six-week postpartum check-up was independently associated with LARC initiation, of which the adjusted odds ratio (OR) (95% confidence interval) was 3.01 (2.26 to 4.02).
Conclusions
Our findings demonstrated that accessing postpartum care significantly associate with the use of LARC. The data suggest the strong influence of postpartum check-ups in facilitating the adoption of effective contraception, emphasizing the need for accessible postpartum care to sustain maternal health during health crises.
Plain language summary
In this study, we looked at how often new mothers used birth control methods after giving birth during the COVID-19 pandemic in Thailand. We also wanted to find the factors that influenced their decision to use birth control. We reviewed the medical records of 4,506 women who had recently given birth at King Chulalongkorn Memorial Hospital. Out of these, 3,765 women were included in the study. Some gave birth during the pandemic, and others gave birth before the pandemic. We found that a similar number of women started using birth control about six weeks after giving birth, whether it was during the pandemic or before it. However, slightly fewer women chose very effective methods of birth control during the pandemic compared to before it. One important factor we found was that women who went for a check-up six weeks after giving birth were more likely to use highly effective birth control. This means that getting regular check-ups after childbirth can help women make better choices about birth control. In summary, our study showed that receiving postpartum care is closely linked to using LARC. This underlines how important it is for new mothers to have their check-ups after giving birth, to help them start using effective birth control if they choose.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
Global health crises have profound impacts on healthcare systems by disrupting access to essential services including sexual and reproductive healthcare [1]. These disruptions are particularly significant during the postpartum period, a time when high motivation for contraceptive initiation was reported [2, 3]. The early phase of the COVID-19 pandemic saw an unprecedented a strain on healthcare resources, leading to a significant reduction in non-urgent care like postpartum follow-up. This was a critical time for postpartum women, who often rely on these appointments to initiate contraception [4]. This can lead to an increase in unintended and closely spaced pregnancies, which can negatively impact maternal physical and mental health [5,6,7]. The situation in Thailand during the COVID-19 pandemic mirrors the global trends, with significant increases in calls to the unintended pregnancy hotline, reflecting the challenges in accessing family planning services during the pandemic [8].
The importance of timely contraceptive initiation is underscored by the World Health Organization (WHO)’s recommendation for a two-year interval between pregnancies, as shorter intervals may pose adverse effects on maternal health [9]. The National Institute for Health and Care Excellence (NICE) guidelines categorize long-acting reversible contraception (LARCs) as critical during this period for their effectiveness and low discontinuation rates. This category includes copper intrauterine devices (IUDs), levonorgestrel intrauterine systems (LNG-IUS), contraceptive implants, and progestogen-only injectable contraceptives, all of which necessitate intervention by a healthcare provider for initiation [10, 11].
Initiating LARCs during the immediate postpartum period, before hospital discharge, can mitigate the barriers to accessing postpartum care, as women are already in a medical facility [12]. Despite the safety and efficacy of immediate postpartum contraception and recommended by medical society, in addition to female sterilization this approach has not gained much popularity in Thailand [12,13,14]. Thus, this study was conducted to determine the prevalence of immediate postpartum contraceptive initiation and during postpartum check-up amidst the COVID-19 pandemic in Thailand. We also sought to identify the factors associated with LARC initiation during this period. The findings are crucial in ensuring uninterrupted access to contraceptive services during pandemics and other healthcare system challenges. This may inform the policymakers and program implementers on how to maintain essential reproductive health services even in times of crisis.
Methods
Study design and population
This time series study was approved by the Institutional Review Board of the Faculty of Medicine, Chulalongkorn University (IRB No. 794/63). The study was conducted in accordance with the Declaration of Helsinki. We reviewed the electronic medical records of 4506 postpartum women who delivered at KCMH during the COVID-19 period (January 1 to June 30, 2020) and the historical cohort period (January 1 to June 30, 2019). January was selected as the initiation time point because, in Thailand, the first cases of COVID-19 were officially reported in this month [15]. Historical control of the same period was used because we aimed to mitigate the seasonality trend [16]. We excluded those who delivered before 22 weeks, underwent cesarean hysterectomy, or could not be contacted by telephone. To confirm the accuracy of data entry, electronic medical records were reviewed by two investigators (LS and SS). For women who did not return for a six-week postpartum visit at KCMH, an experienced family planning nurse conducted a five-minute telephonic interview. We repeated the phone call a maximum of five times. Informed consent was obtained from all eligible women before conducting the telephone interview.
Measurements
Study data were collected and managed using REDCap electronic data capture tools hosted at KCMH [17]. The demographic information included age, ethnicity, marital status, address, and reimbursement. Obstetric characteristics included gravidity, number of living children, number of antenatal care (ANC) visits, pre-pregnancy body mass index (BMI), underlying medical conditions, obstetric complications, route of delivery, gestational age at delivery, birth weight, and APGAR score at 1 and 5 min. Data regarding immediate postpartum contraceptive initiation were gathered from the discharge summary, while data regarding six-week postpartum contraceptive initiation, among those who returned for postpartum visits at KCMH, were obtained from the electronic medical records of the family planning and reproductive health clinic. We confirmed the type of contraceptive initiation based on the prescription history. The primary outcome variable, contraceptive method use at six weeks postpartum, was defined as method initiation. The following methods are considered non-permanent modern contraceptives: combined oral contraceptive pills (COCs), combined hormonal contraceptive patch, depot medroxyprogesterone acetate (DMPA), progestin-only pills (POPs), contraceptive implant(s), copper IUD, LNG-IUS, and male condoms [18]. We interviewed participants to determine whether they were using any of the following in addition to the aforementioned methods: withdrawal method, lactation amenorrhea, or fertility awareness. For those who were using more than one method simultaneously, contraceptives that provided better efficacy were considered at the participants’ discretion [18]. Immediate postpartum contraceptive initiation was defined as contraceptive initiation either after delivery or before discharge from the postpartum hospital stay [12]. LARC was defined according to NICE guidelines [10].
Study setting
At KCMH, we provide comprehensive contraceptive counseling to all postpartum women during the immediate postpartum period. Our facility offers an extensive range of immediate postpartum contraception options, including POPs, DMPA, contraceptive implant, IUDs. During the COVID-19 period, this approach has been emphasized. All medically eligible contraceptives were initiated upon request before hospital discharge. At the six-week postpartum visit, all women underwent a standardized contraceptive assessment by family planning nurses. All participants were educated with up-to-date evidence-based and precise information on each contraceptive method, its effectiveness, the risk of side effects, and tips on adherence. The women then selected their contraceptive method, which was provided by the family planning facility. During the historical cohort period, six-week postpartum visits at KCMH were scheduled for all women. However, during the COVID-19 period, only those with obstetric complications or medical diseases were scheduled to return for postpartum visits to KCMH. Others were asked to visit a nearby clinic or hospital for postpartum visits. In Thailand, COCs, POPs, and combined hormonal contraceptive patches are available over the counter, which women can access without a prescription.
Statistical analysis
Statistical analyses were performed using SPSS version 22 (IBM Corp., Armonk, NY, USA) and STATA version 17 (StataCorp. 2021. Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC.). Quantitative variables with a normal distribution were characterized using mean values and standard deviations (SDs), whereas those with a non-normal distribution were presented using medians and interquartile ranges (IQR). Qualitative variables were characterized by the number and percentage of participants in each category. Fisher’s exact test was used to test the association between the qualitative variables. Univariable logistic regression was conducted to test the association between delivery during the early phase of COVID-19 and the six-week post-partum LARC initiation. A backward logistic regression model was used to control for the potential confounders. The results were presented as odds ratios (OR) and 95% confidence intervals (CI). We tested the interaction between the COVID-19 period and follow-up at a family planning clinic to identify the association between these two variables and LARC initiation. The multicollinearity of the final model was tested using the variance inflation factor (VIF).
Results
Population
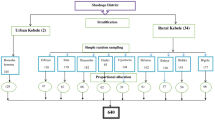
A total of 3765 among 4506 women (83.6%), of whom 1821 delivered during the COVID-19 pandemic and 1944 during the historical cohort period, were included in this study (Fig. 1). The sociodemographic characteristics of the participants are presented in Table 1. Mean (SD) age between the COVID-19 and the historical cohort groups were comparable at 31.7 (5.5) and 31.0 (5.9) years, respectively. Almost all women (96.9%) were Thai. Most of them (69.8%) were married. The majority (46.7%) were primiparas after delivery of the most recent pregnancy. Approximately 35% of pre-pregnancy BMIs were in the range of overweight/obesity [19], of which the mean (SD) total weight gain was 13.3 (5.0) kg. Mean (SD) of total weight gain between the COVID-19 and the historical cohort groups were comparable at 13.2 (4.8) and 13.5 (5.1) kg, respectively. Around 5% developed preeclampsia during recent gestation, and approximately 9% had gestational diabetes. Approximately half delivered by cesarean section, and the majority (70%) delivered term newborns.

Study flow aElectronic medical record. b King Chulalongkorn Memorial Hospital
Outcome data
During the COVID-19 period, the prevalence of immediate contraceptive use was 379/1821 (20.9%), and in the historical cohort period, 368/1944 (18.9%), (p = 0.05). Postpartum female sterilization was the most commonly selected method, with 17.0% and 17.9% in the COVID-19 and historical periods, respectively. The use of contraceptive implants was comparable between the COVID-19 (2.1%) and historical cohort periods (2.3%), as shown in Table 2. Excluding those who underwent postpartum female sterilization, the proportion of women who initiated non-permanent modern contraceptives at six weeks postpartum was comparable between the COVID-19 (73.4%, 1094/1490) and historical cohort periods (75.3%, 1217/1618) (p = 0.27), as shown in Table 3. The most commonly initiated method was male condoms in the COVID-19 (23.5%, 350/1490) and historical cohort periods (23.0%, 372/1618), followed by COCs in the COVID-19 (20.7%, 308/1490) and historical cohort periods (22.2%, 359/1618). The proportion of women who did not use contraception was comparable (22.6% and 21.9% during the COVID-19 and historical periods, respectively). The proportion of women who initiated LARC, were comparable between the historical cohort period (22.5%, 364/1618) and the COVID-19 period (19.7%, 293/1490) (p = 0.05).
Univariable analysis showed that the COVID-19 period tended to be associated with lower odds of initiating LARC compared to the historical cohort period, in which the OR (95% CI) was 0.83 (0.70−1.01), as shown in Table 4. This association was attenuated and did not reach statistical significance in the multivariable model, in which the adjusted OR (95% CI) was 0.92 (0.76−1.11). Postpartum follow-up at the family planning clinic was associated with higher odds of initiating LARC in the univariable model, in which the OR (95% CI) was 3.58 (2.82−4.54). This association was not attenuated in the multivariable model, in which the adjusted OR (95% CI) was 3.94 (2.96−5.23). We performed an additional analysis, including six-week postpartum visits outside our institution. The univariable analysis showed a smaller effect size, in which the OR (95% CI) was 2.48 (1.95−3.15). This association was not attenuated in the multivariate model, in which the adjusted OR (95% CI) was 3.01 (2.26−4.02). We tested the interaction between the COVID-19 and historical cohort periods and the six-week postpartum visit with LARC initiation but did not find a significant effect. Other sociodemographic and obstetric characteristics associated with higher odds of initiating LARC in the multivariable model were age < 35 years, having more than one child, having never attended antenatal care, and having delivered vaginally. These potential confounders were used to adjust the final multivariable model to test the association between the COVID-19 and historical cohort periods and six-week postpartum follow-up visits with LARC initiation. The VIF tests did not show multicollinearity among the adjusted variables in the final model.
Discussion
The prevalence of immediate postpartum contraceptive initiation at the KCMH was comparable between the COVID-19 and the historical cohort periods. In addition to postpartum female sterilization, very few women initiated contraceptive use despite the recommendation of the medical societies about the efficacy and safety of these methods [12]. In our setting, the comprehensive contraceptive counseling is routinely provided in the postpartum ward and most women are eligible for the government’s LARC reimbursement benefits. This contrast points to the existence of barriers beyond the upfront payments for LARC. Further exploration into the clinician-patient discussion could provide additional insights on this issue. The lack of emphasis or detailed discussion by healthcare providers on the importance, efficacy, and safety of immediate postpartum contraceptive methods may be a significant barrier [20, 21]. The potential reasons for this gap in communication may include time constraints during consultation, clinicians’ perceptions or biases towards certain contraceptives, or possibly a lack of updated training regarding postpartum contraceptive options.
The six-week postpartum non-permanent modern contraceptive prevalence was comparable between the COVID-19 and historical cohort period, which differs from other settings [22,23,24]. This finding is notable because it contrasts with publications from other settings where the use of modern contraceptives decreased globally during the COVID-19 crisis, including in Asian countries [22,23,24,25]. Our study highlights a unique aspect of Thailand, where COCs, the preferred choice for contraception here, can be bought without a prescription [26]. The variation in study settings may explain the differences in our results compared to others.
Multivariable logistic regression analysis showed that the opportunity to return for postpartum visits influenced the use of LARC. Postpartum visits allows women to initiate LARC, a cost-saving strategy for preventing unintended pregnancy [27]. During the pandemic, in resource-limited settings, the demand for healthcare access increased, affecting non-urgent care, such as postpartum visits [28, 29]. LARC initiation immediately after giving birth is another strategy to ensure the prevention of the rising rate of unintended pregnancy during the pandemic [30].
The sociodemographic factor associated with LARC initiation was age. The increased odds of LARC use by younger women of reproductive age (< 24 years) may reflect the efforts to prioritize adolescents in pregnancy prevention programs in Thailand. According to the Act for Prevention and Solution of the Adolescent Pregnancy Problem, B.E. 2559, the government launched a policy to increase access by providing free LARC to 10 to 20-year-old women. Additionally, LARC can be initiated without a guardian’s consent [31]. This policy underscores the emphasis on reducing adolescent pregnancies by increasing contraceptive access among this age group. Older adolescents and young adults, particularly those in their early twenties, face different challenges and influences regarding contraceptive use. Being a university student or transitioning into higher education or the workforce can greatly impact their contraceptive needs, influencing behavior differently than younger adolescents targeted by current policies. The association between age and the unmet need for contraception is complex and depends on the demographic and societal context. For example, a study conducted among Guineans found a higher prevalence of unmet need for contraceptives among adolescents compared to young women as young women are more likely to live in union and may desire to have children while adolescents may face stigma of using contraceptive services outside their marriage [32]. Recognizing and addressing the unique needs of these age groups can enhance the effectiveness of reproductive health policies and better support individual’s needs.
An increasing number of children was associated with higher odds of LARC initiation. This association is consistent with that reported by Branum et al. [33]. Women with higher parity are usually more motivated to prevent further pregnancies. Postpartum women who had never come for antenatal care visits had higher odds of using LARC. This reflects our institute’s policy of providing special care to vulnerable groups at risk of further unintended pregnancy. Postpartum women who delivered vaginally had higher odds of using LARC than those who had cesarean sections. This discrepancy may be explained due to the exclusion of individuals who underwent postpartum tubal sterilization, a procedure commonly performed alongside cesarean deliveries [14].
The strengths of this analysis include analyzing a large dataset, considering numerous potential confounders for postpartum contraceptive use, and employing logistic regression to adjust for these confounders. Sensitivity and seasonal variation analyses ensured the reliability of the data regarding contraceptive use, particularly the initiation LARCs, which was verified through electronic medical records and prescription data. Nonprescription method assessments and telephonic interviews were conducted by an experienced family planning nurse. Another strength is that the KCMH is a tertiary care facility that can provide almost every modern contraceptive and provide same-visit contraceptive initiation for all requested methods. This contributes to an unbiased estimate owing to the availability of the methods.
However, this study had several limitations, including its quantitative nature that overlooks the qualitative reasons behind contraceptive choices and the lack of consideration for partners’ opinions. The reliance on electronic medical records, which may not be comprehensive, could introduce bias, although this is mitigated by cross-referencing with prescription records. The study’s single-center design and focus on the early COVID-19 phase in Thailand limit its generalizability and relevance to other pandemic peaks. Further research should focus on contraceptive prevalence during each peak of the pandemic periods, as well as the efficacy of employing telemedicine as an adjunctive tool to encourage postpartum contraceptive initiation, as this has been widely used in Thailand since the peak of the pandemic [34]. Furthermore, investigating the interval between postpartum delivery and follow-up visits for initiating contraception presents another valuable research avenue. This exploration could shed light on how this timing affects postpartum mothers’ contraceptive choices and outcomes.
Conclusion
Our findings demonstrated the six-week postpartum visit was a significant factor in initiating LARC, providing an opportunity for women to access clinician-initiated contraceptive methods. The findings underscore the vital importance of postpartum check-ups in enabling the uptake of effective contraception, highlighting the urgent need for accessible postpartum care to ensure the continuation of maternal health services during health crises.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author (SS2) upon reasonable request.
Abbreviations
- KCMH:
-
King Chulalongkorn Memorial Hospital
- NICE:
-
National Institute for Health and Care Excellence
- Copper IUD:
-
copper intrauterine devices
- LNG-IUS:
-
levonorgestrel intrauterine system
- LARC:
-
long-acting reversible contraceptive
- ANC:
-
antenatal care
- BMI:
-
body mass index
- COCs:
-
combined oral contraceptive pills
- DMPA:
-
depot medroxyprogesterone acetate
- POPs:
-
progestin-only pills
- SDs:
-
standard deviations
- OR:
-
odds ratios
- CI:
-
confidence intervals
- VIF:
-
variance inflation factor
References
Azmat SK, Ali M, Siddiqui FJ, Tirmizi SFA, Kiarie J. Scoping review on the Impact of Outbreaks on Sexual and Reproductive Health Services: proposed frameworks for Pre-, Intra-, and Postoutbreak situations. Biomed Res Int. 2021;2021:9989478. https://doi.org/10.1155/2021/9989478. PMID: 34541003; PMCID: PMC8443356.
Loewenberg Weisband Y, Keder LM, Keim SA, Gallo MF. Postpartum intentions on contraception use and method choice among breastfeeding women attending a university hospital in Ohio: a cross-sectional study. Reprod Health. 2017;14(1):45. https://doi.org/10.1186/s12978-017-0307-4. PMID: 28320478; PMCID: PMC5360022.
Taub RL, Jensen JT. Advances in contraception: new options for postpartum women. Expert Opin Pharmacother. 2017;18(7):677–88. https://doi.org/10.1080/14656566.2017.1316370. Epub 2017 Apr 17. PMID: 28375776.
Semaan A, Dey T, Kikula A, Asefa A, Delvaux T, Langlois EV, van den Akker T, Benova L. Separated during the first hours-postnatal care for women and newborns during the COVID-19 pandemic: a mixed-methods cross-sectional study from a global online survey of maternal and newborn healthcare providers. PLOS Glob Public Health. 2022;2(4):e0000214. https://doi.org/10.1371/journal.pgph.0000214. PMID: 36962168; PMCID: PMC10022345.
Sökmen Y, Kaya Odabaş R, Bal Şaraldı H, Taşpınar A. The frequency of unplanned pregnancies during the COVID-19 pandemic and the factors affecting the situation. J Obstet Gynaecol. 2022;42(8):3621–7. Epub 2022 Nov 17. PMID: 36394223.
Rezaei F, Amiri-Farahani L, Haghani S, Pezaro S, Behmanesh F. The impact of the COVID-19 pandemic on contraceptive methods, abortion, and unintended pregnancy: a cross-sectional study. BMC Womens Health. 2023;23(1):357. https://doi.org/10.1186/s12905-023-02512-y. PMID: 37403093; PMCID: PMC10318765.
Berthelot N, Lemieux R, Garon-Bissonnette J, Drouin-Maziade C, Martel É, Maziade M. Uptrend in distress and psychiatric symptomatology in pregnant women during the coronavirus disease 2019 pandemic. Acta Obstet Gynecol Scand. 2020;99(7):848–55. https://doi.org/10.1111/aogs.13925. Epub 2020 Jun 3. PMID: 32449178.
Hfocus.org [Internet]. Bangkok: The rising of unintended pregnancy in Thailand during the Covid-19 pandemic; 2021 [cited 2023 May 25]. https://www.hfocus.org/content/2021/06/22005.
World Health Organization. Report of a WHO Technical Consultation on Birth Spacing: Geneva, Switzerland 13–15 June 2005 (No. WHO/RHR/07.1). Geneva: World Health Organization; 2007. https://www.who.int/publications/i/item/WHO-RHR-07.1. Accessed 25 May 2023.
Long-acting reversible contraception. London, National Institute for Health and Care Excellence (NICE). : 2019 Jul. (NICE Clinical Guidelines, No. 30.) https://www.nice.org.uk/guidance/cg30.
Jaisamrarn U, Santipap M, Santibenchakul S. Discontinuation rates of different contraceptive methods in Thai women up to 1-year after method initiation. Sci Rep. 2021;11(1):10819. https://doi.org/10.1038/s41598-021-90373-6. PMID: 34031521; PMCID: PMC8144200.
American College of Obstetricians and Gynecologists’ Committee on Obstetric Practice. Committee Opinion No. 670: Immediate Postpartum Long-Acting Reversible Contraception. Obstet Gynecol. 2016;128(2):e32–7. https://doi.org/10.1097/AOG.0000000000001587. PMID: 27454734.
Sothornwit J, Kaewrudee S, Lumbiganon P, Pattanittum P, Averbach SH. Immediate versus delayed postpartum insertion of contraceptive implant and IUD for contraception. Cochrane Database Syst Rev. 2022;10(10):CD011913. https://doi.org/10.1002/14651858.CD011913.pub3. PMID: 36302159; PMCID: PMC9612833.
Uaamnuichai S, Phutrakool P, Thammasitchai N, Sathitloetsakun S, Santibenchakul S, Jaisamrarn U. Does socioeconomic factors and healthcare coverage affect postpartum sterilization uptake in an urban, tertiary hospital? Reprod Health. 2023;20(1):23. https://doi.org/10.1186/s12978-023-01572-5. PMID: 36707807; PMCID: PMC9881507.
Coronavirus cases in Thailand [Internet]. Delaware: Worldometer.info [cited 2023 May 25]. https://www.worldometers.info/coronavirus/country/thailand/.
Franklin TE, Theisen G, Salyer CV, Pinkston C, Gunaratnam B. The seasonality of abortion in Kentucky. Contraception. 2017;95(2):181–5. https://doi.org/10.1016/j.contraception.2016.08.019. Epub 2016 Sep 1. PMID: 27593333.
Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O’Neal L, McLeod L, Delacqua G, Delacqua F, Kirby J, Duda SN, REDCap Consortium. The REDCap consortium: building an international community of software platform partners. J Biomed Inf. 2019;95:103208. https://doi.org/10.1016/j.jbi.2019.103208. Epub 2019 May 9. PMID: 31078660; PMCID: PMC7254481.
Taylor HS, Pal L, Seli E. Family planning, sterilization, and abortion. In: Seli E, editor. Speroff’s clinical gynecologic endocrinology and infertility. 9th ed. Philadelphia: Lippincott Williams & Wilkins (LWW); 2020.
WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–63. https://doi.org/10.1016/S0140-6736(03)15268-3. Erratum in: Lancet. 2004 Mar 13;363(9412):902. PMID: 14726171.
Santibenchakul S, Tschann M, Carlson ADP, L Hurwitz E, Salcedo J. Promotion of Long-Acting Reversible Contraception among adolescents and Young adults. J Midwifery Womens Health. 2019;64(2):194–200. https://doi.org/10.1111/jmwh.12934. Epub 2018 Dec 20. PMID: 30570219; PMCID: PMC6438728.
Oduyebo T, Zapata LB, Boutot ME, Tepper NK, Curtis KM, D’Angelo DV, Marchbanks PA, Whiteman MK. Factors associated with postpartum use of long-acting reversible contraception. Am J Obstet Gynecol. 2019;221(1):43.e1-43.e11. https://doi.org/10.1016/j.ajog.2019.03.005. Epub 2019 Mar 15. PMID: 30885772; PMCID: PMC6592782.
Miller HE, Henkel A, Leonard SA, Miller SE, Tran L, Bianco K, Shaw KA. The impact of the COVID-19 pandemic on postpartum contraception planning. Am J Obstet Gynecol MFM. 2021;3(5):100412. https://doi.org/10.1016/j.ajogmf.2021.100412. Epub 2021 May 28. PMID: 34058421; PMCID: PMC8161810.
Sakowicz A, Matovina CN, Imeroni SK, Daiter M, Barry O, Grobman WA, Miller ES. The association between the COVID-19 pandemic and postpartum care provision. Am J Obstet Gynecol MFM. 2021;3(6):100460. https://doi.org/10.1016/j.ajogmf.2021.100460. Epub 2021 Aug 14. PMID: 34403823; PMCID: PMC8364402.
Walker SH. Effect of the COVID-19 pandemic on contraceptive prescribing in general practice: a retrospective analysis of English prescribing data between 2019 and 2020. Contracept Reprod Med. 2022;7(1):3. https://doi.org/10.1186/s40834-022-00169-w. PMID: 35287763; PMCID: PMC8918589.
Dasgupta A, Kantorová V, Ueffing P. The impact of the COVID-19 crisis on meeting needs for family planning: a global scenario by contraceptive methods used. Gates Open Res. 2020;4:102. https://doi.org/10.12688/gatesopenres.13148.2. PMID: 33330836; PMCID: PMC7720714.
National Statistical Office of Thailand [Internet]. Thailand multiple indicator cluster survey 2019, survey findings report [cited 2023 May 25]. Bangkok: National Statistical Office of Thailand. https://www.unicef.org/thailand/reports/thailand-multiple-indicator-cluster-survey-2019.
Madden T, Barker AR, Huntzberry K, Secura GM, Peipert JF, McBride TD. Medicaid savings from the Contraceptive CHOICE Project: a cost-savings analysis. Am J Obstet Gynecol. 2018;219(6):595. https://doi.org/10.1016/j.ajog.2018.08.043. e1-595.e11. Epub 2018 Sep 5. PMID: 30194049; PMCID: PMC6741429.
Bayrampour H, Tsui MYE. Postpartum people’s experiences of and responses to the COVID-19 pandemic during the first year of the pandemic: A descriptive qualitative study. Womens Health (Lond). 2023;19:17455057231157480. https://doi.org/10.1177/17455057231157480. PMID: 36846969; PMCID: PMC9971703.
Ombere SO. Access to Maternal Health Services during the COVID-19 pandemic: experiences of Indigent Mothers and Health Care Providers in Kilifi County, Kenya. Front Sociol. 2021;6:613042. https://doi.org/10.3389/fsoc.2021.613042. PMID: 33898553; PMCID: PMC8058360.
Chin E, Leung K, Moore Simas TA, Kumaraswami T. Changes in postpartum contraception utilization rates during the early stage of the COVID-19 pandemic. Womens Health (Lond). 2023;19:17455057231175312. https://doi.org/10.1177/17455057231175311. PMID: 37334467; PMCID: PMC10277878.
ACT for prevention and solution of the adolescent pregnancy problem, B.E. 2559. (2016) [cited 2023 May 25]. https://www.mol.go.th/wp-content/uploads/sites/2/2021/02/ACT-FOR-PREVENTION-AND-SOLUTION-OF.pdf.
Sidibé S, Grovogui FM, Kourouma K, Kolié D, Camara BS, Delamou A, Kouanda S. Unmet need for contraception and its associated factors among adolescent and young women in Guinea: a multilevel analysis of the 2018 demographic and health surveys. Front Glob Womens Health. 2022;3:932997. https://doi.org/10.3389/fgwh.2022.932997. PMID: 36467288; PMCID: PMC9712725.
Branum AM, Jones J. Trends in long-acting reversible contraception use among U.S. women aged 15–44. NCHS Data Brief. 2015;(188):1–8. PMID: 25714042.
Sothornwit J, Kaewrudee S, Somboonporn W, Seanbon O, Ngamjarus C. Implementing the individualized postpartum care with telemedicine during the COVID-19 pandemic at tertiary hospital in Thailand. Heliyon. 2023;9(5):e16242. https://doi.org/10.1016/j.heliyon.2023.e16242.
Acknowledgements
We acknowledge the contribution and cooperation of The Family Planning Research Team: Ms. Nitada Thaiyanant, Ms. Rachanee Wongwathanavikrom, Ms. Kangsadal Amatayakul, Ms. Chalalai Thamprawat, Ms. Sasithorn Thongin, and Ms. Nantana Thongrod, and all nurses and staff at the Family Planning and Reproductive Health Clinic, King Chulalongkorn Memorial Hospital. We also thank Dr. Yuda Chongpison at the Biostatistics Excellence Center, Research Affairs, Faculty of Medicine, Chulalongkorn University, for her statistical advice. We would like to thank Editage (http://www.editage.com) for editing and reviewing this manuscript for language. We extend our thanks to ChatGPT by OpenAI for its grammar assistance. We confirm that, despite this help, all work and final revisions were carried out independently.
Funding
This study was supported by the Family Planning and Reproductive Health Unit, Department of Obstetrics and Gynecology, Faculty of Medicine, Chulalongkorn University.
Author information
Authors and Affiliations
Contributions
SS1 (Sarochinee Sathitloetsakun): literature review, study concept design, data acquisition, statistical analysis, primary manuscript drafting PP1 (Phanupong Phutrakool): statistical analysis DM: study concept design SS2 (Somsook Santibenchakul): study concept design, data acquisition, manuscript editing, and revision for intellectual content UJ: study concept design PP1 (Pimpitcha Puangsricharoen): primary manuscript drafting, editing, and revision for intellectual content.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written Consent for Medical Record Review: For the initial retrospective cross-sectional study that involved the review of medical records, written informed consent was obtained from all participants during their admission to the hospital, as per standard institutional protocol. The ethics committee approved this form of written consent.
Verbal Consent for Phone Interviews: For the missing information that could not be retrieved from the medical records, we conducted brief phone interviews. Verbal informed consent was obtained at the beginning of the phone call. During the call, the participants were informed about the purpose of the study, the nature of the information we were seeking, and how the data would be used and protected. Participants were explicitly asked for their permission to include their information in the study.
Documentation and Witnessing: This verbal consent was documented in the research logs, specifying the date and time of the phone call and summarizing the elements of informed consent that were communicated. The phone interviews were conducted by the trained research assistant who was briefed on ethical considerations, and the procedure was witnessed by another member of the research team.
Ethics Committee Approval: This method of verbal consent for the phone interviews was approved by the Institutional Review Board of the Faculty of Medicine, Chulalongkorn University (IRB No. 794/63), and a waiver was granted for the necessity of written consent for this specific aspect of the study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sathitloetsakun, S., Phutrakool, P., Maitreechit, D. et al. The prevalence of contraceptive use among postpartum women and its associated factors during the early phase of COVID-19 outbreak: a time series study. Reprod Health 21, 80 (2024). https://doi.org/10.1186/s12978-024-01803-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12978-024-01803-3