
Abstract
Background
Globally, there are 42 million women and girls estimated to be forcibly displaced. Adolescent girls and young women in humanitarian settings have their sexual and reproductive health (SRH) neglected. This systematic review aimed to describe SRH obstacles that adolescent girls and young women (10–24 years old) face in humanitarian settings in line with the Sustainable Development Goals.
Methods
We conducted a mixed-methods systematic review in six databases, focusing on migrant women ages 10 – 24and their SRH outcomes. The mixed-methods appraisal tool was used to evaluate the quality of the studies. This review follows PRISMA and the Systematic Review Guidelines from the Centre for Reviews and Dissemination recommendations.
Results
Among the 1290 studies screened by abstracts, 32 met the eligibility criteria: 15 were qualitative, 10 were quantitative and seven were mixed-methods studies. Most studies were performed in the last four years, in African countries. They discussed the increased frequency of adolescent pregnancies (16–23%), lack of contraceptive use and access (8–32%), poor menstrual hygiene management (lack of water, shortage of menstrual hygiene supplies), ignorance and stigma about sexually transmitted infections and HIV, a higher number of child, early and forced marriage or partnership and sexual and gender-based violence, challenging to obtain SRH information/knowledge/access, and unmet SRH needs.
Conclusion
Migration is a current issue. Although there is a growing number of studies on adolescent girls and young women’s SRH in humanitarian settings, this population remains overlooked, and face several challenges in SRH. There is a need for targeting interventions on SRH.
Plain language summary
This systematic review describes the available evidence on the sexual and reproductive health (SRH) challenges faced by adolescent girls and young women in humanitarian settings. Thirty-two studies were analyzed, demonstrating poor SRH outcomes: higher incidence of adolescent pregnancy, lack of access to contraceptives and low rates of its use, precarious menstrual hygiene management (MHM), ignorance and stigma about sexually transmitted infections (STIs) and HIV, higher rates of child, early and forced marriage or partnership (CEFMP) and sexual and gender-based violence (SGBV). Identifying these challenges can help humanitarian actors address the SRH needs of these populations.
Similar content being viewed by others


Background
In 2022, the United Nations High Commissioner for Refugees (UNHCR) estimated that 100 million people were forcibly displaced worldwide due to conflict, violence, and weather-related events such as floods, storms, and cyclones [1]. The Internal Displacement Monitoring Center (IDMC) reported that nearly 42 million of the displaced people were women and girls, 65% from African and Middle Eastern countries. [2].
The Sustainable Development Goals (SDGs) aim to reduce maternal mortality (Goal 3.1), ensure universal access to sexual and reproductive health services (Goal 3.7), end all forms of violence against all women and girls (Goal 5.2), and end child marriage (Goal 5.3) by 2030 [3]. These targets are interlinked and have an impact in the sexual and reproductive health (SRH).
Despite of the SDGs, sexual and reproductive health needs for migrant adolescent girls and young women (10–24 years old) in humanitarian settings remain unmet [4].Studies have described the lack of access and inequalities regarding SRH for migrant adolescent girls and young women (AGYW), including language barriers, difficulties in obtaining contraceptives, fees, waiting times, travel distances, and the insufficiency of specific programs for this population [4,5,6,7,8]. They have higher rates of repeated and unsafe abortions, lower antenatal care (ANC) attendance, more postpartum complications such as perinatal mortality, fetal death and stillbirth, and a higher risk of HIV and sexual violence [7,8,9]. Approximately 60% of maternal deaths or childbirth among adolescent girls occur in conflict or disaster contexts [9].
The discussion of SRH needs for AGYW in humanitarian settings has gained global attention in recent years, however there are gaps in the collection and systematization of comprehensive data, making their use in policy design and implementation in these scenarios challenging and further away from the SDGs [10].
This systematic review aims to explore the current qualitative and quantitative research landscape on SRH issues of adolescent girls and young women displaced by humanitarian crises living in fragile settings in line with the SDGs, given the amount of recent new studies.
Methods
Search strategy and study design
This mixed-methods systematic review was conducted according to Sandelowski et al. [11] and followed the three steps: segregated (qualitative and quantitative studies were analyzed separately), integrated (the differences between qualitative and quantitative studies were minimized), and contingent (addressing the same research questions).
We followed the reporting guidelines described in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and the Systematic Review Guidelines from the Centre for Reviews and Dissemination [12, 13]. For the studies’ evaluation, we used the “Additional file 1: Mixed Methods Appraisal Tool (MMAT) version 2018” [14].
The MMAT includes research evaluative criteria for quantitative, qualitative, and mixed-method studies. This tool was first published in 2009 and revised and upgraded in 2018 [15,16,17]. A user manual with an algorithm guides the studies' analyses. [15].
This review is registered in the PROSPERO platform under the registration number CRD42023403907.
Our research question was "What is the available evidence on sexual and reproductive health among migrant girls and young women in humanitarian settings?"
The search strategy (Additional file 1: Annex S1) was built with the guidance of an information specialist. The chosen research terms and their variations, including Medical Subject Headings (MeSH)[18], were combined according to each database's requirements and specifications.
The databases used for searching were PUBMED, PUBMED PMC, EMBASE, BVS / LILACS, SCOPUS, and WEB OF SCIENCE. The syntax was: "adolescent", "reproductive health", and "refugees"; related words such as plurals and alternative forms of the terms (e.g., youth) were also included. A detailed search strategy is available in Additional file 1: Annex S1.
Eligibility criteria
Original quantitative and qualitative studies which investigated sexual and reproductive health outcomes from the perspective of migrant (defined as displaced women such as refugees, asylum seekers or internally displaced people) adolescent girls and young women (10–24 years old), published until January 05, 2023 (with no lower range), written in English, Spanish or French, were included.
Exclusion criteria
Editorials, opinion articles, letter to editors, call for action, short reports, brief communications, protocol guidelines, book chapters, retrospective studies, congress annals, newsletters, and other reviews were excluded. The research team opted not to consider grey literature.
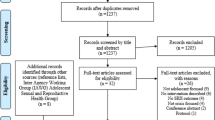
Figure 1 shows the process of the review according to the PRISMA guidelines [13].

PRISMA 2020 flow diagram: process of the integrative review
Critical appraisal
The search fields were title and abstract. The Rayyan Systematic Review Tool [19] was initially used to screen abstracts and titles.
Two independent reviewers performed the initial blind screening and selection of studies, considering the title and abstract. The study coordinator approached conflicts of selection and made the final decision of inclusion or exclusion among conflicting evaluations.
The full texts were read assessing quality and appropriateness.
To evaluate the quality of the included studies, the “Mixed Methods Appraisal Tool (MMAT) version 2018” [17] was used. The MMAT user manual instructs to provide the analysis with a detailed presentation of each one of the five core criteria, according to the study category [15].
The latest MMAT version, 2018, (Additional file 2: Annex S2) includes two screening questions and a total of 25 criteria, divided into five methodological categories of study designs: (a) qualitative, (b) randomized controlled trials, (c) nonrandomized, (d) quantitative descriptive studies and (e) mixed methods. For each category, there are five core criteria rated in three response options: "yes" (the criterion is met), "no" (the criterion is not met) or "can’t tell" (there is not enough information in the paper to evaluate if the criterion is met or not). Mixed-method studies must be assessed in both, qualitative and quantitative categories and then reevaluated into the integration of quantitative and qualitative studies. [15, 17].
Data extraction and analysis
Data from all included articles were extracted following the headlines: authors and title, year, study setting, sample size, study population, age of participants, main objectives, study design and conclusions/recommendations (Table 1). Each study was evaluated under its methodological categories. As each category has five items, we considered 20% for each, scoring 100%. Mixed-methods studies were evaluated as mixed-method, and qualitative and quantitative components were independently assessed on their corresponding quality criteria. All articles were given a final quality score, all articles analysed were included in the study (Table 2).
Results
The results were analyzed using a narrative approach and thematic analysis of the original quotations [20, 21]. Disagreements were resolved through discussion until a consensus was reached. After reviewing all of the literature, seven categories emerged [52]: adolescent pregnancy, contraceptive use and access, menstrual hygiene management (MHM), sexually transmitted infections (STI) and HIV, SRH information/knowledge/access, overview of the main SRH needs, other issues related to SRH (sexual and gender-based violence and child, early and forced marriage or partnership).
Overview of the studies
Among 1290 studies screened by abstracts, 32 met the eligibility criteria; 15 were qualitative studies [22,23,24,25,26,27,28,29,30,31,32,33,34,35,36], 10 were quantitative [6, 37,38,39,40,41,42,43,44,45] and seven were mixed-methods studies [46,47,48,49,50,51,52]. The PRISMA flowchart of included studies is shown in Fig. 1.
More than 50% [6, 9, 22,23,24, 26, 27, 29, 31,32,33,34,35,36,37,38,39, 41,42,43,44, 46, 49,50,51,52], 12 studies were published between 2017 and 2020 [21, 25, 26, 28, 32, 35, 36, 38, 39, 38,39,40,41,42,43,44,45,46,47], one was published in 2013 [30] and two in 2010 [44, 48].
There were 20 studies with female participants only [9, 22,23,24,25,26, 29, 30, 33,34,35,36, 38, 40,41,42,43, 49, 50], and 12 studies with female and male participants [22, 25, 28,29,30, 32, 40, 46, 48, 50]. Parents, non-governmental organizations workers, and health workers were interviewed regarding their opinion of the AGYW's SRH issues. [22, 30, 33, 36, 48, 52].
Most of the studies were performed in African countries: nine in Uganda [32, 35, 37, 40,41,42, 47, 48, 52], four in Nigeria [26, 43, 49, 50], two in Ethiopia [30, 31], one in Egypt [33], one in Ghana [38], and one in Rwanda [29]. The remainder were: three studies were from Thailand [22, 25, 46], three from Lebanon [23, 24, 36], one from Iraq [45], two from Bangladesh [51, 52], one from Jordan [34], two from Brazil [6, 44], one from Australia [27] and one study was performed in two different countries (Thailand and Ethiopia) [39].
Adolescent pregnancy
Four studies reported specifically on adolescent pregnancy: two of them were quantitative [31, 42], and the other two were qualitative [22, 27].
The studies were conducted with refugee AGYW in refugee camps or informal settlements on the Thailand-Myanmar border [22], Uganda [42], Southwest Ethiopia [31], and Australia [27]. The overall prevalence of pregnancy among AGYW was 16% for the study conducted in Australia [27], 21.7% in Uganda [42] and 23% in Ethiopia [31], and more than 50% had no formal or primary education [22, 31, 42]. In the qualitative studies [22, 27], all AGYW students dropped out of school after becoming pregnant. Access to and utilization of maternal health services by pregnant AGYW were not investigated in any of these studies.
The two qualitative studies [21, 30] interviewed specific pregnant women. Asnong et al. (two refugee camps in Thailand-Myanmar border) [21] reported three adolescents and young women were forced to marry after getting pregnant, and only two pregnant young women over 20 said they stopped contraception intending to get pregnant. In both qualitative studies, all the adolescents quit school: some were too ashamed to continue studying, others were expelled because of pregnancy, and others due to motherhood responsibilities.
The adolescents also complained about social isolation due to the burden of taking care of a child and doing all of the housework.
The two quantitative studies reported a pregnancy prevalence of 21.7 (five informal settlements in Kampala,Uganda) [41] and 23% (refugee camp in Ethiopia) [30]. Bol et al. [31] described poor SRH knowledge (40%), low prevalence of contraceptive use (6.5%), and low educational status (42% with no formal education). The pregnancy rates among adolescent girls and young women with no formal education were 3.4 times higher than girls who attended secondary school and above.
Regarding access to and utilization of maternal health services, all pregnant AGYW in the refugee communities on the Thailand-Myanmar border were attending ANC as the study was conducted in the ANC clinics [22]. The other three studies did not report on that.
Malama et al. (Uganda) [41] reported AGYW who are mothers were twice as likely to experience food insecurity and depressive symptoms.
All studies reported financial difficulties, including among the married subjects, and few of the pregnant, unmarried AGYW had received family support.
Contraceptive use and access
Four studies reported contraceptive use and access, three quantitative [37, 38, 43] and one mixed method [50].
The studies were performed in refugee camps in Northern Uganda [37], Ghana [38], Northeastern [43] and Southwest Nigeria [50]. They addressed the use and access to modern contraceptives and the cultural and religious beliefs for not using them.
All the studies reported very low use of modern contraceptives: 8% (Nigeria) [43], 8.7% (Uganda) [37], and 11,7% [38] for the quantitative studies [37, 38, 43] and 32% for the mixed-method study [50]). The method used by the AGYW varied among the studies: injectable contraceptive (42%), oral contraceptive (5.5–29%), male condom (16–55%), implant (36%), emergency contraception (18%).
The reasons reported for not using contraceptives were difficulties accessing health services or lack of information about health services: Ganle et al. [38] reported 39% of AGYW (refugee camp, Ghana) who heard about contraception did not know where they could get it, and Okanlawon et al. (refugee camp, Nigeria) [50] reported 60% did not use contraception due fear of side effects (39–80%); cultural beliefs (11–17%); and partner prohibition (16–40%).
The studies also reported misinformation regarding contraception: Okanlawon et al. [50] described a belief that AGYW would become infertile after contraception use, and 84% of the AGYW in the Ganle et al. [38] study believed that the women who use contraceptives become promiscuous.
Menstrual hygiene management (MHM)
Five studies reported on MHM, two quantitative [39, 44], one qualitative [35] and two mixed methods [51, 52]. They were performed in refugee camps or migrant settlements: Venezuelan migrant settlements in the North-western border of Venezuela-Brazil [44], refugee settlements in Cox's Bazar Bangladesh [51, 52], refugee settlement in Uganda [35], Kobe refugee camp in Ethiopia, and Myanmar migrant communities in Thailand [39], and all described a poor MHM: distance to reach toilets, lack of water, shortage of menstrual hygiene supplies and lack of knowledge about menstruation.
The studies reported there was no private toilet for the majority of the AGYW to use (85–93%) [39, 51], and a lack of MHM products such as hygienic pads (disposable or reusable), soap and clean water (55–83%) [39, 44, 51]. In the Venezuelan migrant settlements in the North-western border of Venezuela-Brazil and in the refugee settlements in Cox's Bazar Bangladesh there was no proper place to wash or dry the disposable pads (65%) [44, 51].
The AGYW reported feeling embarrassed during menstruation (50–60%) [35, 44, 51] and missing school because of MHM issues (refugee settlement in Uganda) [35].
The study performed in the Rohingya camp reported that 72% of AGYW were not allowed to go out during the menstruation period, and 88% were not allowed to cook [51].
The studies also reported that the toilets in the internally displaced people (IDP) camps were distant, and the AGYW (55–65%) feared going to the toilet because of the risk of sexual violence [35, 44, 51].
Sexually transmitted infections (STI) and HIV
Two studies reported on STI [40] and HIV [32]. Both were conducted with urban refugees and displaced youth living in informal settlements in Kampala, Uganda. They described there is a stigma associated with STI and HIV testing.
The study on STIs [39] described 74% had never been tested for STIs and more than half of the adolescents (56%) were unaware of the STI testing services. Among those tested, 16% did not know to inform the test results received. The STIs reported by the adolescents were: 10% more than two STIs, 15% herpes, 9% gonorrhea, and 6% syphilis. There was no information regarding HIV.
Among AGYW, stigma on STI testing was associated with lower contraceptive use and food insecurity [39].
The HIV study evidenced the barriers to HIV testing and prevention are the cost of transportation to HIV testing services, language barriers, lack of private spaces to do the self-test, medical mistrust, and inequitable gender norms [34].
SRH information/knowledge/access
Seven studies reported on SRH information, knowledge and access: five qualitative [23,24,25, 29, 34] and two mixed methods [46, 47]. The qualitative studies were conducted in Rwanda (Mahama camp and in the surrounding host community) [29], in a town in Lebanon’s Bekaa governorate (Syrian Refugee Adolescent Girls) [23], in the West Bank and Jordan (Palestinian refugee camps) [34], in an industrial area in North-East Beirut in Lebanon (Syrian refugee adolescent girls) [24], in Thailand border with Myanmar (one migrant community and one Refugee camp) [25]; the mixed-methods study were conducted in villages along the northwestern border inside Thailand (two refugee camps with young Burmese refugees) [46] and in Nakivale refugee settlement, Uganda (migrants from DR Congo and Burundi) [47]. Overall, there is a lack of SRH information and misconceptions, and an unsatisfactory number of SRH services.
Three studies identified family members, mostly mothers, as trusted sources of SRH information. [23, 24, 47].
Schools were also described as a place to obtain SRH information, although most AGYW did not attend school. [23, 25, 29, 47].
Regarding SRH knowledge, in the Nakivale refugee settlement, Uganda, Ivavona et al. [47] reported that 16% of the AGYW did not know about STIs and 52% were able to mention only one STI; 14% did not know about contraception, 44% knew one method and 15% knew three or more methods.
Benner et al. [46] identified that 66% of Burmese refugees AGYW in Thailand refugee camps did not know if it was possible to get pregnant after the first sexual intercourse, 68% did not know if women can take contraceptive pills daily, 59% did not know if condoms can be used during sex, and 45% did not know if it is accceptable for a boy to sometimes force a girl to have sex if he loves her.
Meyer et al. [29] described the decrease in SRH information sessions and SRH services after the onset of the COVID-19 pandemic in Rwanda refugee community; the AGYW complained of unplanned pregnancies due to the contraception disruptions and about the suspension of the SRH activities from local Non-Governmental Organizations (NGOs).
All studies highlighted the need for shaping programs by sex and age to address SRH information and recommended empowering adolescent mothers as agents of SRH evidence-based information.
Overview of the main SRH needs
Four studies, two qualitative [26, 30], one quantitative [6] and one mixed methods [49] reported an overview of SRH information, needs, access to it, and outcomes. The qualitative studies were conducted in IDP camps in Nigeria [26] and a refugee camp in Ethiopia (Somali adolescent girls) [30]; the quantitative study was conducted in Venezuelan migrant settlements on the Northwestern border of Venezuela and Brazil [6]; and the mixed-methods studies were conducted in IDP camps in Borno State (Nigeria). [49].
All of them evidence poor SRH outcomes as limited access to family planning, unsafe sex, early marriages, pregnancy complications and low knowledge and access to SRH services.
Soeiro et al. [6] reported that, among Venezuelan pregnant AGYW (in migrant settlements on the Northwestern border of Venezuela and Brazil), 33% were not attending ANC, and the reasons were not knowing where to go (40%), difficulty reaching the health center (20%) and not having personal documents (20%). The main self-reported SRH concerns were contraception (35%), and 75% of the adolescents who went to a health center did not get it.
In the Odo et al. [49] study, 98% of adolescent girls (IDP camps, Nigeria) described sex education as important, and they agreed that the main SRH problems were teenage pregnancy (72%), early marriage (76%), menstrual problems (70%), and maternal mortality (80%).
Marlow et al. [26] also demonstrate that food insecurity in the IDP camp (Nigeria) has driven adolescent girls to sex in exchange for goods or into forced marriages.
All articles highlighted the need for specific SRH services for IDP, refugees or migrant AGYW.
Other issues related to SRH
Child early and forced marriage or partnership (CEFMP)
Four studies one quantitative [45], two qualitative [33, 36] and one mixed methods [48] reported on CEFMP (formal marriage or an informal union, before reaching the age of 18) [53]. The quantitative study was conducted in the Kurdistan Region of Iraq (IDPs AGYW) [45]. The qualitative study was conducted in a Palestinian refugee camp [36] and in three governorates in Egypt (Syrian refugees AGYW) [33], and the mixed-methods study was conducted in a refugee settlement in Uganda (South Sudanese AGYW) [48].
In the countries where the studies were conducted, the minimum age of marriage for girls is 18 in Egypt, Iraq, and Uganda, and 17 in Palestine. In Syria and South Sudan (AGYW origin countries), the minimum age of marriage is 18 for Syrian girls, and there is no minimum age of marriage for South Sudanese girls [54]. The four studies had an association between social and financial insecurity and early marriage.
Adolescent marriage was associated with negative SRH outcomes such as lack of family planning, unplanned pregnancies, and disruption of schooling [33, 36, 45, 48]. Elnakib et al. (Syrian refugees AGYW, in Egypt) [33] described adolescent girls' isolation after marriage and difficulties with their baby birth registration.
Goers et al. (IDP AGYW in the Kurdistan Region of Iraq) [45] described that 38% of the AGYW [10,11,12,13,14,15,16,17,18,19] were married. The risk of marriage before 18 years was 6.2 times higher for girls than boys. Only 6% of the married or engaged refugee adolescent girls were in school. The influencing factors in marriage decisions were displacement (12%), money/resources (21%) and war/conflict (29%).
In the Loutet et al. (South-Sudanese AGYW in Uganda) [48] study, 75% of AGYW were married, and 57% had primary-level education or lower. CEFMP was associated with forced pregnancy (50%), forced abortion (45%), missed school due to sexual violence (95%) and survival sex work (64%).
In contrast to the other three studies, the findings of Knox et al. (Palestine refugee camp) [36] demonstrated that not all child marriages were forced. Some AGYW reported that they felt they were a burden to their families due to post-conflict economic crises and chose to marry.
Sexual and gender-based violence (SGBV)
Two studies reported SGBV as the main outcome of their research. The quantitative study was conducted in informal settlements in Kampala, Uganda (refugee AGYW were from South Sudan, DR Congo, Burundi and Rwanda); the qualitative study was conducted in a refugee camp in the Yumbe District, Uganda (refugee AGYW were from South Sudan and DR Congo).
In a quantitative study, Logie et al. [41] evidenced that over half of the participants (54%) reported intimate partner violence (IPV) in the last 12 months (55% reported polyvictimization: physical, sexual, and control violence). IPV polyvictimization was associated with depressive symptoms (90%), and food insecurity (94%).
In a qualitative study, Logie et al. [28] explored the refugee adolescent well-being factors and SGBV was associated with poverty, food insecurity, and unemployment, leading to CEFMP and transactional sex. The study also described how deforestation exacerbated sexual violence, as the AGYW must go further to collect water and firewood.
The studies did not report which resources were available to address SGBV in the research settings.
Discussion
This review aimed to explore the current qualitative and quantitative research landscape on the SRH needs of adolescent girls and young women displaced by humanitarian crises.
Specific studies targeting SRH of AGYW migrants (10–24 years old) are recent, with a significant increase since 2021. Possible explanations for this increase could be that the forcibly displaced population has quintupled in the last two decades, from 20.7 million in 2000 to 100 million in 2022 [55], and that adolescent health, including SRH, has been included in the 2030 Sustainable Development Goals since 2015 [3].
The reviewed studies reported greater pregnancy rates before age 18, ranging from 16% (migrant settlements in Australia) [27] to 23% (refugee camps in Ethiopia) [31], compared with the global pregnancy rate before age 18 (14%) [56]. They also reported that 100% of the adolescents had quit school, more than twice reported in a study conducted with pregnant AGYW in Cameroon (41.6% drop-off rate). [57].
Regarding modern contraceptive use, 43% of AGYW in low- and middle-income countries use male condoms, oral pills or injectables [58], compared with 8–32% [50] of contraceptive use in the presented studies.
The CEFMP has been described as a cultural and societal pattern in some countries [59]. However, in the countries where the studies were conducted, the minimum age of marriage for girls was 17 years. The analyzed studies corroborate that in humanitarian settings, the situation of insecurity, increased poverty and often the loss of family members lead to girls being more likely to engage in CEFMP. [33, 45, 48]. Recommendations on how to address it do not include humanitarian settings [55, 56].
Furthermore, CEFMP is also linked to lack of contraception [60] and adolescent pregnancies [9, 59], as well as. Pregnancy and childbirth complications are one of the leading causes of death among 15- to 19-year-old girls worldwide [9, 60]. Studies in this review showed a high prevalence of adolescent pregnancies, frequently unplanned [22, 27, 31, 42], but most of them did not discuss those pregnant adolescent's morbidity and mortality rate in the study settings. As there is a lack of health services and proper data systems records in humanitarian settings, the impact of those pregnancies probably remains underestimated. [10].
The global increase of STIs among adolescents has been described for boys and girls. However, the prevalence is higher among adolescent girls [61]. New HIV infections are also higher among adolescent girls [62]. Logie et al. [32, 40] identified barriers to HIV and STI testing and stigma among adolescent refugee girls living in Kampala, Uganda, hindering these diagnoses among AGYW. There are few studies on STIs and HIV among migrant AGYW; a study conducted in South Africa also reported difficulty accessing health services as a risk factor for HIV [63].
Concerning access to SRH services, the findings evidence a lack of these services in humanitarian contexts [46, 47], which have been further affected by the COVID-19 pandemic. There are scarce studies on this topic and even fewer for migrant AGYW. A systematic review conducted in low- and middle-income countries also reported the impact of the COVID-19 pandemic on the AGYW's SRH due to the interruption of SRH services, resulting in increased rates of early marriage, sexual or intimate partner violence, and disruption of maternal care [64]. Meyer et al. [29] described unplanned pregnancies among refugee AGYW in Rwanda due to contraception disruptions during this period.
Most studies also recommended specific SRH programs and health services for adolescents in humanitarian settings. However, they did not report which interventions were available in the studies' countries. Notwithstanding the increasing number of studies on this subject, specific interventions targeting SRH for adolescent girls are still uncommon. A systematic review [65] published in 2019 identified only nine SRH interventions for adolescents and youth in armed conflict settings. Only one study was published before 2012 (in 2006), and the majority were implemented in African countries, one in Colombia and one in Pakistan, evidencing the need for global SRH interventions targeting AGYW.
This systematic review evaluated qualitative, quantitative and mixed-methods studies on SRH issues of AGYW displaced by humanitarian crises in African, Asia and South American countries. All issues reported in the studies are included in the SDG targets. There are some strategies and tools described to address the SRH of AGYW in humanitarian contexts [7, 66]. However, the studies did not mention these or any other strategies to improve SRH in the study settings. In addition, data collection, monitoring and evaluation in these contexts still need to be standardized to understand the gaps better and adapt specific interventions in to reach the SDGs 2023.
Limitations
We included studies with girls and young women from 10 to 24 years old, and we may have missed data from studies which included all women of reproductive age. Moreover, as we considered studies in English, Spanish and French, we may have missed some studies in other languages and some reports from grey literature.
Conclusions
The SRH of adolescent girls and young women in humanitarian crisis contexts has been neglected. Despite the growing number of studies on this population (32 studies were analyzed, and most of them were published between 2020 and 2022), there was no description of local interventions to address the reported issues. The migrant AGYW have difficulty accessing contraceptives, a high prevalence of unplanned pregnancies, child marriage, and sexual and gender-based violence. Improving data collection, monitoring, and evaluation may help humanitarian support and researchers to establish specific interventions for this population.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- AGYW:
-
Adolescent girls and young women
- ANC:
-
Antenatal care
- CEFMP:
-
Child, early and forced marriage or partnership
- COVID-19:
-
Coronavirus Disease 2019
- FGD:
-
Focal Groups Discussion
- HIV:
-
Human Immunodeficiency Virus
- IDI:
-
In-depth interviews
- IDP:
-
Internally displaced population
- IPV:
-
Intimate partner violence
- KRI:
-
Kurdistan Region of Iraq
- MeSH:
-
Medical Subject Headings
- MHM:
-
Menstrual hygiene management
- MMAT:
-
Mixed Methods Appraisal Tool
- NGO:
-
Non-Governmental Organization
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- SDG:
-
Sustainable Development Goals
- SGBV:
-
Sexual and Gender Based Violence
- SRH:
-
Sexual and reproductive health
- STI:
-
Sexually transmitted infections
- UNFPA:
-
United Nations Funds for Population
- UNHCR:
-
United Nations High Commissioner for Refugees
- VYA:
-
Very young adolescents
- WHO:
-
World Health Organization
References
UNHCR (United Nations High Commissioner for Refugees). UNHCR: A record 100 million people forcibly displaced worldwide [Internet]. May. 2022. https://news.un.org/en/story/2022/05/1118772. Accessed 7 Jan 2023.
Christelle Cazabat. WOMEN AND GIRLS in internal displacement. UN Women,IMPACT Initiat Int [Internet]. 2020;1–5. http://www.internationalinspiration.org/women-and-girls
United Nations (UN). 2030 Sustainable Development Goals [Internet]. https://sdgs.un.org/goals. Accessed 2 Apr 2023.
Ivanova O, Rai M, Kemigisha E. A systematic review of sexual and reproductive health knowledge, experiences and access to services among refugee, migrant and displaced girls and young women in Africa. Int J Environ Res Public Health. 2018;15(8):1–12.
World Health Organization. World report on the health of refugees and migrants [Internet]. 2022. 344 p. https://www.who.int/publications/i/item/9789240054462
Soeiro RE, Rocha L, Surita FG, Bahamondes L, Costa ML. A neglected population: Sexual and reproductive issues among adolescent and young Venezuelan migrant women at the northwestern border of Brazil. Int J Gynecol Obstet. 2022;157(1):51–8.
Inter-Agency Working Group on Reproductive Health in Crises (IAWG). Adolescent sexual and reproductive health toolkit for humanitarian settings. 2020
United Nations Population Fund (UNFPA). State of world population 2023. 2023.
United Nations Population Fund (UNFPA). Adolescent Girls in Disaster & Conflict. Interventions for Improving Access to Sexual and Reproductive Health Services. 2016;
Broaddus-Shea ET, Kobeissi L, Ummer O, Say L. A systematic review of monitoring and evaluation indicators for sexual and reproductive health in humanitarian settings. Confl Health. 2019;13(1):1–26.
Sandelowski Margarete, Voils Corrine I. Defining and designing mixed research synthesis studies. NIH Public Access. 2006;23(1):1–7.
Centre for Reviews and Dissemination U of Y. Systematic Reviews CRD’s guidance for undertaking reviews in health care. 2008. 282.
Moher D, Liberati A, Tetzlaff J AD. The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement.
Pluye P, Robert E, Cargo M, Barteltt G, Cathain A, Griffiths F, et al. Tool development developers method of development contact person resources title of primary resource proposal: a mixed methods appraisal tool for systematic mixed studies title of supplementary resource title of supplementary resource. J Heal Serv Res Policy Ref Landis Biometrics. 2011;13(33):92–8.
Hong QN, Fàbregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ Inf. 2018;34(4):285–91.
Hong QN, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, et al. Improving the content validity of the mixed methods appraisal tool: a modified e-Delphi study. J Clin Epidemiol. 2019;111:49-59.e1.
Hong QN, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, Dagenais P G, M-P, Griffiths F, Nicolau B, O’Cathain A, Rousseau M-C VI. Mixed Methods Appraisal Tool (MMAT), version 2018. Regist Copyr (#1148552), Can Intellect Prop Off Ind Canada.
Segen’s Medical Dictionary. Medical Subject Headings. In: The Free Dictionary; Farlex: Huntingdon Valley, PA, USA, 2012.
Ouzzani M. Rayyan—a web and mobile app for systematic reviews. Syst Rev. 2017;2016:1–10. https://doi.org/10.1186/s13643-016-0384-4.
Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Narrative synthesis in systematic reviews: a product from the ESRC methods programme. ESRC Methods Program. 2006;2006:93.
Popay J, Rogers A, Williams G. Rationale and standards for the systematic review of qualitative literature in health services research. Qual Health Res. 1998;8(3):341–51.
Asnong C, Fellmeth G, Plugge E, Wai NS, Pimanpanarak M, Paw MK, et al. Adolescents’ perceptions and experiences of pregnancy in refugee and migrant communities on the Thailand-Myanmar border: a qualitative study. Reprod Health. 2018;15(1):1–13.
El Ayoubi LL, Abdulrahim S, Sieverding M. Sexual and reproductive health information and experiences among syrian refugee adolescent girls in Lebanon. Qual Health Res. 2021;31(5):983–98.
Korri R, Hess S, Froeschl G, Ivanova O. Sexual and reproductive health of Syrian refugee adolescent girls: a qualitative study using focus group discussions in an urban setting in Lebanon. Reprod Health. 2021;18(1):1–17. https://doi.org/10.1186/s12978-021-01178-9.
Lee C, Aules Y, Sami S, Lar PK, Schlect J, Robinson C. Sexual and reproductive health needs and risks of very young adolescent refugees and migrants from Myanmar living in Thailand. Confl Health. 2017;11(Suppl 1).
Marlow HM, Kunnuji M, Esiet A, Bukoye F, Izugbara C. The sexual and reproductive health context of an internally displaced persons’ camp in Northeastern Nigeria: narratives of girls and young women. Front Reprod Heal. 2022;3(January):1–7.
McMichael C. Unplanned but not unwanted? Teen pregnancy and parenthood among young people with refugee backgrounds. J Youth Stud. 2013;16(5):663–78.
Logie CH, Okumu M, Latif M, Musoke DK, Odong Lukone S, Mwima S, et al. Exploring resource scarcity and contextual influences on wellbeing among young refugees in Bidi Bidi refugee settlement, Uganda: findings from a qualitative study. Confl Health. 2021;15(1):1–11.
Meyer K, Abimpaye M, de Harerimana JD, Williams C, Gallagher MC. Understanding the sexual and reproductive health experiences of refugee and host community adolescents and youth in rwanda during COVID-19: needs, barriers, and opportunities. Front Reprod Heal. 2022;4(March):1–13.
Ortiz-Echevarria L, Greeley M, Bawoke T, Zimmerman L, Robinson C, Schlecht J. Understanding the unique experiences, perspectives and sexual and reproductive health needs of very young adolescents: Somali refugees in Ethiopia. Confl Health. 2017;11(Suppl 1).
Bol KN, Negera E, Gedefa AG. Pregnancy among adolescent girls in humanitarian settings: a case in refugee camp of Gambella regional state, community-based cross-sectional study, Southwest Ethiopia, 2021. BMJ Open. 2022;12(11).
Logie CH, Okumu M, Kibuuka Musoke D, Hakiza R, Mwima S, Kacholia V, et al. The role of context in shaping HIV testing and prevention engagement among urban refugee and displaced adolescents and youth in Kampala, Uganda: findings from a qualitative study. Trop Med Int Heal. 2021;26(5):572–81.
Elnakib S, Hussein SA, Hafez S, Elsallab M, Hunersen K, Metzler J, et al. Drivers and consequences of child marriage in a context of protracted displacement: a qualitative study among Syrian refugees in Egypt. BMC Public Health. 2021;21(1):1–14.
Ghandour R, Hammoudeh W, Giacaman R, Holmboe-Ottesen G, Fjeld HE. Coming of age: a qualitative study of adolescent girls’ menstrual preparedness in Palestinian refugee camps in the West Bank and Jordan. Sex Reprod Heal Matters. 2022;30(1):1–17.
Kemigisha E, Rai M, Mlahagwa W, Nyakato VN, Ivanova O. A qualitative study exploring menstruation experiences and practices among adolescent girls living in the nakivale refugee settlement, Uganda. Int J Environ Res Public Health. 2020;17(18):1–11.
Knox SEM. How they see it: Young women’s views on early marriage in a post-conflict setting. Reprod Health Matters. 2017;25:S96-106. https://doi.org/10.1080/09688080.2017.1383738.
Bakesiima R, Cleeve A, Larsson E, Tumwine JK, Ndeezi G, Danielsson KG, et al. Modern contraceptive use among female refugee adolescents in northern Uganda: prevalence and associated factors. Reprod Health. 2020;17(1):1–9.
Ganle JK, Amoako D, Baatiema L, Ibrahim M. Risky sexual behaviour and contraceptive use in contexts of displacement: Insights from a cross-sectional survey of female adolescent refugees in Ghana. Int J Equity Health. 2019;18(1):1–11.
Kågesten AE, Zimmerman L, Robinson C, Lee C, Bawoke T, Osman S, et al. Transitions into puberty and access to sexual and reproductive health information in two humanitarian settings: a cross-sectional survey of very young adolescents from Somalia and Myanmar. Confl Health. 2017;11(Suppl 1).
Logie CH, Okumu M, Mwima S, Kyambadde P, Hakiza R, Kibathi IP, et al. Sexually transmitted infection testing awareness, uptake and diagnosis among urban refugee and displaced youth living in informal settlements in Kampala, Uganda: a cross-sectional study. BMJ Sex Reprod Heal. 2020;46(3):192–9.
Logie CH, Okumu M, Mwima S, Hakiza R, Irungi KP, Kyambadde P, et al. Social ecological factors associated with experiencing violence among urban refugee and displaced adolescent girls and young women in informal settlements in Kampala, Uganda: a cross-sectional study. Confl Health. 2019;13(1):1–15.
Malama K, Logie CH, Okumu M, Hakiza R, Mwima S, Kyambadde P. Factors associated with motherhood among urban refugee adolescent girls and young women in informal settlements in Kampala. Uganda Women Heal. 2023;63(1):51–8. https://doi.org/10.1080/03630242.2022.2158411.
Marlow HM, Kunnuji M, Esiet A, Bukoye F, Izugbara C. Contraceptive use, menstrual resumption, and experience of pregnancy and birth among girls and young women in an internally displaced persons camp in Northeastern Nigeria. Afr J Reprod Health. 2022;26(12):138–45.
Soeiro RE, Rocha L, Surita FG, Bahamondes L, Costa ML. Period poverty: menstrual health hygiene issues among adolescent and young Venezuelan migrant women at the northwestern border of Brazil. Reprod Health. 2021;18(1):1–9. https://doi.org/10.1186/s12978-021-01285-7.
Goers M, Hunersen K, Karim LS, Jeffery A, Zedan A, Robinson C, et al. Child marriage among displaced populations – a 2019 study in Kurdistan Region of Iraq. BMC Public Health. 2022;22(1):1–11. https://doi.org/10.1186/s12889-022-13220-x.
Benner MT, Townsend J, Kaloi W, Htwe K, Naranichakul N, Hunnangkul S, et al. Reproductive health and quality of life of young Burmese refugees in Thailand. Confl Health. 2010;4(1):1–9.
Ivanova O, Rai M, Mlahagwa W, Tumuhairwe J, Bakuli A, Nyakato VN, et al. A cross-sectional mixed-methods study of sexual and reproductive health knowledge, experiences and access to services among refugee adolescent girls in the Nakivale refugee settlement, Uganda. Reprod Health. 2019;16(1):1–11.
Loutet MG, Logie CH, Okumu M, Berry I, Lukone SO, Kisubi N, et al. Sexual and reproductive health factors associated with child, early and forced marriage and partnerships among refugee youth in a humanitarian setting in Uganda: mixed methods findings. Afr J Reprod Health. 2022;26(12):66–77.
Odo AN, Musa K, Oladugba AV. Sexual and reproductive health needs and problems of internally displaced adolescents (IDAs) in Borno State, Nigeria: a mixed method approach. Afr J Reprod Health. 2020;24(1):87–96.
Okanlawon K, Reeves M, Agbaje OF. Contraceptive use: knowledge, perceptions and attitudes of refugee youths in Oru Refugee Camp, Nigeria. Afr J Reprod Health. 2010;14:16–25.
Pandit K, Hasan MJ, Islam T, Rakib TM. Constraints and current practices of menstrual hygiene among Rohingya adolescent girls. Heliyon. 2022;8(5).
Rakhshanda S, Ahmed S, Saidu S, Nderitu C, Thapa B, Awal A, et al. Knowledge and practice regarding menstrual hygiene management among the Rohingya refugee adolescent girls in Cox’s Bazar, Bangladesh: a mixed method study. Int J Hum Rights Healthc. 2021;14(4):311–26.
United Nations Population Fund (UNFPA). Child marriage [Internet]. https://www.unfpa.org/child-marriage. Accessed 2 Apr 2023.
World Economic Forum. These are the countries where child marriage is legal [Internet]. 2016. [cited 2023 Oct 23]. https://www.weforum.org/agenda/2016/09/these-are-the-countries-where-child-marriage-is-legal/. Accessed 23 Oct 2023.
Institute T online J of the MP. Top Statistics on Global Migration and Migrants [Internet]. 2022. https://www.migrationpolicy.org/print/17530#Humanitarian.migrants. Accessed 25 Oct 2023.
UNICEF - United Nations Children’s Fund. Early childbearing [Internet]. 2022. https://data.unicef.org/topic/child-health/adolescent-health/. Accessed 25 Oct 2023.
Sobngwi-Tambekou JL, Tsague-Agnoux M, Fezeu LK, Ndonko F. Teenage childbearing and school dropout in a sample of 18,791 single mothers in Cameroon. Reprod Health. 2022;19(1):1–9. https://doi.org/10.1186/s12978-021-01323-4.
UNFPA. Contraception for adolescents and Youths. 2019;21.
Das M, Guedes A, Moletsane R, Svanemyr J. Singularity and diversity in child, early, and forced marriage and unions. J Adolesc Heal. 2022;70(3):S1-4.
Liang M, Simelane S, Fortuny Fillo G, Chalasani S, Weny K, Salazar Canelos P, et al. The state of adolescent sexual and reproductive health. J Adolesc Heal. 2019;65(6):S3-15. https://doi.org/10.1016/j.jadohealth.2019.09.015.
Amiri M, El-Mowafi IM, Chahien T, Yousef H, Kobeissi LH. An overview of the sexual and reproductive health status and service delivery among Syrian refugees in Jordan, nine years since the crisis: a systematic literature review. Reprod Health. 2020;17(1):1–20.
Starrs AM, Ezeh AC, Barker G, Basu A, Bertrand JT, Blum R, et al. Accelerate progress—sexual and reproductive health and rights for all: report of the Guttmacher-Lancet Commission. Lancet. 2018;391:2642–92.
Temin M, Milford C, Beksinska M, Van Zyl D, Cockburn J. Inclusive HIV prevention in South Africa: reaching foreign migrant adolescent girls. Front Reprod Heal. 2021;3(May):1–9.
Meherali S, Adewale B, Ali S, Kennedy M, Salami B, Richter S, et al. Impact of the COVID-19 pandemic on adolescents’ sexual and reproductive health in low-and middle-income countries. Int J Environ Res Public Health. 2021;18(24):13221.
Jennings L, George AS, Jacobs T, Blanchet K, Singh NS. A forgotten group during humanitarian crises: a systematic review of sexual and reproductive health interventions for young people including adolescents in humanitarian settings. Confl Health. 2019;13(1):15–7.
Inter-Agency Working Group Women’s Refugee Comission (IAWG). Minimum Initial Service Package (MISP) Process Evaluation Tools (2017). 2017.
Acknowledgements
To Ana Paula de Morais e Oliveira for her collaboration on the search strategy.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
RES and MLC had the initial idea for the study. RES and JCS were responsible for the blind review and studies analysis. MLC was accountable for solving the conflicts. RES, RES wrote the first draft of the paper. JPSG reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Search strategy.
Additional file 2.
Mixed methods appraisal tool (MMAT) version 2018.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Soeiro, R.E., de Siqueira Guida, J.P., da-Costa-Santos, J. et al. Sexual and reproductive health (SRH) needs for forcibly displaced adolescent girls and young women (10–24 years old) in humanitarian settings: a mixed-methods systematic review. Reprod Health 20, 174 (2023). https://doi.org/10.1186/s12978-023-01715-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12978-023-01715-8