
Abstract
Background
Anencephaly is a fatal congenital anomaly characterized by the absence of brain hemispheres and cranial arch. Timely preventive measures can be taken by knowing the exact prevalence of this common neural tube defect; thus, carried out through systematic review and meta-analysis, the present study was conducted to determine the worldwide prevalence, incidence and mortality of anencephaly.
Methods
Cochran’s seven-step instructions were used as the guideline. Having determined the research question and inclusion and exclusion criteria, we studied MagIran, SID, Science Direct, WoS, Web of Science, Medline (PubMed), Scopus, and Google Scholar databases. Moreover, the search strategy in each database included using all possible keyword combinations with the help of “AND” and “OR” operators with no time limit to 2021. The I2 test was used to calculate study heterogeneity, and Begg and Mazumdar rank correlation tests were employed to assess the publication bias. Data were analyzed by Comprehensive Meta-Analysis software (Version 2).
Results
In this study, the statements of Preferred Reporting Items for Systematic Reviews and Meta-Analyzes (PRISMA) were used. In the first stage, 1141 articles were found, of which 330 duplicate studies were omitted. 371 articles were deleted based on the inclusion and exclusion criteria by reviewing the title and abstract of the study. 58 articles were removed by reviewing the full text of the article because it was not relevant to the research. 360 studies with a sample size of 207,639,132 people were considered for the meta-analysis. Overall estimate of the prevalence, incidence and attenuation of anencephaly worldwide were 5.1 per ten thousand births (95% confidence interval 4.7–5.5 per ten thousand births), 8.3 per ten thousand births (95% confidence interval 5.5–9.9 per ten thousand births), 5.5 per ten thousand births (95% confidence interval 1.8–15 per ten thousand births) respectively the highest of which according to the subgroup analysis, belonged to the Australian continent with 8.6 per ten thousand births (95% confidence interval 7.7–9.5 per ten thousand births).
Conclusion
The overall prevalence of anencephaly in the world is significant, indicating the urgent need for preventive and treating measures.
Plain Language summary
Anencephaly is a fatal congenital anomaly characterized by the absence of brain hemispheres and cranial arch. Cochran’s seven-step instructions were used as the guideline. Having determined the research question and inclusion and exclusion criteria, we studied MagIran, SID, Science Direct, WoS, Web of Science, Medline (PubMed), Scopus, and Google Scholar databases. Moreover, the search strategy in each database included using all possible keyword combinations with the help of “AND” and “OR” operators with no time limit to 2021. Out of 1141 initial articles found, and after excluding repetitive ones in various databases and those irrelevant to inclusion criteria, 360 studies with a sample size of 207,639,132 people were considered for the meta-analysis. Overall estimate of the prevalence, incidence and attenuation of anencephaly worldwide were 5.1 per ten thousand births (95% confidence interval 4.7–5.5 per ten thousand births), 8.3 per ten thousand births (95% confidence interval 5.5–9.9 per ten thousand births), 5.5 per ten thousand births (95% confidence interval 1.8–15 per ten thousand births) respectively the highest of which according to the subgroup analysis, belonged to the Australian continent with 8.6 per ten thousand births (95% confidence interval 7.7–9.5 per ten thousand births). The overall prevalence of anencephaly in the world is significant, indicating the urgent need for preventive and treating measures.
Similar content being viewed by others

Background
Neural Tube Defects (NTDs) are considered the most common congenital anomalies of the central nervous system (CNS) [1], and the second most serious ones after inborn heart defects [2]. Non-spontaneous neural tube closure between the 3rd and 4th weeks of intrauterine growth is considered as the leading cause of this defect [1]. Regarding the etiology of these defects, most cases are attributed to the interaction between different genes and environmental factors, known as a multifactorial inheritance [3]. Studies indicate that immediate family members are more at risk compared to others; in other words, if a child is born with NTD, the risk of recurrence in future pregnancies is between 25 and 50 times higher than in general cases [4, 5, 6]. Moreover, diabetes mellitus, using valproic acid to treat epilepsy during pregnancy, obesity, zinc deficiency, hyperthermia, and folate deficiency are all predisposing factors for neural tube defects [7, 8].
Though being significantly various in different geographical areas, the incidence of NTD is generally around 1 in 1000 live births or (NTD affects about 1 in 1000 live births on average, however this varies greatly by area.) [4, 9]. Pathologically, neural tube defects vary from a small, uncomplicated opening in the posterior canal of the vertebrae to the failure of the entire neural tube to close, leading to the most severe type of defect that is craniorachischisis [10]. The most recurring cases include anencephaly, spina bifida, and encephalocele [10].
Anencephaly is a fatal congenital malformation characterized by the absence of hemispheres of the brain and cranial arch [11]. Anencephaly is the most common CNS disorder in the Western world, occurring 37 times more frequently in women than men [12]. Babies born with such defects generally die at birth or shortly thereafter while newborns with spina bifida and encephalocele require special medical care and surgery to survive [13]. Prevalence of anencephaly mortality (100%), compared to Spina bifida (7%) and encephalocele (46%), is significantly higher [14]; thus, anencephaly is considered as a taxing burden on public health worldwide that may lead to significant human resources loss [15].
Frog-like appearance, short neck, bulging eyes, and large tongue are characteristic features of infants with anencephaly [16]. About 12% of cases of anencephaly are associated with other structural abnormalities [17], including Cleft lip, cleft palate, clubfoot and omphalocele (Anencephaly is linked to additional structural abnormalities in around 12% of cases [17], such as cleft lip, cleft palate, clubfoot, and omphalocele) [16]. Anencephaly was the first congenital anomaly to be detected by ultrasound, and it can be diagnosed at weeks 12–13 of pregnancy while preventive measures include controlling known risk factors and offering medical counseling to couples about termination of pregnancy [16]. Previous studies have demonstrated that anencephaly is a multifactorial process that is controlled by genes and numerous other environmental factors. However, recent studies reveal that folic acid supply before and in the early stages of pregnancy (1 to 3 months before pregnancy and up to 12 weeks of gestation) can dramatically prevent anencephaly and reduce its prevalence by 50–70% [18]. The U.S. Public Health Service and the Food and Nutrition Council of the Institute of Medicine, along with the National Research Council, recommend that all women of childbearing potential can take 0.4 mg of folic acid daily to reduce the risk of developing neural tube defects [19, 20].
Annually, about 300,000 babies are born with neural tube defects, resulting in 88,000 deaths and 8.6 million lifelong disabilities [21]. The occurrence of anencephaly varies over time and geographically. For instance, the prevalence of this defect in northern Iran in 1998–2005 was estimated at 12 per 10,000 births [22] while In Texas, the United States, 2.81 per 10,000 births during 1999–2003 were reported [23]. The prevalence of anencephaly based on data collected from (EUROCAT) member countries during the years 2000 and 2010, was estimated at 3.52 per 10,000 births [24].
Considering the importance of anencephaly as the most severe type of neural tube defect, and its detrimental effects on the quantity and quality of patients’ and parents’ life, and regarding the serious health, psychological, social and economic costs for the individual and society, accurate identification of patients is of great importance to organize health care services and implement preventive measures. In addition, because of various statistics on the prevalence of anencephaly and the worldwide absence of a comprehensive investigation capable of analyzing the outcomes of these studies, the present research was conducted through a systematic review and meta-analysis to shed light on the prevalence, incidence and mortality of anencephaly worldwide.
Methods
The present systematic review and meta-analysis was conducted based on the Cochrane 7-step approach, including: research question selection, inclusion and exclusion criteria, article identification, study selection, study quality evaluation, data extraction, and analysis and interpretation of findings [25]. In this study, the statements of Preferred Reporting Items for Systematic Reviews and Meta-Analyzes (PRISMA) were used [26].
Research question and keyword determination
According to the research question “How has the prevalence, incidence and mortality of anencephaly changed worldwide?” the following were defined:
The study population (Population) included patients with anencephaly, result (Outcome) comprised the prevalence of anencephaly, date of publishing the first related article until March 23, 2021 was specified as the time range (Time or Duration), and type of study (study design) included cross-sectional studies (descriptive, descriptive-analytical). Keywords were extracted from the MeSH browser. Keywords related to the studied population (P): Anencephaly, Congenital Absence of Brain, Anencephalus, Anencephalia, Incomplete Anencephaly, Partial Anencephaly, Hemicranial Anencephaly, Aprosencephaly and Keywords related to outcome were (O), Prevalence, outbreak.
Inclusion and exclusion criteria according to the research question
Cross-sectional population-based studies (descriptive, descriptive-analytical) that reported the prevalence of anencephaly in different parts of the world, published in Persian and English with full texts available included in the study. Analytical, interventional, conferential, and group-case studies irrelevant to the research question and studies that were not in English or did not have English abstracts were excluded from the investigation.
Article identification
To review the literature, two Persian databases, including MagIran and SID, and four international ones, Science Direct, Web of Science (WoS), Medline (PubMed), and Scopus, were selected. The Google Scholar scientific search engine was considered for final review while no time limit was set for the search to retrieve relevant results; thus, all articles published up to March 23, 2021 were reviewed. Searching was limited to studies published in Persian and English and strategy in each database was determined using Advanced Search (Advance Search) with the help of all possible keyword combinations with the help of AND and OR operators. For example, searching strategy in the PubMed database was determined as follows:
(prevalence [Title/Abstract] OR outbreak [Title/Abstract]) AND (Anencephaly [Title/Abstract] OR Congenital Absence of Brain [Title/Abstract] OR Anencephalus [Title/Abstract] OR Anencephalia [Title/Abstract] OR Incomplete Anencephaly [Title/Abstract] OR Partial Anencephaly [Title/Abstract] OR Hemicranial Anencephaly [Title/Abstract] OR Aprosencephaly [Title/Abstract]).
In order to access the latest published studies, an alert was created on a number of important databases, including PubMed and Scopus, to check if new articles were published during the study. Also, in order to access all related studies, the sources of articles that met the inclusion criteria were manually reviewed. To avoid error, all steps of article search, study selection, qualitative evaluation and data extraction were performed independently by two researchers (BF and ND). If there was a difference of opinion among the researchers regarding the inclusion of the article in the study, in order to avoid the risk of biased selections for specific studies, first a final agreement was reached through discussion and in some cases with the participation and opinion of a third party (MM).
Selection of studies based on inclusion and exclusion criteria
The information of all articles found in each database was transferred to EndNote X8 software. After completing the search in all the databases, duplicate articles were excluded. Then, in order to avoid the risk of prejudice in selecting studies, the names of the authors and the titles of the journals of the articles were removed and a checklist was prepared based on the titles and abstracts of the studies. In the next step, two authors (N.D. and B.F.) independently examined the title and abstract of the research and eliminated irrelevant papers based on the inclusion and exclusion criteria. Studies with no full text were not considered for the systematic review and meta-analysis process. The full text of all remaining articles was then evaluated. Studies that did not meet the inclusion criteria based on the research question were out listed.
Qualitative evaluation of studies
Qualitative evaluation of studies was performed using the Newcastle–Ottawa Scale, the NOS assigns a maximum of 9 points for the three areas of study group selection, group comparison, and exposure and outcome for the case and group studies [27]. Based on this, articles were classified as high quality (≥ 5) and low quality (< 5).
Extracting the data
After selecting the studies to enter the systematic review and meta-analysis process, the data were extracted and the studies were summarized. An electronic checklist was prepared for this purpose. The various items on the checklist included: the surname of the first author, year of publication and year of the report, sample size, number of patients, prevalence, incidence and mortality of patients.
Statistical analysis
To analyze and combine the results of different studies, in each study, the prevalence of anencephaly was considered as the probability of two-sentence distribution and its variance was calculated through two-sentence distribution. Heterogeneity of studies was assessed using I2 test. A Random effect model was used in case of I2 index above 50%. In this model, parameter changes between studies are also considered in the calculations, so it can be said that the results of this model in heterogeneous conditions can be more generalized than the model with a fixed effect. Due to the large sample size investigated in the study, Begg and Mazumdar rank correlation test was used at a significance level of 0.1 to check the publication bias. Data were analyzed using Comprehensive Meta-Analysis (Version 2) software.
Results
Summary of how articles entered the meta-analysis
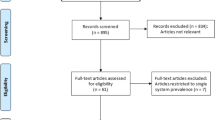
In this study, the statements of Preferred Reporting Items for Systematic Reviews and Meta-Analyzes (PRISMA) were used [26]. In the first stage, 1141 articles (1104 articles in international, 9 articles in Persian databases and 28 studies in reviewing article sources) were found, of which 330 duplicate studies were omitted. 811 studies entered the screening stage and 371 articles were deleted based on the inclusion and exclusion criteria by reviewing the title and abstract of the study. In the next stage (competency assessment), out of the remaining 440 studies from the screening stage, 58 articles were removed by reviewing the full text of the article because it was not relevant to the research. The quality evaluation of 382 articles included in this study was performed using the STROBE checklist, of which 22 studies had poor methodological quality and were deleted. Thus, 360 related studies entered the process of systematic review and meta-analysis (Fig. 1) [28].

Preferred reporting items for systematic reviews and meta-analyses (PRISMA 2020) flow diagram
General characteristics of the studies:
The total sample size of the prevalence studies was 169,407,738 people. The studies were published between 1969 and March 23, 2021. The lowest sample size was related to the study of Castilla-17 et al. (1985) with 1623 people in [29] Colombia and the highest sample size was related to the study of James et al. (1993) with 15,487,449 people in the USA [30]. The surname of the first author, year of publication and year of reporting, place of study, maternal age, sample size, number of cases, prevalence, incidence and attenuation of anencephaly reported in Tables 1, 2 and 3.
The result of the I2 test for the prevalence of anencephaly in different parts of the world indicates a significant heterogeneity between studies (I2 = 99.9), so the data were analyzed by meta-analysis using a random effects model. Due to the high heterogeneity of the studies, sensitivity analysis was performed and the effect of each study on the final result and the degree of heterogeneity were evaluated. Based on Begg and Mazumdar rank correlation tests, the publication bias in the studies with less than 0.1% was not observed. (P = 0.105) (Table 4).
As a result of the combination of studies, the overall estimate of the prevalence of Anencephaly in the world will be 5.1 per ten thousand births (95% confidence interval 4.7–5.5) based on the random effects model (Table 4).
According to different reports of Anencephaly prevalence in different parts of the world, subgroup analysis by different continents (Asia, Europe, USA, Africa and Australia) is reported in Table 2, which has the highest prevalence in Australia with 8.6 per ten thousand births (confidence interval). 95%: 7.7–9.5) (Table 4).
Incidence and mortality of Anencephaly were 8.3 per ten thousand births (95% confidence interval 5.5–9.9) and 5.5 per ten thousand births (95% confidence interval 1.8–15) respectively (Table 5).
Discussion
Neural tube defects (NTDs) are a major congenital structural disorder of the brain and spinal cord that occurs early in pregnancy as a result of defective neural tube closure [9], including abortion, stillbirth, and lifelong disability, as well as high emotional, psychological and economic consequences (138). Many factors, including radiation therapy, drugs, malnutrition, chemicals, and genetic determinants (mutations in folate-responsive or folate-dependent pathways) can adversely affect CNS growth during pregnancy and cause neural tube defects [12].
Anencephaly, which is the partial or complete absence of the brain and skull [3] is one of the most common forms of NTD. The fetus with anencephaly dies or will die in the first few hours after birth [9]. Exposure to methotrexate, aminopterin and valproic acid, maternal characteristics, race, ethnicity, geography, nutritional, biological and poor economic conditions are all risk factors for anencephaly [121, 122].
According to the present systematic review and meta-analysis, the overall prevalence of anencephaly in the world was 5.1 per ten thousand births. The highest prevalence of anencephaly was related to the study of RICHARDS et al. [57] with 230.69 infants with anencephaly per ten thousand births and the lowest prevalence was related to the study of Castilla et al. [31] with zero cases per ten thousand births. The most comprehensive study in terms of sample size was the study of James et al. (1993) with 15,487,449 people in the USA [32] that reported the prevalence of anencephaly at 3.89 per thousand births. Also, the present study estimated the risk of incidence and death due to anencephaly: 8.3 per ten thousand births and 5.5 per ten thousand births worldwide. Bhide et al. (2013) reported the prevalence of anencephaly in India at 2.1 per thousand births through 19 studies [123]. A meta-analysis and systematic review by Bitew et al. (2020) reported the prevalence of NTD in Ethiopia. 63.3 per ten thousand births [124]. Our study is almost in line with these studies and regarding the cause of minor differences between the present study and these studies, we can point out that the number of articles studied in the present study is more (121 articles in the present study versus 19 articles in the study of Bhide et al.) And also, the present study has examined patients with different races and geographical regions in the world.
Due to the change in population structure in different countries and different reports of the prevalence of anencephaly, the need for a detailed study of the prevalence of this defect in different continents in order to pay more attention to the process and its consequences seems inevitable. Therefore, according to the analysis of subgroups according to different continents, the highest prevalence of anencephaly is related to the continent of Australia with 8.6 per ten thousand births and the lowest belongs to the Americas with 4.3 per thousand births.
The results show that in addition to genetics, various environmental factors can also be involved in the development of anencephaly. So far, folic acid is the most important factor in preventing neural tube defects. Reports suggest the use of periovulation fulate supplements significantly reduces the risk of recurrence of anencephaly and other neural tube defects [125].
Regarding the serious nature of anencephaly and its high mortality, genetic counseling, folic acid supplements and prenatal diagnosis of neural tube defects are extremely important or (Given the seriousness of anencephaly and its high mortality rate, genetic counseling, folic acid supplements, and prenatal detection of neural tube abnormalities are critical.). This defect can be diagnosed by screening AFP (alpha-fetoprotein) with a combination of ultrasound and amniocentesis between 14 and 16 weeks of gestation [3, 5]. These studies can provide useful information to health care providers and enrich health care interventions and improve the quality of services and life [126].
Limitations
One of the limitations of this study is that some samples were not based on random selection. Also, non-homogeneous reporting of articles, non-homogeneous method of implementation, and unavailability of the full text of the papers presented at the conference can be added. Such conditions can justify the high heterogeneity reported in the studies, and therefore, if these limitations and differences in the studies did not exist, the heterogeneity analysis could be less.
Conclusion
The results of this study demonstrate that the prevalence of anencephaly in the world is high; therefore, it is necessary for physicians and specialists to emphasize the importance of preventive as well as control and treatment strategies.
Availability of data and materials
Datasets are available through the corresponding author upon reasonable request.
Abbreviations
- NTDs:
-
Neural Tube Defects
- SID:
-
Scientific Information Database
- MESH:
-
Medical Subject Headings
- WoS:
-
Web of Science
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analysis
- STROBE:
-
Strengthening the reporting of observational studies in epidemiology for cross-sectional study
References
Gong TT, Wu QJ, Chen YL, Jiang CZ, Li D, Li J, et al. Changing trends in the prevalence of anencephaly in Liaoning province of Northeast China from 2006–2015: data from a population-based birth defects registry. Oncotarget. 2017;8(32):52846–53.
Pei LJ, Chen G, Song XM, Wu JL, Li CF, Zou JZ, et al. Effect of pathoanatomic diagnosis on the quality of birth defects surveillance in China. Biomed Environ Sci. 2009;22(6):464–71.
Afshar M, Golalipour MJ, Farhud D. Epidemiologic aspects of neural tube defects in South East Iran. Neurosciences. 2006;11(4):289–92.
Golalipour MJ, Mobasheri E, Vakili MA, Keshtkar AA. Epidemiology of neural tube defects in northern Iran, 1998–2003. East Mediterr Health J. 2007;13(3):560–6.
Li Z, Ren A, Zhang L, Ye R, Li S, Zheng J, et al. Extremely high prevalence of neural tube defects in a 4-county area in Shanxi Province, China. Birth Defects Res A. 2006;76(4):237–40.
Lian ZH, Yang HY, Li Z. Neural tube defects in Beijing-Tianjin area of China. Urban-rural distribution and some other epidemiological characteristics. J Epidemiol Community Health. 1987;41(3):259–62.
Golalipour M, Najafi L, Keshtkar A. Neural tube defects in native fars ethnicity in northern Iran. Iran J Public Health. 2010;39(3):116–23.
Xie DH, Liang CB, Xiang YY, Wang AH, Xiong LL, Kong FJ, et al. Prenatal diagnosis of birth defects and termination of pregnancy in Hunan Province, China. Prenat Diagn. 2020;40(8):925–30.
Khattak ST, Khan M, Naheed T, Khattak I, Ismail M. Prevalence and management of anencephaly at Saidu Teaching Hospital, Swat. J Ayub Med Coll Abbottabad JAMC. 2010;22(4):61–3.
Golalipour MJ, Najafi L, Keshtkar AA. Prevalence of anencephaly in Gorgan, northern Iran. Arch Iran Med. 2010;13(1):34–7.
Zhang X, Li S, Wu S, Hao X, Guo S, Suzuki K, et al. Prevalence of birth defects and risk-factor analysis from a population-based survey in Inner Mongolia, China. BMC Pediatr. 2012;12:125.
Jung SC, Kim SS, Yoon KS, Lee JS. Prevalence of congenital malformations and genetic diseases in Korea. J Hum Genet. 1999;44(1):30–4.
Jaruratanasirikul S, Kor-anantakul O, Limpitikul W, Dissaneevate P, Khunnarakpong N, Sattapanyo A. Prevalence of neural tube defect in southern Thailand: a population-based survey during 2009–2012. Child’s Nerv Syst. 2014;30(7):1269–75.
Zhu J, Li X, Wang Y, Mu D, Dai L, Zhou G, et al. Prevalence of neural tube defect pregnancies in China and the impact of gestational age of the births from 2006 to 2008: a hospital-based study. J Maternal-Fetal Neonatal Med. 2012;25(9):1730–4.
Jin L, Jin L, Yu J, Xu Y, Liu H, Ren A. Prevalence of neural tube defects and the impact of prenatal diagnosis in three districts of Beijing, ?China. Paediatr Perinat Epidemiol. 2017;31(4):293–300.
Kant S, Malhotra S, Singh AK, Haldar P, Kaur R, Misra P, et al. Prevalence of neural tube defects in a rural area of north india from 2001 to 2014: a population-based survey. Birth Defects Res. 2017;109(3):203–10.
Liu J, Yang GZ, Zhou JL, Cao SP, Chau DHW, Kung HF, et al. Prevalence of neural tube defects in economically and socially deprived area of China. Childs Nerv Syst. 2007;23(10):1119–24.
Ebrahimi S, Ashkani-Esfahani S, Bagheri F. Prevalence of neural tube defects in Yasuj, South West Iran. Shiraz E Med J. 2013;14(1):54–62.
Ghavami M, Abedinzadeh R. Prevalence of perinatal central nervous system anomalies in East Azarbaijan-Iran. Iran J Radiol. 2011;8(2):79–81.
Kondo A, Akada S, Akiyama K, Arakawa M, Ichi S, Inamoto Y, et al. Real prevalence of neural tube defects in Japan: how many of such pregnancies have been terminated? Congenit Anom. 2019;59(4):118–24.
Tiwari P, Gupta MM. Study of lethal congenital malformations at a tertiary-care referral centre in North India. Cureus. 2020;12(4):e7502.
Imaizumi Y, Yamamura H, Nishikawa M, Matsuoka M, Moriyama I. The prevalence at birth of cogenital malformations at a maternity hospital in Osaka City, 1948–1990. Jinrui idengaku zasshi Jpn J Hum Genet. 1991;36(3):275–87.
Zhang TN, Gong TT, Chen YL, Wu QJ, Zhang Y, Jiang CZ, et al. Time trends in the prevalence and epidemiological characteristics of neural tube defects in Liaoning Province, China, 2006–2015: a population-based study. Oncotarget. 2017;8(10):17092–104.
Seto T, Nakagawa H, Morikawa Y, Nishijo M, Miura K, Kadoshima Y. Trend of congenital anomalies over 20 years ascertained by population-based monitoring in Ishikawa Prefecture, Japan. Congenit Anom. 2003;43(4):286–93.
Fakhri I, Iranfar S, Saeedi Borujeni H, Dini M, Taghavi F. Epidemiology of anencephaly in Kermanshah (1375–180). J Kermanshah Univ Med Sci. 1383;8(4(23)):49–67.
Poureisi M, Nami F, Refahi S. Prevalence of anencephaly and its associated anomalies Tabriz 1376–82. J Sch Med. 1384;63(6):88–96.
Alpoim PN, de Barros Pinheiro M, Junqueira DR, Freitas LG, das Gracas Carvalho M, Fernández AP, et al. Preeclampsia and ABO blood groups: a systematic review and metaanalysis. Mol Biol Rep. 2012;40:2253–61.
Stoll C, Alembik Y, Dott B. Are the recommendations on the prevention of neural tube defects working? Eur J Med Genet. 2006;49(6):461–5.
Castilla EE, Orioli IM. Epidemiology of neural tube defects in South America. Am J Med Genet. 1985;22(4):695–702.
James LM. 2. Maps of birth defects occurrence in the U.S., birth defects monitoring program (BDMP)/CPHA, 1970–1987. Teratology. 1993;48(6):551–646.
Richards ID, Roberts CJ, Lloyd S. Area differences in prevalence of neural tube malformations in South Wales. A study of possible demographic determinants. Br J Prev Soc Med. 1972;26(2):89–93.
Stoll C, Dott B, Alembik Y, Roth MP. Associated malformations among infants with neural tube defects. Am J Med Genet A. 2011;155A(3):565–8.
Szabo N, Gergev G, Valek A, Eller J, Kaizer L, Sztriha L. Birth prevalence of neural tube defects: a population-based study in South-Eastern Hungary. Childs Nerv Syst. 2013;29(4):621–7.
Pietrzyk JJ, Grochowski J, Kańska B. CNS malformations in the Kraków region. I. Birth prevalence and seasonal incidence during 1979–1981. Am J Med Genet. 1983;14(1):181–8.
McDonnell RJ, Johnson Z, Delaney V, Dack P. East Ireland 1980–1994: epidemiology of neural tube defects. J Epidemiol Community Health. 1999;53(12):782–8.
Boyd PA, Wellesley DG, De Walle HE, Tenconi R, Garcia-Minaur S, Zandwijken GR, et al. Evaluation of the prenatal diagnosis of neural tube defects by fetal ultrasonographic examination in different centres across Europe. J Med Screen. 2000;7(4):169–74.
Salvador J, Arigita M, Carreras E, Lladonosa A, Borrell A. Evolution of prenatal detection of neural tube defects in the pregnant population of the city of Barcelona from 1992 to 2006. Prenat Diagn. 2011;31(12):1184–8.
Dolk H, De Wals P, Gillerot Y, Lechat MF, Ayme S, Cornel M, et al. Heterogeneity of neural tube defects in Europe: the significance of site of defect and presence of other major anomalies in relation to geographic differences in prevalence. Teratology. 1991;44(5):547–59.
Khoshnood B, Loane M, de Walle H, Arriola L, Addor MC, Barisic I, et al. Long term trends in prevalence of neural tube defects in Europe: population based study. BMJ (Clin Res Ed). 2015;351:h5949.
Loane M, Dolk H, Morris JK. Maternal age-specific risk of non-chromosomal anomalies. BJOG Int J Obstetr Gynaecol. 2009;116(8):1111–9.
Peake JN, Knowles RL, Shawe J, Rankin J, Copp AJ. Maternal ethnicity and the prevalence of British pregnancies affected by neural tube defects. Birth Defects Res. 2021;113:968–80.
Boyd PA, Tonks AM, Rankin J, Rounding C, Wellesley D, Draper ES. Monitoring the prenatal detection of structural fetal congenital anomalies in England and Wales: register-based study. J Med Screen. 2011;18(1):2–7.
Poretti A, Anbeier T, Zimmermann R, Boltshauser E, Swiss Paediat Surveillance U. Neural tube defects in Switzerland from 2001 to 2007: are periconceptual folic acid recommendations being followed. Swiss Med Wkly. 2008;138(4142):608–13.
Obeid R, Pietrzik K, Oakley GP Jr, Kancherla V, Holzgreve W, Wieser S. Preventable spina bifida and anencephaly in Europe. Birth Defects Res A. 2015;103(9):763–71.
Garne E, Loane M, Dolk H, De Vigan C, Scarano G, Tucker D, et al. Prenatal diagnosis of severe structural congenital malformations in Europe. Ultrasound Obstet Gynecol. 2005;25(1):6–11.
Cadas C, Trichopoulos D, Papadatos K, Kalapothaki V, Sparros L. Prevalence at birth of congenital malformations in Athens, Greece, 1955–1965. Int J Epidemiol. 1978;7(3):251–2.
Loncarek K, Mustac E, Frkovic A, Prodan M. Prevalence of anencephaly in the region of Rijeka, Croatia. Eur J Epidemiol. 2001;17(3):241–4.
Prevalence of neural tube defects in 20 regions of Europe and the impact of prenatal diagnosis, 1980–1986. EUROCAT Working Group. J Epidemiol Community Health. 1991;45(1):52–8.
Prevalence of neural tube defects in 16 regions of Europe, 1980–1983. The EUROCAT Working Group. Int J Epidemiol. 1987;16(2):246–51.
Smithells RW, Sheppard S, Wild J. Prevalence of neural tube defects in the Yorkshire Region. Community Med. 1989;11(2):163–7.
Corona-Rivera JR, Olvera-Molina S, Perez-Molina JJ, Aranda-Sanchez CI, Bobadilla-Morales L, Corona-Rivera A, et al. Prevalence of open neural tube defects and risk factors related to isolated anencephaly and spina bifida in live births from the “Dr. Juan I. Menchaca” Civil Hospital of Guadalajara (Jalisco, Mexico). Congenit Anom. 2021;61(2):46–54.
Stone DH, Smalls MJ, Rosenberg K, Womersley J. Screening for congenital neural tube defects in a high-risk area: an epidemiological perspective. J Epidemiol Community Health. 1988;42(3):271–3.
Carstairs V, Cole S. Spina bifida and anencephaly in Scotland. Br Med J (Clin Res Ed). 1984;289(6453):1182–4.
Rankin J, Glinianaia S, Brown R, Renwick M. The changing prevalence of neural tube defects: a population-based study in the north of England, 1984–96. Northern Congenital Abnormality Survey Steering Group. Paediatr Perinat Epidemiol. 2000;14(2):104–10.
Fleurke-Rozema JH, van Leijden L, van de Kamp K, Pajkrt E, Bilardo CM, Snijders RJ. Timing of detection of anencephaly in The Netherlands. Prenat Diagn. 2015;35(5):483–5.
Sever LE. An epidemiologic study of neural tube defects in Los Angeles County II. Etiologic factors in an area with low prevalence at birth. Teratology. 1982;25(3):323–34.
Limb CJ, Holmes LB. Anencephaly: Changes in prenatal detection and birth status, 1972 through 1990. Am J Obstet Gynecol. 1994;170(5):1333–8.
Groisman B, Barbero P, Mastroiacovo P, Botto LD, Bidondo MP, Liascovich R. Application of quality indicators to data from the National Network of Congenital Anomalies of Argentina. Birth Defects Res. 2019;111(6):333–40.
Rowland CA, Correa A, Cragan JD, Alverson CJ. Are encephaloceles neural tube defects? Pediatrics. 2006;118(3):916–23.
Krajewski AK, Rappazzo KM, Langlois PH, Messer LC, Lobdell DT. Associations between cumulative environmental quality and ten selected birth defects in Texas. Birth Defects Res. 2021;113(2):161–72.
Bronberg R, Groisman B, Bidondo MP, Barbero P, Liascovich R. Birth prevalence of congenital anomalies in the City of Buenos Aires, Argentina, according to socioeconomic level. J Community Genet. 2020;11(3):303–11.
Carmichael SL, Shaw GM, Kaidarova Z. Congenital malformations in offspring of Hispanic and African-American women in California, 1989–1997. Birth Defects Res Part a-Clin Mol Teratol. 2004;70(6):382–8.
Shaw GM, Carmichael SL, Nelson V. Congenital malformations in offspring of Vietnamese women in California, 1985–97. Teratology. 2002;65(3):121–4.
Estevez-Ordonez D, Dewan MC, Feldman MJ, Montalvan-Sanchez EE, Montalvan-Sanchez DM, Rodriguez-Murillo AA, et al. Congenital malformations of the central nervous system in rural Western Honduras: a 6-year report on trends. World Neurosurg. 2017;107:249–54.
Biggar RJ, Mortimer EA Jr, Haughie GE. Descriptive epidemiology of neural tube defects, Rochester, New York, 1918–1938. Am J Epidemiol. 1976;104(1):22–7.
Sargiotto C, Bidondo MP, Liascovich R, Barbero P, Groisman B. Descriptive study on neural tube defects in Argentina. Birth Defects Res A. 2015;103(6):509–16.
Pacheco SS, Braga C, de Souza AI, Figueiroa JN. Effects of folic acid fortification on the prevalence of neural tube defects. Rev Saude Publica. 2009;43(4):565–71.
Janerich DT. Epidemic waves in the prevalence of anencephaly and spina bifida in New York State. Teratology. 1973;8(3):253–6.
Jorde LB, Fineman RM, Martin RA. Epidemiology of neural tube defects in Utah, 1940–1979. Am J Epidemiol. 1984;119(4):487–95.
Groisman B, Gili J, Gimenez L, Poletta F, Bidondo MP, Barbero P, et al. Geographic clusters of congenital anomalies in Argentina. J Community Genet. 2017;8(1):1–7.
Forrester MB, Merz RD, Yoon PW. Impact of prenatal diagnosis and elective termination on the prevalence of selected birth defects in Hawaii. Am J Epidemiol. 1998;148(12):1206–11.
Parks SE, Canfield MA, Ramadhani TA. Importance of including all pregnancy outcomes to reduce bias in epidemiologic studies of neural tube defects–Texas, 1999 to 2005. Birth Defects Res A. 2011;91(3):185–91.
Cragan JD, Gilboa SM. Including prenatal diagnoses in birth defects monitoring: experience of the Metropolitan Atlanta Congenital Defects Program. Birth Defects Res A. 2009;85(1):20–9.
Besser LM, Williams LJ, Cragan JD. Interpreting changes in the epidemiology of anencephaly and spina bifida following folic acid fortification of the U.S. grain supply in the setting of long-term trends, Atlanta, Georgia, 1968–2003. Birth Defects Res Part A Clin Mol Teratol. 2007;79(11):730–6.
de Souza S, Nampo FK, Pestana CR. Major birth defects in the Brazilian side of the triple border: a population-based cross-sectional study. Arch Public Health. 2020;78:61.
Parker SE, Mai CT, Canfield MA, Rickard R, Wang Y, Meyer RE, et al. Updated National Birth Prevalence estimates for selected birth defects in the United States, 2004–2006. Birth Defects Res A. 2010;88(12):1008–16.
Feuchtbaum LB, Currier RJ, Riggle S, Roberson M, Lorey FW, Cunningham GC. Neural tube defect prevalence in California (1990–1994): eliciting patterns by type of defect and maternal race/ethnicity. Genet Test. 1999;3(3):265–72.
Windham GC, Sever LE. Neural tube defects among twin births. Am J Hum Genet. 1982;34(6):988–98.
Aguiar MJ, Campos AS, Aguiar RA, Lana AM, Magalhães RL, Babeto LT. Neural tube defects and associated factors in liveborn and stillborn infants. Jornal de pediatria. 2003;79(2):129–34.
Poletta FA, Rittler M, Saleme C, Campana H, Gili JA, Pawluk MS, et al. Neural tube defects: sex ratio changes after fortification with folic acid. PLoS ONE. 2018;13(3):e0193127.
Castilla EE, Orioli IM, Lopez-Camelo JS, Dutra MD, Nazer-Herrera J, Eclamc. Preliminary data on changes in neural tube defect prevalence rates after folic acid fortification in south America. Am J Med Genet Part A. 2003;123A(2):123–8.
Forrester MB, Merz RD. Prenatal diagnosis and elective termination of neural tube defects in Hawaii, 1986–1997. Fetal Diagn Ther. 2000;15(3):146–51.
Winsor EJ, Brown BS. Prevalence and prenatal diagnosis of neural tube defects in Nova Scotia in 1980–84. Can Med Assoc J. 1986;135(11):1269–73.
Bidondo MP, Liascovich R, Barbero P, Groisman B. Prevalence of neural tube defects and estimation of cases averted in the post-fortification period in Argentina. Archivos argentinos de pediatria. 2015;113(6):498–501.
De Wals P, Tairou F, Van Allen MI, Uh S, Lowry RB, Sibbald B, et al. Reduction in neural-tube defects after folic acid fortification in Canada. N Engl J Med. 2007;357(2):135–42.
Yang J, Carmichael SL, Kaidarova Z, Shaw GM. Risks of selected congenital malformations among offspring of mixed race-ethnicity. Birth Defects Res Part A-Clin Mol Teratol. 2004;70(10):820–4.
Boulet SL, Shin M, Kirby RS, Goodman D, Correa A. Sensitivity of birth certificate reports of birth defects in Atlanta, 1995–2005: effects of maternal, infant, and hospital characteristics. Public Health Rep (Washington, DC: 1974). 2011;126(2):186–94.
McBride ML. Sib risks of anencephaly and spina bifida in British Columbia. Am J Med Genet. 1979;3(4):377–87.
Siffel C, Alverson CJ, Correa A. Analysis of seasonal variation of birth defects in Atlanta. Birth Defects Res A. 2005;73(10):655–62.
Mathews TJ, Honein MA, Erickson JD. Spina bifida and anencephaly prevalence—United States, 1991–2001. MMWR Recomm Rep. 2002;51(Rr-3):9–11.
Cragan JD, Roberts HE, Edmonds LD, Khoury MJ, Kirby RS, Shaw GM, et al. Surveillance for anencephaly and spina bifida and the impact of prenatal diagnosis–United States, 1985–1994. MMWR CDC Surveill Summ Morb Mortal Wkly Rep CDC Surveill Summ. 1995;44(4):1–13.
Canfield MA, Marengo L, Ramadhani TA, Suarez L, Brender JD, Scheuerle A. The prevalence and predictors of anencephaly and spina bifida in Texas. Paediatr Perinat Epidemiol. 2009;23(1):41–50.
Feldman JG, Stein SC, Klein RJ, Kohl S, Casey G. The prevalence of neural tube defects among ethnic groups in Brooklyn, New York. J Chronic Dis. 1982;35(1):53–60.
Naggan L. The recent decline in prevalence of anencephaly and spina bifida. Am J Epidemiol. 1969;89(2):154–60.
Windham GC, Bjerkedal T, Sever LE. The association of twinning and neural tube defects: studies in Los Angeles, California, and Norway. Acta Genet Med Gemellol. 1982;31(3–4):165–72.
Boulet SL, Yang Q, Mai C, Kirby RS, Collins JS, Robbins JM, et al. Trends in the postfortification prevalence of spina bifida and anencephaly in the United States. Birth Defects Res A. 2008;82(7):527–32.
Bupp CP, Sarasua SM, Dean JH, Stevenson RE. When folic acid fails: insights from 20 years of neural tube defect surveillance in South Carolina. Am J Med Genet A. 2015;167(10):2244–50.
Nasri K, Ben Fradj MK, Hamdi T, Aloui M, Ben Jemaa N, Nahdi S, et al. Epidemiology of neural tube defect subtypes in Tunisia, 1991–2011. Pathol Res Pract. 2014;210(12):944–52.
Berihu BA, Welderufael AL, Berhe Y, Magana T, Mulugeta A, Asfaw S, et al. High burden of neural tube defects in Tigray, Northern Ethiopia: Hospital-based study. PLoS ONE. 2018;13(11):e0206212.
Forci K, Alami MH, Bouaiti E, Slaoui M, Alaoui AM, Izgua AT. Prevalence of congenital malformations at the “les Orangers” maternity and reproductive health Hospital of Rabat: descriptive study of 470 anomalies. BMC Pediatr. 2020;20(1):272.
Buccimazza SS, Molteno CD, Dunne TT, Viljoen DL. Prevalence of neural tube defects in Cape Town, South Africa. Teratology. 1994;50(3):194–9.
Omer IM, Abdullah OM, Mohammed IN, Abbasher LA. Research: Prevalence of neural tube defects Khartoum, Sudan August 2014-July 2015. BMC Res Notes. 2016;9(1):495.
Riley MM, Halliday JL, Lumley JM. Congenital malformations in Victoria, Australia, 1983–95: an overview of infant characteristics. J Paediatr Child Health. 1998;34(3):233–40.
Owen TJ, Halliday JL, Stone CA. Neural tube defects in Victoria, Australia: potential contributing factors and public health implications. Aust N Z J Public Health. 2000;24(6):584–9.
Chan A, Robertson EF, Haan EA, Keane RJ, Ranieri E, Carney A. Prevalence of neural tube defects in South Australia, 1966–91: effectiveness and impact of prenatal diagnosis. BMJ (Clin Res Ed). 1993;307(6906):703–6.
Barry Borman G, Smith AH, Keir HJ. Risk factors in the prevalence of anencephalus and spina bifida in New Zealand. Teratology. 1986;33(2):221–30.
Borman B, Cryer C. The prevalence of anencephalus and spina bifida in New Zealand. J Paediatr Child Health. 1993;29(4):282–8.
Safdar OY, Al-Dabbagh AA, AbuElieneen WA, Kari JA. Decline in the incidence of neural tube defects after the national fortification of flour (1997–2005). Saudi Med J. 2007;28(8):1227–9.
Al-Ani ZR, Al-Hiali SJ, Al-Mehimdi SM. Neural tube defects among neonates delivered in Al-Ramadi Maternity and Children’s Hospital, western Iraq. Saudi Med J. 2010;31(2):163–9.
Bener A, Kurdi B, Hoffmann GF, Caksen H, Teebi A. The pattern of neural tube defects in a highly endogamous society: a 25-year incidence trends. J Pediatr Neurol. 2012;10(3):193–8.
Akar N, Cavdar AO, Arcasoy A. High incidence of neural tube defects in Bursa, Turkey. Paediatr Perinat Epidemiol. 1988;2(1):89–92.
Onrat ST, Seyman H, Konuk M. Incidence of neural tube defects in Afyonkarahisar, Western Turkey. Genet Mol Res. 2009;8(1):154–61.
Šípek A, Horáček J, Gregor V, Rychtaříková J, Dzurová D, Mašátová D. Neural tube defects in the Czech Republic during 1961–1999: incidences, prenatal diagnosis and prevalences according to maternal age. J Obstet Gynaecol. 2002;22(5):501–7.
McDonnell R, Delany V, O’Mahony MT, Mullaney C, Lee B, Turner MJ. Neural tube defects in the Republic of Ireland in 2009–11. J Public Health. 2015;37(1):57–63.
Evans DR. Neural-tube defects: importance of a history of abortion in aetiology. BMJ. 1979;1(6169):975–6.
Van Allen MI, Boyle E, Thiessen P, McFadden D, Cochrane D, Chambers GK, et al. The impact of prenatal diagnosis on neural tube defect (NTD) pregnancy versus birth incidence in British Columbia. J Appl Genet. 2006;47(2):151–8.
Kancherla V, Oakley GP Jr. Total prevention of folic acid-preventable spina bifida and anencephaly would reduce child mortality in India: implications in achieving Target 3.2 of the Sustainable Development Goals. Birth Defects Res. 2018;110(5):421–8.
Tanner JP, Salemi JL, Hauser KW, Correia JA, Watkins SM, Kirby RS. Birth defects surveillance in Florida: infant death certificates as a case ascertainment source. Birth Defects Res A. 2010;88(12):1017–22.
Wen SW, Liu SL, Joseph KS, Rouleau J, Allen A. Patterns of infant mortality caused by major congenital anomalies. Teratology. 2000;61(5):342–6.
Dixon M, Kancherla V, Magana T, Mulugeta A, Oakley GP Jr. High potential for reducing folic acid-preventable spina bifida and anencephaly, and related stillbirth and child mortality, in Ethiopia. Birth Defects Res. 2019;111(19):1513–9.
Tort J, Lelong N, Prunet C, Khoshnood B, Blondel B. Maternal and health care determinants of preconceptional use of folic acid supplementation in France: results from the 2010 National Perinatal Survey. BJOG. 2013;120(13):1661-7.
Gucciardi E, Pietrusiak M-A, Reynolds DL, Rouleau J. Incidence of neural tube defects in Ontario, 1986–1999. CMAJ. 2002;167(3):237–40.
Bhide P, Sagoo GS, Moorthie S, Burton H, Kar A. Systematic review of birth prevalence of neural tube defects in India. Birth Defects Res A Clin Mol Teratol. 2013;97(7):437–43.
Bitew ZW, Worku T, Alebel A, Alemu A. Magnitude and associated factors of neural tube defects in ethiopia: a systematic review and meta-analysis. Glob Pediatr Health. 2020;7:2333794X20939423.
Abramsky L, Botting B, Chapple J, Stone D. Has advice on periconceptional folate supplementation reduced neural-tube defects? Lancet. 1999;354(9183):998–9.
Seretis K, Goulis D, Demiri EC, Lykoudis EG. Prevention of Seroma Formation Following Abdominoplasty: A Systematic Review and Meta-Analysis. Aesthet Surg J. 2017;37(3):316–23.
Acknowledgements
This study is the result of research project No. 4000613 approved by the Student Research Committee of Kermanshah University of Medical Sciences. We would like to thank the esteemed officials of the center for financing this study.
Funding
By Deputy for Research and Technology, Kermanshah University of Medical Sciences (IR) (4000613). This deputy has no role in the study process.
Author information
Authors and Affiliations
Contributions
NS and BF and ND contributed to the design, MM statistical analysis, participated in most of the study steps. MM and RF and PM and MK prepared the manuscript. MM and ND and BF and AR and PM and SHSH assisted in designing the study, and helped in the, interpretation of the study. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval was received from the ethics committee of deputy of research and technology, Kermanshah University of Medical Sciences (IR.KUMS.REC.1400.504).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Salari, N., Fatahi, B., Fatahian, R. et al. Global prevalence of congenital anencephaly: a comprehensive systematic review and meta-analysis. Reprod Health 19, 201 (2022). https://doi.org/10.1186/s12978-022-01509-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12978-022-01509-4