
Abstract
Background
Kawasaki disease (KD) is an acute systemic vasculitis of unknown etiology that affects infants and young children but is extremely rare in neonates, especially afebrile KD. We present a case of KD without fever in a neonate and review the literature on KD in neonates.
Case presentation
A newborn female was hospitalized because her peripheral blood leukocytes increased for half a day. The admission diagnosis was considered neonatal sepsis and bacterial meningitis. She had no fever since the admission, but a rash appeared on her face by the 7th day. On day 11 after admission, there was a desquamation on the distal extremities. On day 15 after admission, ultrasound showed non-suppurative cervical lymphadenopathy. Echocardiogram revealed coronary artery aneurysms in both sides. Finally, the patient was diagnosed with incomplete KD (IKD). The follow-up echocardiogram showed that the internal diameter of both coronary arteries returned to normal three months after birth.
Conclusions
Fever, rash, and distal extremity desquamation during the recovery phase are the most common symptoms of IKD. When newborns present with clinical manifestations such as rash, distal extremity desquamation and cervical lymph adenitis and with an increased peripheral blood leukocyte count and progressive increase in platelets simultaneously, the medical staff should be highly alert to the possibility of KD even without fever. The echocardiogram needs to be performed promptly. The incidence of coronary artery lesions is significantly higher if neonatal KD patients miss timely diagnosis and treatment.
Similar content being viewed by others

Background
Kawasaki disease (KD) is an acute systemic vasculitis of unknown etiology that affects infants and young children [1], but is extremely rare in neonates, especially afebrile KD. Data on 130,323 patients from the Japanese nationwide surveys of KD (2001–2012) identified 23 neonatal KD cases, representing 0.02% of KD in patients of all ages [2]. In this study, we present a neonatal case of incomplete KD (IKD) without fever and review the literature on KD in neonates. This report aims to increase awareness of afebrile KD in neonates to reduce the risk of cardiac complications.
Case presentation
A 19-hour-old female patient was transferred to the pediatric ward of China-Japan Friendship Hospital because her peripheral blood leukocytes increased for half a day. She was G1P1, at a gestational age of 40 weeks + 2days, and delivered by cesarean section due to acute intrauterine distress with III-degree contaminated amniotic fluid and slowed fetal heart rate. The Apgar score was 10-point at 1, 5, and 10 min after birth, respectively. The birth weight was 3386 g. The child had no fever, no irritability with a high-pitched cry, no convulsions, and no groans or vomiting after admission. Her temperature was 36.5 ℃, pulse 140/minute, respiration 40/minute, BP 80/55 mmHg, capillary refill less than two seconds. The face and trunk were light yellow. The bregma was bulged and the pressure was slightly higher. The neck resistance was suspiciously positive. The muscular tension in the limbs was normal, and the primitive reflexes were derived.
Laboratory investigations on the day of birth showed white blood cell (WBC) was 41.33 × 109/L (neutrophils 75.3%, lymphocytes 15.4%, monocytes 7.8%), red blood cell (RBC) was 4.65 × 1012/L, hemoglobin was 167 g/L, platelet (PLT) was 266 × 109/L, and C-reactive protein (CRP) was 6.86 mg/L. Total bilirubin was 124.11 µmol/L and direct bilirubin was 10.4 µmol/L. The cerebrospinal fluid contained total cells was 15 × 106/L, WBC was 13 × 106/L (multinuclear 85%, mononuclear 15%), protein 0.603 g/L, glucose 4.48 mmol/L (peripheral blood glucose: 5.1 mmol/L), and LDH 96 IU/L. Hepatitis B virus, hepatitis C virus, human immunodeficiency virus, treponema pallidum antibody and TORCH were all negative. Rheumatoid factor was normal. Chest X-ray, cranial ultrasound and abdominal ultrasound were unremarkable. Amplitude integration EEG showed no abnormal discharges. The patient was suspiciously diagnosed with neonatal sepsis and bacterial meningitis upon admission. Meropenem and vancomycin were given to control the infection. Mannitol was used to lower the intracranial pressure, and dexamethasone was used to prevent adhesions. On day 2 of hospitalization, intravenous immunoglobulin (IVIG) was used for three days (total dose 2 g/kg) as supportive therapy.
On day 4, cerebrospinal fluid was rechecked and contained total cells 6 × 106/L, WBC 5 × 106/L, protein 0.758 g/L, glucose 2.21 mmol/L (peripheral blood glucose 4.9 mmol/L), and LDH 76 IU/L. She had transient hyponatremia (127 mmol/L). Bacterial cultures from blood and cerebrospinal fluid were sterile.
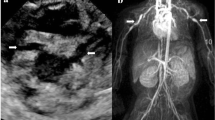
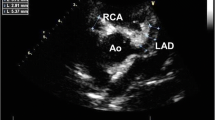
The patient had no fever since admission, but a rash appeared on her face by the 7th day and lasted for five days. The PLT reached from 603 × 109/L on day 7 to 1345 × 109/L on day 12 (Table 1). Distal extremity desquamation began on day 11 and continued for ten days (Fig. 1). However, other manifestations including conjunctivitis, erythematous dry lips, red raspberry tongue and swollen extremities did not appeared. Low molecular dextran was given to reduce blood viscosity, enoxaparin sodium was given for anticoagulation, and dipyridamole and low-dose aspirin (5 mg/kg) were administered for anti-platelet aggregation. On the 15th day of the illness, ultrasound showed non-suppurative cervical lymphadenopathy. Echocardiogram showed that the internal diameter of the proximal segment of the left main coronary artery (LMCA) was 5.9 mm (Z = 11.40), the internal diameter of the left anterior descending coronary artery (LAD) was 2.4 mm (Z = 5.19) and the internal diameter of the right coronary artery (RCA) was 3.1 mm (Z = 8.07) (Fig. 2). Electrocardiogram was normal. Moreover, no abnormal blood flow was found in the arteries of the upper and lower extremities. No thrombus was found in the deep veins. Finally, the patient was diagnosed with IKD. Low-dose aspirin and dipyridamole were given to prevent platelet aggregation continuously.

Sheet-like desquamation of extremities emerged on day 11. (A) Skin on toes peeling. (B) Skin on fingers peeling

Echocardiography on 15th day after birth revealed coronary artery aneurysms in the left coronary artery
On 21 days after admission, the blood analyses showed WBC was 10.17 × 109/L (neutrophils was 17.2%, lymphocytes was 61.2%, monocytes was 12.1%), RBC was 2.69 × 1012/L, hemoglobin was 90 g/L, PLT was 499 × 109/L, and CRP was < 2.5 mg/L. Echocardiogram revealed LMCA of 2.6 mm (Z = 4.29), LAD of 2.1 mm (Z = 4.13), and RCA of 2.3 mm (Z = 4.95).
The patient was discharged with low-dose aspirin and dipyridamole after 21 days in the hospital. Regular follow-up was carried out every 2–4 weeks after discharge. Echocardiogram revealed LMCA of 2.0 mm (Z = 1.69) and RCA of 1.7 mm (Z = 1.78) three months after birth (Table 2).
Discussion
KD is an acute febrile condition seen in children. The diagnostic criteria for KD are fever, bilateral bulbar conjunctival injection, changes in the lips and oral cavity, rash, changes in the peripheral extremities, and non-suppurative cervical lymphadenopathy. Fever is no longer necessary for the diagnosis of KD, according to the sixth revised edition of the Japanese diagnostic criteria [3]. Statistically, neonates with KD have a higher risk of incomplete presentation than older children [2].
The number of IKD cases increased yearly from 10% to the current level, which is greater than 20% of all KD patients [3]. Fever, redness, and swelling of the extremities are the most common symptoms of IKD [4]. We searched case reports of neonatal KD published in English from January 1, 2000 to February 18, 2023 with the search formula: ((“Mucocutaneous Lymph Node Syndrome“[Mesh]) OR (((Kawasaki Syndrome[Title/Abstract]) OR (Lymph Node Syndrome, Mucocutaneous [Title/Abstract])) OR (Kawasaki Disease [Title/Abstract]))) AND ((“Infant, Newborn“[Mesh]) OR (((((((((Infants, Newborn) OR (Newborn Infant)) OR (Newborns)) OR (Newborn)) OR (Neonate)) OR (Neonates)). The inclusion criteria were cases of KD in newborns and the diagnosis met the Revision of diagnostic guidelines for Kawasaki disease (6th revised edition) [3]. The exclusion criteria were duplication or literature with incomplete case information (no clinical features, no laboratory findings and outcomes). Nineteen cases in 15 papers were analyzed [2, 5,6,7,8,9,10,11,12,13,14,15,16,17,18] (Table 3). IKD accounted for 68.4% (13/19). The clinical manifestations included rash in 94.7% (18/19), changes in the terminal extremities in 78.9% (15/19), fever in 78.9% (15/19), erythematous changes in the lips and oral mucosa in 68.4% (13/19), bilateral non-purulent conjunctivitis in 42.1% (8/19), cervical lymph adenitis in 10.5% (2/19), and coronary artery lesions (CALs) in 89.5% (17/19). Laboratory tests showed that elevated CRP accounted for 63.2% (12/19) and PLT > 300 × 109/L accounted for 57.9% (11/19) (Table 4).
There were four patients with no fever among the 19 neonatal KD cases in our literature review. Only one afebrile patient was diagnosed as IKD purely based on CALs [11]. The other three afebrile patients [9–10], including the present case, had the same clinical manifestations, such as rash and periungual desquamation. In addition to the above-mentioned manifestations, conjunctival congestion, changes in the lips, and extremity edema were also observed in cases 6 and 7 [9–10] (Table 3).
The immune system of newborns is in a special developmental stage, which might lead to heterogeneity in neonatal KD and explain the higher incidence of IKD in neonates than older children. In this case, the patient did not have fever and other clinical manifestations, such as bilateral bulbar conjunctival injection, changes in the lips and oral cavity, probably associated with the early stage of neonate and the impact of early use of IVIG and dexamethasone.
To date, the etiology of KD is not clear. Previous studies suggested that KD is triggered by an infectious agent based on its occurrence in epidemiological clusters, seasonal variation, and a very low risk of recurrence [19]. Other research suggested that neonatal KD could be associated with sepsis and pneumonia [20, 21]. Although the patient’s blood culture and cerebrospinal fluid were all sterile, the infection could not be excluded since abnormally elevated WBC and III-degree contaminated amniotic fluid at birth. We could not distinguish exactly whether this case was a KD secondary to systemic infection or just a KD case from the beginning.
CALs are the primary serious complication affecting the prognosis of KD. Several studies suggested that infants under the age of 6 months not only present more commonly with IKD, but are also at higher risk for coronary artery abnormalities and death [8]. In the 19 cases of neonatal KD mentioned above, CALs occurred in 89.5% in 19 neonates and 75% in the four cases of afebrile neonatal KD. 61.1% (11/18) of the patients with CALs had a favorable prognosis after using IVIG. Although this patient initially presented with medium to large coronary aneurysms, the internal diameter of the coronary arteries returned to normal after three months by IVIG treatment on 2nd day after birth. The 24th Nationwide Surveillance in Japan reported that approximately 9%, 25%, and 35% of KD patients received the first IVIG treatment on the 3rd, 4th, and 5th days of illness, respectively, and the prevalence of CALs were lower than before [3]. Consistent with this finding, our case suggests that early use of IVIG might be beneficial for long-term prognosis in KD.
Conclusions
This case report and review of the literature suggest a relatively higher incidence of IKD in neonates. Therefore, when newborns present with rash, terminal changes in the extremities or cervical lymph adenitis, increased peripheral blood leukocyte count and CRP, or progressive increase in platelets, the medical staff should be highly alert to the possibility of KD even without fever. Echocardiogram needs to be performed promptly. The incidence of CALs in neonatal KD is significantly higher. Timely diagnosis and treatment are essential for neonatal KD to improve the prognosis.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AB:
-
Abnormal
- CAAs:
-
Coronary artery aneurysms
- CALs:
-
Coronary artery lesions
- CRP:
-
C-reactive protein
- ESR:
-
Erythrocyte sedimentation rate
- IKD:
-
Incomplete Kawasaki disease
- IVIG:
-
Intravenous immunoglobulin
- KD:
-
Kawasaki disease
- LAD:
-
Left anterior descending
- LCA:
-
Left coronary artery
- PCT:
-
Procalcitonin
- PLT:
-
Platelet
- RBC:
-
Red blood cell
- RCA:
-
Right coronary artery
- WBC:
-
White blood cell
References
Burns JC, Glode MP. Kawasaki syndrome. Lancet. 2004;364(9433):533–44.
Hangai M, Kubota Y, Kagawa J, Yashiro M, Uehara R, Nakamura Y, et al. Neonatal Kawasaki disease: case report and data from nationwide survey in Japan. Eur J Pediatr. 2014;173(11):1533–6.
Kobayashi T, Ayusawa M, Suzuki H, Abe J, Ito S, Kato T et al. Revision of diagnostic guidelines for Kawasaki disease (6th revised edition). Pediatr Int. 2020; 62(10):1135-8.
McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, Gewitz M, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation. 2017;135(17):e927–99.
Li C, Du Y, Wang H, Wu G, Zhu X. Neonatal Kawasaki disease: case report and literature review. Med (Baltim). 2021;100(7):e24624.
Tomiko T, Shigetoyo K, Kunihiko T, Futoshi K. Successful infliximab treatment for refractory Kawasaki disease in a neonate: a case report and literature review. Prog Pediatr Cardiology. 2020; 101255.
Zhao QM, Liang XC, Wu L, Liu F. Neonatal Kawasaki disease with multiple arterial aneurysms: a case report. Pediatr Rheumatol Online J. 2020;18(1):50–4.
Altammar F, Lang B. Kawasaki disease in the neonate: case report and literature review. Pediatr Rheumatol Online J. 2018;16(1):43–9.
Cristina MRDM, Riccardo P, Lenora G, Rosa HU, Claudia BP. Onset of Kawasaki disease immediately after birth. Case Rep Perinat Med. 2018; 7(2).
Okazaki K, Matsui K, Takahashi N, Miura M, Kondo M. Kawasaki disease in a preterm neonate: case report and cytokine profile. Pediatr Int. 2018;60(11):1037–9.
Parashar R, Lysecki PJ, Mondal T. Diffuse coronary artery dilatation in a neonate: a case report. J Neonatal Perinatal Med. 2013;6(3):263–6.
Nasir A, Al Tatari H, Hamdan MA. Very high serum ferritin levels in three newborns with Kawasaki-like illness. Paediatr Child Health. 2012;17(4):201–4.
Mitchell S, Francis J, Burgner D. Kawasaki Disease in the neonate period. J Pediat Inf Dis-ger. 2011;6(4):265–7.
Karia VR, Hescock GC, Gedalia A, Ross-Ascuitto N. Successful emergent coronary thrombolysis in a neonate with Kawasaki’s disease. Pediatr Cardiol. 2010;31(8):1239–42.
Nakagawa N, Yoshida M, Narahara K, Kunitomi T. Kawasaki disease in an 8-day-old neonate. Pediatr Cardiol. 2009;30(4):527–9.
Thapa R, Pramanik S, Dhar S, Kundu R. Neonatal Kawasaki disease with multiple coronary aneurysms and thrombocytopenia. Pediatr Dermatol. 2007;24(6):662–3.
Bhatt M, Anil SR, Sivakumar K, Kumar K. Neonatal Kawasaki disease. Indian J Pediatr. 2004;71(4):353–4.
Stanley TV, Grimwood K. Classical Kawasaki disease in a neonate. Arch Dis Child Fetal and Neonatal Ed. 2002;86(2):F135–6.
Kumrah R, Vignesh P, Rawat A, Singh S. Immunogenetics of Kawasaki disease. Clin Rev Allergy Immunol. 2020;59(1):122–39.
Takeuchi A, Sugino N, Namba T, Tamai K, Nakamura K, Nakamura M, et al. Neonatal sepsis and Kawasaki disease. Eur J Pediatr. 2022;181(8):2927–33.
Kawamura Y, Miura H, Saito K, Kanno T, Yokoyama T, Aizawa Y, et al. An atypical case of Kawasaki disease with severe pneumonia in a neonate. BMC Pediatr. 2022;22(1):132–7.
Acknowledgements
Not applicable.
Funding
No funds were needed to publish this case.
Author information
Authors and Affiliations
Contributions
Mingjun Shen, Die Liu and Jing Zhang conceptualized and designed the work, drafted the initial manuscript, and reviewed and revised the manuscript. Fang Ye acquired, analyzed and interpreted patient’s data for diagnosis of KD. Jun Wang reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved and registered by the Bioethics Committee of China-Japan Friendship Hospital (accept no. 2019-162-K111), and it was performed by the Declaration of Helsinki. Also, informed consent to publish was obtained from the parents of the patient.
Consent for publication
Not applicable.
Competing interests
The authors declared that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shen, M., Liu, D., Ye, F. et al. Kawasaki disease in neonates: a case report and literature review. Pediatr Rheumatol 22, 23 (2024). https://doi.org/10.1186/s12969-024-00959-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12969-024-00959-3