
Abstract
Background
The purpose of this meta-analysis was to comprehensively investigate the diagnostic ability of 1.5 T and 3.0 T whole heart coronary angiography (WHCA) to detect significant coronary artery disease (CAD) on X-ray coronary angiography.
Methods
A literature search of electronic databases, including PubMed, Web of Science Core Collection, Cochrane advanced search, and EMBASE, was performed to retrieve and integrate articles showing significant CAD detectability of 1.5 and 3.0 T WHCA.
Results
Data from 1899 patients from 34 studies were included in the meta-analysis. 1.5 T WHCA had a summary area under ROC of 0.88 in the patient-based analysis, 0.90 in the vessel-based analysis, and 0.92 in the segment-based analysis. These values for 3.0 T WHCA were 0.94, 0.95, 0.96, respectively. Contrast-enhanced 3.0 T WHCA had significantly higher specificity than non-contrast-enhanced 1.5 T WHCA on a patient-based analysis (0.87, 95% CI 0.80–0.92 vs. 0.74, 95% CI 0.64–0.82, P = 0.02). There were no differences in diagnostic performance on a patient-based analysis by use of vasodilators, beta-blockers or between Asian and Western countries.
Conclusions
The diagnostic performance of WHCA was deemed satisfactory, with contrast-enhanced 3.0 T WHCA exhibiting higher specificity compared to non-contrast-enhanced 1.5 T WHCA in a patient-based analysis. There were no significant differences in diagnostic performance on a patient-based analysis in terms of vasodilator or beta-blocker use, nor between Asian and Western countries. However, further large-scale multicentre studies are crucial for the widespread global adoption of WHCA.
Similar content being viewed by others

Background
Coronary artery disease (CAD) is a primary cause of mortality in the United States, and ranks as the third most common cause of death globally, responsible for 17.8 million deaths annually [1]. X-ray coronary angiography is utilized to diagnose CAD; however, it is an invasive procedure, and its complications cannot be overlooked. Presently, coronary computed tomography (CT) is widely employed in clinical practice as a non-invasive examination method. Coronary artery CT boasts a high negative predictive value and is efficacious in ruling out CAD [2]. Furthermore, there is evidence that evaluating coronary plaque [3] and implementing CT-based strategies can enhance prognosis [4]. Additionally, cost-effectiveness is also favorable in low to moderate prevalence rates [5]. Despite the utility of coronary CT being extremely high, it does have several drawbacks including radiation exposure, the administration of contrast agent, and difficulties in utilizing the method for highly calcified coronary arteries.
Whole heart coronary magnetic resonance angiography (WHCA) is considered as an alternative to coronary CT, possessing advantages over CT such as no radiation exposure, less susceptibility to coronary calcification [6]. Prior meta-analyses have been conducted on the diagnostic capabilities of WHCA [7, 8]. However, it should be noted that non-contrast imaging is recommended for 1.5 T WHCA, whereas contrast imaging is recommended for 3.0 T WHCA. The rationale behind this recommendation is that in 1.5 T WHCA, it is difficult to achieve increased arterial contrast with the administration of contrast agents [9]. In contrast, in 3.0 T WHCA, the use of steady state free precession (SSFP) is challenging due to banding artifacts caused by specific absorption ratio (SAR) limitations and B1 inhomogeneity. Therefore, it is generally advised to use gadolinium based contrast agents in gradient echo (GRE) sequence for 3.0 T WHCA [10]. To date, no meta-analysis has compared the diagnostic accuracy of non-contrast 1.5 T WHCA and contrast-enhanced 3.0 T WHCA. There is also debate about the need for premedication (vasodilators and beta-blockers) prior to imaging and differences in utilization by region (Western vs. Asian countries). These issues have not been evaluated in prior meta-analyses. Therefore, the purpose of this study was to perform a comprehensive meta-analysis on the diagnostic accuracy of WHCA for detecting significant CAD on X-ray coronary angiography and to evaluate the differences in magnetic field strength and use of contrast agent, with and without premedication, and including differences in diagnostic accuracy by region.
Methods
A systematic literature search was conducted in accordance with the guidelines established by the Cochrane Collaboration and the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) on November 10, 2022, utilizing databases such as PubMed, Web of Science Core Collection, Cochrane advanced search, and EMBASE. Search terms utilized included “whole heart coronary magnetic resonance angiography”, “WHCA”, “MRI”, “coronary artery disease”, “diagnostic accuracy” (as outlined in Additional file 1: Material S1). Two evaluators (SK and MA) independently assessed the validity of all titles and abstracts, followed by a review of the relevant complete peer-reviewed studies; any discrepancies were resolved by a third reviewer. The protocol for this study was registered with the University Medical Information Network (registration number: UMIN000050172) and did not require institutional review board approval as it was a meta-analysis and did not involve clinical patient information. Both prospective and retrospective studies that included diagnostic performance of coronary WHCA at 1.5 T and 3.0 T for detecting significant CAD on X-ray coronary angiography were included for data extraction, while literature such as case reports, animal studies, and non-English language articles were excluded.
Outcome measures
The primary objective of this meta-analysis was to estimate the diagnostic performance of coronary WHCA for significant coronary artery stenosis in known or suspected CAD using X-ray coronary angiography as the gold standard and to compare its value at 1.5 T and 3.0 T. Two reviewers (SK and MA) were invited to review the results of the studies, extracting the following study characteristics: author name, year of publication, country, patient disease, age, gender, magnetic resonance imaging (MRI) parameters such as magnetic field strength, sequence used, producer of MRI equipment, MRI coil information, use of gadolinium contrast, and examination time. Definition of significant CAD on X-ray coronary angiogram was also investigated. A meta-analysis of the diagnostic accuracy of coronary WHCA for significant coronary artery stenosis was performed using summary receiver operating characteristics (ROC) analysis. The analysis included the following. (1) All studies including the diagnostic performance of 1.5 T and 3.0 T were used to compare their diagnostic performance. The following sub-analyses were performed: 1. non-contrast enhanced 1.5 T WHCA vs. contrast enhanced 3.0 T WHCA, 2. drug administration (vasodilators and beta-blockers), 3. Comparison between Asian and Western countries. The Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) were utilized to assess risk of bias [11].
Data integration and statistical analysis
Meta-analysis was conducted utilizing RevMan 5.41 (Cochrane Collaboration, London, UK) and R Statistical Software (v3.5.1, Boston, MA, USA). The diagnostic accuracy of WHCA was evaluated through summary ROC analysis. Three levels of diagnostic accuracy were analyzed: patient-based, vessel-based, and segment-based. Sensitivity and specificity were derived from ROC curves and the diagnostic performance was compared at magnetic field strengths of 1.5 T and 3.0 T. A random-effects model was employed to estimate imaging time by coil type. The inverse variance method was utilized to weight each study in the meta-analysis. Heterogeneity was indicated by I2, with 0% indicating no heterogeneity and 100% indicating strong heterogeneity [12]. P < 0.05 was considered statistically significant.
Results
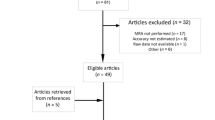
Ultimately, 34 eligible papers were selected from a pool of 140 candidate papers, and data from 1899 patients were consolidated (Fig. 1) [13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45]. The characteristics of the included studies are summarized in Table 1. The publication years of these studies ranged from 2005 to 2022; 23 of these studies utilized 1.5 T MRI technology [13,14,15,16,17,18,19,20,21,22,23,24,25, 28, 30, 31, 33,34,35,36,37, 44,45,46], while 11 utilized 3.0 T technology [26, 27, 29, 32, 38,39,40,41,42,43, 45]. The countries of publication were diverse, with China having 11 reports [18, 26, 32, 34, 38, 39, 41,42,43,44,45], Germany having 8 reports [13, 15, 19, 25, 27, 29, 31, 35], Japan having 7 reports [14, 17, 24, 28, 30, 37, 40], United Kingdom [21, 46] having two reports and various other countries such as the United States [20], Korea [16], Switzerland [36], Portugal [33], Belgium [23], and Turkey [22] having one report each. In terms of study design, one study employed a prospective multicenter design [28], while 19 employed prospective single-center designs [13,14,15, 17, 21, 23, 25,26,27, 29,30,31,32, 37,38,39, 43,44,45,46]. The remaining studies were retrospective in nature. The MRI sequences utilized in these studies were steady state free precession [13,14,15,16,17,18,19,20,21,22,23,24,25, 28, 30, 31, 33,34,35,36,37, 40, 44, 46] or gradient-echo [26, 27, 29, 32, 38, 39, 41,42,43, 45]. Twenty-three studies demonstrated the diagnostic capability of 1.5 T WHCA [13,14,15,16,17,18,19,20,21,22,23,24,25, 28, 30, 31, 33,34,35,36,37, 44, 46], three of which used contrast [31, 33, 36] (Table 2). That is, the majority of studies (87%; 20/23) performed 1.5 T WHCA imaging without contrast. Eleven studies showed diagnostic performance of 3.0 T WHCA [26, 27, 29, 32, 38,39,40,41, 43, 45], of which two studies used non-contrast imaging [29, 45]. In other words, the majority of studies (82%, 9/11) evaluated the diagnostic performance of 3.0 T with gadolinium contrast administration. In terms of sequence used, all studies at 1.5 T used SSFP (100%, 23/23). In contrast, only one study at 3.0 T used SSFP [40], while the others used GRE-based sequencing (91%, 10/11). The information of pre-pulse and fat suppression was summarized in Table 2. The definition of significant CAD was luminal narrowing ≥ 50% in almost all studies (97%, 33/34). Only one study defined significant CAD as “luminal narrowing ≥ 90%, ≥ 50% in LMT, or FFR ≤ 0.80” [33]. In terms of cardiac coils, 32-channel coils were employed in 11 reports [29,30,31,32, 37, 39, 40, 42, 44,45,46]. Vasodilators such as sublingual nitroglycerin were utilized in 18 studies [14, 15, 17, 18, 24, 26, 27, 29,30,31,32,33,34,35, 37, 40, 41, 46], and beta-blockers were utilized in 12 studies [18, 19, 22, 26, 29, 32,33,34,35, 41, 43, 46]. The results of QUADAS-2 are summarized in Additional file 1: Material S2.

Preferred reporting items for systematic reviews and meta-analyses flow diagram
Diagnostic accuracy of WHCA—1.5 T vs. 3.0 T
Figure 2 illustrates the summary receiver operating characteristic analysis of the ability of 1.5 T WHCA to detect significant stenosis when the gold standard is significant stenosis on X-ray coronary angiography. The area under the curve was 0.88 for patient-based analysis (N = 979 patients from 16 studies), 0.90 for vessel-based analysis (N = 2905 vessels from 15 studies), and 0.92 for segment-based analysis (N = 7171 segments from 16 studies). Figure 3 illustrates the summary receiver operating characteristic analysis of the ability of 3.0 T WHCA to detect significant stenosis. The area under the curve was 0.94 for patient-based analysis (N = 604 patients from 9 studies) and 0.95 for vessel-based analysis (N = 2032 vessels from 9 studies), and 0.96 for segment-based analysis (N = 4795 segments from 8 studies). Table 3 summarizes the sensitivity and specificity calculated from the receiver operating characteristic curves. The 3.0 T WHCA technique had significantly higher sensitivity in the segment-based analysis compared to 1.5 T (0.88, 95% confidence interval (CI) 0.84–0.91 vs. 0.80, 95% CI 0.72–0.86, P = 0.04). The individual diagnostic performance of each study is summarized in Additional file 1: Materials S3–S5.

Summary ROC curve of 1.5 T whole-heart coronary MRA

Summary ROC curve of 3.0 T whole-heart coronary MRA
Sub-analysis of diagnostic performance of WHCA
As previously stated, 1.5 T WHCA is typically performed without the use of gadolinium contrast, while 3.0 T WHCA is typically performed with contrast administration. Keeping this in mind, we conducted a comparison of the diagnostic performance of non-contrast 1.5 T WHCA and contrast-enhanced 3.0 T WHCA. The 3.0 T WHCA technique demonstrated significantly higher specificity compared to the non-contrast enhanced 1.5 T WHCA on a patient-based analysis (Table 4). Additionally, we performed a subgroup analysis based on the presence or absence of drug use and geographical difference (Asian and Western countries). There were no differences in diagnostic performance on a patient-based analysis were observed in the use of vasodilators and beta-blockers (Tables 5, 6) or comparison between Asian and Western countries (Table 7). However, in the vessel-based analysis, the sensitivity of studies using the vasodilator was lower than those not using it (P = 0.03) (Table 5). Mean heart rate in the study with beta-blocker administration was 64.6 bpm (95% CI 63.9–65.3 bpm) and in the study without beta-blocker administration mean heart rate was 68.6 bpm (95% CI 67.9–69.2 bpm), a significant difference was found between the two groups (P < 0.001). There was a significant difference in heart rate between trials with and without beta-blockers, but no difference in diagnostic performance. In the regional analysis, the body mass index (BMI) reported in Western countries was significantly higher than that in Asian countries (27.0 kg/m2, 95% CI 26.6–27.3 vs. 23.7 kg/m2, 95% CI 23.3–24.1, P < 0.001).
Discussion
The main findings of this study are as follows: Receiver operating characteristic analysis showed that the 3 T field strength was superior in detecting significant coronary arteries compared to the 1.5 T. In addition, a direct comparison of non-contrast 1.5 T WHCA and contrast-enhanced 3.0 T WHCA was performed as a practical comparison, with the latter showing significantly higher specificity on a patient-based analysis. Subgroup analyses also showed no significant difference in diagnostic performance of 1.5 T WHCA in terms of the use of vasodilators and beta-blockers on a patient-based analysis. Although BMI was higher in Western patients compared to Asian patients, there was no difference in the diagnostic performance of the 1.5 T WHCA. These results suggest that WHCA is useful for noninvasive detection of significant CAD.
WHCA is well-established as a non-invasive method for the screening of CAD and possesses a number of advantages, such as the absence of ionizing radiation exposure, decreased susceptibility to calcification, and the lack of a requirement for contrast agent administration at 1.5 T. However, there is limited evidence for its clinical utility. To date, numerous studies have utilized X-ray coronary angiography as the gold standard, yet the majority of these studies have been conducted on small patient populations at a single institution. The only prospective, multi-center study was conducted in Japan and reported a sensitivity of 88% and specificity of 72% for 1.5 T WHCA [28]. Unfortunately, there have been no further multi-center studies since. Additionally, 3 T MR is often performed utilizing the gradient echo method, which necessitates the administration of a contrast agent [26, 27, 32, 38,39,40,41,42,43]. After contrast agent administration, 3 T WHCA provides a higher signal-to-noise ratio compared to 1.5 T WHCA and has been reported to have high diagnostic performance for the detection of coronary artery stenosis. However, one of the major advantages of MRI, the lack of requirement for contrast agent administration, is lost with 3 T WHCA. Recently, attempts have been made to perform non-contrast 3 T WHCA imaging, with promising results, but the number of reports on this technique is limited [29, 45]. The administration of a gadolinium contrast agent is necessary for 3 T WHCA due to the difficulties in using SSFP caused by SAR limitations and banding artifacts resulting from B1 inhomogeneity. Therefore, GRE is generally the preferred imaging sequence, but in order to achieve sufficient vascular contrast, the administration of gadolinium contrast is required [10]. As the imaging methods and diagnostic accuracy of 1.5 T and 3 T coronary WHCA are fundamentally different, separate meta-analyses are required. However, meta-analyses reported to date have included a mixture of 1.5 T and 3 T WHCA systems [7, 8]. Therefore, the primary objective of the present meta-analysis was to compare the diagnostic performance of WHCA with two different magnetic field strengths. Our results demonstrated that 3 T provided superior diagnostic performance when compared to 1.5 T, however, the number of reports regarding 3 T WHCA was small and there was a large bias in the countries and facilities where the studies were conducted (8/11 reports from China), making it difficult to generalize the obtained data. Further evidence accumulation and large-scale, prospective, multi-center studies are needed in the future to further investigate the diagnostic performance of 3 T MR. The clinical significance of the difference in diagnostic performance between 1.5 and 3.0 T WHCA is debatable. While 3.0 T WHCA exhibits slightly superior diagnostic performance, its major disadvantage of requiring the administration of gadolinium-based contrast agents negates its advantages over coronary CTA. Therefore, 1.5 T WHCA, which has unique benefits such as no radiation exposure and no need for gadolinium-based contrast administration, may be more clinically practical.
Another significant clinical query revolves around the necessity of nitroglycerin or beta-blockers in WHCA. Subgroup analyses of trials including and excluding both medications demonstrated comparable diagnostic performance in patient-based analyses, irrespective of drug usage (Tables 5, 6). Notably, there was no disparity in diagnostic performance, despite lower heart rates observed in studies employing beta-blockers. This could be attributed to the minimal absolute difference in heart rates (64.6 bpm vs. 68.6 bpm). Furthermore, although no distinctions were found in patient-based or segment-based analyses concerning vasodilator use, the sensitivity of studies employing vasodilators was lower than those that did not, as revealed by the vessel-based analysis (0.81 vs 0.91, P = 0.03, Table 5). Although the exact cause remains unclear, the vessel-based analysis exhibited higher AUC values for both groups, with an AUC of 0.90 for studies utilizing vasodilators and an AUC of 0.92 for studies without vasodilators. Given the trade-off relationship between sensitivity and specificity, the AUC does not appear to indicate a substantial disparity in diagnostic performance between studies with and without vasodilator use.
In addition, it is posited that coronary MRA is utilized by numerous institutions in Asian countries, with fewer employing it in Western countries. In light of this, we conducted a subgroup analysis of 1.5 T WHCA, taking into account the possibility of reduced diagnostic performance in larger patients due to their larger body size in Western countries (3.0 T studies could not be analyzed due to their small number). The findings indicated that BMI was significantly higher in patients from Western countries, but no significant differences in diagnostic performance were discerned between the two groups (Table 7). This suggests that WHCA can maintain its diagnostic efficacy even in patients with larger body mass.
The assessment of diagnostic efficiency between WHCA and coronary CT is a highly pertinent clinical inquiry. Nevertheless, there are few studies that have directly compared the two modalities. For instance, it has been demonstrated that WHCA is more diagnostically reliable than coronary CT in highly calcified segments of coronary arteries with calcification scores of 100 or above [18]. Conversely, other studies have found that 3 T WHCA has comparable diagnostic accuracy to CTA [43, 47]. Although such small-scale studies are dispersed, there is a lack of large-scale, coherent data, and it is challenging to statistically validate the comparison in this meta-analysis. Regardless, it is incontrovertible that coronary CT is the primary test for screening for CAD, owing to its spatial resolution, imaging duration, and reported high diagnostic accuracy. WHCA may serve as a viable alternative for patients for whom coronary CT cannot be performed, such as those with iodine allergies. Additionally, it should be utilized assertively in young patients who should not be exposed to radiation, female patients, and patients with coronary artery malformations [48] or coronary aneurysms in Kawasaki disease [49], which can be adequately evaluated with MRI resolution. Further accumulation of evidence on these points is also desirable.
Recent advancements in high-speed imaging techniques, such as compressed sensing, have the potential to shorten the imaging time for WHCA [50]. Furthermore, advancements in imaging techniques utilizing artificial intelligence are anticipated to enhance spatial resolution and decrease noise, thereby improving the image quality of WHCA. Deep learning reconstruction techniques have been used to improve the contrast-to-noise ratio and image quality of high-resolution WHCA [51]. A volunteer study has also demonstrated the potential of deep learning reconstruction for WHCA with sub-millimeter isotropic resolution at 3T [52]. These innovations in imaging technology are expected to further enhance the diagnostic accuracy of WHCA.
Limitations
First, many of the studies analysed were single centre studies with a limited number of cases, and the variability in study results cannot be ruled out. Prospective multicentre studies that include a larger number of patients are desirable. Second, we performed several subgroup analyses, but the number of included studies may be too small to produce statistically valid results.
Conclusions
The diagnostic performance of WHCA was deemed satisfactory, with contrast-enhanced 3.0 T WHCA exhibiting higher specificity compared to non-contrast-enhanced 1.5 T WHCA in a patient-based analysis. No significant differences in diagnostic performance were observed on a patient-based analysis based on the use of vasodilators, beta-blockers, or geographical regions (Asian and Western countries). Further large multicentre studies are imperative to facilitate the global adoption of WHCA.
Availability of data and materials
The datasets analysed in the current study are available from the corresponding author upon reasonable request.
Abbreviations
- BMI:
-
Body mass index
- CAD:
-
Coronary artery disease
- CI:
-
Confidence interval
- CT:
-
Computed tomography
- GRE:
-
Gradient echo
- MRI:
-
Magnetic resonance imaging
- ROC:
-
Receiver operating characteristics
- SSFP:
-
Steady state free precession
- WHCA:
-
Whole heart coronary magnetic resonance angiography
References
Brown JC, Gerhardt TE, Kwon E. Risk factors for coronary artery disease. Treasure Island: StatPearls Publishing LLC; 2022.
Chow BJ, Abraham A, Wells GA, et al. Diagnostic accuracy and impact of computed tomographic coronary angiography on utilization of invasive coronary angiography. Circ Cardiovasc Imaging. 2009;2:16–23. https://doi.org/10.1161/circimaging.108.792572.
Seitun S, Clemente A, Maffei E, et al. Prognostic value of cardiac CT. Radiol Med. 2020;125:1135–47. https://doi.org/10.1007/s11547-020-01285-w.
Newby DE, Adamson PD, Berry C, et al. Coronary CT angiography and 5-year risk of myocardial infarction. N Engl J Med. 2018;379:924–33. https://doi.org/10.1056/NEJMoa1805971.
Min JK, Gilmore A, Budoff MJ, Berman DS, O’Day K. Cost-effectiveness of coronary CT angiography versus myocardial perfusion SPECT for evaluation of patients with chest pain and no known coronary artery disease. Radiology. 2010;254:801–8. https://doi.org/10.1148/radiol.09090349.
Hajhosseiny R, Munoz C, Cruz G, et al. Coronary magnetic resonance angiography in chronic coronary syndromes. Front Cardiovasc Med. 2021;8:682924. https://doi.org/10.3389/fcvm.2021.682924.
Danias PG, Roussakis A, Ioannidis JP. Diagnostic performance of coronary magnetic resonance angiography as compared against conventional X-ray angiography: a meta-analysis. J Am Coll Cardiol. 2004;44:1867–76. https://doi.org/10.1016/j.jacc.2004.07.051.
Di Leo G, Fisci E, Secchi F, et al. Diagnostic accuracy of magnetic resonance angiography for detection of coronary artery disease: a systematic review and meta-analysis. Eur Radiol. 2016;26:3706–18. https://doi.org/10.1007/s00330-015-4134-0.
Scheffler K, Lehnhardt S. Principles and applications of balanced SSFP techniques. Eur Radiol. 2003;13:2409–18. https://doi.org/10.1007/s00330-003-1957-x.
Liu X, Bi X, Huang J, et al. Contrast-enhanced whole-heart coronary magnetic resonance angiography at 3.0 T: comparison with steady-state free precession technique at 1.5 T. Investig Radiol. 2008;43:663–8. https://doi.org/10.1097/RLI.0b013e31817ed1ff.
Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155:529–36. https://doi.org/10.7326/0003-4819-155-8-201110180-00009.
Migliavaca CB, Stein C, Colpani V, et al. Meta-analysis of prevalence: I(2) statistic and how to deal with heterogeneity. Res Synth Methods. 2022;13:363–7. https://doi.org/10.1002/jrsm.1547.
Jahnke C, Paetsch I, Nehrke K, et al. Rapid and complete coronary arterial tree visualization with magnetic resonance imaging: feasibility and diagnostic performance. Eur Heart J. 2005;26:2313–9. https://doi.org/10.1093/eurheartj/ehi391.
Sakuma H, Ichikawa Y, Suzawa N, et al. Assessment of coronary arteries with total study time of less than 30 minutes by using whole-heart coronary MR angiography. Radiology. 2005;237:316–21. https://doi.org/10.1148/radiol.2371040830.
Dewey M, Teige F, Schnapauff D, et al. Noninvasive detection of coronary artery stenoses with multislice computed tomography or magnetic resonance imaging. Ann Intern Med. 2006;145:407–15. https://doi.org/10.7326/0003-4819-145-6-200609190-00004.
Kim YJ, Seo JS, Choi BW, et al. Feasibility and diagnostic accuracy of whole heart coronary MR angiography using free-breathing 3D balanced turbo-field-echo with SENSE and the half-Fourier acquisition technique. Korean J Radiol. 2006;7:235–42. https://doi.org/10.3348/kjr.2006.7.4.235.
Sakuma H, Ichikawa Y, Chino S, et al. Detection of coronary artery stenosis with whole-heart coronary magnetic resonance angiography. J Am Coll Cardiol. 2006;48:1946–50. https://doi.org/10.1016/j.jacc.2006.07.055.
Liu X, Zhao XH, Huang J, et al. Comparison of 3D free-breathing coronary MR angiography and 64-MDCT angiography for detection of coronary stenosis in patients with high calcium scores. Am J Roentgenol. 2007;189:1326–32. https://doi.org/10.2214/ajr.07.2805.
Maintz D, Ozgun M, Hoffmeier A, et al. Whole-heart coronary magnetic resonance angiography: value for the detection of coronary artery stenoses in comparison to multislice computed tomography angiography. Acta Radiol. 2007;48:967–73. https://doi.org/10.1080/02841850701630292.
McCarthy RM, Deshpande VS, Beohar N, et al. Three-dimensional breathhold magnetization-prepared TrueFISP—a pilot study for magnetic resonance imaging of the coronary artery disease. Investig Radiol. 2007;42:665–70. https://doi.org/10.1097/RLI.0b013e3180661a77.
Klein C, Gebker R, Kokocinski T, et al. Combined magnetic resonance coronary artery imaging, myocardial perfusion and late gadolinium enhancement in patients with suspected coronary artery disease. J Cardiovasc Magn Reson. 2008;10:45. https://doi.org/10.1186/1532-429x-10-45.
Oncel D, Oncel G, Türkoğlu I. Accuracy of MR coronary angiography in the evaluation of coronary artery stenosis. Diagn Interv Radiol. 2008;14:153–8.
Pouleur AC, de Waroux JBL, Kefer J, et al. Direct comparison of whole-heart navigator-gated magnetic resonance coronary angiography and 40- and 64-slice multidetector row computed tomography to detect the coronary artery stenosis in patients scheduled for conventional coronary angiography. Circ Cardiovasc Imaging. 2008;1:114–21. https://doi.org/10.1161/circimaging.107.756304.
Kunimasa T, Sato Y, Matsumoto N, et al. Detection of coronary artery disease by free-breathing, whole heart coronary magnetic resonance angiography: our initial experience. Heart Vessel. 2009;24:429–33. https://doi.org/10.1007/s00380-008-1143-9.
Langer C, Peterschröder A, Franzke K, et al. Noninvasive coronary angiography focusing on calcification: multislice computed tomography compared with magnetic resonance imaging. J Comput Assist Tomogr. 2009;33:179–85. https://doi.org/10.1097/RCT.0b013e3181839624.
Yang Q, Li K, Liu X, et al. Contrast-enhanced whole-heart coronary magnetic resonance angiography at 3.0-T: a comparative study with X-ray angiography in a single center. J Am Coll Cardiol. 2009;54:69–76. https://doi.org/10.1016/j.jacc.2009.03.016.
Chen Z, Duan Q, Xue X, et al. Noninvasive detection of coronary artery stenoses with contrast-enhanced whole-heart coronary magnetic resonance angiography at 3.0 T. Cardiology. 2010;117:284–90. https://doi.org/10.1159/000323829.
Kato S, Kitagawa K, Ishida N, et al. Assessment of coronary artery disease using magnetic resonance coronary angiography: a national multicenter trial. J Am Coll Cardiol. 2010;56:983–91. https://doi.org/10.1016/j.jacc.2010.01.071.
Hamdan A, Asbach P, Wellnhofer E, et al. A prospective study for comparison of MR and CT imaging for detection of coronary artery stenosis. JACC Cardiovasc Imaging. 2011;4:50–61. https://doi.org/10.1016/j.jcmg.2010.10.007.
Nagata M, Kato S, Kitagawa K, et al. Diagnostic accuracy of 1.5-T unenhanced whole-heart coronary MR angiography performed with 32-channel cardiac coils: initial single-center experience. Radiology. 2011;259:384–92. https://doi.org/10.1148/radiol.11101323.
Wagner M, Rösler R, Lembcke A, et al. Whole-heart coronary magnetic resonance angiography at 1.5 Tesla: does a blood-pool contrast agent improve diagnostic accuracy? Investig Radiol. 2011;46:152–9. https://doi.org/10.1097/RLI.0b013e3181fac6ef.
Yang Q, Li KC, Liu X, et al. 3.0T whole-heart coronary magnetic resonance angiography performed with 32-channel cardiac coils a single-center experience. Circ Cardiovasc Imaging. 2012;5:573–9. https://doi.org/10.1161/circimaging.112.974972.
Bettencourt N, Ferreira N, Chiribiri A, et al. Additive value of magnetic resonance coronary angiography in a comprehensive cardiac magnetic resonance stress-rest protocol for detection of functionally significant coronary artery disease: a pilot study. Circ Cardiovasc Imaging. 2013;6:730–8. https://doi.org/10.1161/circimaging.113.000280.
Cheng L, Ma L, Schoenhagen P, et al. Comparison of three-dimensional volume-targeted thin-slab FIESTA magnetic resonance angiography and 64-multidetector computed tomographic angiography for the identification of proximal coronary stenosis. Int J Cardiol. 2013;167:2969–76. https://doi.org/10.1016/j.ijcard.2012.08.058.
Heer T, Reiter S, Höfling B, Pilz G. Diagnostic performance of non-contrast-enhanced whole-heart magnetic resonance coronary angiography in combination with adenosine stress perfusion cardiac magnetic resonance imaging. Am Heart J. 2013;166:999–1009. https://doi.org/10.1016/j.ahj.2013.08.018.
Piccini D, Monney P, Sierro C, et al. Respiratory self-navigated postcontrast whole-heart coronary MR angiography: initial experience in patients. Radiology. 2014;270:378–86. https://doi.org/10.1148/radiol.13132045.
Yonezawa M, Nagata M, Kitagawa K, et al. Quantitative analysis of 1.5-T whole-heart coronary MR angiograms obtained with 32-channel cardiac coils: a comparison with conventional quantitative coronary angiography. Radiology. 2014;271:356–64. https://doi.org/10.1148/radiol.13122491.
Yun H, Jin H, Yang S, et al. Coronary artery angiography and myocardial viability imaging: a 3.0-T contrast-enhanced magnetic resonance coronary artery angiography with Gd-BOPTA. Int J Cardiovasc Imaging. 2014;30:99–108. https://doi.org/10.1007/s10554-013-0297-4.
He Y, Pang J, Dai Q, et al. Diagnostic performance of self-navigated whole-heart contrast-enhanced coronary 3-T MR angiography. Radiology. 2016;281:401–8. https://doi.org/10.1148/radiol.2016152514.
Namba Y, Fuke S, Kashihara Y, et al. Diagnostic accuracy of three different protocols for 3.0T coronary magnetic resonance angiography. Int Heart J. 2016;57:535–40. https://doi.org/10.1536/ihj.15-436.
Chen ZY, Sun B, Duan Q, Xue YJ, Chen LL. 3.0T Contrast-enhanced whole-heart coronary magnetic resonance angiography for simultaneous coronary artery angiography and myocardial viability in chronic myocardial infarction: a single-center preliminary study. Medicine. 2018. https://doi.org/10.1097/md.0000000000013138.
Zhang L, Song X, Dong L, et al. Additive value of 3T cardiovascular magnetic resonance coronary angiography for detecting coronary artery disease. J Cardiovasc Magn Reson. 2018;20:29. https://doi.org/10.1186/s12968-018-0450-2.
Sun B, Chen Z, Duan Q, et al. A direct comparison of 3 T contrast-enhanced whole-heart coronary cardiovascular magnetic resonance angiography to dual-source computed tomography angiography for detection of coronary artery stenosis: a single-center experience. J Cardiovasc Magn Reson. 2020;22:40. https://doi.org/10.1186/s12968-020-00630-2.
Lin L, Wang L, Zhang XN, et al. A clinical strategy to improve the diagnostic accuracy of 1.5-T non-contrast MR coronary angiography for detection of coronary artery disease: combination of whole-heart and volume-targeted imaging. Eur Radiol. 2021;31:1894–904. https://doi.org/10.1007/s00330-020-07135-7.
Lu H, Guo J, Zhao S, et al. Assessment of non-contrast-enhanced dixon water-fat separation compressed sensing whole-heart coronary MR angiography at 3.0 T: a single-center experience. Acad Radiol. 2022;29(Suppl 4):S82–90. https://doi.org/10.1016/j.acra.2021.05.009.
Nazir MS, Bustin A, Hajhosseiny R, et al. High-resolution non-contrast free-breathing coronary cardiovascular magnetic resonance angiography for detection of coronary artery disease: validation against invasive coronary angiography. J Cardiovasc Magn Reson. 2022;24:26. https://doi.org/10.1186/s12968-022-00858-0.
Hajhosseiny R, Rashid I, Bustin A, et al. Clinical comparison of sub-mm high-resolution non-contrast coronary CMR angiography against coronary CT angiography in patients with low-intermediate risk of coronary artery disease: a single center trial. J Cardiovasc Magn Reson. 2021;23:57. https://doi.org/10.1186/s12968-021-00758-9.
McConnell MV, Ganz P, Selwyn AP, et al. Identification of anomalous coronary arteries and their anatomic course by magnetic resonance coronary angiography. Circulation. 1995;92:3158–62. https://doi.org/10.1161/01.cir.92.11.3158.
Takemura A, Suzuki A, Inaba R, et al. Utility of coronary MR angiography in children with Kawasaki disease. Am J Roentgenol. 2007;188:W534–39. https://doi.org/10.2214/ajr.05.1414.
Hirai K, Kido T, Kido T, et al. Feasibility of contrast-enhanced coronary artery magnetic resonance angiography using compressed sensing. J Cardiovasc Magn Reson. 2020;22:15. https://doi.org/10.1186/s12968-020-0601-0.
Yokota Y, Takeda C, Kidoh M, et al. Effects of deep learning reconstruction technique in high-resolution non-contrast magnetic resonance coronary angiography at a 3-Tesla machine. Can Assoc Radiol J. 2021;72:120–7. https://doi.org/10.1177/0846537119900469.
Kariyasu T, Machida H, Takahashi S, et al. Denoising using deep-learning-based reconstruction for whole-heart coronary MRA with sub-millimeter isotropic resolution at 3 T: a volunteer study. Diagn Interv Radiol. 2022;28:470–7. https://doi.org/10.5152/dir.2022.21291.
Acknowledgements
Not applicable.
Funding
Japanese Society for the Promotion of Science, Grant-in-Aid for Scientific Research (C).
Author information
Authors and Affiliations
Contributions
SK, MA analysed and interpreted the data. NN, KF, MI, NS, NH and DU contributed significantly to writing the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
IRB approval was not obtained, as this study was a meta-analysis.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Material S1.
PubMed 106, WOS 73, Cochrane 4, EMBASE. Material S2. QUADAS-2. Material S3. Sensitivity and Specificity of WHCA on patient-based analysis. Material S4. Sensitivity and Specificity of WHCA on vessel-based analysis. Material S5. Sensitivity and Specificity of WHCA on segment-based analysis.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kato, S., Azuma, M., Nakayama, N. et al. Diagnostic accuracy of whole heart coronary magnetic resonance angiography: a systematic review and meta-analysis. J Cardiovasc Magn Reson 25, 36 (2023). https://doi.org/10.1186/s12968-023-00949-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12968-023-00949-6