
Abstract
Background
Vitamin D deficiency is common among the population, but its relationship with mortality of postmenopausal females is unclear. The aim of this study is to explore the association between serum 25-Hydroxyvitamin D (25(OH)D) and all-cause and cause-specific mortality among postmenopausal women in the United States.
Methods
6812 participants of postmenopausal females from the National Health and Nutrition Examination Survey (2001–2018) were included in this study. The mortality status of the follow-up was ascertained by linkage to National Death Index (NDI) records through 31 December 2019. We used cox proportional hazards models to estimate the association of serum 25(OH)D concentrations and mortality of postmenopausal females.
Results
The mean level of serum 25(OH)D was 72.57 ± 29.93 nmol/L, and 65.34% had insufficient vitamin D. In postmenopausal females, low serum 25(OH)D concentrations were significantly associated with higher levels of glycohemoglobin, glucose, and lower levels of HDL. During follow-up, 1448 all-cause deaths occurred, including 393 cardiovascular disease (CVD)-related deaths and 263 cancer deaths. After multivariate adjustment, higher serum 25(OH)D levels were significantly related with lower all-cause and CVD mortality. In addition, serum 25(OH)D presented a L-shaped relationship with all-cause mortality, while appeared a U-shaped with CVD mortality, and the cut-off value is 73.89 nmol/L and 46.75 nmol/L respectively.
Conclusions
Low serum 25(OH)D levels are associated with the higher risk of all-cause and CVD mortality in postmenopausal females. These findings provide new ideas and targets for the health management of postmenopausal women.
Similar content being viewed by others

Introduction
Menopause refers to the cessation of the menstrual cycle due to anovulation, which is an inevitable process of aging [1, 2]. Menopause causes significant fluctuations of sexual hormones in females. The decline of estrogen secreted by the ovaries during menopause may lead to physical discomfort and a series of medical issues, including hot flashes and night sweats, emotional changes, insomnia, urogenital atrophy, osteoporosis, susceptibility to cardiovascular disease and diabetes. The age of menopause varies greatly. The average age of menopause is 51 years old, ranging from 40 to 60 years old [3]. A large amount of studies have indicated that postmenopausal women have a higher risk of cardiovascular disease (CVD) and death [4,5,6]. Therefore, it is crucial to identify modifiable factors to prevent complications and reduce mortality in postmenopausal women, especially to reduce the risk of cardiovascular death.
Vitamin D is a kind of fat-soluble vitamin that promotes calcium and phosphorus absorption, and 25-hydroxyvitamin D (25(OH)D) is the primary storage in the body [7]. Vitamin D deficiency is highly prevalent among the general populations [8,9,10,11]. Serum 25(OH)D deficiency is a common risk factor for various diseases, such as CVD, hypertension, diabetes, cancer, chronic kidney disease, sepsis and so on [12,13,14,15]. It is suggested that vitamin D deficiency has been strongly associated with all-cause mortality [16]. In particular, current researches suggested that Vitamin D deficiency is associated with the severity and mortality rate of Coronavirus disease 2019 (COVID-19) cases, which has raised public concern about the association between vitamin D deficiency and health status [17, 18].
Current research suggested that the lack of 25(OH)D increased the risk of fracture across the menopause [19]. It has also been reported that high 25(OH)D concentrations in serum reduced the risk of breast cancer [20], and even low 25(OH)D concentration is associated with lower overall survival rate of patients with ovarian cancer [21]. However, the association between 25(OH)D levels and all-cause and cause-specific mortality in postmenopausal females remains unclear. Based on this, we investigated the relationship between serum 25(OH)D concentrations and all-cause and cause-specific mortality in a nationally representative sample of postmenopausal women in the United States.
Methods
Study design and population
National Health and Nutrition Examination Survey (NHANES) is a cross-sectional survey aimed at collecting information on the health and nutritional status of adults and children in the United States, which was conducted by the National Center for Health Statistics (NCHS) of the Centers for Disease Control and Prevention (CDC). All NHANES protocols were approved by the CDC’s National Center for Health Statistics Ethics Review Board, and all participants of survey provided written informed consent.
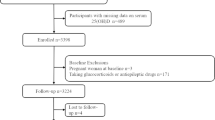
In this study, seven cycles of NHANES from 2001 to 2018 (2001–2002, 2003–2004, 2005–2006, 2007–2008, 2009–2010, 2011–2012, 2013–2014, 2015–2016, 2017–2018) were selected for further analysis. Menopausal status was determined according to the responses of the questionnaire on reproductive health. Participants were first asked, “Had regular periods in past 12 months?”. The subjects who answered “no” continued to be asked, “Reason not having regular periods. (Options: Menopause/change of life; Pregnancy; Breastfeeding; Medical conditions/treatments; other)”. So first, 9607 postmenopausal women at enrollment were included. After excluding those with missing serum 25(OH)D concentrations (n = 609), having cancer at baseline or missing medical conditions data (n = 1373), missing demo and related covariates data (n = 813), the final sample population for the purposes of this study was 6812 participants (Fig. 1).

Flow chart of study participants
Measurement of serum 25(OH)D concentrations
In the 2001–2006 cycle of the NHANES, serum 25(OH)D concentrations were measured by DiaSorin RIA kit (Stillwater MN) and by a standardized liquid chromatography–tandem mass spectrometry (LC–MS/MS) method in 2007–2018. So as to use and analyze 25(OH)D concentration, the regression equations were selected to converted RIA measurements of 25(OH)D concentration to equivalent 25(OH)D measurements in the standardized LC–MS/MS method to adjust for assay drifts. Follow the recommendations of CDC, LC–MS/MS data was performed for analysis [22].
Determination of mortality outcomes
To determine the mortality status of the follow-up population, we used 2001–2018 NHANES public-use linked mortality files, the survival status of participants was followed up to December 31, 2019. The ICD-10 was used to determine disease-specific death, and NCHS classified heart diseases (054–068), malignant neoplasms (019–043), and all other causes (010) [23]. Serum 25(OH)D levels were classified according to the Endocrine Society Clinical Practice guidelines [24], as follows: < 25.00 nmol/L, indicating severe vitamin D deficiency; 25.00–49.99 nmol/L, indicating vitamin D deficiency; 50.00–74.99 nmol/L, indicating vitamin D insufficiency; ≥ 75.00 nmol/L, indicating vitamin D sufficiency.
Covariates
Based on previous research, we used additional covariates in this study. Questionnaires were collected to acquire demographic information (age, race/ethnicity, education level, family income), smoking status, and alcohol intake. Body mass index (BMI, kg/m2) were measured at the Mobile Examination Center. The history of hypertension or diabetes obtained from laboratory, examination and questionnaire data.
Race/ethnicity was categorized as Mexican American, other Hispanic, non-Hispanic White, non-Hispanic Black, other Hispanic or other race; education levels were classified as less than a high school education, some high school, high school graduate/GED, some college or associate’s degree, college graduate or more; BMI was categorized as underweight (< 18.5 kg/m2), normal (18.5 to < 25 kg/m2), overweight (25 to < 30 kg/m2), subjects with obesity (BMI 30 kg/m2 or greater); alcohol intake was defined by the monthly alcohol consumption, and categorized by (non-drinker, 1 to < 5 drinks/month, 5 to < 10 drinks/month, or 10 + drinks/month; and smoking status was classified as current, former, or never smoker.
Plasma glycohemoglobin (%), glucose (mg/dL), cholesterol (mg/dL), direct HDL-cholesterol (mg/dL), LDL-cholesterol (mg/dL) and triglycerides (mg/dL) were acquired from the NHANES laboratory examination component.
Statistical analyses
The data in this research were statistically analyzed according to the CDC guidelines [25]. Serum 25(OH)D levels were classified as mentioned above. We presented continuous variables using the mean and standard deviation, and described categorical variables as percentages. And we used three Cox regression models to explore the association of serum 25(OH)D concentrations and mortality: Model 1 (unadjusted); Model 2 was adjusted for age and race/ethnicity; Model 3 was adjusted for age, race/ethnicity, education level, PIR, BMI, smoking status, alcohol intake, hypertension and diabetes.
In addition, restricted cubic spline regression (RCS) model was used to investigate the non-linear relationship between serum 25(OH)D concentration and mortality. And the lowest point of hazard ratios (HRs) in RCS analysis was defined as cut-off value. At last, we conducted subgroup analyses based on age (< 60 years old or ≥ 60 years old), race/ethnicity (Whites or non-Whites), BMI (< 25.00 or ≥ 25.00), hypertension, and diabetes. R version 3.4.3 was used for all statistical analyses.
Results
Baseline characteristics of study participants
6812 participants of postmenopausal women were enrolled in this study. The mean age of participants was 61.00 ± 10.86 years old. The weighted mean concentration of serum 25(OH)D was 72.57 ± 29.93 nmol/L; 29.70% of participants had deficient vitamin D (< 50.00 nmol/L), and 65.34% had insufficient vitamin D (< 75.00 nmol/L). The baseline characteristics of the selected female participants according to serum 25(OH)D are presented in the Table 1. Participants who had higher 25(OH)D concentrations were more likely to be older, non-Hispanic White; had higher education levels and family income; were less likely to be subjects with obesity, current smokers and alcohol intake. And higher levels of serum 25(OH)D were also associated with lower incidence rate of hypertension and diabetes.
In addition, we also explored the relationship between cardiometabolic biomarkers and serum 25(OH)D. As shown in Table 2, the levels of serum 25(OH)D were negatively associated with the levels of glycohemoglobin, glucose and triglycerides, and positively associated with HDL levels at baseline.
Association of 25(OH)D concentration with mortality
During the follow-up of this study, 1448 all-cause deaths occurred, including 393 CVD-related deaths and 263 cancer deaths (Table 3). We constructed three Cox regression models to explore the independent effect of serum 25(OH)D levels in mortality. The multivariate adjustments including age, race/ethnicity, education level, PIR, BMI, smoking status, alcohol intake, hypertension and diabetes. As shown, multivariate adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) from lowest to highest serum 25(OH)D categories (< 25.00, 25.00–49.99, 50.00–74.99, and ≥ 75.00 nmol/L) were 1.00 (reference), 0.63 (0.44, 0.92), 0.50 (0.34,0.71), and 0.46 (0.31,0.69), respectively, for all-cause mortality (Model 3). While for CVD mortality, the multivariate adjusted HRs and 95% CIs were 1.00 (reference), 0.34 (0.19, 0.61), 0.40 (0.22, 0.74), and 0.60 (0.31,1.15), respectively. In addition, we also explored the relationship between serum 25(OH)D concentrations and cancer mortality. The results showed the HRs and 95% CIs were 1.00 (reference), 0.87 (0.45, 1.70), 0.72 (0.38, 1.36), and 1.36 (0.67, 2.73). Compared with the group of serum 25(OH)D < 25.00 nmol/L, postmenopausal females with higher levels of serum 25(OH)D (≥ 25.00 nmol/L) had lower all-cause and CVD mortality. Although there are statistical differences in trend for cancer mortality, there is no statistical difference among groups, which may be due to the small sample size.
Results of nonlinear of 25(OH)D concentration and mortality
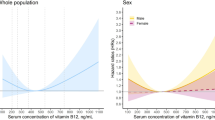
By using the restricted cubic spline regression (RCS) models with full adjustment for confounders, we found that there was the L-shaped association between serum 25(OH)D concentrations and all-cause mortality, while serum 25(OH)D levels displayed a U-shaped relationship with CVD mortality (Fig. 2). And the cut-off value for all-cause mortality were 73.89 nmol/L, and 46.75 nmol/L for CVD mortality.

Association between 25(OH)D concentration and all-cause (A) and CVD mortality (B) in postmenopausal women. Adjusted for age, race/ethnicity, education level, PIR, BMI, smoking status, alcohol intake, hypertension and diabetes. The solid and dotted lines represent the estimated values and their corresponding 95% CIs, respectively
Stratified analyses
The data of Fig. 3 showed the association of serum 25(OH)D concentrations and all-cause mortality as stratified by age, race, BMI, and race/ethnicity, history of hypertension, and history of diabetes. In subgroup analysis, lower serum 25(OH)D levels (< 73.89 nmol/L) and higher 25(OH)D concentrations (≥ 73.89 nmol/L) present similar advantages for survival rate among postmenopausal females. Additionally, our results showed a stronger inverse relationship between serum 25(OH)D concentrations and all-cause mortality in older, white, with no history of diabetes postmenopausal women.

Forest plots of stratified analyses of serum 25(OH)D and all-cause mortality. Adjusted for age, race/ethnicity, education level, PIR, BMI, smoking status, alcohol intake, hypertension and diabetes, except the variable itself
Discussion
In this large prospective cohort study, we revealed the association between serum 25(OH)D concentrations and all-cause and CVD mortality of postmenopausal women. The results indicated a L-shaped relationship between serum 25 (OH) D levels and all-cause mortality for postmenopausal females, while it seems to be a U-shaped with CVD mortality. That means within a certain range, lower serum 25 (OH) D levels were significantly associated with higher risk of all-cause and CVD mortality.
According to Clinical Practice guidelines of Endocrine Society, our result indicated that 65.34% of postmenopausal females have suffering serum 25(OH)D insufficiency, which means vitamin D deficiency was commonly present in women of postmenopausal. And above result is consistent with previous researches [26,27,28]. Our data also suggested that compared to postmenopausal women with serum 25(OH)D ≥ 25.00 nmol/L, those with serum 25(OH)D < 25.00 nmol/L had higher all-cause mortality and CVD mortality.
Vitamin D deficiency may have adverse effects on the immune system and increase the risk of acute respiratory infections. The mortality rate of COVID-19 patients in recent years is positively correlated with Vitamin D deficiency [17, 18]. And another meta-analysis indicated that COVID-19 positive patients have lower serum Vitamin D concentrations, which is more prominent in women [29]. Although there is currently no research to elucidate the relationship between vitamin D concentration and the onset and progression of COVID-19 in postmenopausal women, it is still recommended that supplementing vitamin D may reduce the severity of COVID-19 infection [30].
Currently, a series of studies suggested that low levels of 25(OH)D in serum were closely related to a higher risk of mortality, but the optimal concentration of serum 25(OH)D remained controversial. The American Institute of medicine suggested that 50.00 nmol/L was sufficient for bone health [31]. However, the Endocrinology Society proposed that the optimal concentration of 25(OH)D in serum among general adults should be at least 75.00 nmol/L for better health condition [28]. A study put forward that the thresholds of serum 25(OH)D was 27.70 and 54.40 nmol/L for CVD and all-cause mortality respectively in American patients with osteoarthritis [28]. But another meta-analysis suggested that with the increase of circulating 25(OH)D, the mortality risk showed a non-linear decrease, and the optimal concentration was about 75.00–87.50 nmol/L [32]. The reasons for the above controversy may be due to differences in the target population, sample size, and basic health status. Lack of vitamin D may worsen menopausal symptoms, but the evidence is not sufficient [30]. And insufficient Vitamin D can affect the bone health and exacerbate osteoporosis in postmenopausal females [30, 33]. But no research has yet focused on the relationship between 25(OH)D and mortality rate among postmenopausal women. The data of this study indicated that lower 25(OH)D levels in serum of postmenopausal women may lead to a higher risk of all-cause and CVD mortality. And the values corresponding to the lowest all-cause and CVD mortality rate are 73.89 nmol/L and 46.75 nmol/L, respectively.
The relationship between vitamin D and cancer mortality is uncertain [34,35,36,37]. Cervical, ovarian, and uterine cancer are the three most common types of gynecologic cancers. The relationship between vitamin D exposure and survival rate of ovarian cancer survivors is controversial [24, 38, 39]. And serum 25(OH)D does not seem to improve the prognosis of uterine cancer [40, 41]. Although a meta-analysis showed that circulating 25(OH)D was associated with overall mortality in in stage I-IIIa postmenopausal breast cancer patients [42], there was no significant correlation between serum 25(OH)D levels and cancer mortality in postmenopausal women in our study. The reason for the above results may be due to the insufficient sample size for cancer in this study, a larger scale prospective study is needed to investigate the relationship between vitamin D and cancer mortality.
To further identify the population at higher risk of all-cause mortality in postmenopausal females, we conducted a sub layer analysis. The results showed that higher serum vitamin D concentrations (≥ 73.89) had a better advantage on all-cause mortality in the elderly (≥ 60 years old), Whites, and without a history of diabetes populations. The absorption and utilization of Vitamin D vary among different races [43]. Previous study proposed that non-Hispanic Blacks with a higher proportion of lower serum 25(OH)D below 25.00 nmol/L in the osteoarthritis patients [28], which is consistent with our results of postmenopausal women. However, White people seem to have poorer adaptability to vitamin D deficiency. An analysis of the American population suggested that 25-hydroxyvitamin D deficiency was related to an increased risk of fatal stroke in Whites but not Blacks [44]. And lower serum 25(OH)D concentrations appeared to hurt more in Whites osteoarthritis patients [28]. Consistent with the above results, our study also showed that the lack of vitamin D in Whites postmenopausal women is more correlated with a higher risk of all-cause mortality. It is worth noting that elderly postmenopausal females with low levels of serum 25(OH)D have a higher risk of death. The mechanism of the above results is still unclear, but in the process of clinical health management, more attention should be paid to the elderly and Whites population.
The potential mechanism for the association between lower 25(OH)D levels and increased risk of death is currently unclear. From a biological perspective, a lot of tissues and cells respond to 25(OH)D [45, 46]. 25(OH)D is a kind of self-balancing regulator of the renin angiotensin aldosterone system, which can affect blood pressure [47]. And Vitamin D can influence the migration and differentiation of macrophages and the uptake of cholesterol, inhibit the formation of foam cells, and reverse the cholesterol metabolism that causes atherosclerosis among diabetes patients, which may increase the risk of cardiovascular disease in related populations [48, 49]. Vitamin D deficiency is related with an increased risk of cardiovascular events (including metabolic syndrome, type 2 diabetes mellitus and dyslipidemia) [30], thus, we also explored the relationship between the index of cardiovascular metabolism and serum 25(OH)D in postmenopausal women. Higher serum 25(OH)D levels were significantly associated with lower levels of glycohemoglobin and glucose, and with high level of HDL. A large number of studies indicated that low concentrations of vitamin D were related with CVD, including coronary calcification and elevated triglyceride levels [50, 51]. Our study suggests that lower levels of serum 25(OH)D levels are associated with CVD mortality in postmenopausal women. Interestingly, our results indicated that the optimal protective concentration of 25(OH)D for CVD related death in postmenopausal females was 46.75 nmol/L. That is to say, when the serum 25(OH)D concentration is higher than 46.75 nmol/L, the risk of CVD death increases. There is currently controversy over whether vitamin D is a protective factor for cardiovascular health. As mentioned above, a large number of studies have proposed that high 25(OH)D can reduce the risk of CVD and CVD related mortality, but there are also studies that suggest that excessive supplementation of vitamin D may increase the risk of cardiovascular events [52,53,54]. The potential biological explanation may be that high concentration of 25(OH)D leads to high blood calcium concentration, which eventually leads to vascular calcification, atherosclerosis and hypercoagulability [55, 56]. Thus, determining the most suitable serum 25(OH)D concentration is crucial. Unfortunately, this article is currently unable to define the relationship between serum 25(OH)D concentration and blood calcium, which will be the focus of our next research.
In addition to cardiovascular factors, osteoporosis is another major cause of death in postmenopausal females. Postmenopausal women experience rapid bone loss due to decreased levels of sex hormones caused by ovarian disfunction, which affects calcium metabolism and increases the possibility of osteoporosis. The probability of osteoporosis in postmenopausal women significantly increases, and it seriously endangers health and lifespan [57]. The decrease in estrogen levels after menopause can cause cardiovascular symptoms and osteoporosis. Estrogen deficiency can induce the loss of cancellous and cortical bone in menopause [58]. The use of hormone replacement therapy in menopause can reduce the risk of osteoporosis, but it is related to the increased risk of cardiovascular and cerebrovascular events, breast cancer and other adverse health outcomes [59, 60]. Previous studies had indicated that Vitamin D supplementation can prevent osteoporosis and fractures in postmenopausal women [61,62,63,64]. Due to current article lacks complete information on osteoporosis and serum estrogen, whether Vitamin D reduces postmenopausal mortality is due to the reduction of osteoporosis, and whether this process is mediated by estrogen, requires further research in the future.
Conclusions
In conclusion, this study is the first to explore the relationship between serum 25 (OH) D and all-cause mortality and specific mortality in postmenopausal women. Lower serum 25(OH)D concentrations were significantly and nonlinearly associated with a higher risk of all-cause and CVD death among postmenopausal females in the United States. These data provide new clues for the health management of postmenopausal females. For postmenopausal women, regular testing of blood serum 25(OH)D concentrations may be necessary, and based on the results, it is recommended to sunlight exposure supplement, or even Vitamin D supplementation.
Availability of data and materials
Data described in the manuscript are publicly and freely available without restriction at https://www.cdc.gov/nchs/nhanes/index.htm.
Abbreviations
- 25(OH) D:
-
25-Hydroxyvitamin D
- NDI:
-
National Death Index
- CVD:
-
Cardiovascular disease,
- LC–MS/MS:
-
Liquid chromatography–tandem mass spectrometry
- BMI:
-
Body mass index
Reference:s
Nelson HD. Menopause. Lancet. 2008;371(9614):760–70. https://doi.org/10.1016/S0140-6736(08)60346-3.
Davis SR, Lambrinoudaki I, Lumsden M, et al. Menopause. Nat Rev Dis Primers. 2015;1:15004. https://doi.org/10.1038/nrdp.2015.4.
te Velde ER, Pearson PL. The variability of female reproductive ageing. Hum Reprod Update. 2002;8(2):141–54. https://doi.org/10.1093/humupd/8.2.141.
Newson L. Menopause and cardiovascular disease. Post Reprod Health. 2018;24(1):44–9. https://doi.org/10.1177/2053369117749675.
Tandon VR, Mahajan A, Sharma S, Sharma A. Prevalence of cardiovascular risk factors in postmenopausal women: a rural study. J Midlife Health. 2010;1(1):26–9. https://doi.org/10.4103/0976-7800.66993.
Mendelsohn ME, Karas RH. Molecular and cellular basis of cardiovascular gender differences. Science. 2005;308(5728):1583–7. https://doi.org/10.1126/science.1112062.
Li A, Yi B, Han H, et al. Vitamin D-VDR (vitamin D receptor) regulates defective autophagy in renal tubular epithelial cell in streptozotocin-induced diabetic mice via the AMPK pathway. Autophagy. 2022;18(4):877–90. https://doi.org/10.1080/15548627.2021.1962681.
Schleicher RL, Sternberg MR, Looker AC, et al. National estimates of serum total 25-Hydroxyvitamin D and metabolite concentrations measured by liquid chromatography-tandem mass spectrometry in the US population during 2007–2010. J Nutr. 2016;146(5):1051–61. https://doi.org/10.3945/jn.115.227728.
Sarafin K, Durazo-Arvizu R, Tian L, et al. Standardizing 25-hydroxyvitamin D values from the Canadian health measures survey. Am J Clin Nutr. 2015;102(5):1044–50. https://doi.org/10.3945/ajcn.114.103689.
Cashman KD, Vitamin D. Deficiency: defining, prevalence, causes, and strategies of addressing. Calcif Tissue Int. 2020;106(1):14–29. https://doi.org/10.1007/s00223-019-00559-4.
Cashman KD, Dowling KG, Škrabáková Z, et al. Vitamin D deficiency in Europe: pandemic? Am J Clin Nutr. 2016;103(4):1033–44. https://doi.org/10.3945/ajcn.115.120873.
Amrein K, Scherkl M, Hoffmann M, et al. Vitamin D deficiency 2.0: an update on the current status worldwide. Eur J Clin Nutr. 2020;74(11):1498–513. https://doi.org/10.1038/s41430-020-0558-y.
de Borst MH, de Boer RA, Stolk RP, Slaets JP, Wolffenbuttel BH, Navis G. Vitamin D deficiency: universal risk factor for multifactorial diseases? Curr Drug Targets. 2011;12(1):97–106. https://doi.org/10.2174/138945011793591590.
Pilz S, Iodice S, Zittermann A, Grant WB, Gandini S. Vitamin D status and mortality risk in CKD: a meta-analysis of prospective studies. Am J Kidney Dis. 2011;58(3):374–82. https://doi.org/10.1053/j.ajkd.2011.03.020.
Gunta SS, Thadhani RI, Mak RH. The effect of vitamin D status on risk factors for cardiovascular disease. Nat Rev Nephrol. 2013;9(6):337–47. https://doi.org/10.1038/nrneph.2013.74.
Gaksch M, Jorde R, Grimnes G, et al. Vitamin D and mortality: Individual participant data meta-analysis of standardized 25-hydroxyvitamin D in 26916 individuals from a European consortium. PLoS ONE. 2017;12(2):e0170791. https://doi.org/10.1371/journal.pone.0170791.
Barrea L, Verde L, Grant WB, et al. Vitamin D: a role also in long COVID-19? Nutrients. 2022;14(8):1625. https://doi.org/10.3390/nu1408162.
Verdoia M, De Luca G. Potential role of hypovitaminosis D and vitamin D supplementation during COVID-19 pandemic. QJM. 2021;114(1):3–10. https://doi.org/10.1093/qjmed/hcaa234.
Cauley JA, Greendale GA, Ruppert K, et al. Serum 25 hydroxyvitamin D, bone mineral density and fracture risk across the menopause. J Clin Endocrinol Metab. 2015;100(5):2046–54. https://doi.org/10.1210/jc.2014-4367.
Engel P, Fagherazzi G, Boutten A, et al. Serum 25(OH) vitamin D and risk of breast cancer: a nested case-control study from the French E3N cohort. Cancer Epidemiol Biomarkers Prev. 2010;19(9):2341–50. https://doi.org/10.1158/1055-9965.EPI-10-0264.
Walentowicz-Sadlecka M, Grabiec M, Sadlecki P, et al. 25(OH)D3 in patients with ovarian cancer and its correlation with survival. Clin Biochem. 2012;45(18):1568–72. https://doi.org/10.1016/j.clinbiochem.2012.07.110.
CDC/National Center for Health Statistics. Analytical note for 25-hydroxy-vitamin D data analysis using NHANES III (1988–1994), NHANES 2001–2006, and NHANES 2007–2010. 2015. https://wwwn.cdc.gov/nchs/nhanes/vitamind/analyticalnote.aspx?b=2013&e=2014&d= VID_H. Accessed 8 Jan 2022.
International statistical classification of diseases and related health problems, 10th revision, Fifth edn. 2016. https://apps.who.int/iris/handle/10665/246208. Accessed 20 Mar 2022.
Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):1911–30. https://doi.org/10.1210/jc.2011-0385.
NHANES Tutorials. https://wwwn.cdc.gov/nchs/nhanes/tutorials/default.aspx. Accessed 20 Mar 2022.
Al-Jarallah KF, Shehab D, Al-Awadhi A, Nahar I, Haider MZ, Moussa MA. Are 25(OH)D levels related to the severity of knee osteoarthritis and function? Med Princ Pract. 2012;21(1):74–8. https://doi.org/10.1159/000330025.
Wan Z, Guo J, Pan A, Chen C, Liu L, Liu G. Association of serum 25-hydroxyvitamin D concentrations with all-cause and cause-specific mortality among individuals with diabetes. Diabetes Care. 2021;44(2):350–7. https://doi.org/10.2337/dc20-1485.
Xiao Q, Cai B, Yin A, et al. L-shaped association of serum 25-hydroxyvitamin D concentrations with cardiovascular and all-cause mortality in individuals with osteoarthritis: results from the NHANES database prospective cohort study. BMC Med. 2022;20(1):308. https://doi.org/10.1186/s12916-022-02510-1.
Pereira M, Dantas Damascena A, Galvão Azevedo LM, de Almeida OT, da Mota SJ. Vitamin D deficiency aggravates COVID-19: systematic review and meta-analysis. Crit Rev Food Sci Nutr. 2022;62(5):1308–16. https://doi.org/10.1080/10408398.2020.1841090.
Anagnostis P, Livadas S, Goulis DG, et al. EMAS position statement: vitamin D and menopausal health. Maturitas. 2023;169:2–9. https://doi.org/10.1016/j.maturitas.2022.12.006.
Ross AC, Manson JE, Abrams SA, et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the institute of medicine: what clinicians need to know. J Clin Endocrinol Metab. 2011;96(1):53–8. https://doi.org/10.1210/jc.2010-2704.
Zittermann A, Iodice S, Pilz S, Grant WB, Bagnardi V, Gandini S. Vitamin D deficiency and mortality risk in the general population: a meta-analysis of prospective cohort studies. Am J Clin Nutr. 2012;95(1):91–100. https://doi.org/10.3945/ajcn.111.014779.
Rizzoli R, Boonen S, Brandi ML, et al. Vitamin D supplementation in elderly or postmenopausal women: a 2013 update of the 2008 recommendations from the European society for clinical and economic aspects of osteoporosis and osteoarthritis (ESCEO). Curr Med Res Opin. 2013;29(4):305–13. https://doi.org/10.1185/03007995.2013.766162.
Mondul AM, Weinstein SJ, Layne TM, Albanes D. Vitamin D and cancer risk and mortality: state of the science, gaps, and challenges. Epidemiol Rev. 2017;39(1):28–48. https://doi.org/10.1093/epirev/mxx005.
Chowdhury R, Kunutsor S, Vitezova A, et al. Vitamin D and risk of cause specific death: systematic review and meta-analysis of observational cohort and randomised intervention studies. BMJ. 2014;348:g1903. https://doi.org/10.1136/bmj.g1903.
Sutherland JP, Zhou A, Hyppönen E. Vitamin D deficiency increases mortality risk in the UK biobank : a nonlinear mendelian randomization study. Ann Intern Med. 2022;175(11):1552–9. https://doi.org/10.7326/M21-3324.
Khaw KT, Luben R, Wareham N. Serum 25-hydroxyvitamin D, mortality, and incident cardiovascular disease, respiratory disease, cancers, and fractures: a 13-y prospective population study. Am J Clin Nutr. 2014;100(5):1361–70. https://doi.org/10.3945/ajcn.114.086413.
L’Espérance K, Datta GD, Qureshi S, Koushik A. Vitamin D exposure and ovarian cancer risk and prognosis. Int J Environ Res Public Health. 2020;17(4):1168. https://doi.org/10.3390/ijerph17041168.
Webb PM, de Fazio A, Protani MM, et al. Circulating 25-hydroxyvitamin D and survival in women with ovarian cancer. Am J Clin Nutr. 2015;102(1):109–14. https://doi.org/10.3945/ajcn.114.102681.
Liu JJ, Bertrand KA, Karageorgi S, et al. Prospective analysis of vitamin D and endometrial cancer risk. Ann Oncol. 2013;24(3):687–92. https://doi.org/10.1093/annonc/mds509.
McCullough ML, Bandera EV, Moore DF, Kushi LH. Vitamin D and calcium intake in relation to risk of endometrial cancer: a systematic review of the literature. Prev Med. 2008;46(4):298–302. https://doi.org/10.1016/j.ypmed.2007.11.010.
Vrieling A, Seibold P, Johnson TS, et al. Circulating 25-hydroxyvitamin D and postmenopausal breast cancer survival: Influence of tumor characteristics and lifestyle factors? Int J Cancer. 2014;134(12):2972–83. https://doi.org/10.1002/ijc.28628.
Ames BN, Grant WB, Willett WC. Does the high prevalence of vitamin D deficiency in African Americans contribute to health disparities? Nutrients. 2021;13(2):499. https://doi.org/10.3390/nu13020499.
Michos ED, Reis JP, Post WS, et al. 25-Hydroxyvitamin D deficiency is associated with fatal stroke among whites but not blacks: the NHANES-III linked mortality files. Nutrition. 2012;28(4):367–71. https://doi.org/10.1016/j.nut.2011.10.015.
Muñoz A, Grant WB. Vitamin D and cancer: an historical overview of the epidemiology and mechanisms. Nutrients. 2022;14(7):1448. https://doi.org/10.3390/nu14071448.
Wimalawansa SJ. Associations of vitamin D with insulin resistance, obesity, type 2 diabetes, and metabolic syndrome. J Steroid Biochem Mol Biol. 2018;175:177–89. https://doi.org/10.1016/j.jsbmb.2016.09.017.
Li YC, Kong J, Wei M, Chen ZF, Liu SQ, Cao LP. 1,25-dihydroxyvitamin D(3) is a negative endocrine regulator of the renin-angiotensin system. J Clin Invest. 2002;110(2):229–38. https://doi.org/10.1172/JCI15219.
Oh J, Weng S, Felton SK, et al. 1,25(OH)2 vitamin d inhibits foam cell formation and suppresses macrophage cholesterol uptake in patients with type 2 diabetes mellitus. Circulation. 2009;120(8):687–98. https://doi.org/10.1161/CIRCULATIONAHA.109.856070.
Riek AE, Oh J, Bernal-Mizrachi C. 1,25(OH)2 vitamin D suppresses macrophage migration and reverses atherogenic cholesterol metabolism in type 2 diabetic patients. J Steroid Biochem Mol Biol. 2013;136:309–12. https://doi.org/10.1016/j.jsbmb.2012.12.019.
Watson KE, Abrolat ML, Malone LL, et al. Active serum vitamin D levels are inversely correlated with coronary calcification. Circulation. 1997;96(6):1755–60. https://doi.org/10.1161/01.cir.96.6.1755.
Martins D, Wolf M, Pan D, et al. Prevalence of cardiovascular risk factors and the serum levels of 25-hydroxyvitamin D in the United States: data from the third national health and nutrition examination survey. Arch Intern Med. 2007;167(11):1159–65. https://doi.org/10.1001/archinte.167.11.1159.
Khan SU, Khan MU, Riaz H, et al. Effects of nutritional supplements and dietary interventions on cardiovascular outcomes: an umbrella review and evidence map. Ann Intern Med. 2019;171(3):190–8. https://doi.org/10.7326/M19-0341.
Bolland MJ, Grey A, Avenell A, Gamble GD, Reid IR. Calcium supplements with or without vitamin D and risk of cardiovascular events: reanalysis of the women’s health initiative limited access dataset and meta-analysis. BMJ. 2011;342:d2040. https://doi.org/10.1136/bmj.d2040.
Heravi AS, Michos ED. Vitamin D and calcium supplements: helpful, harmful, or neutral for cardiovascular risk? Methodist Debakey Cardiovasc J. 2019;15(3):207–13. https://doi.org/10.14797/mdcj-15-3-207.
Chin K, Appel LJ, Michos ED. Vitamin D, calcium, and cardiovascular disease: A"D"vantageous or “D”etrimental? An era of uncertainty. Curr Atheroscler Rep. 2017;19(1):5. https://doi.org/10.1007/s11883-017-0637-2.
Anderson JJ, Kruszka B, Delaney JA, et al. Calcium intake from diet and supplements and the risk of coronary artery calcification and its progression among older adults: 10-year follow-up of the multi-ethnic study of atherosclerosis (MESA). J Am Heart Assoc. 2016;5(10):e003815. https://doi.org/10.1161/JAHA.116.003815.
Palacios S, Borrego RS, Forteza A. The importance of preventive health care in post-menopausal women. Maturitas. 2005;52(Suppl 1):S53–60. https://doi.org/10.1016/j.maturitas.2005.06.013.
Vaananen HK, Harkonen PL. Estrogen and bone metabolism. Maturitas. 1996;23(Suppl):S65–9. https://doi.org/10.1016/0378-5122(96)01015-8.
Rozenberg S, Al-Daghri N, Aubertin-Leheudre M, et al. Is there a role for menopausal hormone therapy in the management of postmenopausal osteoporosis? Osteoporos Int. 2020;31(12):2271–86. https://doi.org/10.1007/s00198-020-05497-8.
Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the women’s health initiative randomized controlled trial. JAMA. 2002;288(3):321–33. https://doi.org/10.1001/jama.288.3.321.
Reyes-Garcia R, Mendoza N, Palacios S, et al. Effects of daily intake of calcium and vitamin D-enriched milk in healthy postmenopausal women: a randomized, controlled double-blind nutritional study. J Womens Health. 2018;27(5):561–8. https://doi.org/10.1089/jwh.2017.6655.
Liu C, Kuang X, Li K, Guo X, Deng Q, Li D. Effects of combined calcium and vitamin D supplementation on osteoporosis in postmenopausal women: a systematic review and meta-analysis of randomized controlled trials. Food Funct. 2020;11(12):10817–27. https://doi.org/10.1039/d0fo00787k.
Avenell A, Mak JC, O’Connell D. Vitamin D and vitamin D analogues for preventing fractures in post-menopausal women and older men. Cochrane Database Syst Rev. 2014;2014(4):CD000227. https://doi.org/10.1002/14651858.CD000227.
Agostini D, Zeppa Donati S, Lucertini F, et al. Muscle and bone health in postmenopausal women: role of protein and vitamin D supplementation combined with exercise training. Nutrients. 2018;10(8):1103. https://doi.org/10.3390/nu10081103.
Acknowledgements
None
Funding
This work was supported by the Major Research Program of National Natural Science Foundation of China (NSFC, 92057119, 31970798, 82071624, 81871143), the Shanghai Natural Science Foundation (23ZR1408200), the Program for Zhuoxue of Fudan University (JIF157602) and the Support Project for Original Personalized Research of Fudan University (IDF157014/002).
Author information
Authors and Affiliations
Contributions
Manuscript draft and data analysis: JWS, JNW; conception and design: JWS, XYZ, WHZ, JJY, and MQL; all authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
National Health and Nutrition Examination Survey (NHANES) is a cross-sectional survey conducted by the National Center for Health Statistics (NCHS) of the Centers for Disease Control and Prevention (CDC), which aimed at collecting information on the health and nutritional status of adults and children in the United States. All NHANES protocols were approved by the CDC’s National Center for Health Statistics Ethics Review Board, and all participants of survey signed written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shi, JW., Wu, JN., Zhu, XY. et al. Association of serum 25-hydroxyvitamin D levels with all-cause and cause-specific mortality among postmenopausal females: results from NHANES. J Transl Med 21, 629 (2023). https://doi.org/10.1186/s12967-023-04413-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12967-023-04413-y