
Abstract
MicroRNAs (miRNAs) are small non-coding RNAs that play critical roles in regulating host gene expression. Recent studies have indicated a role of miRNAs in the pathogenesis of gestational diabetes mellitus (GDM), a common pregnancy-related disorder characterized by impaired glucose metabolism. Aberrant expression of miRNAs has been observed in the placenta and/or maternal blood of GDM patients, suggesting their potential use as biomarkers for early diagnosis and prognosis. Additionally, several miRNAs have been shown to modulate key signaling pathways involved in glucose homeostasis, insulin sensitivity, and inflammation, providing insights into the pathophysiology of GDM. This review summarizes the current knowledge on the dynamics of miRNA in pregnancy, their role in GDM as well as their potential as diagnostic and therapeutic targets.
Similar content being viewed by others


Introduction
According to the World Health Organization (WHO) and the International Federation of Gynecology and Obstetrics (FIGO), Gestational Diabetes Mellitus (GDM) is defined as a pregnancy-related carbohydrate intolerance that is first diagnosed during pregnancy [1, 2]. This results in varying degrees of hyperglycemia and is associated with potential complications such as pre-eclampsia, premature rupture of membranes, cesarean section, preterm delivery, high blood pressure, and babies with large birth weight [3,4,5,6]. The worldwide prevalence of GDM is around 14%, varying based on the population ethnicity and the diagnostic test used [6,7,8]. The American Diabetes Association (ADA) recommends performing the oral glucose tolerance test (OGTT) for the diagnosis of GDM in the second trimester (between 24 and 28 weeks) for low-risk pregnant women, but early diagnosis in the first trimester can identify those at high risk for GDM and prevent adverse complications by adjusting the cut-off points of the OGTT plasma glucose test [9, 10]. Despite that the OGTT can detect up to 80.3% of GDM cases, there is a need for additional diagnostic biomarkers to achieve 100% diagnostic accuracy for GDM cases as early as the first trimester. This would improve outcomes for pregnant women and their infants.
Pregnancy is characterized by physiological and metabolic changes that prepare the mother's body for fetal growth, which is a well-established fact [11, 12]. These include temporal variations in the expression profile of microRNAs (miRNAs), particularly in the first trimester [13]. miRNAs have the potential to identify pregnant women with complications such as preeclampsia (PE), or GDM [13]. These non-coding and highly conserved RNAs are typically 18–22 nucleotides in length and are known to regulate targeted gene expression by binding to their 3'UTR [14]. They are among the most commonly emerging epigenetic regulators for metabolic adaptation during pregnancy [15,16,17]. However, their dysregulation has been associated with several pregnancy complications, including PE, intrauterine growth restriction (IUGR), miscarriage, preterm birth, and GDM [17,18,19,20,21,22]. Interestingly, a panel of miRNAs has already been validated for several other diseases, including gastric cancer, breast cancer, and diabetes [23,24,25], however, there are relatively few studies that have validated the role of miRNAs as a diagnostic biomarker for pregnancy complications, including GDM [26]. Several risk factors, including advanced maternal age, overweight and obesity, macrosomia, history of perinatal complications, diabetes in the family, parity, and Asian ethnicity, are known to play a significant role in the pathogenesis of GDM [6, 27,28,29]. By correlating these risk factors with other established diagnostic biomarkers, it may be possible to achieve an optimal diagnosis of GDM as early as the first trimester.
The objective of this review is to highlight the most dysregulated miRNAs and their mechanisms of action in pregnant women with GDM, as well as to explore their correlation with other risk factors for GDM.
Role of microRNA in GDM
Up-regulated microRNAs and their mechanism of action
miRNAs have been shown to be involved in the regulation of glucose metabolism and insulin secretion. The expression levels of different miRNAs can vary significantly according to gestational age and across different populations [30,31,32,33,34,35,36,37,38,39,40]. For instance, two previous studies showed a significant overexpression of miR7-5P in maternal blood of women with GDM [41, 42]. In vitro validation of the genetic targets revealed a down regulated expression levels for IRS1/2 (Insulin Receptor Substrate) and RAF genes [30, 31]. This can be mediated by the overexpression of miRNA 7 in women with GDM which highlighted its potential role in regulating insulin, GnRH, and inflammatory signaling pathways associated with IRS1/2 and RAF genes [41, 42]. Interestingly, Mexican women with GDM exhibited significantly upregulated levels of miR-9-5p, miR-29a-3p, and miR-330-3p during the second trimester [30]. Notably, miR-9-5p may contribute to GDM by targeting HK-2 (Hexokinase-2), which in turn regulates genes involved in glycolytic pathways such as GLUT1 (glucose transporter 1), PFK (phosphofructokinase), and LDH (lactate dehydrogenase) [43]. Furthermore, miR-9-5p has also been found to be overexpressed in the serum of newly diagnosed individuals with type 2 diabetes (T2D), suggesting a potential role in glucose metabolism regulation [44].
Additionally, several previous studies have reported elevated levels of miR-16-5p, miR17-5p, miR-19a-3p, miR-19b-3p, and miR-20a-5p in the blood of Chinese and Polish women with GDM as early as 16 weeks, with this correlation increasing and persisting throughout the second and third trimesters [31, 32, 45, 46]. The observed upregulation of miRNAs was also shown to be positively correlated with insulin resistance (IR), a known risk factor for GDM [31]. Network analysis of these upregulated miRNAs has revealed their association with five pathways, namely MAPK signaling, insulin signaling, T2D, TGF-β signaling, and mTOR signaling [46]. Abnormal MAPK signaling is associated with pregnancy complications and sensitivity to insulin, while the TGF-β signaling pathway is linked to PE [47]. Furthermore, the mTOR signaling pathway controls energy balance and food intake in the hypothalamus. [48]. Therefore, the dysregulation of these pathways may play a role in the development of GDM. Remarkably, miR-16 has been demonstrated to target multiple genes that participate in various biological processes such as pancreatic β-cell proliferation and apoptosis [49], insulin signaling [50], and insulin receptor substrate (IRS) proteins 1 and 2 which are involved in insulin-like growth factor-I (IGF-I) regulation, a factor closely linked to insulin resistance [46, 51,52,53]. MiR-16 has been found to impact insulin resistance and inhibit cell apoptosis induced by hyperglycemia, by targeting genes involved in biological processes such as insulin signaling, insulin receptor substrate (IRS) proteins 1 and 2, and insulin-like growth factor-I (IGF-I) [50]. Although miR-17-5p and miR-16-5p have been associated with T2D and other metabolic diseases, their exact role in the pathogenesis of GDM remains unclear [54]. Notably, an increase in miR-16-5p expression has been observed during hypoglycemic episodes in individuals with T1D or T2D, with a negative correlation observed with interleukin (IL)-6, intercellular adhesion molecule (ICAM), and vascular cell adhesion molecule (VCAM) [55] (NCT03460899). Moreover, miR-16 has been found to exert distinct anti-inflammatory effects by promoting the secretion of anti-inflammatory factors such as IL-10 and TGF-β, while simultaneously reducing the levels of pro-inflammatory factors including IL-6, TNF-α, MCP-1, and IL-1β [56]. These complex anti-inflammatory mechanisms are mediated through downregulation of several targets including nuclear factor-κB (NF-κB) or NOD-like receptor protein 3 (NLRP3) inflammasome [57]. MiR-16 is a down-regulated target of Toll-like receptor 4 (TLR4) and has been found to be upregulated in patients with acute myocardial infarction [57]. For microRNA-20a-5p, one study has shown its upregulation in pre-eclampsia, which has a close relationship with GDM [58], however, its correlation with IR needs further clarification. In a recent study of 82 European obese pregnant women, a distinct dysregulated pattern of miR-16-5p, -29a-3p, 103-3p, 134-5p, -122-5p, -223-3p, -330-3p, and miR-433-3p was observed throughout pregnancy in both GDM and control groups, nonetheless, the initial increase of miR-433-3p was significant only in the GDM group [33] as shown in Table 1. Furthermore, miR-195-5p has been shown to target genes involved in fatty acid metabolism, particularly during the second trimester [37].
MiR-122-5p was significantly upregulated solely in the third trimester [33]. Interestingly, a previous study conducted on individuals with T2D revealed a negative correlation between miR-122-5p and Bacteriodes uniformis and Phascolarctobacterium Faecium [59]. Considering the metabolic adaptation that occurs during pregnancy is similar to that in metabolic syndrome, it is plausible to suggest a potential association between miRNA and gut microbiota in the regulation of key genes involved in glucose metabolism [59, 60]. Despite showing a positive correlation with gestational weight gain, miR-433-3p has been found to maintain pancreatic beta cell function in high-glucose conditions, indicating a potential role in protecting against diabetes [33, 61].
In normal pregnancies, the induction of endothelial cell apoptosis by trophoblast cells is a crucial mechanism for uterine spiral artery remodeling [62]. However, defective remodeling has been linked to pregnancy complications such as PE and IUGR [63, 64]. MiR-17-5p expression was found to be significantly higher in 30 Turkish women with GDM, with regulatory effects on mitochondrial fusion-related proteins (Mfn1/Mfn2) in trophoblast cells, affecting endothelial cell apoptosis [65]. This upregulation was positively correlated with fasting glucose levels, HbA1C, and total cholesterol, which are known to be associated with endothelial and vascular dysfunction [65]. Since diabetes is known to be associated with endothelial and vascular dysfunction [66], it is becoming a promising biomarker of GDM. MiR-19a and miR-19b were found to have a higher expression level in the blood of Chinese pregnant women with GDM, primarily during the second and third trimesters, though further validation in a larger group is necessary [45]. These miRNAs were also associated with GDM risk factors, such as age, alcoholism, and smoking, which could potentially exacerbate the disease [45]. Moreover, three studies, as detailed in Table 1, have demonstrated a positive association between miR-29a and GDM in women from Canada, Mexico, and various regions in Europe [30, 36, 67]. In addition, miR-155-5p and miR-21-3p were found to have significantly higher plasma expression levels in overweight and obese American women with GDM [35]. These findings suggest that obesity and fetal gender may play a role in the changes in miRNAs observed in women with GDM. However, they need to be confirmed in larger cohorts comprising diverse ethnic and socioeconomic backgrounds and a wider selection of candidate miRNAs.
Multiple miRNAs were also overexpressed in GDM women from different ethnic groups including miR-16–2-3p, miR-1910-5p and miR-92a-3 (Table 1) [37, 68]. These miRNAs showed a positive correlation with the increased pre-pregnancy BMI [69] which can be mediated by modulating the metabolic activity since the higher concentration of the circulatory miR-92a-3p is inversely linked to the metabolic activity of the brown adipose tissue [70] indicating an impaired metabolic status and increased insulin sensitivity [71]. Furthermore, transfection of skeletal muscles with miR-92a-3p appears to affect the expression of genes involved in Janus kinase/signal transducers and activators of transcription (JAK/STAT) signaling pathways, as well as those associated with T2D and hyperglycemia pathways, underscoring its ability to regulate glucose metabolism in response to insulin within skeletal muscle cells [68]. Interestingly, miRNAs implicated in neural development, including miR-183-5p and miR-200b-3p, exhibit increased expression levels during the first trimester in Mexican women with GDM compared to controls, which may be linked to alterations in neurogenesis and cell proliferation (as delineated in Table 1) [72]. Although several studies have reported elevated expression levels of circulatory miR-142, miR-144-3p, and miR-143 in Chinese, Turkish, and German women with GDM compared to controls [31, 37, 74], these results have yet to be validated in larger cohorts [32, 34, 42]. Notably, both miR-144-3p and miR-142 have been shown to be upregulated in peripheral blood mononuclear cells of individuals with T1D and T2D, as well as in women with GDM [73] indicating an overlapping effects in all types of diabetes.
Overexpression of miR-142-3p in the blood and embryonic tissue of GDM-induced mice showed to promote the proliferation β-cells through targeting FOXO1 gene which is known to control glycogenolysis and gluconeogenesis [74, 75]. Overexpression of miR-142-3p was observed only in pre-T2D women, showing a positive association with insulin, HOMA-IR, BMI, adiponectin, and leptin levels in in obese individuals [76,77,78]. In addition, upregulated expression and a positive correlation with HOMA-IR of circulating miR-144-3p were observed in a Chinese cohort with impaired fasting glucose making it a predictor of T2D development [79]. Higher circulatory levels of let-7 g was observed in Estonian and Caucasian women with GDM [34, 37]. However, in the Caucasian population, this higher expression was solely reported in the screening group and not in the validation group [34]. The regulatory function of the miRNA-let-7 family in the glucose metabolism is widely recognized, with altered expression levels being associated with metabolic disorders such as T2D [80, 81] indicating similarities in different miRNA induced metabolic pathways. Two studies investigated higher expression of miR-195 in plasma of Estonian and Chinese women with GDM compared to controls [37, 82] which was positively associated with increased BMI, obesity and fasting blood glucose level in patients with metabolic syndrome [83], indicating that aberrant expression of miR-195-5p might function as a novel diagnostic biomarker for GDM.
Australian women with GDM showed elevated levels of miR-197 in their placental exosomes, which were found to be correlated with insulin sensitivity in skeletal muscle tissues [84]. In contrast, Mexican women with GDM had higher expression levels of miR-16-5p and miR-222 only during their second trimester, as detected in placental exosomes isolated from urine samples. [85]. Most of genes that are targeted by miR-16-5p and miR-222-3p are involved in the insulin resistance pathway [54, 86] highlighting the role of these miRNAs in modulating different metabolic processes in women with GDM. Moreover, multiple miRNAs including miR‒122-5p; miR‒210-3p; miR‒29a-3p; miR‒29b-3p; miR‒342-3p, and miR-520 h (Table 1) showed significantly higher levels in GDM cases than in controls. These miRNAs are involved in trophoblast proliferation/differentiation as well as in insulin secretion/regulation and glucose transport during pregnancy [36]. In addition, two independent studies found elevated levels of miR222 in omental adipose tissue and plasma samples collected from Chinese and Canadian women with GDM, respectively [37, 87]. Interestingly, miR222 has been shown to impact glucose uptake in mature adipocytes by regulating the expressions of estrogen receptor ERα and insulin-sensitive membrane transporter GLUT4, suggesting its potential as both a biomarker and therapeutic target for GDM [87]. Additionally, two other studies reported increased levels of miR-223 in serum and plasma samples from women diagnosed with GDM, originating from Italy, Spain and Egypt, respectively [88]. This was correlated with the increased levels of angiopoietin-like protein 8 (ANGPTL8) in addition to lipid markers and fasting blood glucose [88]. Upregulation of miR-330 was observed in serum and plasma of Italian, Mexican, Spanish, and Turkish women with GDM compared to controls as shown in Table 1 [30, 38, 39]. MiR-330-3p is known to target genes involved in beta-cell proliferation and differentiation in addition to insulin secretion, such as E2F1, CDC42 and AGT2R2 [38].
In a previous study, miRNA 340 was significantly elevated in GDM patients [34]. While not all GDM subjects exhibited this elevation in comparison to their matched control group, it was positively linked with insulin levels and BMI, as well as the expression levels of the Poly (A) Binding Protein Interacting Protein 1(PAIP1) gene in these women [34]. Interestingly, miRNA-340 has been recently identified as being differentially expressed in diabetic conditions, such as newly diagnosed T1D children [89]. Functional investigations have shown that miRNA-340 responds to insulin and glucose stimuli in cultured lymphocytes suggesting that it may play a crucial role in the alterations in gene expression induced by hyperinsulinemia [34]. Furthermore, miRNA 503 was found to be upregulated in both blood and placenta samples obtained from women with GDM [90]. Notably, miR-503 has been shown to regulate pancreatic β-cell activity by targeting the mTOR pathway, implying that targeting the miR-503/mTOR axis could be a promising therapeutic strategy for GDM [90]. Interestingly, miRNAs isolated from extracellular vesicles in blood, such as miR-520 h, miR-1323, miR-136-5p, and miR-342-3p, were also significantly upregulated in women with GDM [36, 91] Among these, miR-520 h was found to inhibit cell viability and promote cell apoptosis by regulating mTOR expression in a GDM cell model [91]. Additionally, miR-1323 was shown to suppress trophoblast cell viability by downregulating the expression of TP53INP1 gene, highlighting its potential as a therapeutic target for GDM. Moreover, two separate studies reported higher expression levels of miR-657 in placental and placental-derived mononuclear macrophages in women with GDM [92, 93]. The dysregulation of miR-657 has been shown to impact the placental inflammatory response in GDM through its targeting of the IL-37/NF-κB signaling axis [92, 93]. Additionally, it regulates macrophage proliferation, migration, and polarization by targeting FAM46C, suggesting that it holds promise as both a diagnostic and therapeutic target for GDM [92, 93]. While many other miRNAs have been investigated in various studies, we have specifically focused on the most common and significant miRNAs (as depicted in Figs. 1 and 2), along with their known mechanisms of action, highlighting their potential clinical applications for GDM patients.

Dynamics of the most common significantly dysregulated miRNA in pregnant women with GDM. List of upregulated and downregulated miRNAs during pregnancy progression.

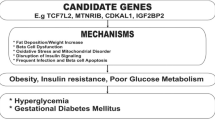
Mechanisms of action for the most common significantly dysregulated miRNA in pregnant women with GDM
Controversial and down-regulated miRNA profiles in GDM
In the preceding section, we provided a summary of the most prevalent and significant upregulated miRNAs in women with GDM. In this section, we have shifted our focus to the controversial and significantly down-regulated miRNAs. While several miRNAs were found to be significantly upregulated across various GDM cohorts, there were also conflicting results. For instance, miR-9-5p and miR-137 demonstrated a significant upregulation pattern in the blood of women with GDM (as illustrated in Table 1). However, in placental tissues from women with GDM and an associated risk of macrosomia, the opposite—a down-regulated level—was observed [30, 94, 95].
Furthermore, miRNAs such as miR-27a, miR-137, miR-92a, miR-33a, miR-30d, miR-362-5p, and miR-502-5p were downregulated in women with GDM, and they are known to target the epidermal growth factor receptor/Class I phosphoinositide—3 kinases (EGFR/PI3K/Akt) pathway, which sheds light on the potential mechanisms underlying GDM and the associated risk of macrosomia [95]. Although some miRNAs, such as miR-16-5p, miR-17-5p, and miRNA 19, were significantly increased in Chinese and Turkish women with GDM and polycystic fibrosis [45, 96], their association with GDM was not observed in Caucasian and South African women [34, 40]. As previously mentioned, the expression levels of certain miRNAs in women with GDM show variations among different ethnic groups. For instance, miR-20a-5p was found to be significantly upregulated in Chinese pregnant women with GDM, while a study on South African pregnant women reported a significant downregulation of miR-20a-5p and miR-222-3p in the GDM group, which affected genes not related to GDM [31, 40, 46]. Meanwhile, American women with GDM showed no significant difference in the expression of miR-222 and miR-223 in their plasma [35]. Interestingly, miR-29a was found to have a significantly higher level in plasma of Canadian women with GDM, but two previous studies on Chinese women with GDM showed a significantly downregulated pattern of miR-29a and miR-29b in serum and placental samples, respectively [35, 36, 97, 98].
These down-regulated miRNAs can partially play a role in the pathogenies of GDM through modulating glucose metabolism and Placental trophoblast development via targeting the Insulin-induced gene 1 (Insig1) and Hypoxia Inducible Factor 3 Subunit Alpha (HIF3A) gene by miRNA 29a and 29b respectively [97, 98]. Furthermore, miR-30d expression in the placenta has been found to be significantly associated with GDM, as it enhances trophoblast proliferation and glucose uptake capacity by targeting Ras-Related Protein Rab-8A (RAB8A) gene [99]. On the other hand, a lower expression of miR-96 in placental and blood samples of women with GDM has been reported, which affects trophoblast viability and promotes the functions of pancreatic β cells via targeting P21 Protein (Cdc42/Rac)-Activated Kinase (PAK1) gene [105, 106]. These findings shed light on the mechanisms and diagnostic targets of GDM. However, there are conflicting results regarding miR-21 and miR-155, which have been found to be significantly elevated in plasma of American women with GDM [35], but not in Turkish women [96, 100].
The lower expression of miR-21 and miR-155 in Turkish women has been linked to both GDM and PE, suggesting that the expression pattern of miRNA can be influenced by the presence of other pregnancy complications [100]. In Chinese women with GDM, a significant downregulation of miR494 in peripheral blood samples was observed, which inhibited pancreatic β-cell function by targeting the Protein Tyrosine Phosphatase (PTEN) signaling cascade, highlighting a potential therapeutic target for GDM [101]. However, a trend towards increased levels of miR-494-3p was observed in the serum of Canadian women with GDM, but this was not statistically significant [36]. In Italian women with GDM, a downregulation of both miR-548c-3p and miR-532-3p was observed in the screening group but not the validation group [38]. These findings suggest that variation in the miRNA profiles can arise from differences in sample type, gestational age, ethnic group, and the presence of other pregnancy complications. To develop a novel diagnostic panel for GDM, it is useful to focus on the most common dysregulated miRNA profiles across populations (as shown in Figs. 1 and 2) and to replicate these findings in larger pregnancy cohorts.
Future directions for use of miRNA as a diagnostic tool
This review has highlighted the significant variability in miRNA expression across different studies, which can be influenced by various factors including medication use, diet, physical activity, ethnicity, socioeconomic and environmental factors, and viral infections [102,103,104,105,106]. Another factor is the variations in the gestational ages between pregnant women [85]. Furthermore, technical factors such as sample collection and storage, miRNA isolation procedures, measurement platforms, and normalization methods can also affect miRNA expression levels [107,108,109]. To improve reproducibility across studies, standard protocols for sample collection, transport, and storage, as well as miRNA isolation procedures and data analysis, should be developed. Using miRNA panels rather than individual miRNAs can also enhance their clinical applicability, given their ability to regulate multiple genes involved in different biological processes in various diseases [104, 110].
Technological advancements in sequencing can pave the way for the use of miRNAs as inexpensive clinically applicable biomarkers in the future, although pre-analytical, analytical, and biological challenges must first be addressed to overcome poor reproducibility between studies. Although OGTT remains the gold standard diagnostic test for GDM, it is primarily applicable between 24 and 28 weeks of gestation. Therefore, early diagnosis may only be possible by lowering the glucose level cut-off points. Thus, additional early diagnostic markers such as miRNAs are necessary to achieve optimal diagnosis of GDM as early as the first trimester, enabling timely treatment to prevent potential complications of GDM.
In conclusion, dysregulated miRNAs in women with GDM have the potential to serve as noninvasive biomarkers, aiding in the identification of underlying mechanisms for gestational diabetes and associated pregnancy complications. Advanced functional studies are necessary to validate and improve our understanding of these miRNAs by investigating their target genes and pathways. Such studies may help to uncover the link between GDM subtypes and pregnancy outcomes, providing valuable insights into the pathogenesis of GDM.
Availability of data and materials
Not applicable.
References
Knowler WC, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346(6):393–403.
Ramachandran A, et al. The Indian diabetes prevention programme shows that lifestyle modification and metformin prevent type 2 diabetes in Asian Indian subjects with impaired glucose tolerance (IDPP-1). Diabetologia. 2006;49(2):289–97.
Herman WH, et al. The cost-effectiveness of lifestyle modification or metformin in preventing type 2 diabetes in adults with impaired glucose tolerance. Ann Intern Med. 2005;142(5):323–32.
Tuomilehto J, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med. 2001;344(18):1343–50.
Retnakaran R, et al. Glucose intolerance in pregnancy and future risk of pre-diabetes or diabetes. Diabetes Care. 2008;31(10):2026–31.
Wang H, et al. IDF diabetes Atlas: estimation of global and regional gestational diabetes mellitus prevalence for 2021 by international association of diabetes in pregnancy study group’s criteria. Diabetes Res Clin Pract. 2022;183:109050.
Schmidt MI, et al. Gestational diabetes mellitus diagnosed with a 2-h 75-g oral glucose tolerance test and adverse pregnancy outcomes. Diabetes Care. 2001;24(7):1151–5.
Murgia C, et al. Gestational diabetes mellitus in Sardinia: results from an early, universal screening procedure. Diabetes Care. 2006;29(7):1713–4.
American Diabetes. 2 Classification and diagnosis of diabetes: standards of medical care in diabetes-2021. Diabetes Care. 2021;44(Suppl 1):S15–33.
Plasencia W, et al. Criteria for screening and diagnosis of gestational diabetes mellitus in the first trimester of pregnancy. Fetal Diagn Ther. 2011;30(2):108–15.
Parrettini S, Caroli A, Torlone E. Nutrition and metabolic adaptations in physiological and complicated pregnancy: focus on obesity and gestational diabetes. Front Endocrinol (Lausanne). 2020;11:611929.
Kohlhepp LM, et al. Physiological changes during pregnancy. Anaesthesist. 2018;67(5):383–96.
Legare C, et al. Human plasma pregnancy-associated miRNAs and their temporal variation within the first trimester of pregnancy. Reprod Biol Endocrinol. 2022;20(1):14.
O’Brien J, et al. Overview of MicroRNA biogenesis, mechanisms of actions, and circulation. Front Endocrinol (Lausanne). 2018;9:402.
Mitchell MD, et al. Placental exosomes in normal and complicated pregnancy. Am J Obstet Gynecol. 2015;213(4 Suppl):S173–81.
Poirier C, et al. MicroRNAs in pregnancy and gestational diabetes mellitus: emerging role in maternal metabolic regulation. Curr Diab Rep. 2017;17(5):35.
Cai M, Kolluru GK, Ahmed A. Small molecule, big prospects: MicroRNA in pregnancy and its complications. J Pregnancy. 2017;2017:6972732.
Akgor U, Ayaz L, Cayan F. Expression levels of maternal plasma microRNAs in preeclamptic pregnancies. J Obstet Gynaecol. 2021;41(6):910–4.
Salimi S, et al. Association of polymorphisms in miR146a, an inflammation-associated MicroRNA, with the risk of idiopathic recurrent spontaneous miscarriage: a case-control study. Dis Markers. 2022;2022:1495082.
Kochhar P, et al. microRNA signatures associated with fetal growth restriction: a systematic review. Eur J Clin Nutr. 2022;76(8):1088–102.
Winger EE, et al. MicroRNAs isolated from peripheral blood in the first trimester predict spontaneous preterm birth. PLoS ONE. 2020;15(8):e0236805.
Yoffe L, et al. Early detection of preeclampsia using circulating small non-coding RNA. Sci Rep. 2018;8(1):3401.
So JBY, et al. Development and validation of a serum microRNA biomarker panel for detecting gastric cancer in a high-risk population. Gut. 2021;70(5):829–37.
Zou R, et al. Development and validation of a circulating microRNA panel for the early detection of breast cancer. Br J Cancer. 2022;126(3):472–81.
Khan A, et al. Altered circulating microRNAs in patients with diabetic neuropathy and corneal nerve loss: a pilot study. J Clin Med. 2022. https://doi.org/10.3390/jcm11061632.
Filardi T, et al. Identification and validation of miR-222–3p and miR-409–3p as plasma biomarkers in gestational diabetes mellitus sharing validated target genes involved in metabolic homeostasis. Int J Mol Sci. 2022. https://doi.org/10.3390/ijms23084276.
Di Cianni G, et al. Prevalence and risk factors for gestational diabetes assessed by universal screening. Diabetes Res Clin Pract. 2003;62(2):131–7.
Chen L, et al. Influence of acculturation on risk for gestational diabetes among Asian women. Prev Chronic Dis. 2019;16:E158.
Xiong X, et al. Gestational diabetes mellitus: prevalence, risk factors, maternal and infant outcomes. Int J Gynaecol Obstet. 2001;75(3):221–8.
Martinez-Ibarra A, et al. Unhealthy levels of phthalates and bisphenol a in Mexican pregnant women with gestational diabetes and its association to altered expression of miRNAs involved with metabolic disease. Int J Mol Sci. 2019. https://doi.org/10.3390/ijms20133343.
Cao YL, et al. Plasma microRNA-16-5p, -17-5p and -20a-5p: novel diagnostic biomarkers for gestational diabetes mellitus. J Obstet Gynaecol Res. 2017;43(6):974–81.
Juchnicka I, et al. miRNAs as Predictive Factors in Early Diagnosis of Gestational Diabetes Mellitus. Front Endocrinol (Lausanne). 2022;13:839344.
Sorensen AE, et al. The temporal profile of circulating miRNAs during gestation in overweight and obese women with or without gestational diabetes mellitus. Biomedicines. 2022. https://doi.org/10.3390/biomedicines10020482.
Stirm L, et al. Maternal whole blood cell miRNA-340 is elevated in gestational diabetes and inversely regulated by glucose and insulin. Sci Rep. 2018;8(1):1366.
Wander PL, et al. Circulating early- and mid-pregnancy microRNAs and risk of gestational diabetes. Diabetes Res Clin Pract. 2017;132:1–9.
Gillet V, et al. miRNA profiles in extracellular vesicles from serum early in pregnancies complicated by gestational diabetes mellitus. J Clin Endocrinol Metab. 2019;104(11):5157–69.
Tagoma A, et al. MicroRNA profiling of second trimester maternal plasma shows upregulation of miR-195-5p in patients with gestational diabetes. Gene. 2018;672:137–42.
Sebastiani G, et al. Circulating microRNA (miRNA) expression profiling in plasma of patients with gestational diabetes mellitus reveals upregulation of miRNA miR-330-3p. Front Endocrinol (Lausanne). 2017;8:345.
Pfeiffer S, et al. Circulating miR-330-3p in late pregnancy is associated with pregnancy outcomes among lean women with GDM. Sci Rep. 2020;10(1):908.
Pheiffer C, et al. Decreased expression of circulating miR-20a-5p in South African women with gestational diabetes mellitus. Mol Diagn Ther. 2018;22(3):345–52.
Bhushan R, et al. MicroRNA-7 regulates insulin signaling pathway by targeting IRS1, IRS2, and RAF1 genes in gestational diabetes mellitus. Microrna. 2022;11(1):57–72.
Balci S, et al. Expression level of miRNAS in patients with gestational diabetes. Turkish J Biochem. 2020;45(6):825–31.
Zhang X, et al. Association of gestational diabetes mellitus and abnormal vaginal flora with adverse pregnancy outcomes. Medicine (Baltimore). 2018;97(34):e11891.
Kong L, et al. Significance of serum microRNAs in pre-diabetes and newly diagnosed type 2 diabetes: a clinical study. Acta Diabetol. 2011;48(1):61–9.
Wang F, Zhang X, Zhou H. Role of cell free microRNA-19a and microRNA-19b in gestational diabetes mellitus patients. 3 Biotech. 2019;9(11):406.
Zhu Y, et al. Profiling maternal plasma microRNA expression in early pregnancy to predict gestational diabetes mellitus. Int J Gynaecol Obstet. 2015;130(1):49–53.
Perucci LO, et al. Soluble endoglin, transforming growth factor-Beta 1 and soluble tumor necrosis factor alpha receptors in different clinical manifestations of preeclampsia. PLoS ONE. 2014;9(5):e97632.
Kumar A, et al. Fat cell-specific ablation of rictor in mice impairs insulin-regulated fat cell and whole-body glucose and lipid metabolism. Diabetes. 2010;59(6):1397–406.
Gao X, Zhao S. miRNA-16-5p inhibits the apoptosis of high glucose-induced pancreatic beta cells via targeting of CXCL10: potential biomarkers in type 1 diabetes mellitus. Endokrynol Pol. 2020;71(5):404–10.
Ye EA, Steinle JJ. miR-15b/16 protects primary human retinal microvascular endothelial cells against hyperglycemia-induced increases in tumor necrosis factor alpha and suppressor of cytokine signaling 3. J Neuroinflammation. 2015;12:44.
Carew RM, et al. Insulin receptor substrate 2 and FoxO3a signalling are involved in E-cadherin expression and transforming growth factor-beta1-induced repression in kidney epithelial cells. FEBS J. 2011;278(18):3370–80.
Geng Y, et al. Insulin receptor substrate 1/2 (IRS1/2) regulates Wnt/beta-catenin signaling through blocking autophagic degradation of dishevelled2. J Biol Chem. 2014;289(16):11230–41.
Hubal MJ, et al. Circulating adipocyte-derived exosomal MicroRNAs associated with decreased insulin resistance after gastric bypass. Obesity (Silver Spring). 2017;25(1):102–10.
Guarino E, et al. Circulating MicroRNAs as biomarkers of gestational diabetes mellitus: updates and perspectives. Int J Endocrinol. 2018;2018:6380463.
Eyileten C, et al. Alteration of circulating platelet-related and diabetes-related microRNAs in individuals with type 2 diabetes mellitus: a stepwise hypoglycaemic clamp study. Cardiovasc Diabetol. 2022;21(1):79.
Liang X, et al. MicroRNA-16 suppresses the activation of inflammatory macrophages in atherosclerosis by targeting PDCD4. Int J Mol Med. 2016;37(4):967–75.
Yang Y, et al. miR-16 inhibits NLRP3 inflammasome activation by directly targeting TLR4 in acute lung injury. Biomed Pharmacother. 2019;112:108664.
Wang W, et al. Preeclampsia up-regulates angiogenesis-associated microRNA (i.e., miR-17, -20a, and -20b) that target ephrin-B2 and EPHB4 in human placenta. J Clin Endocrinol Metab. 2012;97(6):E1051-9.
Li L, et al. Correlation between alterations of gut microbiota and miR-122-5p expression in patients with type 2 diabetes mellitus. Ann Transl Med. 2020;8(22):1481.
Nuriel-Ohayon M, Neuman H, Koren O. Microbial changes during pregnancy, birth, and infancy. Front Microbiol. 2016;7:1031.
Wang M. miR-433 protects pancreatic beta cell growth in high-glucose conditions. Mol Med Rep. 2017;16(3):2604–10.
Badacz R, et al. Expression of miR-1–3p, miR-16–5p and miR-122–5p as possible risk factors of secondary cardiovascular events. Biomedicines. 2021. https://doi.org/10.3390/biomedicines9081055.
Bhatt MP, et al. C-peptide activates AMPKalpha and prevents ROS-mediated mitochondrial fission and endothelial apoptosis in diabetes. Diabetes. 2013;62(11):3851–62.
Brosens JJ, Pijnenborg R, Brosens IA. The myometrial junctional zone spiral arteries in normal and abnormal pregnancies: a review of the literature. Am J Obstet Gynecol. 2002;187(5):1416–23.
Li J, et al. MicroRNA-17–5p acts as a biomarker and regulates mitochondrial dynamics in trophoblasts and endothelial cells by targeting the mitofusins Mfn1/Mfn2 in gestational diabetes mellitus. Archiv Med Sci. 2022. https://doi.org/10.5114/aoms/145778.
Dziedzic EA, et al. Vitamin D level is associated with severity of coronary artery atherosclerosis and incidence of acute coronary syndromes in non-diabetic cardiac patients. Arch Med Sci. 2019;15(2):359–68.
Sorensen AE, et al. The predictive value of miR-16, -29a and -134 for early identification of gestational diabetes: a nested analysis of the DALI Cohort. Cells. 2021. https://doi.org/10.3390/cells10010170.
Nair S, et al. Extracellular vesicle-associated miRNAs are an adaptive response to gestational diabetes mellitus. J Transl Med. 2021;19(1):360.
Hod M, et al. The international federation of Gynecology and obstetrics (FIGO) initiative on gestational diabetes mellitus: a pragmatic guide for diagnosis, management, and care. Int J Gynaecol Obstet. 2015;131(Suppl 3):S173-211.
Chen Y, et al. Exosomal microRNA miR-92a concentration in serum reflects human brown fat activity. Nat Commun. 2016;7:11420.
Chondronikola M, et al. Brown adipose tissue improves whole-body glucose homeostasis and insulin sensitivity in humans. Diabetes. 2014;63(12):4089–99.
Lamadrid-Romero M, et al. Central nervous system development-related microRNAs levels increase in the serum of gestational diabetic women during the first trimester of pregnancy. Neurosci Res. 2018;130:8–22.
Collares CV, et al. Identifying common and specific microRNAs expressed in peripheral blood mononuclear cell of type 1, type 2, and gestational diabetes mellitus patients. BMC Res Notes. 2013;6:491.
Zhang T, Ji C, Shi R. miR-142-3p promotes pancreatic beta cell survival through targeting FOXO1 in gestational diabetes mellitus. Int J Clin Exp Pathol. 2019;12(5):1529–38.
Kitamura T. The role of FOXO1 in beta-cell failure and type 2 diabetes mellitus. Nat Rev Endocrinol. 2013;9(10):615–23.
Prats-Puig A, et al. Changes in circulating microRNAs are associated with childhood obesity. J Clin Endocrinol Metab. 2013;98(10):E1655–60.
Al-Rawaf HA. Circulating microRNAs and adipokines as markers of metabolic syndrome in adolescents with obesity. Clin Nutr. 2019;38(5):2231–8.
Prabu P, et al. Circulating MiRNAs of “Asian Indian Phenotype” identified in subjects with impaired glucose tolerance and patients with type 2 diabetes. PLoS ONE. 2015;10(5):e0128372.
Liang YZ, et al. Identification of neuroendocrine stress response-related circulating MicroRNAs as biomarkers for type 2 diabetes mellitus and insulin resistance. Front Endocrinol (Lausanne). 2018;9:132.
Zhu H, et al. The Lin28/let-7 axis regulates glucose metabolism. Cell. 2011;147(1):81–94.
Jiang LQ, et al. Autocrine role of interleukin-13 on skeletal muscle glucose metabolism in type 2 diabetic patients involves microRNA let-7. Am J Physiol Endocrinol Metab. 2013;305(11):E1359–66.
Wang J, et al. Serum miR-195-5p is upregulated in gestational diabetes mellitus. J Clin Lab Anal. 2020;34(8):e23325.
Karolina DS, et al. Circulating miRNA profiles in patients with metabolic syndrome. J Clin Endocrinol Metab. 2012;97(12):E2271–6.
Nair S, et al. Human placental exosomes in gestational diabetes mellitus carry a specific set of miRNAs associated with skeletal muscle insulin sensitivity. Clin Sci (Lond). 2018;132(22):2451–67.
Herrera-Van Oostdam AS, et al. Placental exosomes isolated from urine of patients with gestational diabetes exhibit a differential profile expression of microRNAs across gestation. Int J Mol Med. 2020;46(2):546–60.
Ibarra A, et al. Diabetes in pregnancy and MicroRNAs: promises and limitations in their clinical application. Noncodind RNA. 2018. https://doi.org/10.3390/ncrna4040032.
Shi Z, et al. Differential expression of microRNAs in omental adipose tissue from gestational diabetes mellitus subjects reveals miR-222 as a regulator of ERalpha expression in estrogen-induced insulin resistance. Endocrinology. 2014;155(5):1982–90.
Abdeltawab A, et al. Circulating micro RNA-223 and angiopoietin-like protein 8 as biomarkers of gestational diabetes mellitus. Br J Biomed Sci. 2021;78(1):12–7.
Nielsen LB, et al. Circulating levels of microRNA from children with newly diagnosed type 1 diabetes and healthy controls: evidence that miR-25 associates to residual beta-cell function and glycaemic control during disease progression. Exp Diabetes Res. 2012;2012:896362.
Xu K, et al. microRNA-503 contribute to pancreatic beta cell dysfunction by targeting the mTOR pathway in gestational diabetes mellitus. EXCLI J. 2017;16:1177–87.
Wen J, Bai X. miR-520h Inhibits cell survival by targeting mTOR in gestational diabetes mellitus. Acta Biochim Pol. 2021;68(1):65–70.
Wang P, et al. Dysregulation of microRNA-657 influences inflammatory response via targeting interleukin-37 in gestational diabetes mellitus. J Cell Physiol. 2019;234(5):7141–8.
Wang P, et al. miR-657 promotes macrophage polarization toward M1 by targeting FAM46C in gestational diabetes mellitus. Mediators Inflamm. 2019;2019:4851214.
Peng HY, Li HP, Li MQ. High glucose induces dysfunction of human umbilical vein endothelial cells by upregulating miR-137 in gestational diabetes mellitus. Microvasc Res. 2018;118:90–100.
Li J, et al. A MicroRNA signature in gestational diabetes mellitus associated with risk of macrosomia. Cell Physiol Biochem. 2015;37(1):243–52.
Hocaoglu M, et al. Identification of miR-16-5p and miR-155-5p microRNAs differentially expressed in circulating leukocytes of pregnant women with polycystic ovary syndrome and gestational diabetes. Gynecol Endocrinol. 2021;37(3):216–20.
Zhao C, et al. Early second-trimester serum miRNA profiling predicts gestational diabetes mellitus. PLoS ONE. 2011;6(8):e23925.
Sun DG, et al. The miRNA-29b Is downregulated in placenta during gestational diabetes mellitus and may alter placenta development by regulating trophoblast migration and invasion through a HIF3A-dependent mechanism. Front Endocrinol (Lausanne). 2020;11:169.
Zhang L, et al. Down-regulation of microRNA-30d-5p is associated with gestational diabetes mellitus by targeting RAB8A. J Diabetes Complicat. 2021;35(8):107959.
Hocaoglu M, et al. Differential expression of candidate circulating microRNAs in maternal blood leukocytes of the patients with preeclampsia and gestational diabetes mellitus. Pregnancy Hypertens. 2019;17:5–11.
He Y, et al. miR-494 protects pancreatic beta-cell function by targeting PTEN in gestational diabetes mellitus. EXCLI J. 2017;16:1297–307.
Pheiffer C, et al. MicroRNA profiling in HIV-infected South African women with gestational diabetes mellitus. Mol Diagn Ther. 2019;23(4):499–505.
Florio MC, et al. Aging, MicroRNAs, and heart failure. Curr Probl Cardiol. 2020;45(12):100406.
Krek A, et al. Combinatorial microRNA target predictions. Nat Genet. 2005;37(5):495–500.
Bovell LC, et al. The prognostic value of microRNAs varies with patient race/ethnicity and stage of colorectal cancer. Clin Cancer Res. 2013;19(14):3955–65.
Karere GM, et al. Sex Differences in MicroRNA expression and cardiometabolic risk factors in hispanic adolescents with obesity. J Pediatr. 2021;235:138-143 e5.
Pritchard CC, Cheng HH, Tewari M. MicroRNA profiling: approaches and considerations. Nat Rev Genet. 2012;13(5):358–69.
Wang K, et al. Comparing the MicroRNA spectrum between serum and plasma. PLoS ONE. 2012;7(7):e41561.
Dias S, et al. MicroRNA expression varies according to glucose tolerance, measurement platform, and biological source. Biomed Res Int. 2017;2017:1080157.
Lewis BP, Burge CB, Bartel DP. Conserved seed pairing, often flanked by adenosines, indicates that thousands of human genes are microRNA targets. Cell. 2005;120(1):15–20.
Yu X, et al. miR-96-5p: A potential diagnostic marker for gestational diabetes mellitus. Medicine (Baltimore). 2021;100(21):e25808.
Funding
Open Access funding provided by the Qatar National Library. Financial support is provided to Dr. Souhaila Al Khodor by Sidra Medicine.
Author information
Authors and Affiliations
Contributions
DE and SAK wrote the first draft, reviewed the manuscript, and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
All authors reviewed the final version of the manuscript and approved it for publication.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Elhag, D.A., Al Khodor, S. Exploring the potential of microRNA as a diagnostic tool for gestational diabetes. J Transl Med 21, 392 (2023). https://doi.org/10.1186/s12967-023-04269-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12967-023-04269-2