
Abstract
Background
The etiology of fetal growth restriction (FGR) is complex and currently, there is a paucity of research about the genetic etiology of fetal growth restriction. We investigated the genetic associations and pregnancy outcomes in cases of fetal growth restriction.
Methods
A retrospective analysis of 210 pregnant women with fetal growth restriction was performed using karyotype analysis and single nucleotide polymorphism arrays (SNP-array). The differences in pathogenic copy number variation (CNV) detected by the two methods were compared. At the same time, the fetuses were divided into three groups: isolated FGR (n = 117), FGR with ultrasonographic soft markers (n = 48), and FGR with ultrasonographic structural anomalies (n = 45). Further, the differences in pathogenic copy number variations were compared among the groups.
Results
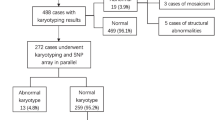
The total detection rate of pathogenic CNVs was 12.4% (26/210). Pathogenic copy number variation was detected in 14 cases (6.7%, 14/210) by karyotype analysis. Furthermore, 25 cases (11.9%, 25/210) with pathogenic CNVs were detected using the SNP-array evaluation method. The difference in the pathogenic CNV detection rate between the two methods was statistically significant. The result of the karyotype analysis and SNP-array evaluation was inconsistent for 13 cases with pathogenic CNV. The rate of detecting pathogenic CNVs in fetuses with isolated FGR, FGR combined with ultrasonographic soft markers, and FGR combined with ultrasonographic structural malformations was 6.0, 10.4, and 31.1%, respectively, with significant differences among the groups. During the follow-up, 35 pregnancies were terminated, two abortions occurred, and 13 cases were lost to follow-up. Of the 160 deliveries, nine fetuses had adverse pregnancy outcomes, and the remaining 151 had normal postnatal growth and developmental assessments.
Conclusions
Early diagnosis and timely genomic testing for fetal growth restriction can aid in its perinatal prognosis and subsequent intervention.
Similar content being viewed by others


Background
Fetal growth restriction (FGR) refers to the condition of inadequate growth of a fetus due to a variety of factors. The American College of Obstetricians and Gynecologists defines FGR in terms of fetal birth mass that is below the 10th percentile of the average body mass for a child of the same gestational age [1]. FGR is a common obstetric complication that is associated with premature delivery, fetal death in utero, neonatal death, and other adverse outcomes [2, 3]. Hence, preventing FGR is significant in improving the pediatric outcomes. However, the etiology of FGR is complex, and can be caused by maternal, fetal, placental, and umbilical cord factors [3]. These factors do not allow the fetus to receive adequate energy and nutrients for growth and development [4].
It is essential to identify the etiology of FGR for better diagnosis and providing possible treatments for this condition. Previous research focused on diagnosis, intrauterine monitoring, treatment, and prognosis of fetuses with FGR; however, currently there are only a few studies on the genetic etiology of FGR. Genetic factors that cause FGR have rarely been reported, and some studies that reported a genetic association were conducted with small sample sizes [5]. Single-nucleotide polymorphism array (SNP-array) can detect copy number variations (CNVs) at a genome-wide level, as well as chimeras (> 30%), loss of heterozygosity, and uniparental disomy (UPD) [6, 7]. SNP-array has been widely used in the diagnosis of fetal structural malformations, primary mental retardation, growth and developmental retardation, autism, and tumors [8, 9]. In this study, we utilized karyotyping and SNP-array for the genomic analysis of 210 fetuses who were prenatally diagnosed with FGR using ultrasound, and investigate the genetic etiology of FGR and evaluate the diagnostic value of SNP-array. The outcomes of these pregnancies were also monitored.
Methods
Patient data
This study retrospectively enrolled 210 pregnant women, who received a prenatal diagnosis of FGR by fetal ultrasound at a tertiary care center between November 2016 and February 2021. The gestational age range was 16–35+6 weeks and the maternal age range was 17–48 years. Depending on the gestational age, amniotic fluid or cord blood samples were collected for karyotype analysis and SNP-array evaluation. The inclusion criteria were as follows: Gestational age determined based on the date of last menstruation, a detailed menstrual history, and ultrasound examination during the first trimester. Fetal abdominal circumference, head circumference, biparietal diameter, and femur length were measured by ultrasound, and the estimated fetal weight was calculated using the Hadlock formula. FGR was defined as a fetal mass below the 10th percentile of the average weight of a normal fetus of the same gestational age [10]. The exclusion criteria were as follows: FGR resulting from a clear maternal cause, such as hypertensive disease during pregnancy, maternal infection, or maternal nutritional abnormalities.
Depending on the co-occurrence of FGR with other ultrasonographic abnormalities into, the patients in this study were divided into three groups i.e., isolated FGR group (117 cases), FGR with ultrasonographic soft markers (48 cases) group, and FGR with ultrasonographic structural malformations (45 cases) group (Fig. 1). Ultrasonographic soft markers refer to abnormalities other than the ultrasonic structure found in the fetal ultrasound examination. They are non-specific indicators and cannot completely indicate fetal structural abnormalities, and may just be normal variations.

Enrollment of Study Participants between November 2016 and February 2021
Karyotype analysis
Using ultrasonography, 30 mL amniotic fluid was extracted. Of this, 20 mL of the fluid was used for cell culture and 10 mL was used for SNP-array. Alternatively, 2.5 mL of cord blood was extracted under ultrasonographic guidance, of which 1.5 mL was used for cell culture and 1.0 mL was used for SNP-array. We also collected 2 mL of peripheral blood from all the pregnant women and their spouses in EDTA anticoagulant tubes. Amniotic fluid or umbilical cord blood samples were extracted and inoculated in RPMI-1640 culture medium (Ningbo Bosheng Medical Technology). Cells were harvested from umbilical cord blood samples after 3 days of culture, and from amniotic fluid samples after 8 days of culture. Thereafter, samples were mounted on drop slides and Giemsa staining was conducted (if necessary, C band and N band were also included). Finally, karyotypes were identified using the GSL-120 automatic chromosome scanning platform (Leica Biosystems, Wetzler, Germany), and karyotype calculation and analysis was performed. Karyotypes were named according to the International System for (Human) Cytogenetic Nomenclature 2016. Forty karyotypes were counted in each case, five were analyzed, and 20 more karyotypes were counted and analyzed in case of any abnormality.
Single-nucleotide polymorphism array
Affymetrix® (Affymetrix, Santa Clara, CA, USA) microarray chips and CytoScan™ (Thermo Fisher Scientific Inc., Waltham, MA, USA) 750 K microarray reagent were used for the SNP-array. Digestion, ligation, amplification, purification, labeling, hybridization, washing, and scanning of DNA samples was conducted according to the standard operating procedures provided by the company. Affymetrix Genechip Microarray Instrumentation System (Affymetrix, California, USA) and the supporting Chromosome Analysis Suite software were used to analyze the data. The SNP results were further analyzed using related databases. The databases used included the international public DGV benign variation database (http:// projects. The tcag. Ca/variation), the international public DECIPHER pathological variation database (https://www.deciphergenomics.org/), the online Human Mendelian genetic database OMIM (http://www.omim.org), the international federation of cell gene chip standardized ISCA (https://www.iscaconsortium.org/), and the global Affymetrix pathological shared database user CAGdb (http://www.cagdb.org/), NCBI, PubMed, etc. The nature of CNVs was determined according to standards and guidelines of the American Society of Medical Genetics for the interpretation and reporting of genetic CNVs. CNVs can be roughly divided into five categories: pathogenic CNV, likely pathogenic CNV, variants of uncertain clinical significance (VUS) CNV, likely benign CNV, and benign CNV [11, 12]. For VUS CNV, it recommended to perform an SNP-array using the parents’ blood samples, combined with a pedigree analysis to further clarify the nature of the CNV.
Pregnancy outcome
All cases were followed up telephonically to obtain information regarding fetal development, pregnancy outcome, and postpartum growth and development.
Statistical analysis
IBM SPSS Statistics for Windows, version 25 (IBM Corp., Armonk, N.Y., USA) was used for statistical analyses. Chi-square test was used for comparison between groups for categorical variables. Statistical significance was set at p < 0.05.
Results
Karyotype analysis
Among 210 cases of FGR, 14 (6.7%, 14/210) had abnormal karyotypes, including nine cases with abnormal chromosomal numbers and five with abnormal structure (Table 1). The parents of fetuses with abnormal karyotypes chose to terminate the pregnancy following genetic counseling. Among nine cases, there were two cases of trisomy 21, two of trisomy 18, three of a sex chromosome abnormality, and two cases of chimeric abnormality. The five cases of chromosomal structural abnormalities consisted of one case of partial deletion, three cases of partial duplication, and one case of chimeric structural abnormalities. Among the 14 abnormal karyotypes, six cases were of isolated FGR and eight cases were of FGR with miscellaneous ultrasonographic abnormalities. The most common ultrasonographic abnormality with FGR was congenital heart disease (five cases). The other three cases had thickened nuchal translucency, small size of the kidneys, and facial deformity, respectively.
Single-nucleotide polymorphism array
Of the 210 samples, SNP-array analysis detected 32 abnormal cases, including 25 cases of pathogenic CNV (11.9%, 25/210), five cases of VUS CNV (2.4%, 5/210), and two cases of benign CNV (1.0%, 2/210) (Tables 1 and 2). The 25 cases of pathogenic CNV included eight cases of aneuploidy, 14 cases of partial deletion/duplication, one case of chimerism, and three cases of UPD.
Of the 32 abnormal cases detected by the SNP-array, 19 cases were normal as per karyotype analysis (Table 2), including six cases of isolated FGR and 13 cases of FGR with miscellaneous ultrasonographic abnormalities. Among the 13 cases with miscellaneous ultrasonographic abnormalities, there were six cases of ventricular septal defect. The 19 cases with normal karyotype analysis but abnormal SNP-array, included 12 cases of pathogenic CNVs, five VUS CNVs, and one benign CNV. The parents of 12 fetuses with pathogenic CNV chose to terminate the pregnancy following genetic counseling. The parents of five fetuses with VUS CNV and one fetus with benign CNV chose to continue the pregnancy.
Comparison of karyotype analysis and SNP-array results
The total detection rate of pathogenic CNVs was 12.4% (26/210) using karyotype analysis and SNP-array. The detection rates of pathogenic CNVs by karyotype analysis alone, and SNP-array alone, were 6.7% (14/210) and 11.9% (25/210), respectively, and the difference between the two methods was statistically significant (χ2 = 3.42, P = 0.046). The results of karyotype analysis and SNP-array were inconsistent in 13 of the 210 samples (Fig. 2), including one case of a low proportion of sex chromosome chimera, nine cases of chromosome microduplication or microdeletion, and three cases of UPD. The low proportion of sex chromosome chimera was detected as normal by the SNP-array analysis. Microduplication, microdeletion, and UPD were normal upon karyotype analysis.

The consistent and inconsistent cases for karyotype analysis and SNP-array. The blue circle represents SNP-array analysis. The red circle represents karyotype analysis. A shows abnormal results detected by karyotype analysis and SNP-array. B shows normal results detected by karyotype analysis and SNP-array
Comparison of pathogenic CNVs in different FGR groups
Fetuses with FGR were divided into three groups according to the presence of ultrasonographic abnormalities: isolated FGR group, FGR with ultrasonographic soft markers group, and FGR with ultrasonographic structural anomalies group. For the group with isolated FGR (n = 117), seven cases of pathogenic CNV were detected with a positivity rate of 6.0%. For FGR with ultrasonic soft markers (n = 48), five cases of pathogenic CNV were detected with a positivity rate of 10.4%. There were 45 cases of FGR with ultrasonographic structural anomalies, and 14 cases of pathogenic CNVs were detected with a positivity rate of 31.1%. The difference in pathogenic CNVs among the three groups was statistically significant (χ2 = 19.138, P = 0.00007) (Fig. 3).

Comparison of pathogenic CNVs in fetuses with FGR among three groups. A isolated FGR group; B FGR with ultrasonographic soft markers group; C FGR with ultrasonographic structural anomalies. The difference in pathogenic CNVs among the three groups was statistically significant
Follow-up and pregnancy outcomes
The 210 FGR cases were followed up to assess the outcomes and to document postnatal development (Table 3). Among them, 35 pregnancies were terminated (nine with normal karyotype analysis and SNP-array results, 26 with pathogenic CNVs), two fetuses were aborted (normal karyotype analysis and SNP-array results), and 13 were lost to follow-up. Of the 160 deliveries, four infants died within 5 months, four were dwarf after birth, one infant was diagnosed with a cardiac defect after birth, and 151 infants demonstrated normal growth and development after birth (Additional file 1).
Discussion
Karyotype analysis can detect both numerical and structural chromosomal anomalies. In this study, karyotype analysis detected eight cases of abnormal chromosome number and six cases of structural chromosomal abnormality in FGR fetuses. Conventional karyotype analysis can only detect abnormal results in chromosomes larger than 10 Mb, but cannot detect minor structural chromosomal anomalies. SNP-array analysis can detect microdeletions, microduplications, and UPD, but cannot detect balanced translocation chromosomal abnormalities and low proportion chimerism [13]. In this study, SNP-array analysis was used to identify not only pathogenic CNVs that were detected by karyotype analysis, but also nine additional microdeletions or microduplications of less than 5 Mb in size as well as three cases of UPD. The detection rates of pathogenic CNVs in cases of FGR detected using karyotype analysis and SNP-array evaluation were 6.7% (14/210) and 11.9% (25/210), respectively, and the results were statistically significant. Therefore, SNP-array may have advantages for etiological investigation of FGR [14, 15]. However, it should be noted that the karyotype analysis result of a specific FGR case was low proportion of sex chromosome chimera, while the SNP-array for the same case was normal. Karyotype analysis may have an advantage over SNP-array analysis in detecting low proportions of chimera. Therefore, a combination of karyotype analysis and SNP-array analysis is recommended for the evaluation of genetic etiologies in cases of FGR.
The pathogenesis and mechanisms involved in FGR are complex. It has been suggested that approximately 7% of FGR is caused as a result of chromosome aneuploidy [15,16,17]. In this study, the chromosome aneuploidy rate in cases of FGR was 4.3% (9/210), which was slightly lower than that reported in previous studies. It has been reported that the genetic etiology of FGR is not only related to structural chromosomal abnormalities or aneuploidy, but also to chromosomal microdeletion/microduplication [2, 18]. Gruchy et al. performed chromosome microarray analysis (CMA) on 38 pregnant women with FGR or/combined multiple fetal malformations and found that CMA could detect 8% of meaningful chromosomal abnormalities under normal karyotype analysis [19]. Using SNP-array evaluation, we detected an additional 5.7% (12/210) pathogenic genomic abnormalities, which was slightly less than the value reported earlier. Chen et al. [20] proposed that 22q11.2 microdeletion syndrome in a fetus can likely lead to FGR combined with congenital heart disease. In our study, 22q11.2 microdeletion syndrome was detected in one FGR fetus with congenital heart disease, while 22q11.2 microduplication syndrome was detected in another FGR fetus along with other structural malformations. Similarly, Wolf-Hirschhorn syndrome is a common genomic disease that can reportedly cause FGR [18, 21]. The main locus contributing to FGR is on chromosome 4p16.3, and TACC3 [22] and SLBP [23], which are found in the very same region, may be candidate genes for FGR. In our study, an FGR fetus with CNV microdeletion (6.5 MB) on chromosome 4p16.3 was identified, and ultrasonography detected FGR and pulmonary stenosis in the fetus.
Changes in the gene imprinting regions of some chromosomes and UPD may also lead to FGR. Three cases in this study had UPD. Further, chromosome 6q24 has gene imprinting regions [24], including PLAG1 and HYMAI genes, and abnormalities in these may lead to fetal intrauterine growth retardation, temporary neonatal diabetes, macroglossia, or umbilical hernia. SNP-array analysis confirmed the existence of heterozygous deletion on chromosome 6 in a fetus, and paternal UPD was identified via pedigree analysis. Fetal ultrasonography in this case revealed FGR, echogenic bowel, mild tricuspid regurgitation, and reverse ductus alpha wave.
Prader-Willi syndrome (PWS) is a typical example of imprinting inheritance [25]. Maternal UPD on chromosome 15 can lead to PWS, and the main intrauterine manifestations of PWS are reduced fetal movement and FGR [26]. This study confirmed that one fetus had maternal UPD on chromosome 15 (PWS), and ultrasonographic findings of this fetus revealed FGR and polyhydramnios. Moreover, imprinted genes on chromosome 2 [27] are also associated with fetal growth restriction, growth retardation, heart malformation, hypospadias, and oligohydramnios. In our study, chromosome 2 of one of the fetuses exhibited maternal UPD, and ultrasonography demonstrated FGR, persistent left superior vena cava, and renal parenchyma echo enhancement in the fetus. These cases confirmed that the genetic etiology of FGR was not only related to chromosomal structural abnormalities or aneuploidy but also chromosomal submicroscopic abnormalities and UPD.
An et al. [28] carried out invasive prenatal diagnoses of isolated FGR fetuses and found that the detection rate of chromosomal karyotype abnormalities was 9.4%, among which the detection rate of CMA was 5.5%. Borrell et al. [29] conducted a meta-analysis using CMA analysis of FGR fetuses with normal karyotypes and found that that the abnormal detection rate of CMA in fetuses with isolated FGR and normal karyotype was 4%. In this study, fetuses were divided into isolated FGR group—FGR with ultrasonographic soft markers and FGR with ultrasonographic structural anomalies. The rates of pathogenic CNVs in fetuses with isolated FGR, FGR combined with ultrasonographic soft markers, and FGR combined with ultrasonographic structural anomalies were 6.0%, 10.4%, and 31.1%, respectively. FGR with ultrasonographic structural anomalies had a high rate of pathogenic CNVs due to high prevalence of fetal anomalies caused by genomic abnormalities. This study showed that the group with isolated FGR had 6% pathogenic CNVs. Therefore, identification of genetic causes in FGR using karyotype analysis and SNP-array analysis is recommended, irrespective of whether the FGR is isolated or combined with other ultrasonographic findings.
This study had certain limitations. Firstly, the samples were not analyzed based on age group, and maternal age may also be a factor influencing FGR. Secondly, the diagnosis of FGR was based on the ultrasonographic measurement standard at our institution, which may have some variation. Thirdly, the participants in this study were more likely to terminate their pregnancies after being informed of the presence of fetal pathogenic CNVs; thus, there was a lack of long-term follow up to evaluate the prognoses of the cases being investigated. VUS is challenging for laboratory technicians and clinical consultants—the detection rate of VUS is dependent on the type of microarray chip and the study population [30, 31]. According to literature, VUS accounts for 5.2% of FGR cases [30]. In this study, VUS accounted for 2.4% (5/210) of the FGR cases, which was lower than that reported previously. The five fetuses with VUS in this study developed well das determined during postnatal follow-ups, while nine FGR cases with normal karyotype and abnormal SNP-array had adverse pregnancy outcomes. Next-generation sequencing may provide a comprehensive prenatal diagnostic tool for use in cases of FGR as a new technique for the detection of single gene mutations and CNVs, and allow for improved evaluation of fetal prognosis.
Conclusion
As a prenatal diagnostic tool in FGR, SNP-array analysis is not only conducive to the discovery of FGR-related genomic abnormalities but also for accurate assessment of fetal prognosis, which can aid in genetic counseling. Early diagnosis of FGR and timely detection of genomic abnormalities will positively impact fetal intervention and perinatal prognosis in cases of FGR. Such diagnostic modalities can make it possible to prevent the etiology of FGR and reduce its consequences.
Availability of data and materials
All data generated during and/or analyzed during the current study are available upon request by contact the corresponding author.
Abbreviations
- FGR:
-
Fetal growth restriction
- SNP-array:
-
Single-nucleotide polymorphism array
- CNVs:
-
Copy number variations
- CNVs:
-
Copy number variations
References
ACOG Practice bulletin no. 134: fetal growth restriction. Obstet Gynecol. 2019; 121(5):1122-1133
Nardozza L, Caetano A, Zamarian A, Mazzola JB, Júnior E. Fetal growth restriction: current knowledge. Arch Gynecol Obstet. 2017;295:1–17.
Figueras F, Gratacós E. Update on the diagnosis and classification of fetal growth restriction and proposal of a stage-based management protocol. Fetal Diagn Ther. 2014;30:86–98.
Figueras F, Caradeux J, Crispi F, Eixarch E, Peguero A, Gratacos E. Diagnosis and surveillance of late-onset fetal growth restriction. Am J Obstet Gynecol. 2018. https://doi.org/10.1016/j.ajog.2017.12.003.
Chen Y, Xie Y, Jiang Y, Luo Q, Shi L, Zeng S, Zhuang J, Lyu G. The genetic etiology diagnosis of fetal growth restriction using single-nucleotide polymorphism-based chromosomal microarray analysis. Front Pediatr. 2021;9:743639.
Zhang Y, Zhong M, Zheng D. Chromosomal mosaicism detected by karyotyping and chromosomal microarray analysis in prenatal diagnosis. J Cell Mol Med. 2021;25(1):358–66.
Brady PD, Vermeesch JR. Genomic microarrays: a technology overview. Prenat Diagn. 2012;32(4):336–43.
Srebniak MI, Opstal DV, Joosten M, Diderich K, Vries F, Riedijk S, et al. Whole-genome array as a first-line cytogenetic test in prenatal diagnosis. Ultrasound Obstet Gynecol. 2015;45(4):363–72.
Melanie M, Louanne H. Array-based technology and recommendations for utilization in medical genetics practice for detection of chromosomal abnormalities. Genet Med. 2010;12(11):742–5.
Choi HY, Kim JH, Park JY, Jung EY, No JH, Oh KJ, Hong JS. Simple mathematical formulae for estimation of median values of fetal biometry at each gestational age. Obstet Gynecol Sci. 2016;59:91–6.
South ST, Lee C, Lamb AN, Higgins AW, Kearney HM. ACMG Standards and Guidelines for constitutional cytogenomic microarray analysis, including postnatal and prenatal applications: revision 2013. Genet Med. 2013;15(11):901–9.
Kearney HM, Thorland EC, Brown KK, Quintero-Rivera F, South ST. American College of Medical Genetics standards and guidelines for interpretation and reporting of postnatal constitutional copy number variants. Genet Med. 2011;13(7):680–5.
Jelin A, Sagaser K, Lawson C, Forster KR, Blakemore K. Chromosomal microarray analysis results from pregnancies with various ultrasonographic anomalies. Obstet Gynecol. 2019;133(4):827–8.
Zhu H, Lin S, Huang L, He Z, Huang X, Zhou Y, Fang Q, Luo Y. Application of chromosomal microarray analysis in prenatal diagnosis of fetal growth restriction. Prenat Diagn. 2016;36:686.
Vanlieferinghen S, Bernard JP, Salomon LJ, Chalouhi GE, Russell NE, Ville Y. Second trimester growth restriction and underlying fetal anomalies. Gynecol Obstet Fertil. 2014;42(9):567–71.
Snijders RJ, Sherrod C, Gosden CM, Nicolaides KH. Fetal growth retardation: associated malformations and chromosomal abnormalities. Am J Obstet Gynec. 1993;168:547–55.
Maulik D. Fetal growth restriction: the etiology. Clin Obstet Gynecol. 2006;49(2):228–35.
Xing Y, Holder JL, Liu Y, Sun L. Prenatal diagnosis of Wolf-Hirschhorn syndrome: from ultrasound findings, diagnostic technology to genetic counseling. Arch Gynecol Obstet. 2018;298(2):289–95.
Gruchy N, Decamp M, Richard N, Leporrier N. Array CGH analysis in high-risk pregnancies: comparing DNA from cultured cells and cell-free fetal DNA. Prenat Diagn. 2012;32(4):383–8.
Chen M, Hwu WL, Kuo SJ, Chen CP, Lin C-C. Subtelomeric rearrangements and 22q11.2 deletion syndrome in anomalous growth-restricted fetuses with normal or balanced G-banded karyotype. Ultrasound Obstet Gynecol. 2006;28(7):939–43.
Zhen L, Fan SS, Huang LY, Pan M, Han J, Yang X, Li DZ. Prenatal diagnosis of Wolf-Hirschhorn syndrome: ultrasonography and molecular karyotyping results. Eur J Obstet Gynecol Reprod Biol. 2018;225:19–21.
Guo Y, Scheuermann TH, Partch CL, Tomchick DR, Gardner KH. Coiled-coil coactivators play a structural role mediating interactions in hypoxia-inducible factor heterodimerization. J Biol Chem. 2015;290(12):7707–21.
Narita T, Yung TM, Yamamoto J, Tsuboi Y, Tanabe H, Tanaka K, Yamaguchi Y, Handa H. NELF interacts with CBC and participates in 3’ end processing of replication-dependent histone mRNAs. Mol Cell. 2007;26(3):349–65.
Docherty LE, Kabwama L, Hawke H, Flanagan SE, Ellard H. Clinical presentation of 6q24 transient neonatal diabetes mellitus (6q24 TNDM) and genotype-phenotype correlation in an international cohort of patients. Diabetologia. 2013;56(4):758–62.
Mian-Ling Z, Yun-Qi C, Chao-Chun Z. Prader-willi syndrome: molecular mechanism and epigenetic therapy. Curr Gene Ther. 2020;20:36–43.
Hu Y, Xue XD, Fu JH. Case report: clinical analysis of seven neonates with prader-willi syndrome and review of the literature. Front Pediatr. 2021;9:633532.
Carmichael H, Shen Y, Nguyen T, Hirschhorn J, Dauber A. Whole exome sequencing in a patient with uniparental disomy of chromosome 2 and a complex phenotype. Clin Genet. 2013;84(3):213–22.
An G, Lin Y, Xu LP, Yang F. Application of chromosomal microarray to investigate genetic causes of isolated fetal growth restriction. Mol Cytogenet. 2018;11:33–9.
Borrell A, Grande M, Pauta M, Figueras F. Chromosomal microarray analysis in fetuses with growth restriction and normal karyotype: a systematic review and meta-analysis. Fetal Diagn Ther. 2018;44(1):1–9.
Wapner RJ, Martin CL, Levy B, Jackson L. Chromosomal microarray versus karyotyping for prenatal diagnosis. N Engl J Med. 2012;367(23):2175–84.
Ganapathi M, Nahum O, Levy B. Prenatal diagnosis using chromosomal SNP microarrays. Methods Mol Biol. 2019;1885:187–205.
Acknowledgements
We thank the patients that participated in this study.
Funding
This work was funded by the Fujian Provincial Natural Science Foundation (2021J01407) and Fujian provincial health technology project (2020GGA020).
Author information
Authors and Affiliations
Contributions
MC collected data and wrote the manuscript. NL designed study and searched literature. XF and LS researched data. XW and XX managed study. SX designed study. LX interpreted data. HH designed study and revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Fujian Maternal and Child Health Hospital (Approval No. 2014042). All procedures were applied following the Declaration of Helsinki, as well as international and national laws, guidelines and regulations. Signed informed consent was obtained from all the pregnant women enrolled in this study.
Consent for publication
All authors consented to publish.
Competing interests
The authors declare no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Detailed supplemental material to cases for abnormal karyotype analysis results of fetuses with FGR.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cai, M., Lin, N., Su, L. et al. Fetal growth restriction: associated genetic etiology and pregnancy outcomes in a tertiary referral center. J Transl Med 20, 168 (2022). https://doi.org/10.1186/s12967-022-03373-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12967-022-03373-z