
Abstract
Background
Interleukin-33 (IL-33) plays a pivotal role in regulating innate immune response and metabolic homeostasis. However, whether its circulating level is correlated with obesity and metabolic disorders in humans remains largely unknown. We aimed to address this gap by determining IL-33 serum level and its downstream type 2 inflammatory cytokines interleukin-5 (IL-5) and interleukin-13 (IL-13) in overweight/obese population, and analyzing the specific associations between IL-33 and obesity metabolic phenotypes.
Methods
217 subjects were enrolled and divided into three groups: healthy control (HC) subjects, metabolically healthy overweight/obese (MHOO) subjects and metabolically unhealthy overweight/obese (MUOO) subjects. Circulating levels of IL-33, IL-5 and IL-13 were measured using ELISA analyses. Multivariate regression analyses were further performed to determine the independent association between IL-33 and obesity metabolic phenotypes.
Results
Circulating levels of IL-33 were significantly elevated in subjects of MUOO group compared with HC group and MHOO group, while no significant difference was observed between the latter two groups in IL-33 levels. Consistent with this, serum levels of IL-5/13 were higher in the MUOO group compared with HC and MHOO groups. After adjusted for all confounders, MUOO phenotype was significantly associated with increased IL-33 serum levels (OR = 1.70; 95% CI 1.09–2.64; p = 0.019). With the MHOO group as the reference population, higher circulating level of IL-33 was also positively associated with MUOO phenotype after adjusting for confounders (OR = 1.50; 95% CI 1.20–1.88; p = 2.91E−4). However, there was no significant association between MHOO phenotype and IL-33 levels (p = 0.942). Trend analysis further confirmed the positive correlation between MUOO phenotype and IL-33 level (p for trend = 0.019). Additionally, IL-33 was significantly and positively correlated with diastolic blood pressure (DBP), total cholesterol (TC), alanine aminotransferase (ALT), aspartate aminotransferase (AST), white blood cell (WBC), neutrophil and IL-5 only in MUOO group, while inversely correlated with high density lipoprotein cholesterol (HDL-C) in MHOO subjects.
Conclusion
Circulating levels of IL-33 were significantly elevated in overweight/obese Chinese adults with metabolic disorders. Increased levels of IL-33 were positively associated with metabolically unhealthy overweight/obese phenotype and several metabolic syndrome risk factors.
Similar content being viewed by others

Introduction
Obesity and its related metabolic complications have become important public health issues globally, contributing to disease burden worldwide [1,2,3,4]. According to the recent research by WHO in 2017, more than two billion of people on the world are overweight and about one-third of them are obese [4]. With the occurrence and development of obesity, inflammatory immune cells infiltrated into adipose tissue and other metabolically active organs, causing inflammation and insulin resistance [5, 6]. Therefore, obesity has been well documented as a low-grade but chronic inflammatory disease [6,7,8], which contributes to the development and progression of its related metabolic complications such as cardiovascular diseases and type 2 diabetes mellitus (T2DM) [2]. However, the precise mechanism underlying obesity-induced inflammation remains incompletely understood.
IL-33, a newly discovered cytokine in the interleukin-1 (IL-1) family, is associated with Th1 and Th2 immune responses, which has been shown to be broadly expressed in various tissues and play a significant role as an ‘alarmin’ of some diseases [9,10,11,12]. Several reports have shown that IL-33 is important for maintaining immune cell homeostasis in adipose tissue [6] as well as the involvement of adipose tissue microenvironment in the obesity-related inflammation and complications [13]. In addition, IL-33 promotes the beiging of white adipocytes and energy expenditure by activating group 2 innate lymphoid cells (ILC2s) in adipose tissue, contracting obesity and its related disorders [14,15,16]. Despite the beneficial effects as an anti-inflammatory factor [9,10,11, 17], the double-edged sword effect of IL-33 in immunity and metabolism has gained growing attention [10, 11, 18]. Meanwhile, studies have also reported that IL-33 may play an undetermined role in obesity and its cardiovascular or diabetic complications since the specific role of IL-33 in the pathogenesis and development of several metabolic diseases seems to be inconsistent [9, 14,15,16,17]. Compared with its decoy receptor soluble ST2, IL-33 appears to be more complex [9, 18] and may have pro-inflammatory or anti-inflammatory effects in different environments [9, 18]. IL-33 expression was shown to be up-regulated by obesity in white adipose tissue, but resident ILC2s were paradoxically decreased in mice and humans [13, 14, 19]. Therefore, it is urgently needed to clarify whether systemic level and tissue level of IL-33 is differentially regulated by obesity.
Obese patients are mostly accompanied by a cluster of metabolic abnormalities such as hyperlipemia, hyperglycemia and hypertension [7], manifesting as metabolic syndrome [20, 21]. During the development of obesity, even at the overweight stage (BMI 25–28 kg/m2), some patients may have significant changes in their metabolic indicators with the disrupted metabolic immune balance [4, 7, 22, 23]. Thus, early intervention in overweight and obese people can effectively slow down the development of T2DM and cardiovascular events [22, 23]. Studies have indicated that two major types of overweight/obesity metabolic phenotypes have significant differences in inflammation levels [7, 24]. Metabolic healthy overweight/obesity (MHOO) phenotype is associated with a lower level of systemic inflammation [25]. However, when obesity progresses into metabolic unhealthy overweight/obesity (MUOO) phenotype, a higher inflammatory state occurs and is associated with T2DM and cardiovascular diseases [20, 26]. Therefore, understanding whether inflammation and metabolic syndrome risk factors contribute to IL-33 production during obesity progression will provide important evidence for further clarification of the interrelationship between obesity, metabolic health and inflammation [7].
Herein, we analyzed serum levels of IL-33 and its downstream Th2 cytokines IL-5/13 in overweight/obese population. We found a significant association between IL-33 circulating levels and MUOO phenotype. In addition, IL-33 was positively correlated with metabolic syndrome risk factors such as dyslipidemia and hypertension rather than obesity itself.
Materials and methods
Subjects
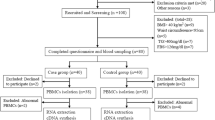
Initially, five hundred participants aged from 18 to 78 years were recruited from physical examination population in Second Xiangya Hospital of Central South University in China from Sep 2018 to Apr 2019. The exclusion criteria included cancer, organic heart disease, autoimmune disease, chronic hepatic or renal disease, hyperthyroidism, Cushing syndrome, hyperparathyroidism, infectious disease, pregnancy, lactation and surgery in the previous month. Additionally, participants who had recently (within 1 month) taken antihypertensive drugs, hypoglycemic drugs and antilipemic drugs had also been excluded. In order to compare the IL-33 serum levels in healthy population and overweight/obese population with or without metabolic abnormalities, a total sample size of 186 individuals was estimated by PASS15 software, since the two-sided test was required, with α of 0.05 and the power of 90%. Taken into account that 15% of patients may be lost during the follow-up, a total of 217 participants were eventually included in this study. Through matching, 144 overweight/obese subjects (BMI ≥ 25.0 kg/m2) were divided into the MHOO group (72 subjects) and MUOO group (72 subjects) according to their metabolic abnormalities, and 73 healthy participants were matched with both the MUOO and MHOO groups for gender and age. The study was conducted according to the guidelines of the Declaration of Helsinki and the study protocol was approved by the ethics committee of the Second Xiangya Hospital of Central South University (Ethics Number: 089/2016). Written informed consents were obtained from all participants.
Definition of terms
Metabolic abnormalities were identified using non-obese ATP III criteria [27] metabolic syndrome components (SBP/DBP > 130/85 mmHg, TG ≥ 1.7 mmol/L, HDL-C < 1.04 mmol/L in men, HDL < 1.29 mmol/L in women, FBG > 5.6 mmol/L) [28]. As for the overweight/obese participants (BMI ≥ 25.0 kg/m2), the presence of ≤ 1 ATP III component of metabolic syndrome were defined as MHOO, while the presence of > 1 components were defined as MUOO [20, 21].
Data collection
BMI was calculated by height and weight (weight divided by height squared, kg/m2). Systolic and diastolic blood pressure (SBP, DBP) were measured using digital sphygmomanometer with a standard protocol. All blood samples were collected in the morning (7–8 a.m.) after a 10–12 h overnight fast. Serum samples (centrifugation: 3000g for 5 min) or whole blood samples were used as required for subsequent tests.
Serum levels of fasting blood glucose (FBG), triglycerides (TG), total cholesterol (TC), high density lipoprotein cholesterol (HDL-C), low density lipoprotein cholesterol (LDL-C), alanine aminotransferase(ALT), aspartate aminotransferase (AST), urea nitrogen (Urea), creatinine (Crea), uric acid (UA), nonesterified fatty acid (NEFA) were all examined by HITACHI7600 automatic analyzer (Hitachi Ltd, Japan). Whole blood level of HbA1c was measured by Tosoh Automated Glycohemoglobin Analyzer HLC-723 G8 (Tosoh Corporation, Japan) and several parameters of blood routine (i.e. white blood cell, neutrophil, eosnophils) were measured by Sysmex XN-20 automated hematology analyzer (Sysmex Corporation, Japan). The relevant information of the methods of above parameters see in Additional file 1: Table S1 and all indexes were measured under standardized conditions in an ISO 15189 accredited medical laboratory [29].
IL-33, IL-5, and IL-13 measurements
Serum samples were obtained and collected into tubes and then stored at − 70 °C until use. Serum levels of IL-33 (CSB-E13000h, CUSABIO, China), IL-5 (CSB-E04636h, CUSABIO, China) and IL-13 (CSB-E04601h, CUSABIO, China) were assessed by specific commercially available enzyme-linked immunosorbent assays (ELISA). The lower limits of detection of IL-33, IL-5 and IL-13 assays were 15.6 pg/mL, 0.78 pg/mL and 62.55 pg/mL, respectively. The intra-assay coefficients of variation of IL-33, IL-5, and IL-13 assays were all 8%, and the inter-assay coefficients of variation of IL-33, IL-5, and IL-13 assays were all 10%. All of the cytokine measurements were performed simultaneously.
Statistical analysis
Mean (SD) were given to describe the continuous variables of normal distribution and median values (and interquartile ranges (IQR)) were given to describe the continuous variables of non-normal distribution. The One-way ANOVA and Kruskal–Wallis rank sum test were used to compared the continuous variables of normal distribution and non-normal distribution among the three groups, respectively, while comparisons of nominal variables were performed using the χ2 test. The effect of gender and group on IL-33 serum level was evaluated by 2-way ANOVA. The relationship between IL-33 and clinic-metabolic parameters were analyzed by the Spearman’s correlation coefficient.
Covariates were screened based on the influence of introducing covariates into the basic model or removing covariates from the complete model, which is depended on whether the regression coefficient of IL-33 was more than 10% or the regression coefficient p value of covariant with respect to obesity phenotype less than 0.1. The indexes that defined the MHOO phenotype and MUOO phenotype in the present study (i.e. TG, SBP, DBP, HDL-C and FBG) were not suitable to be included into the regression model for analysis as covariates. Multivariate logistic regression analyses were performed to determine the independent correlation between IL-33 levels and metabolic phenotypes of obesity. Non-adjusted and adjusted models were used to assess confounders. In all of the models, IL-33 serum levels were treated as both continuous variables scaled to 10 pg/mL increments and categorical variables divided into tertiles. Trend analysis was then performed by modeling the IL-33 tertiles as continuous variables. Stratified analyses and interaction analyses by gender, age (≥ 45 years, < 45 years) and BMI (25–28 kg/m2, ≥ 28 kg/m2) were further conducted.
The software Empower (R) (www.empowerstats.com, X & Y Solutions Inc., Boston MA) and R (http://www.R-project.org) [30] were performed for all statistical analyses. Two-tailed p-values less than 0.05 were considered statistically significant.
Results
Clinical characteristics of the participants
Baseline characteristics of the all participants are represented in Table 1. No difference between healthy and overweight/obese subjects was observed at baseline regarding gender and age. Males made up a larger percentage in each group (65.75% of the HC group, 68.06% of the MHOO group and 66.67% of the MUOO group). With the exception of NEFA and Uric, each index showed a significant difference between three groups. In comparison with the HC subjects, both MHOO and MUOO subjects had higher BMI, SBP and DBP, higher circulating levels of TG, ALT, Crea, UA, WBC and lower HDL-C level. Compared with MHOO group, the levels of all metabolic components, TC, LDL-C, HbA1c, UA, WBC and neutrophil in MUOO group were significantly elevated.
Differences in distribution of IL-33 serum levels in three study groups
Circulating levels of IL-33 were higher in all overweight/obese subjects than those in healthy subjects (p = 2.15E−8, Fig. 1a). Interestingly, serum levels of IL-33 were significantly elevated in MUOO subjects compared with MHOO subjects or HC subjects, whereas IL-33 levels in MHOO population were basically similar to those of healthy control subjects (Table 1). IL-33 levels were also analyzed in the three groups based on gender, and the serum levels were basically the same in males and females for each group (Fig. 1b). However, IL-33 serum levels of both male (p = 3.41E−5) and female (p = 0.002) subjects in MUOO group were higher than those in the other two groups, respectively (p = 2.41E−10 when MUOO vs HC and p = 7.16E−9 when MUOO vs MHOO in male; p = 0.017 when MUOO vs MHOO and p = 0.003 when MUOO vs HC in female).

Differences in the distribution of serum IL-33 levels in each study group. a Box-scatter plot showing differences in IL-33 serum levels in healthy controls (n = 73) and overweight/obese subjects (n = 144) by box-scatter plot; Student’s t test were performed in two groups. b Violin plot showing basal serum IL-33 levels in each study group by sex; 2-way ANOVA analysis were performed to analyze the effect of group and sex on IL-33 level
We also analyzed the serum levels of several other Th2 cytokines. Consistent with the distribution trend of IL-33 concentration, serum levels of IL-5 and IL-13 in MUOO group were also significantly higher than those in the MHOO group (Table 1).
Association of serum IL-33 levels with metabolic phenotypes of obesity
Univariate and multivariate logistic regression analysis were performed on the association between each study group to explore the relationship between IL-33 and obesity metabolic phenotypes. In different multivariable models adjusted for potential confounders (Table 2), MUOO phenotype was significantly associated with higher serum levels of IL-33 when compared with HC participants (OR = 1.70; 95% CI 1.09–2.64; p = 0.019) after adjusted for all relevant confounders (model 5). However, no significant correlation was observed between MHOO phenotype and IL-33 levels. In the analyses adjusted for all relevant confounders, MUOO phenotype was still associated with higher odds of serum IL-33 levels in all overweight/obese participants (OR = 1.50; 95% CI 1.20–1.88; p = 2.91E−4).
Trend analysis also showed that MUOO phenotype rather than MHOO phenotype was positively correlated with IL-33 level (Table 3) and the ORs for MUOO phenotype were significantly higher in the third tertile of IL-33 levels than in the first tertile. Compared with HC participants, the third tertile was associated with a 13.34-fold increase in the odds of MUOO phenotype (OR = 13.34; 95% CI 1.35–132.15; p = 0.027) after adjusting all relevant variables (model 5). However, there was no evidence of increased risk of MHOO phenotype in all tertiles of IL-33 levels. With the MHOO participants as a reference group, the subjects with IL-33 levels in both the second (OR = 4.44; 95% CI 1.23–15.99; p = 0.023) and third tertiles (OR = 13.43; 95% CI 2.86–63.12; p = 0.001) had higher increased risk of having MUOO phenotypes after adjusting for confounders (model 5). Specifically, MHOO subjects with IL-33 levels in second tertiles had higher risk of developing MUOO compared with HC subjects under all models. In addition, multivariate logistic regression analyses were further performed to investigate the strength of the association between the circulating level of IL-33 and the susceptibility to MUOO against both HC and MHOO, and results showed MUOO phenotype was still significantly associated with higher serum levels of IL-33 when compared with both HC and MHOO participants (Additional file 2: Table S2).
Stratified and interaction analyses in overweight/obese subjects
Further stratified analysis and interaction analysis were performed by gender, age and BMI in all overweight/obese subjects (Table 4). A slight gender difference was observed in the association between IL-33 and MUOO phenotype. IL-33 level was positively correlated with MUOO in male subjects (p = 3.31E−4) but the correlation was not significant in female participants (p = 0.090). At different ages or BMIs, IL-33 levels showed positive association with MUOO. However, the interaction analysis showed that none of the above variables (i.e., gender, age and BMI) significantly changed the relationship between the IL-33 and MUOO phenotype (all p for the interaction > 0.05).
Correlation between IL-33 serum levels and clinic-metabolic parameters in overweight/obese subjects
We finally analyzed the correlation between clinic-metabolic parameters and serum levels of IL-33 in in each of the MHOO and MUOO groups separately. Our data showed that IL-33 serum levels were positively correlated with DBP, TC, ALT, AST, WBC, Neutrophil and IL-5 in MUOO subjects only in MUOO group (Fig. 2). In MHOO subjects, IL-33 had no significant association with other clinic-metabolic parameters except for negative correlated with HDL-C (Fig. 2). BMI and other biochemistry index did not significantly correlate with IL-33 in MUOO group or MHOO group.

Relationship between IL-33 and major clinic-metabolic parameters in MHOO and MUOO group. Coefficients (r) and P values were calculated by the Spearman’s correlation model. The correlation level was considered significant when < 0.05
Discussion
Obesity, a disorder that is resulted from energy imbalance, has been considered as a chronic low-grade inflammatory disease [7, 31]. As a newly identified cytokine, IL-33 has drawn much attention in the past decade for its ability to regulate multiple immune responses and involved in the pathogenesis of various diseases [9, 11]. In the present study, our results showed that circulating levels of IL-33 in overweight/obese subjects were significantly higher than those in HC subjects, which was partly in agreement with the findings of IL-33 expression in human adipose tissue was upregulated by severe obesity [13]. Obese population with or without metabolic disorders (presented as MUOO phenotype, MHOO phenotype, respectively) could be significantly different in terms of immune and inflammatory response [7, 24, 25]. Our results confirmed that IL-33 levels were increased in MUOO subjects relative to MHOO subjects. For MHOO population, despite being overweight or obese, the circulating level of IL-33 and its distribution were basically the same as those in the healthy individuals, indicating that circulating level of IL-33 may not be significantly affected in the absence of obvious metabolic abnormalities, even if they are overweight or obese.
Although several previous studies based on obese mice models suggested that IL-33 could reduce adiposity, induce anti-inflammation effects in adipose tissue and improve glucose and lipid metabolism [13,14,15,16, 32], there is no reports on the specific correlation between circulating level of IL-33 and human obesity and its associated metabolic disorders. To this end, we analyzed the correlation between IL-33 and metabolic phenotypes of obesity and the results showed that IL-33 was significantly and positively associated with MUOO phenotype, but not associated with MHOO phenotype. Interestingly, when trend analysis was performed on the association of IL-33 with different obesity phenotypes, we found that MHOO subjects with higher IL-33 levels are more likely to develop MUOO compared to HC populations under all models. One of the possible reasons is that people with MHOO phenotype were already overweight/obese and may be more susceptible to external obesogenic/pro-inflammatory factors. What’s more, the contradiction between our results and those of previous studies indicates that IL-33 might have a more complex relationship with the progression of obesity. Several plausible explanations of the dissimilar findings are as follows.
First of all, the study models or populations are different. Our study was focused on overweight/obese population, which was different from the subjects of previous researches who are mostly severely obese people or mice. Secondly, IL-33 can be secreted by various cells or tissues in an autocrine or endocrine manner [9, 13, 14], while the physiological function or distribution pattern of IL-33 is closely related to its secretion mode and production site [33, 34]. Hence, the pathophysiological properties of IL-33 may depend on its secreting cell and temporal expression [33]. So the correlation between the IL-33 serum level and its tissue expression in different depots may be more complicated. Finally, most previous studies have shown that exogenous IL-33, rather than endogenous IL-33, can regulate glucolipid metabolism and inflammation in obesity [9, 15, 17]. Whether endogenous IL-33 can fully maintain the immune balance of obese adipose tissue is controversial [9, 14] and requires by further research.
In the current study, interaction analysis did not showed that gender, age and BMI significantly affected the association between IL-33 and MUOO phenotype, although the association between IL-33 and MUOO phenotype seems insignificant in the female population after gender stratification. We deduced that in addition to the relatively small number of female population, the menstrual cycle, sex hormone and the use of contraceptives in female population may also influence the association between IL-33 and MUOO phenotype. Further research on the mechanism of IL-33 in the occurrence and progression of obesity in different genders are also worth exploring.
In view of the significant correlation between IL-33 and MUOO phenotype, we further analyzed the relationship between IL-33 and metabolic indicators in each of the MHOO and MUOO groups and found that IL-33 was positively associated with several risk factors for cardiovascular disease only in MUOO participants. No studies have reported the relationship between IL-33 and DBP, and the results of significant positive correlation between IL-33 and TC in the MUOO population were partially consistent with those of Hasan et al. [35]. Although it is not clear why the negative correlation between IL-33 and HDL-C was only observed in MHOO population, we deduced that the influence of elevated IL-33 on the HDL-C of cardiovascular disease may be more significant in the MHOO population, since the HDL-C level in this population was relatively higher than that in MUOO group. Therefore, our results demonstrated that IL-33 is closely related to risk factors of cardiovascular disease (e.g. blood pressure, blood lipid level). In addition to this, our study showed positive associations between IL-33 and several nonspecific inflammatory markers (i.e. ALT, AST, WBC and neutrophil) in MUOO subjects. There has been no research about the relationship between inflammatory markers and IL-33 in overweight/obese population. However, several reports have showed that IL-33 is positively correlated with transaminase activity in patients with chronic liver disease [36] and can promote the initiation and recruitment of neutrophils as a direct chemoattractant for neutrophils in inflammatory microenvironment [37, 38]. Based on the above results, our results did not support a cardio-protective effect of IL-33 in overweight/obese people, even if the correlation between IL-33 and metabolic parameters were not strong. On the contrary, the current study demonstrated that IL-33 was closely related with the metabolic-proinflammatory profile in overweight/obese individuals especially in those with MUOO phenotype.
Previous studies have shown that both Th2 and Th1 cytokines levels could be elevated in obese population as well as metabolic syndrome patients [39,40,41]. Given that IL-33 could regulate metabolic inflammation by engaging ILC2s and activating downstream type 2 immune response [42, 43], we tested circulating levels of Th2 cytokines IL-5/13 and found the distribution trend of IL-5/13 levels in different groups were basically consistent with that of IL-33, indicating that Th2 immune responses were activated during the progression of obesity. Thus, it was not difficult to infer that both pro-inflammatory and anti-inflammatory responses were induced in overweight/obese population with metabolic disorders. A recent study has found that adipose derived IL-33 was upregulated in response to short-term high-fat diet, while promoting Th2 immune response and inducing anti-inflammatory response to maintain tissue homeostasis [6], suggesting that adipose tissue could balance local inflammatory responses through a protective feedback mechanism mediated by IL-33.
Although the biological role of IL-33 on MUOO phenotype was not explored in this study, our data could provide an important hint that increased circulating IL-33 level in overweight/obese people with metabolic disorders might be involved in a protective feedback mechanism of immune imbalance caused by obesity and its related metabolic disorders. In any case, our results suggested that the notion that IL-33 was always beneficial in the metabolic diseases was naïve and provide a validation for an association between IL-33 serum level and obesity metabolic phenotypes in Chinese population.
Several limitations are worth consideration when interpreting our findings. First, the criteria for MHOO are not uniform worldwide [21]; thus, part of the results in our study may be affected to some extent by the difference in MHOO definition. Second, information about the daily alcohol intake, dietary intake, work environment, data on the body fat distribution of the participants, sex hormone levels and menstrual cycle of the female population was not effectively collected, which may have influenced the results of this study to some extent. Third, this research has yet to test insulin level and Th1 cytokine levels of the participants, so it was not possible to assess the presence of insulin resistance, which is a major cause of obesity and its related metabolic diseases. Fourth, the IL-33 expression in adipose tissues of the participants was unable to detect in this study; Future research on the role of IL-33 in metabolic diseases from the perspectives of comparing tissue levels and circulatory levels will help to further reveal its action on metabolic disease. Additionally, since the temporal relationship between serum level of IL-33 and the occurrence of metabolic disorders in overweight/obese population was not known, we cannot conclude that IL-33 directly causes metabolic disorders in overweight/obese patients. Prospective longitudinal studies are needed to investigate the causal relationship of IL-33 level and development of obesity.
Conclusions
Circulating levels of IL-33 in overweight/obese people with various metabolic phenotypes were different and was significantly elevated only in MUOO population; IL-33 levels were positively correlated with MUOO phenotype and metabolic syndrome risk factors in overweight/obese Chinese adults.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- HC:
-
Healthy control
- MHOO:
-
Metabolically healthy overweight/obese
- MUOO:
-
Metabolically unhealthy overweight/obese
- BMI:
-
Body mass index
- T2DM:
-
Type 2 diabetes mellitus
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- FBG:
-
Fasting blood glucose
- TG:
-
Triglycerides
- TC:
-
Total cholesterol
- HDL-C:
-
High-density lipoprotein-cholesterol
- LDL-C:
-
Low-density lipoprotein-cholesterol
- NEFA:
-
Non-esterified fatty acids
- ALT:
-
Alanine transaminase
- AST:
-
Aspartate transaminase
- Urea:
-
Blood urea nitrogen
- Crea:
-
Creatinine
- UA:
-
Uric acid
- WBC:
-
White blood cell
- IQR:
-
Interquartile range
- OR:
-
Odd ratio
- CI:
-
Confidence interval
References
Stefan N, Häring HU, Schulze MB. Metabolically healthy obesity: the low-hanging fruit in obesity treatment? Lancet Diabetes Endocrinol. 2018;6(3):249–58.
Duffen J, Zhang M, Masek-Hammerman K, Nunez A, Brennan A, Jones JEC, Morin J, Nocka K, Kasaian M. Modulation of the IL-33/IL-13 axis in obesity by IL-13Rα2. J Immunol. 2018;200(4):1347–59.
Bray GA, Frühbeck G, Ryan DH, Wilding JP. Management of obesity. Lancet. 2016;387(10031):1947–56.
Vasileva LV, Savova MS, Amirova KM, Dinkova-Kostova AT, Georgiev MI. Obesity and NRF2-mediated cytoprotection: where is the missing link?[J]. Pharmacol Res. 2020;156:104760.
Hotamisligil GS. Inflammation, metaflammation and immunometabolic disorders. Nature. 2017;542(7640):177–85.
Mahlakõiv T, Flamar A-L, Johnston LK, Moriyama S, Putzel GG, Bryce PJ, Artis D. Stromal cells maintain immune cell homeostasis in adipose tissue via production of interleukin-33. Sci Immunol. 2019;4(35):eaax0416.
Phillips CM, Perry IJ. Does inflammation determine metabolic health status in obese and nonobese adults? J Clin Endocrinol Metab. 2013;98(10):E1610–9.
Cottam DR, Mattar SG, Barinas-Mitchell E, Eid G, Kuller L, Kelley DE, Schauer PR. The chronic inflammatory hypothesis for the morbidity associated with morbid obesity: implications and effects of weight loss. Obes Surg. 2004;14(5):589–600.
de Oliveira MFA, Talvani A, Rocha-Vieira E. IL-33 in obesity: where do we go from here? Inflamm Res. 2019;68(3):185–94.
Li W, Li Y, Jin J. The essential function of IL-33 in metabolic regulation. Acta Biochim Biophys Sin. 2020;52:gmaa045 (published online ahead of print, 2020 May 22).
Tu L, Yang L. IL-33 at the Crossroads of Metabolic Disorders and Immunity. Front Endocrinol (Lausanne). 2019;10:26.
Schmitz J, Owyang A, Oldham E, Song Y, Murphy E, McClanahan TK, Zurawski G, Moshrefi M, Qin J, Li X, Gorman DM, Bazan JF, Kastelein RA. IL-33, an interleukin-1-like cytokine that signals via the IL-1 receptor-related protein ST2 and induces T helper type 2-associated cytokines. Immunity. 2005;23(5):479–90.
Zeyda M, Wernly B, Demyanets S, Kaun C, Hämmerle M, Hantusch B, Schranz M, Neuhofer A, Itariu BK, Keck M, Prager G, Wojta J, Stulnig TM. Severe obesity increases adipose tissue expression of interleukin-33 and its receptor ST2, both predominantly detectable in endothelial cells of human adipose tissue. Int J Obes (Lond). 2013;37(5):658–65.
Brestoff JR, Kim BS, Saenz SA, Stine RR, Monticelli LA, Sonnenberg GF, Thome JJ, Farber DL, Lutfy K, Seale P, Artis D. Group 2 innate lymphoid cells promote beiging of white adipose tissue and limit obesity. Nature. 2015;519(7542):242–6.
Lee MW, Odegaard JI, Mukundan L, Qiu Y, Molofsky AB, Nussbaum JC, Yun K, Locksley RM, Chawla A. Activated type 2 innate lymphoid cells regulate beige fat biogenesis. Cell. 2015;160(1–2):74–87.
Ding X, Luo Y, Zhang X, Zheng H, Yang X, Yang X, Liu M. IL-33-driven ILC2/eosinophil axis in fat is induced by sympathetic tone and suppressed by obesity. J Endocrinol. 2016;231(1):35–48.
Miller AM, Asquith DL, Hueber AJ, Anderson LA, Holmes WM, McKenzie AN, Xu D, Sattar N, McInnes IB, Liew FY. Interleukin-33 induces protective effects in adipose tissue inflammation during obesity in mice. Circ Res. 2010;107(5):650–8.
Aimo A, Migliorini P, Vergaro G, Franzini M, Passino C, Maisel A, Emdin M. The IL-33/ST2 pathway, inflammation and atherosclerosis: trigger and target? Int J Cardiol. 2018;267:188–92.
Zhao X Y, Zhou L, Chen Z, Ji Y, Peng X, Qi L, Li S, Lin JD. The obesity-induced adipokine sST2 exacerbates adipose T reg and ILC2 depletion and promotes insulin resistance. Science Advances. 2020; 6(20): eaay6191.
Magkos F. Metabolically healthy obesity: what’s in a name? Am J Clin Nutr. 2019;110(3):533–9.
Roberson LL, Aneni EC, Maziak W, Agatston A, Feldman T, Rouseff M, Tran T, Blaha MJ, Santos RD, Sposito A, Al-Mallah MH, Blankstein R, Budoff MJ, Nasir K. Beyond BMI: the “Metabolically healthy obese” phenotype & its association with clinical/subclinical cardiovascular disease and all-cause mortality–a systematic review. BMC Public Health. 2014;14:14.
Nam GE, Park HS. Perspective on diagnostic criteria for obesity and abdominal obesity in Korean adults. J Obes Metab Syndr. 2018;27:134–42.
Aune D, Sen A, Prasad M, Norat T, Janszky I, Tonstad S, Romundstad P, Vatten LJ. BMI and allcause mortality: systematic review and non-linear dose-response meta-analysis of 230 cohort studies with 3.74 million deaths among. million participants. BMJ. 2016;353:i2156.
Gonçalves CG, Glade MJ, Meguid MM. Metabolically healthy obese individuals: key protective factors. Nutrition. 2016;32(1):14–20.
Karelis AD, Faraj M, Bastard JP, St-Pierre DH, Brochu M, Prud’homme D, Rabasa-Lhoret R. The metabolically healthy but obese individual presents a favorable inflammation profile. J Clin Endocrinol Metab. 2005;90(7):4145–50.
Stefan N, Schick F, Häring HU. Causes, Characteristics, and Consequences of Metabolically Unhealthy Normal Weight in Humans. Cell Metab. 2017;26(2):292–300.
Teixeira TF, Alves RD, Moreira AP, Peluzio Mdo C. Main characteristics of metabolically obese normal weight and metabolically healthy obese phenotypes. Nutr Rev. 2015;73(3):175–90.
Camhi SM, Katzmarzyk PT. Differences in body composition between metabolically healthy obese and metabolically abnormal obese adults. Int J Obes (Lond). 2014;38(8):1142–5.
Tang HN, Tang CY, Man XF, Tan SW, Guo Y, Tang J, Zhou CL, Zhou HD. Plasticity of adipose tissue in response to fasting and refeeding in male mice. Nutr Metab (Lond). 2017;14:3.
Tang HN, Xiao F, Chen YR, Zhuang SQ, Guo Y, Wu HX, Zhou HD, Jiang H. Higher serum neuropeptide Y levels are associated with metabolically unhealthy obesity in obese Chinese adults: a cross-sectional study. Mediat Inflamm. 2020;2020:7903140. https://doi.org/10.1155/2020/7903140.
Tang HN, Man XF, Liu YQ, Guo Y, Tang AG, Liao EY, Zhou HD. Dose-dependent effects of neuropeptide Y on the regulation of preadipocyte proliferation and adipocyte lipid synthesis via the PPARγ pathways. Endocr J. 2015;62(9):835–46.
Demyanets S, Kaun C, Kaider A, Speidl W, Prager M, Oravec S, Hohensinner P, Wojta J, Rega-Kaun G. The pro-inflammatory marker soluble suppression of tumorigenicity-2 (ST2) is reduced especially in diabetic morbidly obese patients undergoing bariatric surgery [J]. Cardiovasc Diabetol. 2020;19(1):26–34.
Altara R, Ghali R, Mallat Z, Cataliotti A, Booz GW, Zouein FA. Conflicting vascular and metabolic impact of the IL-33/sST2 axis. Cardiovasc Res. 2018;114(12):1578–94.
Huang HT, Tsai SF, Wu HT, Huang HY, Hsieh HH, Kuo YM, Chen PS, Yang CS, Tzeng SF. Chronic exposure to high fat diet triggers myelin disruption and interleukin-33 upregulation in hypothalamus. BMC Neurosci. 2019;20(1):33.
Hasan A, Al-Ghimlas F, Warsame S, Al-Hubail A, Ahmad R, Bennakhi A, Al-Arouj M, Behbehani K, Dehbi M, Dermime S. IL-33 is negatively associated with the BMI and confers a protective lipid/metabolic profile in non-diabetic but not diabetic subjects. BMC Immunol. 2014;15:19.
Wang J, Zhao P, Guo H, Sun X, Jiang Z, Xu L, Feng J, Niu J, Jiang Y, Fantuzzi G. Serum IL-33 levels are associated with liver damage in patients with chronic hepatitis C. Mediat Inflamm. 2012;2012:819636.
Le HT, Tran VG, Kim W, Kim J, Cho HR, Kwon B. IL-33 priming regulates multiple steps of the neutrophil-mediated anti-Candida albicans response by modulating TLR and dectin-1 signals. J Immunol. 2012;189(1):287–95.
Verri WA Jr, Souto FO, Vieira SM, Almeida SCL, Fukada SY, Xu D, Alves-Filho JC, Cunha TM, Guerrero ATG, Mattos-Guimaraes RB, Oliveira FR, Teixeira MM, Silva JS, McInnes IB, Ferreira SH, Louzada-Junior P, Liew FY, Cunha FQ. IL-33 induces neutrophil migration in rheumatoid arthritis and is a target of anti-TNF therapy. Ann Rheum Dis. 2010;69(9):1697–703.
Martínez-Reyes CP, Gómez-Arauz AY, Torres-Castro I, Manjarrez-Reyna AN, Palomera LF, Olivos-García A, Mendoza-Tenorio E, Sánchez-Medina GA, Islas-Andrade S, Melendez-Mier G, Escobedo G, Portha B. Serum levels of interleukin-13 increase in subjects with insulin resistance but do not correlate with markers of low-grade systemic inflammation. J Diabetes Res. 2018;2018:7209872.
Lucas R, Parikh SJ, Sridhar S, Guo DH, Bhagatwala J, Dong Y, Caldwell R, Mellor A, Caldwell W, Zhu H, Dong Y. Cytokine profiling of young overweight and obese female African American adults with prediabetes. Cytokine. 2013;64(1):310–5.
Surendar J, Mohan V, Rao MM, Babu S, Aravindhan V. Increased levels of both Th1 and Th2 cytokines in subjects with metabolic syndrome (CURES-103). Diabetes Technol Ther. 2011;13(4):477–82.
Engelbertsen D, Lichtman AH. Innate lymphoid cells in atherosclerosis. Eur J Pharmacol. 2017;816:32–6.
Newland SA, Mohanta S, Clément M, Taleb S, Walker JA, Nus M, Sage AP, Yin C, Hu D, Kitt LL, Finigan AJ, Rodewald HR, Binder CJ, McKenzie ANJ, Habenicht AJ, Mallat Z. Type-2 innate lymphoid cells control the development of atherosclerosis in mice. Nat Commun. 2017;8:15781.
Acknowledgements
Not applicable.
Funding
This work was supported by the National Natural Scientific Foundation of China [Grant number 81600666] and the Fundamental Research Funds for the Central Universities of Central South University [2020zzts875].
Author information
Authors and Affiliations
Contributions
LT and HT designed the study; HT, NL, YY, XF, YF, SZ and YD conducted the research; HT, NL, ML and LT analyzed the data; HT, NL and YY wrote the manuscript; ML and LT revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All participants gave their written informed consents. The study was conducted in accordance with the Declaration of Helsinki and the protocol was approved by the ethics committee of the Second Xiangya Hospital of Central South University (Ethics Number: 089/2016).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1:
Table S1. Methods for the determination of the studied biochemical parameters.
Additional file 2:
Table S2. Multivariate analysis of the association between IL-33 levels and susceptibility to MUOO against both HC and MHOO.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tang, H., Liu, N., Feng, X. et al. Circulating levels of IL-33 are elevated by obesity and positively correlated with metabolic disorders in Chinese adults. J Transl Med 19, 52 (2021). https://doi.org/10.1186/s12967-021-02711-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12967-021-02711-x