
Abstract
Background
Obesity is associated with an increased risk of insulin resistance and type 2 diabetes mellitus (T2DM). However, some obese individuals maintain their insulin sensitivity and exhibit a lower risk of associated comorbidities. The underlying metabolic pathways differentiating obese insulin sensitive (OIS) and obese insulin resistant (OIR) individuals remain unclear.
Methods
In this study, 107 subjects underwent untargeted metabolomics of serum samples using the Metabolon platform. Thirty-two subjects were lean controls whilst 75 subjects were obese including 20 OIS, 41 OIR, and 14 T2DM individuals.
Results
Our results showed that phospholipid metabolites including choline, glycerophosphoethanolamine and glycerophosphorylcholine were significantly altered from OIS when compared with OIR and T2DM individuals. Furthermore, our data confirmed changes in metabolic markers of liver disease, vascular disease and T2DM, such as 3-hydroxymyristate, dimethylarginine and 1,5-anhydroglucitol, respectively.
Conclusion
This pilot data has identified phospholipid metabolites as potential novel biomarkers of obesity-associated insulin sensitivity and confirmed the association of known metabolites with increased risk of obesity-associated insulin resistance, with possible diagnostic and therapeutic applications. Further studies are warranted to confirm these associations in prospective cohorts and to investigate their functionality.
Similar content being viewed by others
Background
Obesity has become a global health care problem due to associated comorbidities including type 2 diabetes mellitus (T2DM), coronary artery disease (CAD), non-alcoholic fatty liver disease (NAFLD) and cancer [1,2,3,4]. However, a subset of obese individuals exhibit fewer comorbidities than their equally obese counterparts including maintaining their insulin sensitivity as well as having a healthier lipid profile [5]. The underlying protective mechanisms of the metabolically healthy obesity, also known as insulin sensitive obesity, remain unknown.
Previous studies have suggested that lower levels of inflammatory mediators play a role in the protective phenotype of obese insulin sensitive (OIS) individuals compared to their pathologically obese counterparts, also known as obese insulin resistant (OIR) individuals [6,7,8]. Other reports have suggested that OIS individuals show fewer markers of oxidative stress [8, 9]. These two mediators (inflammation and oxidative stress) could potentially be influenced by various genetic and environmental factors [10]. Although evidence of the genetic component remains limited, the environmental effect of certain pollutants and various medications has been previously established [11, 12].
Advancement in metabolomic tools including mass spectrometry (MS) technologies has allowed the identification of novel metabolic mediators of disease progression, including obesity associated insulin resistance and T2DM [13]. Recent evidence showed that adipose tissue from OIS, OIR and T2DM individuals exhibit a unique lipidomic signature associated with an increased risk of obesity-associated insulin resistance [14, 15]. Furthermore, metabolomics studies in individuals with T2DM have revealed several diabetes-associated metabolites, including 1,5-anhydroglucitol (1,5-AG), mannose and glucose [16, 17]. Additionally, lipidomics analysis of plasma samples from young adults has revealed that waist circumference was associated with levels of several sphingomyelins, diacylphosphatidylcholines and lysophosphatidylcholines, whereas HOMA-IR was associated with specific diacylphosphatidylcholines, lysophosphatidylcholines and diacylphosphatidylcholines [18]. However, no metabolomics studies have compared the metabolic differences in blood between lean healthy controls, OIS, OIR and T2DM. Such an approach can provide a deeper understanding of the underlying protective mechanisms in those lower risk individuals, and help in the design of novel diagnostic and therapeutic strategies targeting those at higher risk of disease [19, 20].
The aim of this study was to employ untargeted metabolomics analysis of blood samples from lean, OIS, OIR and obese-T2DM individuals in order to investigate the metabolic pathways underlying obesity-associated insulin resistance and T2DM.
Methods
Materials
Interleukin 6 (IL-6) and leptin ELISAs were from R&D systems (Abingdon, UK). Insulin ELISA was from Mercodia Diagnostics (Uppsala, Sweden). Other chemicals and reagents were from Sigma (Munich, Germany).
Study design
One hundred and seven individuals (75 obese and 32 lean) were recruited at Al Emadi hospital and Hamad Medical Corporation. Lean participants were healthy females visiting the clinic for acne concerns. Obese participants were amongst patients undergoing weight reduction surgery. Subject inclusion criteria included males and females aged over 18 years and under 65 years of age. Subject exclusion criteria included malignancy or other terminal illness, poorly compliant patients, from whatever cause, inability to give informed consent, or involvement in other research projects. All individuals gave their written informed consent. Protocols were approved by Institutional Review Boards of the Anti-Doping Laboratory Qatar (X2017000224) and Weill Cornell Medicine-Qatar (15-00007). Measurements of body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP) and mean arterial blood pressure (MAP) were recorded. Fasting blood samples were obtained from all participants. Plasma cholesterol (total, HDL, LDL and triacylglycerol), fasting blood glucose (FBG) and liver function enzymes (total protein, ALP, AST, ALT and bilirubin) were measured by COBAS INTEGRA (Roche Diagnostics, Basil). IL-6, leptin and insulin were determined using commercially available ELISA. Insulin resistance was computed by homeostatic model assessment (HOMA-IR, https://www.dtu.ox.ac.uk/homacalculator/) [21] using 30th percentile (HOMA-IR = 2.4) as a threshold point. Accordingly, obese subjects (BMI > 30) were dichotomized into IS (HOMA-IR < 2.4, n = 20, 6 males and 14 females), IR (HOMA-IR > 2.4, n = 41, 15 males and 26 females) and 14 clinically diagnosed T2DM patients (9 males and 5 females) according to the definition of the American Diabetes Association (ADA) “Standards of Medical Care in Diabetes” [22].
Metabolomics
Metabolomics profiling was performed using established protocols at Metabolon, Durham, NC, USA. All methods employed a Waters ACQUITY ultra-performance liquid chromatography (UPLC) and a Thermo Scientific Q-Exactive high resolution/accurate mass spectrometer interfaced with a heated electrospray ionization (HESI-II) source and Orbitrap mass analyzer operated at 35,000 mass resolution. The detailed description of the liquid chromatography-mass spectrometry (LC–MS) methodology was previously described [23, 24]. Briefly, serum samples from the 107 participants were methanol extracted to remove the protein fraction. The resulting extract was divided into five fractions: two for analysis by two separate reverse phase (RP)/UPLC-MS/MS methods with positive ion mode electrospray ionization (ESI), one for analysis by RP/UPLC-MS/MS with negative ion mode ESI, one for analysis by hydrophilic interaction chromatography (HILIC)/UPLC-MS/MS with negative ion mode ESI, and one sample was reserved for backup. Raw data was extracted, peak-identified, and quality control-processed using Metabolon’s hardware and software [25]. Compounds were identified by comparison to library entries of purified standards or recurrent unknown entities with more than 3300 commercially available purified standard compounds. Library matches for each compound were checked for each sample and corrected if necessary [26].
Statistical analysis of metabolomics data
Statistical analyses were carried out using IBM SPSS version 25, R version 3.2.1 and SIMCA 13.0.1 software (Umetrics, Sweden). Variables with skewed distributions were log transformed or taken the square root of as appropriate to ensure normality [27]. Comparisons were performed with t-test, Wilcoxon–Mann–Whitney and 1-way ANOVA as appropriate. Significance was defined as p ≤ 0.05. Non-parametric tests were used for comparing ordinal or non-normal variables. Metabolomics data were log-transformed to ensure normality. Batch correction was performed by Metabolon by rescaling each metabolite’s median to 1. Principle component analysis (PCA) was performed using version 2.14, http://www.r-project.org/. PCA revealed two main components (PC1 and PC2) that together captured 27% of the variance in the data. Linear regression was performed to identify significant metabolites differentiating study groups (OIS vs OIR and T2DM) and (lean = 0, OIS = 1, OIR = 2, T2DM = 3, denoting disease progression) using the R statistical package (version 2.14, http://www.r-project.org/) after correcting for age, gender, BMI and principle components (PC1 and PC2). PCs represent common signals by the metabolites that contribute to the overall variance in the data and uncover fingerprints of confounders allowing their incorporation into the model by assigning them quantifiable measures. In the first model, the variable study group is categorical whereas the variable disease progression in the second group is continuous. Pathway enrichment analyses were carried out using Chi square tests to identify pathways with metabolites enriched at the top of the list of metabolites ranked by p-value from the linear model since Bonferroni level of significance was not observed. Orthogonal partial least square discriminant analysis (OPLS-DA) was used to compare lean, OIS, OIR and T2DM groups using SIMCA 14 with percentage of missing metabolite values across the samples of 50%. A partial correlation analysis was used to determine metabolic traits of disease (age, BMI, blood pressure, lipids, glucose/insulin/HOMA-IR and liver function enzymes) that exhibit best association with metabolites showing significantly differing levels between disease groups using IBM SPSS version 25, R version 3.2.1.
Results
General characteristics of participants
Thirty-two lean (BMI = 22.7 ± 2.5 kg/m2, all females) and seventy-five obese and morbidly obese (BMI = 45 ± 6.7 kg/m2, 45 females and 30 males) individuals were recruited at Hamad Medical Corporation and Al Emadi hospital, respectively. Lean individuals were younger and had significantly lower levels of SBP, MAP, triglycerides, triglycerides/HDL ratio, FBG, ALP, ALT and AST than obese individuals. Among obese participants, OIR individuals showed higher FBG than expected, suggesting a high prevalence of undiagnosed T2DM within this group. Therefore, subsequent analyses considered OIR and T2DM groups as one group (all IR) as both groups share obesity and insulin resistance. OIS subjects showed significantly lower MAP and levels of triacylglycerols, FBG, insulin and HOMA-IR than their equally obese all IR (OIR + T2DM) counterparts (Table 1).
Metabolites differentiating OIS from OIR + T2DM
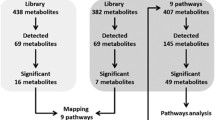
Non-targeted metabolomics of serum samples from the 107 participants was applied to identify metabolites that differentiate OIS vs OIR and OIS vs OIR + T2DM individuals to reveal a metabolic signature of obesity-associated insulin resistance and T2DM. Initial analysis revealed no significant differences in levels of metabolites between OIS and OIR due to their small group sizes (data not shown); however, when combining OIR + T2DM, the linear model revealed 27 metabolites exhibiting significant differences between OIS and OIR + T2DM groups (Table 2). These included metabolites associated with glycolysis, gluconeogenesis and pyruvate metabolism (glucose and 1,5 AG), histidine metabolism (1-methylhistamine, 1-ribosyl-imidazoleacetate and formiminoglutamate) and phospholipid metabolism (choline, glycerophosphoethanolamine and glycerophosphorylcholine). Since the Bonferroni level of significance was not achieved for any of the identified associations, pathway enrichment analysis was performed based on identifying pathways reported by nominally significant metabolites more frequently than can be attributed to random chance. Among the significantly altered metabolic pathways, the phospholipids metabolic pathway was significantly over-represented based on enrichment analysis of the nominally significant metabolites from the group comparisons (p = 3.9E−7). The corresponding metabolites associated with the phospholipids metabolic pathway differentiating OIS from OIR + T2DM included choline, glycerophosphoethanolamine and glycerophosphorylcholine (GPC) (highlighted in Table 2). Figure 1 illustrates levels of significant metabolites that belong to enriched pathways in different study groups. Figure 1 demonstrates higher levels of choline, glycophosphoethanolamine and GPC in OIS compared OIR + T2DM and lean groups. Levels of these metabolites in individual groups are also shown in Additional file 1: Fig. S1.

Boxplot of metabolites that belong to the enriched phospholipid pathway differentiating OIS and OIR + T2DM groups. Linear regression was performed to identify significant metabolites differentiating OIS from OIR and T2DM using the R statistical package after correcting for age, gender, BMI and principle components (PC1 and PC2). Y-axis indicates levels of metabolites (log2). *p-value significance level of 0.05 was used
Metabolites associated with disease progression
An additional a linear model was used to assess the significance of metabolites associated with increased risk of obesity-associated insulin resistance and T2DM (as defined in the method section). Sixty-six metabolites exhibited significant differences with disease progression. The list of metabolites and their associated pathways are shown in Additional file 2: Table S1. These included metabolites associated with glycolysis (glucose), mannose metabolism (mannose), monohydroxy fatty acid (3-hydroxylaurate, 3-hydroxyoctanoate, 3-hydroxydecanoate and 3-hydroxymyristate), medium chain fatty acids (laurate) and urea cycle; arginine and proline metabolism (ADMA + SDMA) among others. Enriched metabolic pathways included glycolysis, gluconeogenesis and the pyruvate metabolic pathway (p = 0.02), fatty acid monohydroxy metabolic pathway, urea cycle metabolic pathway (p = 0.04) and arginine and proline metabolic pathway (p = 0.05). Subsequently, metabolites that showed significant differences with disease progression (Additional file 2: Table S1) within these enriched pathways were identified (Table 3). Figure 2 demonstrates patterns of increased (3-hydroxylaurate, 3-hydrocyoctanoate, 3-hydroxydecanoate, 3-hydroxymyristate, and glucose) or decreased (1,5-AG, ADMA + SDMA, homoarginine, ornithine, 2-oxoarginine) metabolites with disease progression.

Boxplot of metabolites that belong to the enriched pathways associated with increased risk of obesity-associated insulin resistance and T2DM. Linear regression was performed to identify significant metabolites associated with disease progression using the R statistical package after correcting for age, gender, BMI and principle components (PC1 and PC2). Y-axis indicates levels of metabolites (log2). A p-value significance level of 0.05 was used
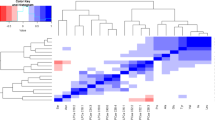
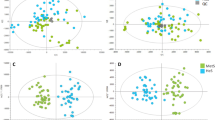
An orthogonal partial least square discriminate analysis (OPLS-DA) comparing subjects from lean, OIS, OIR and T2DM was used for ease of visualization. The model revealed three class-discriminatory components accounting for 48% of the variation in the data due to participant groups (Fig. 3). The score plot in Fig. 3a indicates an x-axis separating the lean group from OIS, OIR and T2DM; the latter group being rather separated along the y-axis. The corresponding loading plot, shown in Fig. 3b, indicates enriched pathways’ associated metabolites significantly differentiating OIS and OIR + T2DM and those associated with disease progression as per linear models. Specifically, higher glucose, choline, GPC, 3-hydroxymyristate and 3-hydroxylaurate and lower 1,5-AG, dimethylarginine (ADMA + SDMA), homoarginine, ornithine and 2-oxoarginine are indicated.

OPLS-DA model comparing metabolites from lean, OIS, OIR and T2DM individuals. a A score plot showing the class-discriminatory component 1 (x-axis) versus class-discriminatory component 2 (y-axis). b The corresponding loading plot showing enriched pathways’ associated metabolites differentiating OIS and OIR + T2DM groups or those associated with disease progression
Correlation of significant metabolites with mediators of metabolic disease
A partial correlation analysis was used to determine traits of disease best associated with metabolites showing significantly differing levels between disease groups. In essence, the correlation between each of such metabolites and each trait was evaluated after correcting for the effect of all other remaining traits. The correlations that remained significant after such correction are listed in Table 4. The trait of liver function enzymes (ALP and ALT), BMI, TAGs, leptin, insulin and HOMA-IR showed the most significant correlations with levels of metabolites differentiating OIS and OIR + T2DM and those associated with disease progression.
Discussion
Obesity triggers a cascade of biochemical changes that increase the risk of various comorbidities including insulin resistance and T2DM. However, some obese individuals seem to be protected against obesity-associated comorbidities. Understanding the underlying mechanisms of this apparently protective phenotype could provide a therapeutic strategy to mitigate the comorbidities associated with pathological obesity. Various studies have investigated the potential mechanisms underlying differences among lean, obese-IS, obese-IR and obese-T2DM individuals [7, 9, 11, 14, 28, 29], however no study has compared the differences in the metabolic signature among these groups as a means to identify potential diagnostic and therapeutic targets. In this study, untargeted metabolomics analysis of serum samples from lean, OIS, OIR and obese-T2DM individuals was utilized to investigate the metabolic pathways underlying progression of insulin resistance and T2DM. Our novel data indicate that the phospholipid metabolites (choline, glycerophosphoethanolamine and glycerophosphorylcholine) were significantly altered when comparing OIS and OIR + T2DM. Additionally, our data confirmed metabolic changes in several metabolic pathways with obesity-associated insulin resistance and T2DM, including fatty acid and arginine metabolism as well as metabolic markers of liver disease, vascular disease, and diabetes. Therefore, the novel metabolites reported here differentiate the metabolically healthy obese group (OIS) from the pathological obese group (OIR + T2DM) and confirm known biomarkers of obesity-associated insulin resistance with potential diagnostic and therapeutic applications. The causative nature of the identified correlations between metabolites and insulin resistance cannot be ruled out particularly as it is recognized that free fatty acids, for instance, increase insulin resistance [30]. Therefore, future in vitro and in vivo functional studies are warranted where the effects of these metabolites on inducing insulin resistance could confirm their functional relevance.
A novel metabolic signature differentiating OIS and OIR + T2DM
Since there were no difference between OIS and OIR likely due to their small group sizes, the analysis was repeated by comparing OIS and combined OIR and T2DM groups as the latter two groups were matched for obesity and insulin resistance. Three phospholipids were found to differentiate between OIS and OIR + T2DM. These included increased levels of choline and GPC in OIS compared to OIR + T2DM and lean groups, suggesting a protective role in obesity-associated insulin resistance. GPC is a natural precursor of phospholipids and a metabolite derived from phosphatidylcholine. It contributes the most to circulating choline levels; therefore, GPC serves as a precursor for acetylcholine. The latter is an important neurotransmitter and a vasodilator that shows a different microvascular reactivity between IR and IS nondiabetic women [31]. Previous studies have reported that dietary choline levels can also lower the risk of fatty liver disease and liver damage [32]. Glycerophosphoethanolamine was another metabolite that differentiated OIS from OIR + T2DM. Glycerophosphoethanolamine represents a membrane degradation product that has been linked to chronic liver disease [33]. The novel associations between higher levels of these phospholipid metabolites and obesity-associated insulin sensitivity could therefore reflect decreased risk of microvascular disease, small vessel disease, lipotoxic cardiac diseases and non-alcoholic liver disease in the OIS group compared to OIR + T2DM group of participants [34,35,36].
Metabolic signature of obesity-associated insulin resistance and T2DM
When comparing the metabolic profiles of lean, obese-IS, IR and T2DM individuals, several metabolites significantly changed with disease progression. These included metabolites that were previously reported in association with insulin resistance and T2DM such as glucose and 1,5-AG [37, 38]. Other identified metabolites were reported in association with comorbidities of insulin resistance and T2DM including fatty acid metabolic disorders (such as 3-hydroxylaurate) [39], impairment of liver function and diabetic status (such as 3-hydroxymyristate and homoarginine) [40, 41] and vascular disease (such as dimethylarginine) [42]. Other novel arginine metabolites were also found to be significantly changed with disease progression including ornithine (a precursor of arginine, also a medication for hepatic encephalopathy) [43] and 2-oxoarginine (a metabolite of arginine catabolism and a marker of argininemia) [44]. Novel metabolites in association with disease progression were also identified including medium chain fatty acids 3-hydroxyoctanoate and 3-hydroxydecanoate that have been reported to be involved in beta-oxidation of longer-chain fatty acids [45, 46]. Previous reports have associated increased plasma levels of 3-hydroxyoctanoate in patients with an inherited deficiency of long-chain 3-hydroxyacyl-CoA dehydrogenase, as a marker of various clinical cases such as recurrent myoglobinuria, hypoketotic hypoglycemic encephalopathy, hypertrophic/dilatative cardiomyopathy, sudden infant death, and fulminant hepatic failure [46, 47].
Correlation between metabolites differentiating OIS and OIR + T2DM and classical mediators of metabolic disease
When considering correlations between the identified metabolites and classical mediators of metabolic disease such as age, BMI, lipids, FBG, insulin, HOMA-IR and liver function enzymes, a partial correlation analysis revealed several significant associations. Choline, previously shown to be lower in hepatic damage [48], was found to positively correlate with leptin and ALT. Despite its positive correlation with ALT, choline was found to be higher in OIS compared to OIR + T2DM, indicating a relationship between this metabolite and the protective phenotype of OIS individuals that requires further investigation. On the other hand, glycerophosphoethanolamine was found to be associated with BMI, suggesting increased levels of this membrane degradation product with obesity.
Correlation of disease progression metabolites and classical mediators of metabolic disease
As expected, glucose and 1,5-AG, previously shown to be associated with T2DM, were found to correlate significantly with levels of insulin and circulating triacylglycerol levels. When considering metabolites that were significantly associated with obesity-related comorbidities, a significant correlation between levels of 3-hydroxylaurate and ALP, was revealed. This suggests that 3-hydroxylaurate, a medium chain fatty acid that is associated with intolerance to prolonged fasting and recurrent episodes of hypoglycemic coma, may constitute a novel marker of fatty liver disease. Similarly, 3-hydroxyocanoate was also found to be associated with ALP and BMI, suggesting that it may also be a novel marker of obesity-associated fatty liver disease. 3-hydroxydecanoate was also found to be associated with BMI, suggesting increased levels of another medium-chain fatty acid with a role in the beta-oxidation and obesity. Ornithine, previously shown to be associated with hepatic damage, was found to be associated with leptin and ALT, providing a further evidence of its association with obesity associated non-alcoholic fatty liver disease.
Study limitations
This has a number of limitations including the relatively low number of participants per group and the cross-sectional nature of the study limited the interpretation of the findings from a pathophysiological point of view. The observational nature of the findings requires functional validation before suggesting any causalities, especially as some findings were based on weak to moderate associations. Furthermore, since blood samples were collected at multiple sites, a batch effect may have occurred, but this was mitigated by standardized protocols for sample collection, processing and storage. It is possible that other unmeasured factors may have impacted our data including dietary habits, medication/supplements and other unknown environmental factors; however, inclusion of principle components in the regression model may have captured part of these potential confounding factors. Finally, controls were not matched for age and gender compared to the study groups, adding an additional variable; however, both age and gender were corrected for in the analysis, but their influence over metabolic differences cannot be ruled out.
Conclusion
In the comparison between equally obese insulin sensitive and insulin resistance individuals, phospholipid metabolites including choline, glycerophosphoethanolamine and glycerophosphorylcholine (GPC) were significantly altered. In addition, several metabolites were identified and were confirmatory for insulin resistance and T2DM (such as glucose and 1,5-AG) or their comorbidities (such as 3-hydroxylaurate, 3-hydroxymyristate, homoarginine and dimethylarginine). This pilot study also identified novel metabolic markers such as the medium chain fatty acids 3-hydroxyoctanoate and 3-hydroxydecanoate and highlighted their potential link to non-alcoholic fatty liver disease, a hallmark of increased risk of obesity-associated insulin resistance. Further studies are needed to confirm these associations in prospective cohorts and to investigate their functional relevance.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
body mass index
- DBP:
-
diastolic blood pressure
- FBG:
-
fasting blood glucose
- HDL:
-
high density lipoprotein
- HOMA-IR:
-
homeostatic model assessment
- IL-6:
-
interleukin 6
- LDL:
-
low density lipoprotein
- MAP:
-
mean arterial blood pressure
- NARP:
-
non-aqueous reverse phase UHPLC separation
- OIS:
-
obese insulin sensitive
- OIR:
-
obese insulin resistant
- OM:
-
omental
- OPLS-DA:
-
orthogonal partial least square discriminate analysis
- PCA:
-
principle component analysis
- SBP:
-
systolic blood pressure
- TAGs:
-
triacylglycerols
- T2DM:
-
type 2 diabetes mellitus
- UHPLC:
-
ultra-high-performance liquid chromatography
- CAD:
-
coronary artery disease
- MS:
-
mass spectrometry
- 1,5-AG:
-
1,5-anhydroglucitol
- UPLC:
-
ultra-performance liquid chromatography
- HESI-II:
-
heated electrospray ionization
- LC–MS:
-
liquid chromatography–mass spectrometry
- HILIC:
-
hydrophilic interaction chromatography
- ADMA:
-
asymmetric dimethylarginine
- SDMA:
-
symmetric dimethylarginine
References
Tsuneto A, Hida A, Sera N, Imaizumi M, Ichimaru S, Nakashima E, Seto S, Maemura K, Akahoshi M. Fatty liver incidence and predictive variables. Hypertens Res. 2010;33:638–43.
Kodama S, Horikawa C, Fujihara K, Yoshizawa S, Yachi Y, Tanaka S, Ohara N, Matsunaga S, Yamada T, Hanyu O, Sone H. Quantitative relationship between body weight gain in adulthood and incident type 2 diabetes: a meta-analysis. Obes Rev. 2014;15:202–14.
Bogers RP, Bemelmans WJ, Hoogenveen RT, Boshuizen HC, Woodward M, Knekt P, van Dam RM, Hu FB, Visscher TL, Menotti A, et al. Association of overweight with increased risk of coronary heart disease partly independent of blood pressure and cholesterol levels: a meta-analysis of 21 cohort studies including more than 300 000 persons. Arch Intern Med. 2007;167:1720–8.
Eliassen AH, Colditz GA, Rosner B, Willett WC, Hankinson SE. Adult weight change and risk of postmenopausal breast cancer. JAMA. 2006;296:193–201.
Denis GV, Obin MS. ‘Metabolically healthy obesity’: origins and implications. Mol Aspects Med. 2013;34:59–70.
Jung CH, Lee WJ, Song KH. Metabolically healthy obesity: a friend or foe? Korean J Intern Med. 2017;32:611–21.
Almuraikhy S, Kafienah W, Bashah M, Diboun I, Jaganjac M, Al-Khelaifi F, Abdesselem H, Mazloum NA, Alsayrafi M, Mohamed-Ali V, Elrayess MA. Interleukin-6 induces impairment in human subcutaneous adipogenesis in obesity-associated insulin resistance. Diabetologia. 2016;59:2406–16.
Ctoi AF, Parvu AE, Andreicut AD, Mironiuc A, Crciun A, Ctoi C, Pop ID. Metabolically healthy versus unhealthy morbidly obese: chronic inflammation, nitro-oxidative stress, and insulin resistance. Nutrients. 2018;10:1199.
Elrayess MA, Almuraikhy S, Kafienah W, Al-Menhali A, Al-Khelaifi F, Bashah M, Zarkovic K, Zarkovic N, Waeg G, Alsayrafi M, Jaganjac M. 4-Hydroxynonenal causes impairment of human subcutaneous adipogenesis and induction of adipocyte insulin resistance. Free Radic Biol Med. 2017;104:129–37.
Keane KN, Cruzat VF, Carlessi R, de Bittencourt PI Jr., Newsholme P. Molecular events linking oxidative stress and inflammation to insulin resistance and beta-cell dysfunction. Oxid Med Cell Longev. 2015;2015:181643.
Helaleh M, Diboun I, Al-Tamimi N, Al-Sulaiti H, Al-Emadi M, Madani A, Mazloum NA, Latiff A, Elrayess MA. Association of polybrominated diphenyl ethers in two fat compartments with increased risk of insulin resistance in obese individuals. Chemosphere. 2018;209:268–76.
Jaganjac M, Almuraikhy S, Al-Khelaifi F, Al-Jaber M, Bashah M, Mazloum NA, Zarkovic K, Zarkovic N, Waeg G, Kafienah W, Elrayess MA. Combined metformin and insulin treatment reverses metabolically impaired omental adipogenesis and accumulation of 4-hydroxynonenal in obese diabetic patients. Redox Biol. 2017;12:483–90.
Guasch-Ferre M, Hruby A, Toledo E, Clish CB, Martinez-Gonzalez MA, Salas-Salvado J, Hu FB. Metabolomics in prediabetes and diabetes: a systematic review and meta-analysis. Diabetes Care. 2016;39:833–46.
Al-Sulaiti H, Diboun I, Banu S, Al-Emadi M, Amani P, Harvey TM, Domling AS, Latiff A, Elrayess MA. Triglyceride profiling in adipose tissues from obese insulin sensitive, insulin resistant and type 2 diabetes mellitus individuals. J Transl Med. 2018;16:175.
Jove M, Moreno-Navarrete JM, Pamplona R, Ricart W, Portero-Otin M, Fernandez-Real JM. Human omental and subcutaneous adipose tissue exhibit specific lipidomic signatures. FASEB J. 2014;28:1071–81.
Yousri NA, Mook-Kanamori DO, Selim MM, Takiddin AH, Al-Homsi H, Al-Mahmoud KA, Karoly ED, Krumsiek J, Do KT, Neumaier U, et al. A systems view of type 2 diabetes-associated metabolic perturbations in saliva, blood and urine at different timescales of glycaemic control. Diabetologia. 2015;58:1855–67.
Suhre K. Metabolic profiling in diabetes. J Endocrinol. 2014;221:R75–85.
Rauschert S, Uhl O, Koletzko B, Kirchberg F, Mori TA, Huang RC, Beilin LJ, Hellmuth C, Oddy WH. Lipidomics reveals associations of phospholipids with obesity and insulin resistance in young adults. J Clin Endocrinol Metab. 2016;101:871–9.
Clish CB. Metabolomics: an emerging but powerful tool for precision medicine. Cold Spring Harb Mol Case Stud. 2015;1:a000588.
Rangel-Huerta OD, Pastor-Villaescusa B, Gil A. Are we close to defining a metabolomic signature of human obesity? A systematic review of metabolomics studies. Metabolomics. 2019;15:93.
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28:412–9.
American Diabetes A. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2019. Diabetes Care. 2019;42:S13–28.
Al-Khelaifi F, Diboun I, Donati F, Botre F, Alsayrafi M, Georgakopoulos C, Suhre K, Yousri NA, Elrayess MA. A pilot study comparing the metabolic profiles of elite-level athletes from different sporting disciplines. Sports Med Open. 2018;4:2.
Evans AM, Bridgewater BR, Liu Q, Mitchell MW, Robinson RJ, Dai H, Stewart SJ, DeHaven CD, Miller LAD. High resolution mass spectrometry improves data quantity and quality as compared to unit mass resolution mass spectrometry in high-throughput profiling metabolomics. Metabolomics. 2014;4:1.
DeHaven CD, Evans JM, Dai H, Lawton KA. Software techniques for enabling high-throughput analysis of metabolomic datasets. Metabolomics. 2012;10:167–92.
Evans AM, DeHaven CD, Barrett T, Mitchell M, Milgram E. Integrated, nontargeted ultrahigh performance liquid chromatography/electrospray ionization tandem mass spectrometry platform for the identification and relative quantification of the small-molecule complement of biological systems. Anal Chem. 2009;81:6656–67.
Feng C, Wang H, Lu N, Chen T, He H, Lu Y, Tu XM. Log-transformation and its implications for data analysis. Shanghai Arch Psychiatry. 2014;26:105–9.
Owei I, Umekwe N, Provo C, Wan J, Dagogo-Jack S. Insulin-sensitive and insulin-resistant obese and non-obese phenotypes: role in prediction of incident pre-diabetes in a longitudinal biracial cohort. BMJ Open Diabetes Res Care. 2017;5:e000415.
Roberson LL, Aneni EC, Maziak W, Agatston A, Feldman T, Rouseff M, Tran T, Blaha MJ, Santos RD, Sposito A, et al. Beyond BMI: the “metabolically healthy obese” phenotype & its association with clinical/subclinical cardiovascular disease and all-cause mortality—a systematic review. BMC Public Health. 2014;14:14.
Halama A, Aye MM, Dargham SR, Kulinski M, Suhre K, Atkin SL. Metabolomics of dynamic changes in insulin resistance before and after exercise in PCOS. Front Endocrinol (Lausanne). 2019;10:116.
Pienaar PR, Micklesfield LK, Levitt NS, Gooding K, Shore AC, Goedecke JH, Gill JM, Lambert EV. Insulin resistance is associated with lower acetylcholine-induced microvascular reactivity in nondiabetic women. Metab Syndr Relat Disord. 2014;12:178–84.
Corbin KD, Zeisel SH. Choline metabolism provides novel insights into nonalcoholic fatty liver disease and its progression. Curr Opin Gastroenterol. 2012;28:159–65.
Karanjia RN, Crossey MM, Cox IJ, Fye HK, Njie R, Goldin RD, Taylor-Robinson SD. Hepatic steatosis and fibrosis: non-invasive assessment. World J Gastroenterol. 2016;22:9880–97.
Bugianesi E, Moscatiello S, Ciaravella MF, Marchesini G. Insulin resistance in nonalcoholic fatty liver disease. Curr Pharm Des. 2010;16:1941–51.
Karaca U, Schram MT, Houben AJ, Muris DM, Stehouwer CD. Microvascular dysfunction as a link between obesity, insulin resistance and hypertension. Diabetes Res Clin Pract. 2014;103:382–7.
Lim HY, Wang W, Wessells RJ, Ocorr K, Bodmer R. Phospholipid homeostasis regulates lipid metabolism and cardiac function through SREBP signaling in Drosophila. Genes Dev. 2011;25:189–200.
Dungan KM. 1,5-anhydroglucitol (GlycoMark) as a marker of short-term glycemic control and glycemic excursions. Expert Rev Mol Diagn. 2008;8:9–19.
Perlmuter LC, Flanagan BP, Shah PH, Singh SP. Glycemic control and hypoglycemia: is the loser the winner? Diabetes Care. 2008;31:2072–6.
Chickos JS, Way BA, Wilson J, Shaharuzzaman M, Laird J, Landt M. Analysis of 3-hydroxydodecanedioic acid for studies of fatty acid metabolic disorders: preparation of stable isotope standards. J Clin Lab Anal. 2002;16:115–20.
Weil D, Pais de Barros JP, Mourey G, Laheurte C, Cypriani B, Badet N, Delabrousse E, Grandclement E, Di Martino V, Saas P, et al. Circulating levels of 3-hydroxymyristate, a direct quantification of endotoxaemia in noninfected cirrhotic patients. Liver Int. 2019;39:106–14.
Pilz S, Putz-Bankuti C, Meinitzer A, Marz W, Kienreich K, Stojakovic T, Pieber TR, Stauber RE. Association of homoarginine and methylarginines with liver dysfunction and mortality in chronic liver disease. Amino Acids. 2015;47:1817–26.
Nijveldt RJ, Van Leeuwen PA, Van Guldener C, Stehouwer CD, Rauwerda JA, Teerlink T. Net renal extraction of asymmetrical (ADMA) and symmetrical (SDMA) dimethylarginine in fasting humans. Nephrol Dial Transplant. 2002;17:1999–2002.
Liu J, Lkhagva E, Chung HJ, Kim HJ, Hong ST. The pharmabiotic approach to treat hyperammonemia. Nutrients. 2018;10:140.
Mizutani N, Hayakawa C, Ohya Y, Watanabe K, Watanabe Y, Mori A. Guanidino compounds in hyperargininemia. Tohoku J Exp Med. 1987;153:197–205.
Tserng KY, Jin SJ, Kerr DS, Hoppel CL. Urinary 3-hydroxydicarboxylic acids in pathophysiology of metabolic disorders with dicarboxylic aciduria. Metabolism. 1991;40:676–82.
Dorland L, Ketting D, Bruinvis L, Duran M. Medium- and long-chain 3-hydroxymonocarboxylic acids: analysis by gas chromatography combined with mass spectrometry. Biomed Chromatogr. 1991;5:161–4.
Bennett MJ, Spotswood SD, Ross KF, Comfort S, Koonce R, Boriack RL, IJlst L, Wanders RJ. Fatal hepatic short-chain L-3-hydroxyacyl-coenzyme A dehydrogenase deficiency: clinical, biochemical, and pathological studies on three subjects with this recently identified disorder of mitochondrial beta-oxidation. Pediatr Dev Pathol. 1999;2:337–45.
Sherriff JL, O’Sullivan TA, Properzi C, Oddo JL, Adams LA. Choline, its potential role in nonalcoholic fatty liver disease, and the case for human and bacterial genes. Adv Nutr. 2016;7:5–13.
Acknowledgements
We thank Qatar National Research Fund (QNRF; Grant No. NPRP8-059-1-009) and the Biomedical Research Program funds of Weill Cornell Medicine—Qatar, a program funded by the Qatar Foundation for funding this project. The statements made herein are solely the responsibility of the authors.
Funding
This publication was made possible by NPRP grant NPRP8-059-1-009 from the Qatar National Research Fund (a member of Qatar Foundation). The findings achieved herein are solely the responsibility of the author[s].
Author information
Authors and Affiliations
Contributions
HS carried out most of the sample preparation, data acquisition and analysis, helped with drafting the article and approved the final version. ID carried out the statistical analysis and helped with data interpretation. MA, AD, FM, and SA contributed to the study design, sample collection and data analysis. MAE and NAM were lead principle investigators, designed the experiments, supervised progress, analyzed data and wrote and approved the final version of the article. MAE and NAM are responsible for the integrity of the work as a whole. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
All participants provided informed consent. Protocols were approved by Institutional Review Boards of Ani Doping Lab Qatar (X2017000224) and Weill Cornell Medicien-Qatar (15-00007).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1: Figure S1.
Boxplot of metabolites in lean, OIS, OIR and T2DM that belong to the enriched phospholipid pathway differentiating OIS and OIR+T2DM groups.
Additional file 2: Table S1.
Metabolites associated with disease progression.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Al-Sulaiti, H., Diboun, I., Agha, M.V. et al. Metabolic signature of obesity-associated insulin resistance and type 2 diabetes. J Transl Med 17, 348 (2019). https://doi.org/10.1186/s12967-019-2096-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12967-019-2096-8