
Abstract
Background
Atrial fibrillation is a progressive arrhythmia, the exact mechanism underlying the progressive nature of recurrent AF episodes is still unknown. Recently, it was found that key players of the protein quality control system of the cardiomyocyte, i.e. Heat Shock Proteins, protect against atrial fibrillation progression by attenuating atrial electrical and structural remodeling (electropathology). HALT & REVERSE aims to investigate the correlation between electropathology, as defined by endo- or epicardial mapping, Heat Shock Protein levels and development or recurrence of atrial fibrillation following pulmonary vein isolation, or electrical cardioversion or cardiothoracic surgery.
Study design
This study is a prospective observational study. Three separate study groups are defined: (1) cardiothoracic surgery, (2) pulmonary vein isolation and (3) electrical cardioversion. An intra-operative high-resolution epicardial (group 1) or endocardial (group 2) mapping procedure of the atria is performed to study atrial electropathology. Blood samples for Heat Shock Protein determination are obtained at baseline and during the follow-up period at 3 months (group 2), 6 months (groups 1 and 2) and 1 year (group 1 and 2). Tissue samples of the right and left atrial appendages in patients in group 1 are analysed for Heat Shock Protein levels and for tissue characteristics. Early post procedural atrial fibrillation is detected by continuous rhythm monitoring, whereas late post procedural atrial fibrillation is documented by either electrocardiogram or 24-h Holter registration.
Conclusion
HALT & REVERSE aims to identify the correlation between Heat Shock Protein levels and degree of electropathology. The study outcome will contribute to novel diagnostic tools for the early recognition of clinical atrial fibrillation.
Trial Registrations: Rotterdam Medical Ethical Committee MEC-2014-393, Dutch Trial Registration NTR4658
Similar content being viewed by others


Background
Atrial fibrillation (AF) initially presents with short, self-terminating episodes and progresses into long-lasting episodes which are unlikely to convert spontaneously to sinus rhythm [1]. The exact mechanism underlying this progression is unknown. At present, there are no diagnostic tests or biomarkers available predicting recurrences of progressive AF episodes. In daily clinical practice, we can for example, not predict which patients develop AF following cardiac surgery or AF recurrences after pulmonary vein isolation (PVI) or electrical cardioversion (ECV).
AF persistence induces atrial remodeling on an electrical, structural and contractile level, also referred to as electropathology [2]. Electrical changes such as shortening of AF cycle length and contractile dysfunction occur within days after AF onset [3, 4]. After weeks of AF persistence, structural alterations become manifest in the extracellular matrix and in cardiomyocytes [1, 5–7]. Electrical and contractile abnormalities are completely reversible within weeks or days after restoration of sinus rhythm [3, 7–10], whereas recovery from structural remodeling is slow and takes up to months [11]. This finding indicates that structural remodeling underlies AF progression and recurrences. Therefore, research is directed at identifying key pathways involved in structural remodeling.
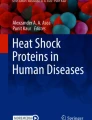
Recently it was demonstrated that derailment of cardiomyocyte proteostasis, underlies AF progression and recurrences [12–15]. Cells, including cardiomyocytes, depend for proper functioning on the maintenance of proteostasis: the balance in protein synthesis, folding, assembling, trafficking, and clearance [16, 17] (Fig. 1). Chaperones, mainly consisting of Heat Shock Proteins (HSPs), assist in the maintenance of proteostasis [17–19]. Upon acute stress e.g. in paroxysmal AF, HSPs are upregulated [20]. The progressive nature of AF lies in the gradual, often age-related, exhaustion of the HSP levels and subsequent derailment of proteostasis, resulting in structural remodeling and contractile dysfunction of cardiomyocytes (Fig. 2). Therefore, compounds that boost HSP expression, such as geranylgeranylacetone (GGA) and GGA derivatives [21, 22], are of clinical interest. Indeed, HSPs boosting, via Heat Shock Factor-1 activation, protected against derailment of proteostasis and AF progression and recurrences in several experimental AF models, including tachypaced cardiomyocytes [23], Drosophilas [15] and canine models [24].

Proteostasis is the balance between protein expression, folding, function and clearance in the cell. When proteins are generated at the ribosomes after translation, chaperones, such as heat shock proteins, guide proper protein folding, and when not folded correctly, they guide remodeling of the protein. Furthermore, these chaperones have a role in limiting protein aggregation and they have a role in protein degradation

Concept of the HALT & REVERSE project. In the normal heart Protein Quality Control (PQC) and the Heat Shock Response (HSR, upper panel: green area) maintain proteostasis in times of stress. However, with the duration of AF and with increasing age, the heat shock protein (HSP) levels get exhausted. This leads to a derailment of proteostasis (upper panel: red area), resulting in structural remodeling and contractile dysfunction of cardiomyocytes, because of, amongst others, degradation of sarcomers (myolysis, left and right lower panel). AF progresses in time (upper panel: solid line), which is rooted in the underlying electropathology. By pharmacological boosting of HSPs, we aim to HALT or even REVERSE atrial electropathology and consequently AF progression (upper panel: dashed line)
The HALT & REVERSE (H sf1 A ctivators L ower C ardiomyocyt damage: T owards a novel approach to REVERSE atrial fibrillation, MEC 2014-393, NTR 4658) project focusses on the correlation between HSPs and progression of electropathology [2]. Hereto, the HSP levels in blood and atrial tissue samples are determined and related to electrophysiological characteristics of the atria obtained from epicardial mapping during cardiothoracic surgery and endovascular mapping during PVI. The findings will elucidate whether HSP levels and electrophysiological characteristics represent a novel diagnostic tool (a so-called “bio-electrical fingerprint”) to predict the clinical outcome for AF patients and/or cardiac surgery.
Study design
HALT & REVERSE is a prospective observational study, with a planned duration of 48 months. This study is carried out according to the principals of the Declaration of Helsinki Version and in accordance with the Medical Research involving Human Subjects Act. The study is approved by the Rotterdam local medical ethical committee (MEC 2014-393).
Study objectives
The primary study objectives are to test the correlation between atrial electropathology as visualised by high-resolution epicardial mapping or endovascular mapping, HSP levels, atrial tissue characteristics and clinical characteristics in patients undergoing either open chest cardiac surgery, PVI or ECV. Secondly, the correlation between HSP levels and development or recurrence of AF in patients undergoing cardiothoracic surgery, PVI or ECV is tested.
Study population
For the HALT & REVERSE project, three separate study groups are defined, consisting of patients scheduled for (1) cardiothoracic surgery, (2) PVI and (3) ECV for symptomatic AF. Each group contains 100 consecutive patients. Patients are recruited at the Department of Cardiothoracic Surgery or at the Department of Cardiology at the Erasmus Medical Center, Rotterdam, The Netherlands. Prior to enrolling in the study, each patient is provided an oral and a written explanation of the study procedure. Written informed consent is obtained from all patients.
Blood samples for baseline HSP level determination taken from all patients prior to the scheduled intervention (surgery, PVI or ECV) (Fig. 3). Patient characteristics (e.g. age, medical history, cardiovascular risk factors) are obtained from the patient’s file.

Timecourse of the HALT & REVERSE project. A baseline blood sample (red bar) is obtained from all patients 1 day prior to the procedure. In the pulmonary vein isolation—and cardiac surgery group, the study procedure (black bar epicardial or endocardial mapping procedure) is performed during the elective therapeutic intervention (yellow bar) and post-procedural continuous rhythm monitoring afterwards (green bars). The blue bars indicate long term follow-up (>3 months) including a visit to the outpatient clinic with electrocardiography, blood samples and 24-h Holter recordings when indicated
Inclusion criteria
In order to be eligible to participate in this study, all subjects must be >18 years old. In the cardiothoracic surgery group, only patients scheduled for elective cardiothoracic surgery for structural heart disease with or without a history of AF are included.
The PVI group will enrol patients with paroxysmal or (long-standing) persistent AF. The ECV group will consist of patients with symptomatic, AF presenting for electrical cardioversion.
Exclusion criteria
A potential subject who meets any of the following criteria in all three study groups are excluded from participation in this study: paced atrial rhythm, haemodynamic instability, presence of cardiac assist devices, usage of inotropic agents prior to intervention or patients undergoing emergency or redo cardiac surgery.
Sample size calculation
Approximately 25 % of patients undergoing cardiothoracic surgery develop early postoperative AF [25]. Estimated AF recurrence rate 1 year after PVI is 45 % as has been shown in previous studies [26–28], whereas the arrhythmia tends to recur within 1 year in 25–40 % [29–31] after ECV.
For none of our study groups, data testing the correlation between HSP and AF development or recurrence (in humans) is available. Therefore, a reliable parameter for sample size calculation is not available. Based upon the data mentioned above, we expect a pilot study with 100 patients in each group to be suitable for further determination of the exact number of patients needed to generate a power of 0.95 with a significance of 0.05.
Intra-operative mapping procedure
High-resolution epicardial mapping of the entire atria according to a previously described mapping scheme is performed during open chest cardiac surgery [32]. A reference electrode is temporarily attached to the right atrial appendage. An indifferent electrode consists of a steel wire, placed in subcutaneous tissue. The mapping procedure will be performed using a custom made 192-site electrode array [32] with a 2 mm inter-electrode distance. Recordings are made at nine consecutive sites following a predefined mapping scheme (Fig. 4) during sinus rhythm (5 s/site), during pacing maneuvers for inducing AF (1 site, Bachman’s Bundle), and during AF (10 s/site). Pacing maneuvers will be performed with epicardial atrial fixed rate pacing at 250–300–350 beats per minute successively, using a standard temporary pacemaker device. If AF sustains until the end of the mapping procedure, sinus rhythm will be restored with 5–10 Joule synchronous electric cardioversion.

Epicardial mapping scheme. 1 Left superior pulmonary vein; 2 right superior pulmonary vein; 3 left inferior pulmonary vein; 4 right inferior pulmonary vein; 5 inferior caval vein; 6 superior caval vein; 7 coronary sinus. The left and right atrium and Bachmann’s Bundle are mapped following a predefined epicardial mapping scheme along anatomical structures, by the use of an 192 polar electrode array (green)
After introduction cannulas of the cardiopulmonary bypass into the right atrium via the right atrial appendage (RAA) a tissue sample is obtained from the incision site in all patients. A tissue sample of the left atrial appendage (LAA) is obtained if the LAA is incised or amputated during surgery. All collected tissue samples are immediately snap-frozen in liquid nitrogen and stored at −80 °C.
After the surgical procedure, heart rhythm is continuously monitored until hospital discharge in order to detect early post-operative AF (PoAF). PoAF is defined as a complete irregular heartbeat without consistent P waves, sustaining for at least 30 s. At 6 months and 1 year after the procedure, patients visit the outpatient clinic for detection of late post-operative AF. A 12-lead electrocardiogram and a blood sample for HSP analysis are obtained. A 24-h Holter registration is performed when AF is suspected.
Pulmonary vein isolation
An endovascular mapping procedure is performed prior to isolation of the pulmonary veins. Atrial electropathology is studied by means of programmed electrical stimulation in the right and the left atrium, including fixed rate atrial pacing, delivery of atrial extra systoles and decremental pacing maneuvers. Recordings of the right atrium are made by a decapolar catheter at the right atrial free wall and pacing is performed from the ablation catheter, which is positioned in the RAA. Mapping in the left atrium is performed by placing a Lasso catheter at the posterior wall and a decapolar catheter in the coronary sinus, while pacing from the left atrial roofline. Subsequently, the PVI is performed according to the electrophysiologist’ choice by either radiofrequency ablation or cryoballoon ablation.
According to standard care, heart rhythm is monitored continuously until discharge. Recordings are analyzed to detect early AF episodes, sustained for at least 30 s. At 3, 6 months and 1 year after the procedure, patients visit the outpatient clinic. During these visits, 12-lead ECGs and 24-h Holter registrations are performed to detect late post procedural AF recurrences and an additional blood sample is obtained for HSP level determination.
Electrical cardioversion
Patients will be interviewed by telephone at 6 and 12 months to detect AF recurrences.
Tissue analysis
All obtained blood samples and atrial tissue samples are stored at −80 °C until analysis. All samples are tested for HSP biomarkers, including HSP70 and HSP27. Biomarker levels are determined by commercially available ELISA’s and Western blot analysis.
Main study parameters
Intra-operative mapping
Custom-made software used for off-line analysis of the recordings have previously been described in detail [32–34]. Local activation times of the unipolar atrial potentials are automatically detected in order to reconstruct color-coded activation-, conduction block-, breakthrough-, voltage- and wavemaps during sinus rhythm and AF [32–34]. An example of an activation and wavemap constructed during AF is given in Fig. 5. The maps are used to quantify electrophysiological variables. These variables are correlated with the pre-operative HSP level and development of post-operative AF.

Epicardial high-resolution mapping of the atria. Atrial electrograms recorded during sinus rhythm (SR), atrial pacing (P) and (electrically induced) atrial fibrillation (AF) obtained during the epicardial mapping procedure are shown in the upper panel. The left lower panel shows an example of an activation map during electrically induced AF of the right atrium in a patient undergoing coronary artery bypass grafting without a history of AF. Isochrones are drawn at 5 ms, areas of conduction block are indicated by black bars, the origin of peripheral and epicardial breakthrough waves by respectively grey dots and white asterisks. The arrows indicate main activation direction. Corresponding wavemap is displayed in the right lower panel. The wavemap shows the different types of fibrillation waves entering the mapping area from various directions. These maps are used to determine the incidence of e.g. conduction block and epicardial breakthrough
Pulmonary vein isolation
The degree of fractionated electrograms obtained from multiple sites in the right and left atrium are studied for fractionation and cycle length variation. HSP levels prior to PVI are correlated with the development of AF recurrence.
Electrical cardioversion
Correlation between HSP levels prior to cardioversion and successful restoration of sinus rhythm and AF recurrences is determined.
Study endpoints
For all groups, endpoint of the study is reached when AF develops after cardiac surgery or recurs after ECV or PVI. The correlation between several biomarkers (HSP70, HSP27) and development or recurrences of AF is determined, but also the correlation between degree of electropathology and development or recurrences of AF. The relationship between atrial electrophysiological variables, as visualised by epicardial mapping, and structural tissue characteristics are tested. The findings will indicate whether HSP levels and/or the degree of electropathology represent a novel diagnostic tool to predict the clinical outcome of AF progression and/or recurrences.
Statistical analysis
The association between biomarker levels and development or recurrence of atrial fibrillation is calculated using multivariate logistic regression (for short term outcome) and cox regression models (for long-term outcome). Furthermore, Kaplan–Meier life tables are created for the three groups (cardiac surgery, PVI and ECV) and Log rank tests are used to compare the different groups.
ANOVA is utilized to compare various electrophysiological continuous parameters, for categorical parameters the Chi-square test will be used. Repeated HSP measurements are conducted by Joint modeling and mixed modeling analysis. Multiple biomarkers levels are corrected by ANOVA with Bonferoni adjustments.
Conclusion
HALT & REVERSE aims to examine the interplay between electropathological substrate underlying AF, and HSP levels in the blood and atrial tissue, in order to predict development, recurrence or progression of AF. The results will elucidate whether HSP levels and electrophysiological characteristics can be used as a future diagnostic tool in the clinical setting.
Abbreviations
- AF:
-
atrial fibrillation
- ECG:
-
electrocardiogram
- ECV:
-
electrical cardioversion
- GGA:
-
geranylgeranylacetone
- HALT & REVERSE:
-
Hsf1 activators lower cardiomyocyt damage; towards a novel approach to reverse atrial fibrillation
- HSP:
-
heat shock protein
- LAA:
-
left atrial appendage
- PVI:
-
pulmonary vein isolation
- PoAF:
-
post-operative atrial fibrillation
- RAA:
-
right atrial appendage
References
Camm AJ, Kirchhof P, Lip GYH, Schotten U, Savelieva I, Ernst S, et al. Guidelines for the management of atrial fibrillation The Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J. 2010;31(19):2369–429. doi:10.1093/eurheartj/ehq278.
Lanters EAH, van Marion DMS, Steen H, de Groot NMS, Brundel BJJM. The future of atrial fibrillation therapy: intervention on heat shock proteins influencing electropathology is the next in line. Neth Heart J. 2015;23(6):327–33. doi:10.1007/s12471-015-0699-0.
Allessie M, Ausma J, Schotten U. Electrical, contractile and structural remodeling during atrial fibrillation. Cardiovasc Res. 2002;54(2):230–46. doi:10.1016/S0008-6363(02)00258-4.
Schotten U, Duytschaever M, Ausma J, Eijsbouts S, Neuberger HR, Allessie M. Electrical and contractile remodeling during the first days of atrial fibrillation go hand in hand. Circulation. 2003;107(10):1433–9. doi:10.1161/01.Cir.000055314.10801.4f.
Ausma J, Litjens N, Lenders MH, Duimel H, Mast F, Wouters L, et al. Time course of atrial fibrillation-induced cellular structural remodeling in atria of the goat. J Mol Cell Cardiol. 2001;33(12):2083–94. doi:10.1006/jmcc.2001.1472.
Neuberger HR, Schotten U, Blaauw Y, Vollmann D, Eijsbouts S, van Hunnik A, et al. Chronic atrial dilation, electrical remodeling, and atrial fibrillation in the goat. J Am Coll Cardiol. 2006;47(3):644–53. doi:10.1016/j.jacc.2005.09.041.
Wijffels MCEF, Kirchhof CJHJ, Dorland R, Allessie MA. Atrial-fibrillation begets atrial-fibrillation—a study in awake chronically instrumented goats. Circulation. 1995;92(7):1954–68.
Yu WC, Lee SH, Tai CT, Tsai CF, Hsieh MH, Chen CC, et al. Reversal of atrial electrical remodeling following cardioversion of long-standing atrial fibrillation in man. Cardiovasc Res. 1999;42(2):470–6. doi:10.1016/S0008-6363(99)00030-9.
Ausma J, Duimel H, Borgers M, Allessie MA. Recovery of structural remodeling after cardioversion of chronic atrial fibrillation. Circulation. 2000;102(18):153.
Ausma J, Duimel H, Lenders MH, Allessie M, Ramaekers F, Borgers M. Altered expression patterns of structural proteins induced by 16 weeks of atrial fibrillation are partially restored 8 weeks after cardioversion. Eur Heart J. 2000;21:241.
Ausma J, van der Velden HMW, Lenders MH, van Ankeren EP, Jongsma HJ, Ramaekers FCS, et al. Reverse structural and gap-junctional remodeling after prolonged atrial fibrillation in the goat. Circulation. 2003;107(15):2051–8. doi:10.1161/01.Cir.0000062689.04037.3f.
Meijering RAM, Henning RH, Brundel BJJM. Reviving the protein quality control system: Therapeutic target for cardiac disease in the elderly. Trends Cardiovas Med. 2015;25(3):243–7. doi:10.1016/j.tcm.2014.10.013.
Meijering RAM, Zhang DL, Hoogstra-Berends F, Henning RH, Brundel BJJM. Loss of proteostatic control as a substrate for atrial fibrillation: a novel target for upstream therapy by heat shock proteins. Front Physiol. 2012;3:36. doi:10.3389/Fphys.2012.00036.
Zhang DL, Wu CT, Qi XY, Meijering RAM, Hoogstra-Berends F, Tadevosyan A, et al. Activation of histone deacetylase-6 induces contractile dysfunction through derailment of alpha-tubulin proteostasis in experimental and human atrial fibrillation. Circulation. 2014;129(3):346–58. doi:10.1161/Circulationaha.113.005300.
Zhang DL, Ke L, Mackovicova K, Van Der Want JJL, Sibon OCM, Tanguay RM, et al. Effects of different small HSPB members on contractile dysfunction and structural changes in a Drosophila melanogaster model for Atrial Fibrillation. J Mol Cell Cardiol. 2011;51(3):381–9. doi:10.1016/j.yjmcc.2011.06.008.
Balch WE, Morimoto RI, Dillin A, Kelly JW. Adapting proteostasis for disease intervention. Science. 2008;319(5865):916–9. doi:10.1126/science.1141448.
Willis MS, Patterson C. Proteotoxicity and cardiac dysfunction reply. New Engl J Med. 2013;368(18):1755.
Powers ET, Balch WE. Diversity in the origins of proteostasis networks—a driver for protein function in evolution. Nat Rev Mol Cell Biol. 2013;14(4):237–48. doi:10.1038/Nrm3542.
Wang XJ, Robbins J. Heart failure and protein quality control. Circ Res. 2006;99(12):1315–28. doi:10.1161/01.Res.0000252342.61447.A2.
Brundel BJJM, Henning RH, Ke L, van Gelder IC, Crijns HJGM, Kampinga HH. Heat shock protein upregulation protects against pacing-induced myolysis in HL-1 atrial myocytes and in human atrial fibrillation. J Mol Cell Cardiol. 2006;41(3):555–62. doi:10.1016/j.yjmcc.2006.06.068.
Brundel BJ, Oi XY, Yeh YH, Shiroshita-Takeshita A, Chartier D, Henning RH, et al. HSP27 is sufficient and required for prevention of tachycardia induced remodeling in a cell model for tachypacing. Circulation. 2006;114(18):9.
Hoogstra-Berends F, Meijering RAM, Zhang DL, Heeres A, Loen L, Seerden JP, et al. Heat shock protein-inducing compounds as therapeutics to restore proteostasis in atrial fibrillation. Trends Cardiovas Med. 2012;22(3):62–8.
Brundel BJJM, Kampinga HH, Henning RH. Calpain inhibition prevents pacing-induced cellular remodeling in a HL-1 myocyte model for atrial fibrillation. Cardiovasc Res. 2004;62(3):521–8. doi:10.1016/j.cardiores.2004.02.007.
Sakabe M, Shiroshita-Takeshita A, Brundel B, Nattel S. Effects of heat shock protein induction on atrial fibrillation caused by acute atrial ischemia. Circulation. 2006;114(18):200.
Pillarisetti J, Patel A, Bommana S, Guda R, Falbe J, Zorn GT, et al. Atrial fibrillation following open heart surgery: long-term incidence and prognosis. J Interv Card Electrophysiol. 2014;39(1):69–75. doi:10.1007/s10840-013-9830-6.
Kuhne M, Schaer B, Ammann P, Suter Y, Osswald S, Sticherling C. Cryoballoon ablation for pulmonary vein isolation in patients with paroxysmal atrial fibrillation. Swiss Med Wkly. 2010;140(15–16):214–21.
Steinberg JS, Palekar R, Sichrovsky T, Arshad A, Preminger M, Musat D, et al. Very long-term outcome after initially successful catheter ablation of atrial fibrillation. Heart Rhythm. 2014;11(5):771–6. doi:10.1016/j.hrthm.2014.02.003.
Van Belle Y, Janse P, Theuns D, Szili-Torok T, Jordaens L. One year follow-up after cryoballoon isolation of the pulmonary veins in patients with paroxysmal atrial fibrillation. Europace. 2008;10(11):1271–6. doi:10.1093/europace/eun218.
Gitt AK, Smolka W, Michailov G, Bernhardt A, Pittrow D, Lewalter T. Types and outcomes of cardioversion in patients admitted to hospital for atrial fibrillation: results of the German RHYTHM-AF Study. Clin Res Cardiol. 2013;102(10):713–23. doi:10.1007/s00392-013-0586-x.
Blich M, Edoute Y. Electrical cardioversion for persistent or chronic atrial fibrillation: outcome and clinical factors predicting short and long term success rate. Int J Cardiol. 2006;107(3):389–94. doi:10.1016/j.ijcard.2005.03.057.
Pisters R, Nieuwlaat R, Prins MH, Le Heuzey JY, Maggioni AP, Camm AJ, et al. Clinical correlates of immediate success and outcome at 1-year follow-up of real-world cardioversion of atrial fibrillation: the Euro Heart Survey. Europace. 2012;14(5):666–74. doi:10.1093/europace/eur406.
Yaksh A, Kik C, Knops P, Roos-Hesselink JW, Bogers AJJC, Zijlstra F, et al. Atrial fibrillation: to map or not to map? Neth Heart J. 2014;22(6):259–66. doi:10.1007/s12471-013-0481-0.
de Groot NMS, Houben RPM, Smeets JL, Boersma E, Schotten U, Schalij MJ, et al. Electropathological substrate of longstanding persistent atrial fibrillation in patients with structural heart disease epicardial breakthrough. Circulation. 2010;122(17):1674–82. doi:10.1161/Circulationaha.109.910901.
Allessie MA, de Groot NMS, Houben RPM, Schotten U, Boersma E, Smeets JL, et al. Electropathological substrate of long-standing persistent atrial fibrillation in patients with structural heart disease. Circ Arrhythm Electrophysiol. 2010;3(6):606–15. doi:10.1161/Circep.109.910125.
Authors’ contributions
EL, DM, BB, NG contributed to conception and design of the study and drafted the manuscript. CK, AB contributed to the study design and critically revised the manuscript. HS contributed to conception of the study and critically revised the manuscript. MA contributed to the study design a critically revised the manuscript. All authors read and approved the final manuscript.
Acknowledgements
Dr. N.M.S. de Groot is supported by grants from the Erasmus Medical Center fellowship, Dutch Heart Foundation (2011T046), CoolSingel foundation (project no. 212), LSH-Impulse grant (40-43100-98-008), Bayer and Boehringer Ingelheim and Dr. B.J.J.M. Brundel by the LSH-Impulse grant (40-43100-98-008) and the Dutch Heart Foundation (2013T144 and 2013T096).
Competing interests
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Lanters, E.A.H., van Marion, D.M.S., Kik, C. et al. HALT & REVERSE: Hsf1 activators lower cardiomyocyt damage; towards a novel approach to REVERSE atrial fibrillation. J Transl Med 13, 347 (2015). https://doi.org/10.1186/s12967-015-0714-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12967-015-0714-7