
Abstract
Background
Time spent in sleep, sedentary behaviour (SB), and physical activity are exhaustive and mutually exclusive parts of a 24-h day that need to be considered in a combination. The aim of this study was to identify validated self-reported tools for assessment of movement behaviours across the whole 24-h day, and to review their attributes and measurement properties.
Methods
The databases PubMed, Scopus, and SPORTDiscus were searched until September 2023. Inclusion criteria were: (i) published in English language, (ii) per-reviewed paper, (iii) assessment of self-reported time spent in sleep, SB, and physical activity, (iv) evaluation of measurement properties of all estimates across the full 24-h day, and (v) inclusion of adolescents, adults, or older adults. The methodological quality of included studies was assessed using the Consensus-based Standards for the selection of health Measurement Instruments checklist.
Results
Our search returned 2064 records. After studies selection, we included 16 articles that reported construct validity and/or test-retest reliability of 12 unique self-reported tools – eight questionnaires, three time-use recalls, and one time-use diary. Most tools enable assessment of time spent in sleep, and domain-specific SB and physical activity, and account that sum of behaviours should be 24 h. Validity (and reliability) correlation coefficients for sleep ranged between 0.22 and 0.69 (0.41 and 0.92), for SB between 0.06 and 0.57 (0.33 and 0.91), for light-intensity physical activity between 0.18 and 0.46 (0.55 and 0.94), and for moderate- to vigorous-intensity physical activity between 0.38 and 0.56 (0.59 and 0.94). The quality of included studies being mostly fair-to-good.
Conclusions
This review found that only a limited number of validated self-reported tools for assessment of 24-h movement behaviours are currently available. Validity and reliability of most tools are generally adequate to be used in epidemiological studies and population surveillance, while little is known about adequacy for individual level assessments and responsiveness to behavioural change. To further support research, policy, and practice, there is a need to develop new tools that resonate with the emerging 24-h movement paradigm and to evaluate measurement properties by using compositional data analysis.
Systematic review registration
PROSPERO CRD42022330868.
Similar content being viewed by others

Background
Sleep, sedentary behaviour (SB), and physical activity (i.e., 24-h movement behaviours) are important determinants of health and well-being [1, 2]. Research shows that sufficient sleep duration, less SB, and greater physical activity are associated with a decreased risk of numerous chronic non-communicable diseases including cardiovascular disease, type 2 diabetes, cancer, mental disorders, and all-cause mortality [2,3,4,5].
Movement behaviours have been traditionally examined and promoted in isolation from each other. However, a recent recognition that time spent in sleep, SB, and physical activity are exhaustive and mutually exclusive parts of any time period (e.g., 24-h day) has shifted the paradigm towards examining movement behaviours in a combination [6,7,8]. Moreover, particular concern has been drawn to the methodological shortcomings of most previous epidemiological studies on time spent in movement behaviours that examined specific movement behaviour in isolation while violating the assumptions of statistical methods used [9, 10]. Data quantifying time spent in movement behaviours are specific type of data (i.e., compositional data), and their specific mathematical properties need to be respected by using sound statistical methods (i.e., compositional data analysis). In compositional data, relevant information is in the relative distribution of the components, which indicates that the components need to be examined in a combination [9,10,11]. Therefore, there is a need for research tools that simultaneously assess movement behaviours across the whole 24-h day.
This novel paradigm has already been adopted by some public health authorities who also recognised the importance of promoting healthy movement behaviours in an integrated way and developed 24-h movement guidelines [12,13,14,15,16,17,18,19]. According to such guidelines, it is recommended to engage in moderate- to vigorous-intensity physical activity (MVPA) for at least 150 min per week, in light-intensity physical activity (LPA) for several hours per day, to avoid SB to the extent that total daily duration do not exceed eight hours per day, while getting between seven and nine hours of sleep. To monitor population prevalence and trends of adherence to the novel 24-h movement guidelines, surveillance systems need to be adapted accordingly [20].
The assessment of 24-h movement behaviours is also needed for individual level counselling, prescription, and referral of guiding discussions regarding behavioural change. Such treatments could be conducted in clinical care settings and community programs for healthy lifestyle promotion, disease prevention and management as well as in occupational and school settings. It has been advocated that integrated 24-h movement paradigm cater to individual differences (e.g., physical abilities, preferences) and offer a wide variety of counselling options on behavioural change (e.g., trading SB for LPA and/or MVPA only, while keeping sleep unchanged), that can bring health benefits [18]. However, a recent scoping review on features, perceptions, and effectiveness of tools to guide discussions on physical activity, SB, and/or sleep between health care providers and patients showed that tools to guide discussions on integrated 24-h movement behaviours are lacking [21].
Therefore, simultaneous assessment of sleep, SB, and physical activity is needed for research, policy, and practice. Such assessment can be conducted using device-based methods (e.g., accelerometers, inclinometers), self-reported methods (e.g., questionnaires, diaries), or using a combination of both methods (e.g., using sleep time diary to inform sleep detection algorithms for accelerometer data [22]). Both groups of measurement methods show certain strengths and weaknesses; and the choice of the measurement tool is usually guided by the level of reliability and validity required for specific purpose of use, resources available, feasibility, practicality, acceptability, sustainability, and the need to provide immediate feedback [23,24,25,26,27]. While device-based methods have advantages of providing more valid estimates, self-reported methods present lower costs, lower burden, and higher compliance. Self-reported methods can also provide contextual information on movement behaviours (e.g., where, with whom) and estimates of movement behaviours from more distant past. Self-reported tools are therefore indispensable in large-scale epidemiological studies, population surveillance, and practice [21, 26, 28].
Most of the self-reported tools were developed for assessment of only one or two movement behaviours [29,30,31,32,33,34,35,36,37,38], and to the best of our knowledge, self-reported tools for assessment of overall 24-h movement behaviours are scarce. While sleep, SB, and physical activity can be assessed using a combination of different self-reports, such an approach might be compromised and/or being inconvenient as different self-reports may have different recall periods, administration guidelines, or instructions to complete the items. It is also less likely that the sum of all movement behaviours assessed using different tools would equal 24 h (or other finite total). This might be of particular concern when using compositional data analysis that closes composition to the finite total [11] and proportionally rescale the components that do not add to the finite total (e.g., 24 h). Rescaling the data is likely to change measurement properties that need re-evaluation. Therefore, the aim of this study was to identify validated self-reported tools for assessment of movement behaviours across the whole 24-h day, and to review their attributes (movement behaviours being assessed including temporal and contextual information, accounting for a 24-h day, recall period, number of questions) and quantitative measurement properties (construct validity, test-retest reliability, responsiveness).
Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [39], and it was registered in the International Prospective Register of Systematic Reviews (PROSPERO) with a registration number CRD42022330868. The review protocol can be accessed on the PROSPERO website (https://www.crd.york.ac.uk/prospero/).
Eligibility criteria
We included studies that met the following criteria: (i) published in English language, (ii) published in a peer-reviewed journal, (iii) reported assessment of time spent in sleep, SB, and physical activity using a single self-reported tool (without any restriction regarding the mode of administration), (iv) reported construct validity (i.e., the extent to which an instrument provides comparable measures to other validated instrument that measure the construct of interest [40]), test-retest reliability (i.e., the extent to which an instrument provide measures that are consistent from one test administration to the next [40]), or responsiveness (i.e., the ability of an instrument to detect change over time in the construct to be measured [40]) of self-reported estimates of movement behaviours across the full 24-h day, and (v) included adolescents (aged 12 to 17 years), adults (aged 18 to 64 years), or older adults (aged 65 years and older). No limitations regarding the sample size and health status of participants were applied. We excluded studies that reported validity by comparing measures of different constructs (e.g., comparing self-reported MVPA with physical fitness test score), secondary data analysis studies, reviews, and meta-analysis.
Literature search and study selection
A literature search was performed in databases of PubMed, Scopus, and SPORTDiscus. The primary search query combined terms: movement behaviours, self-reported method, and validity/reliability (Supplementary Table 1). The search with no publication time limits was performed in May 2022, and updated in September 2023.
All hits from the databases were transferred to the Mendeley Desktop Reference Management Program. After removing the duplicates, three authors (AŠ, LE, and KK) independently screened the titles and abstracts for eligibility. Afterwards, two authors (AŠ or LE, and KK) independently screened the full texts of potentially relevant articles for the final decision on study inclusion. Disagreements between authors were resolved through discussion and consensus. If there were any uncertainties, the fourth author (NŠ) was consulted. Additionally, to identify any relevant articles that might be missed by our primary search query, we performed a backward and forward citation searching, screened relevant reviews and meta-analysis that were identified through primary search query, and authors’ archive of references. Also, we conducted a secondary search that combined terms: title of the tool (tools that were identified during primary search) and validity/reliability.
Data extraction
Data from the included studies were extracted by two authors (AŠ or LE) and checked by the third author (KK). Disagreements between authors were resolved through discussion and consensus. If there were any uncertainties, the fourth author (NŠ) was consulted. The following information were extracted: (i) first author, (ii) year of publication, (iii) title of the self-reported tool, (iv) type of the self-reported tool, (v) movement behaviours assessed using self-reported tool, (vi) whether and how self-reported tool accounted for the finite sum of daily time spent in sleep, SB, and physical activity, (vii) number of questions, (viii) recall period, (ix) sample characteristics (i.e., sample size, proportion of females, mean age), (x) language of evaluated self-reported tool, (xi) reference tool used, (xii) time interval between two administrations, (xiii) construct validity indicators, (xiv) test-retest reliability indicators, and (xv) responsiveness indicators.
Quality assessment
The methodological quality of included studies was assessed using the Consensus-based Standards for the selection of health Measurement Instruments (COSMIN) checklist [41]. This checklist assesses the appropriateness of study design and statistical methods used in individual studies on measurement properties. The quality of the studies for evaluating validity and reliability was assessed using the 4-point scale (i.e., excellent, good, fair, poor) for each of the checklist items, while the final quality score was assessed using the “worst score counts” principle [42]. The COSMIN checklist used is available in Supplementary Tables 2 and 3. The quality assessment was done independently by two authors (AŠ or LE, and KK). Disagreements between authors were resolved through discussion and consensus. If there were any uncertainties, the fourth author (NŠ) was consulted.
Data presentation and interpretation
The data were narratively presented in tables and arranged according to the type of self-reported method (i.e., questionnaires, time-use recalls, time-use diary). Self-reported tools were listed alphabetically. The first table contains data on attributes of self-reported tools, the second table contains data on construct validity, and the third table contains data on test-retest reliability of self-reported tools.
Criteria on interpreting construct validity and test-retest reliability correlation coefficients were set a priori and were based on the findings from previous systematic reviews on measurement properties of physical activity and SB self-reports (Spearman/Pearson correlation coefficients for construct validity usually range from approximately 0.30 to 0.50 [29, 32, 34]; and Intraclass correlation coefficients (ICC) for test-retest reliability usually range from approximately 0.50 to 0.80 [29, 32, 34]). Convergent validity correlation coefficients were interpreted as: 0 to 0.20 as poor; 0.21 to 0.40 as fair; 0.41 to 0.60 as moderate; 0.61 to 0.80 as substantial; 0.81 to 1.00 as nearly perfect [43]. Test-retest reliability correlation coefficients were interpreted as: 0 to 0.49 as poor; 0.50 to 0.74 as moderate; 0.75 to 0.89 as substantial; 0.90 to 1.00 as nearly perfect [44].
Results
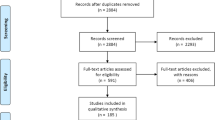
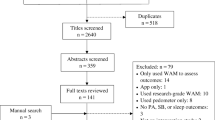
Our search query returned 2064 records (Fig. 1). After removing the duplicates, we screened titles and abstracts of 1507 records. We identified 56 potentially relevant articles and assessed their full texts for eligibility. Of these, we excluded 2 articles that included only children aged 11 years or less [45, 46], 17 articles on tools that do not assess all components across the full 24-h day [47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63], 12 articles that reported measurement properties of some but not all components across the full 24-h day [64,65,66,67,68,69,70,71,72,73,74,75], 7 articles that reported only measurement property of assessing total daily energy expenditure [76,77,78,79,80,81,82] and integrated movement behaviours score [83], 1 article that reported secondary data analysis [84], and 7 review articles [21, 38, 85,86,87,88,89]. Additional seven records were identified through other sources. Finally, 16 articles that reported measurement properties of 12 unique self-reported tools were included in our review [90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105]. There was 100% agreement on the selection of all 16 included articles between the two reviewers (AŠ or LE, and KK).

PRISMA flow diagram on the systematic search process
Attributes of self-reported methods
We identified eight unique self-reported questionnaires, three time-use recalls, and one time-use diary (Table 1). Most questionnaires ask about sleep, and domain-specific SB and physical activity, and account that their sum should be 24 h. The latter is achieved by subtracting non-SB estimates from 24 h to obtain SB (Simple Physical Activity Questionnaire [SIMPAQ]) or by assigning the “remaining time to 24 hours” to SB (Japan Public Health Center-based prospective study- physical activity questionnaire [JPHC-PAQ], Physical activity questionnaire [PAQ], Sedentary Time and Activity Reporting Questionnaire [STAR-Q]) or LPA (Daily Activity Behaviours Questionnaire [DABQ], Physical Activity Scale 2 [PAS 2]). The same method of accounting for 24-h day is also used in one time-use recall (7-Day Physical Activity Recall [7D PAR]), while other two time-use recalls (Computer-Based 24-Hour Physical Activity Recall [cpar24], Multimedia Activity Recall for Children and Adults [MARCA]) are computerised and features of the program ensure/facilitate complete data entry (i.e., 24 h of activities). In computerised time-use recalls, a responder is asked to report activities in the order that they were performed during the day by choosing from a custom compendium of activities. Similarly, in time-use diary (Time-use diary from the Harmonised European Time Use Study [TUD HETUS]) a responder is asked to record activities (in their own words) in the order that they were performed during the day. In computerised time-use recalls and in time-use diary, reported daily activities are converted into sleep, SB, and physical activity by using a compendium of physical activities.
Self-reported measurement tools differ substantially regarding recall period (ranging from the past day to the past year) and comprehensiveness (number of questions for questionnaires ranging from 4 to 88, while time-use recalls and time-use diary record activities over the past day to the past week). Most questionnaires assess total sleep time, domain-specific SB, and domain- and intensity-specific physical activity (DABQ, JPHC-PAQ, PAQ, PAQ SCCS, PAS 2, STAR-Q, 24HMBQ). Most questionnaires also assess at least some specific types of SB and physical activity (Table 1), while only some questionnaires assess sleep timing (DABQ, SIMPAQ, 24HMBQ), movement behaviours at weekdays/weekend days separately (DABQ, 24HMBQ), and social and physical context for some activities (STAR-Q). Time-use recalls (cpar24, MARCA) and time-use diary (TUD HETUS) provide detailed data on specific types of activities and the timing of activities performed during the 24-h day. The TUD HETUS also provide a social and physical context for all reported activities and the level of enjoyment while engaging in activities.
Validity of self-reported methods
A total of 11 studies evaluated validity of 10 self-reported tools for assessment of 24-h movement behaviours among adults (Table 2). Two studies were ranked with an excellent quality [92, 94], three with a good quality [93, 101, 103], three with a fair quality [91, 95, 96], and three with a poor quality [90, 97, 98]. Device-based method was used as a reference method in seven studies, while four studies used another self-reported method to evaluate validity. All but one study used Pearson/Spearman’s correlation coefficient between self-reported method and reference method. Some studies also reported Intraclass correlation coefficient and/or Bland-Altman statistics (e.g., mean difference, limits of agreement).
Studies aggregated self-reported movement behaviours in a diversity of 24-h time-use compositions before being validated. Most studies validated daily time spent in sleep, SB, and physical activity of different intensities, one study validated domain-specific movement behaviours [90], and one study validated time spent in “super domains” [92]. All studies validated each component (i.e., aggregated self-reported movement behaviours) of 24-h time-use composition in isolation. For example, validity correlation coefficients for sleep time ranged between 0.22 and 0.69, for SB between 0.06 and 0.57, for LPA between 0.18 and 0.46, and for MVPA between 0.38 and 0.56.
Reliability of self-reported methods
A total of 11 studies evaluated reliability of 10 unique self-reported tools for assessment of 24-h movement behaviours among adults (Table 3). Three studies were ranked with a good quality [91, 94, 98], seven with a fair quality [95, 96, 99, 100, 102, 104, 105], and one with a poor quality [90]. Studies differed substantially regarding time interval between test and retest administrations (ranged between > 4 h to 15 months). Four studies used Intraclass corelation coefficient to evaluate test-retest reliability, while seven studies reported only Pearson/Spearman’s correlation coefficient. Some studies also reported Bland-Altman statistics (e.g., mean difference, limits of agreement). All studies evaluated test-retest reliability of each component of 24-h time-use composition in isolation. For example, reliability correlation coefficients for sleep time ranged between 0.41 and 0.92, for SB between 0.33 and 0.91, for LPA between 0.55 and 0.94, and for MVPA between 0.59 and 0.94.
Discussion
This systematic review identified 12 validated tools – eight questionnaires, three time-use recalls, and one time-use diary – for assessment of movement behaviours across the whole 24-h day. Most self-reported tools were designed for assessment of sleep, and domain-specific SB and physical activity, and generally showed adequate validity and/or reliability to be used in large-scale epidemiological studies and population surveillance.
Most self-reported tools included in our review showed comparable validity (DABQ, JPHC-PAQ, PAS 2, STAR-Q, 24HMBQ, 7D PAR, cpar24, TUD HETUS) and/or reliability (DABQ, JPHC-PAQ, PAQ, PAS 2.1, STAR-Q, SIMPAQ, 24HMBQ, cpar24, MARCA) correlation coefficients with the validity and/or reliability of most self-reported tools for assessment of a single movement behaviour [29,30,31,32,33,34,35,36,37]. The highest validity was observed for time-use diary TUD HETUS (r range: 0.55 to 0.92), and the highest test-retest reliability for short questionnaire SIMPAQ (rho range: 0.78 to 0.95) and computerised time-use recall MARCA (ICC range: 0.89–0.99). Higher validity of time-use diaries compared to other self-reports that rely on recalling more distant activities has been reported previously [106], and it was suggested that higher validity is associated with diminished recall bias. The highest reliability was observed in two studies that administered self-reported tool twice within the same day [100, 105], while the lowest reliability in a study where time interval between two administrations was more than one year [90]. However, it has been proposed that adequate time interval between two administrations is more than one day (to avoid recalling answers from the first administration), but less than three months for most tools (to guarantee sufficient stability of a behaviour per se) [107]. Therefore, reliability findings in these studies might differ if using adequate time intervals.
Self-reported time spent in sleep, SB, and physical activity is usually under- or over-estimated [29,30,31,32,33,34,35,36,37], which lead to sum of behaviours that do not equal to 24 h. However, most of the self-reported tools included in our review accounted that a sum of behaviours should add to 24 h by using different approaches. Some tools assigned the “remaining time to 24 hours” to either SB or LPA (DABQ, JPHC-PAQ, PAQ, PAS 2, STAR-Q, 7D PAR), one questionnaire (SIMPAQ) provided an alternative method for calculating SB by subtracting non-SB estimates from 24 h, two computerised recalls (cpar24, MARCA) ensured complete data entry by specific features of the program, and time-use diary (TUD HETUS) encourage responder to report activities during the 24-h period by providing a pre-defined recording fields. Most tools that used such approaches showed at least fair validity (DABQ, JPHC-PAQ, STAR-Q, 7D PAR, cpar24, TUD HETUS) and/or reliability (DABQ, JPHC-PAQ, PAQ, PAS 2.1, STAR-Q, SIMPAQ, cpar24, MARCA) for all movement behaviours examined. This is of great importance especially for studies that use compositional data analysis, since all components of time-use composition (e.g., 24-h movement behaviours composition consisting of time spent in sleep, SB, and physical activity) need to have adequate validity and/or reliability so that the time-use composition can be considered as valid and/or reliable.
By using COSMIN checklist, we found that only five validity studies (Table 2) and three reliability studies (Table 3) were ranked with at least good quality. The most frequent reasons for compromised quality of validity studies were poor selection of a reference measure, and insufficient sample size. The most frequent reasons for compromised quality of reliability studies were insufficient description of test and retest conditions, less appropriate use of statistical methods, less optimal time interval between two administrations, and a lack of description how missing data were handled. The COSMIN checklist (Supplementary Tables 2 and 3) can be used in future validation studies to guide methodological decisions in order to achieve high quality of the study. However, a careful consideration should be given to the choice of a reference measure since it is currently largely unknown which tools for assessment of 24-h movement behaviours could be considered as the best reference measure [108,109,110,111]. Accelerometers were frequently proposed to be a “reasonable gold standard” for assessment of free-living movement behaviours; however, hip placement is a preferred location for accurate assessment of physical activity [112], while thigh placement for SB [113], and wrist placement for sleep duration [114]. To avoid usage of multiple accelerometers, it was proposed that the best compromise might be using the same accelerometer at the hip during wake time and at the wrist during bedtime [115], or to combine thigh-worn accelerometer with sleep time diary [116]. The latest method was used in two studies included in our review [93, 94], while other studies used accelerometer placed on the chest, waist, or wrist [96, 97, 101, 103], wearable camera [92], or other self-reported method [90, 91, 95, 98].
Another important consideration is use of statistical analysis. Since data quantifying time spent in movement behaviours are compositional data, a recent study questioned the appropriateness of using Pearson/Spearman’s correlation coefficient and Intraclass correlation coefficients in studies examining validity and reliability of movement behaviours estimates [94]. Although those methods are recommended by COSMIN checklist, they are not intended for compositional data [7]. It has been warned that using traditional statistical methods (that were developed for data in real space) when dealing with compositional data (that lay in a constrained simplex space), may produce misleading results [9, 117]. To the best of our knowledge, compositional data analysis for evaluating validity and reliability of movement behaviours estimates are lacking. Therefore, to further support the development of 24-h movement behaviours research, there is a need to develop statistical analysis suitable for evaluation of validity and reliability of compositional data.
Considerations for research, policy, and practice
The choice of the measurement tool depends on the objective of the study, measurement characteristics of a tool, and resources available. Several decision matrix guides to selecting physical activity or SB measurement tools have been described previously [23, 24, 27]. When selecting the tool, the first step is usually to identify which domains and dimensions of movement behaviours are of interest, and for what purpose data are collected (e.g., study design, individual level counselling). Then, a careful consideration regarding measurement characteristics of the tools (e.g., validity, reliability) and resources available (e.g., cost, time available for administration) is needed.
If the purpose is epidemiological research on the relationship between 24-h movement behaviours and health outcomes, then the important measurement characteristics are strong validity correlations and low random error [23]. However, if the purpose is to assess movement behaviours in longitudinal or intervention studies, then responsiveness to detect change is of great importance [24]. In our review, the strongest validity correlation coefficients were observed for the time-use diary TUD HETUS, while some other tools showed fair-to-substantial correlation coefficients (DABQ, JPHC-PAQ, STAR-Q, 24HMBQ, cpar24), which can be also deemed as sufficient for epidemiological research. However, TUD HETUS and cpar24 assesses behaviours during a single day, indicating that more than one day of assessment is needed to get a representative estimate of individual’s movement behaviours [25], which present additional burden. Therefore, DABQ, JPHC-PAQ, and STAR-Q may be better choice for adult population, and 24HMBQ for a specific population of dormitory students. Those four self-reports also showed fair-to-good reliability coefficients, while quality ratings for their validation studies were fair-to-excellent. None of the studies included in our review reported responsiveness, and therefore, no recommendations for longitudinal or intervention studies could be made.
If the purpose is population surveillance, then low systematic error and high responsiveness to detect change in behaviour of a population are important characteristics [23, 24]. Low systematic error is important for accurate assessment of the proportion of population that have (un)healthy pattern of movement behaviours, while responsiveness is needed to follow population trends. In population health surveys, there is usually a limited space available for questions on movement behaviours, indicating that shorter questionnaires (JPHC-PAQ, PAQ, PAS 2, SIMPAQ) may be more appropriate for most surveys. However, PAS 2 and SIMPAQ showed poor validity (r < 0.21 for some estimates), while only reliability has been evaluated for PAQ. Therefore, JPHC-PAQ might be a preferred choice. Among shorter questionnaires, Bland-Altman plot has been reported only for PAS 2; physical activity estimates were systematically higher, while sum of sleep and SB systematically lower when compared with the reference measure [101]. As the reference measure was not a reasonable gold standard, those findings could not be interpreted as measurement errors. Future studies should carefully consider choosing a highly trusted reference measure and exploring systematic and random error. Also, responsiveness of such tools to detect trends in a population behaviour is yet to be explored.
In practice, assessment of 24-h movement behaviours is usually needed for individual level estimates. If the purpose is to assess whether individual meet recommended levels of 24-h movement behaviours, then important measurement properties are high sensitivity and specificity for such classification [118]. If the purpose is to assess change in individual’s behaviour, then responsiveness to detect change on an individual level needs to be high [24]. As clinicians are usually interested in clinically meaningful change, minimal detectable change (i.e., change that is beyond normal within-individual variability in behaviour and the measurement error and can be interpreted as real change for an individual [24]) should be lower than minimal important change (i.e., minimal within-individual change above which individuals/patients perceive themselves importantly changed [119]). However, none of the studies included in our review explored sensitivity and specificity neither responsiveness to detect change on an individual level. Two studies on test-retest reliability [96, 100] and four studies on construct validity [93, 94, 96, 101] reported substantially large random error (e.g., 95% limits of agreement for MVPA estimate ranged from − 109 to + 102 min/day [96]), indicating that minimal detectable change for these self-reports is likely to be too large to detect minimal important change. In clinical care settings, there is usually only a limited time available for counselling on movement behaviours, and it has been recommended that tool need to be quick to administer (up to three minutes), and to provide immediate feedback [21]. Therefore, only short questionnaires (JPHC-PAQ, PAQ, PAS 2, SIMPAQ) may be a potential candidate tool. As mentioned above, PAQ, PAS 2, and SIMPAQ could not be recommended due to poor or unknown construct validity.
Limitations
This review has some limitations that should be highlighted. First, the review was limited to studies that validated self-reported estimates of movement behaviours across the full 24-h day. This reduced the number of included studies, since studies that did not validate all components of the 24-h day were not included. According to the 24-h movement paradigm, movement behaviours are components of a finite total, and therefore, all components of the total need to be validated simultaneously. Therefore, self-reported tools evaluated in some excluded studies [64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83], need further validation of the whole 24-h time-use composition. Our review also did not include some important time-use tools used in the Multinational Time Use Study (MTUS) that harmonised over 100 national time-use surveys, and therefore, present a key resource for time-use research [120]. It might be that validation studies of most national time-use surveys are lacking. However, our review included TUD HETUS that showed high validity, and it might be that other similar time-use surveys have comparable validity. Second, literature search was conducted in only three databases, and therefore, we might miss some of the relevant studies. However, we used a comprehensive search query and conducted a secondary search, including citation searching, screening authors’ archive of references, and conducted a secondary database search on titles of identified self-reported tools. Third, most studies were conducted on convenience samples; therefore, findings might not be directly generalizable to the general population. As most tools were validated only in one language, future translation and cross-cultural validation studies might be needed for some self-reports.
Conclusions
This systematic review identified 12 validated self-reported tools for assessment of 24-h movement behaviours, indicating that only a limited number of tools are currently available. Validation studies generally showed adequate construct validity and test-retest reliability to be used in epidemiological studies and population surveillance, while little is known about adequacy for individual level assessments and responsiveness to behavioural change. To better support research, policy, and practice on 24-h movement behaviours, there is a need for further developments in measurement methods. There is a need to develop new tools for assessment of 24-h movement behaviours for specific purposes and/or to adapt the existing physical activity and SB self-reports in a way that they will resonate with the emerging 24-h movement paradigm. Future studies should examine measurement properties of 24-h movement behaviours estimates simultaneously and by using statistical methods that respect compositional nature of movement behaviours data.
Data availability
All data generated or analysed during this study are included in this published article and its supplementary information file.
Abbreviations
- 24HMBQ:
-
24-hour movement behaviors questionnaire
- 7D PAR:
-
7-Day Physical Activity Recall
- COSMIN:
-
Consensus-based Standards for the selection of health Measurement Instruments
- CPAR24:
-
Computer-Based 24-Hour Physical Activity Recall
- DABQ:
-
Daily Activity Behaviours Questionnaire
- JPHC-PAQ:
-
Japan Public Health Center-based prospective study- physical activity questionnaire
- LPA:
-
Light-intensity physical activity
- MARCA:
-
Multimedia Activity Recall for Children and Adults
- MVPA:
-
Moderate- to vigorous-intensity physical activity
- PAQ:
-
Physical activity questionnaire
- PAQ SCCS:
-
Physical Activity Questionnaire from the Southern Community Cohort Study
- PAS 2:
-
Physical Activity Scale 2
- PAS 2.1:
-
Physical Activity Scale 2.1
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PROSPERO:
-
International Prospective Register of Systematic Reviews
- SB:
-
Sedentary behaviour
- SIMPAQ:
-
Simple Physical Activity Questionnaire
- STAR-Q:
-
Sedentary Time and Activity Reporting Questionnaire
- TUD HETUS:
-
Time-use diary from the Harmonised European Time Use Study
References
Chaput J-P, Dutil C, Featherstone R, Ross R, Giangregorio L, Saunders TJ, et al. Sleep duration and health in adults: an overview of systematic reviews. Appl Physiol Nutr Metab. 2020;45(10):S218–31. https://doi.org/10.1139/apnm-2020-0034. (Suppl. 2)).
2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report. Washington, DC, USA; 2018.
Chastin SFM, De Craemer M, De Cocker K, Powell L, Van Cauwenberg J, Dall P, et al. How does light-intensity physical activity associate with adult cardiometabolic health and mortality? Systematic review with meta-analysis of experimental and observational studies. Br J Sports Med. 2019;53(6):370–6. https://doi.org/10.1136/bjsports-2017-097563.
Patterson R, McNamara E, Tainio M, de Sa TH, Smith AD, Sharp SJ, et al. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: a systematic review and dose response meta-analysis. Eur J Epidemiol. 2018;33(9):811–29. https://doi.org/10.1007/s10654-018-0380-1.
Saunders TJ, McIsaac T, Douillette K, Gaulton N, Hunter S, Rhodes RE, et al. Sedentary behaviour and health in adults: an overview of systematic reviews. Appl Physiol Nutr Metab. 2020;45(10):S197–217. https://doi.org/10.1139/apnm-2020-0272. (Suppl. 2)).
Matricciani L, Bin YS, Lallukka T, Kronholm E, Wake M, Paquet C, et al. Rethinking the sleep-health link. Sleep Health. 2018;4(4):339–48. https://doi.org/10.1016/j.sleh.2018.05.004.
Pedišić Ž, Dumuid D, Olds TS. Integrating sleep, sedentary behaviour, and physical activity research in the emerging field of time-use epidemiology: definitions, concepts, statistical methods, theoretical framework, and future directions. Kinesiology. 2017;49(2):252–69.
Migueles JH, Aadland E, Andersen LB, Brønd JC, Chastin SF, Hansen BH, et al. GRANADA consensus on analytical approaches to assess associations with accelerometer-determined physical behaviours (physical activity, sedentary behaviour and sleep) in epidemiological studies. Br J Sports Med. 2021;bjsports–2020–103604. https://doi.org/10.1136/bjsports-2020-103604.
Chastin SF, Palarea-Albaladejo J, Dontje ML, Skelton DA. Combined effects of Time spent in physical activity, sedentary behaviors and sleep on obesity and cardio-metabolic health markers: a Novel Compositional Data Analysis Approach. PLoS ONE. 2015;10(10):e0139984. https://doi.org/10.1371/journal.pone.0139984.
Pedišić Ž. Measurement issues and poor adjustments for physical activity and sleep undermine sedentary behaviour research - the focus should shift to the balance between sleep, sedentary behaviour, standing and activity. Kinesiology. 2014;46(1):135–46.
Dumuid D, Stanford TE, Martin-Fernández JA, Pedišić Ž, Maher CA, Lewis LK, et al. Compositional data analysis for physical activity, sedentary time and sleep research. Stat Methods Med Res. 2018;27(12):3726–38. https://doi.org/10.1177/0962280217710835.
Alfawaz RA, Aljuraiban GS, AlMarzooqi MA, Alghannam AF, BaHammam AS, Dobia AM, et al. The recommended amount of physical activity, sedentary behavior, and sleep duration for healthy saudis: a joint consensus statement of the Saudi Public Health Authority. Ann Thorac Med. 2021;16(3):239–44. https://doi.org/10.4103/atm.atm_33_21.
Draper CE, Tomaz SA, Biersteker L, Cook CJ, Couper J, de Milander M, et al. The South African 24-Hour Movement guidelines for Birth to 5 years: an integration of physical activity, sitting behavior, screen time, and Sleep. J Phys Act Health. 2020;17(1):109–19. https://doi.org/10.1123/jpah.2019-0187.
Tremblay MS, Carson V, Chaput JP, Connor Gorber S, Dinh T, Duggan M, et al. Canadian 24-Hour Movement Guidelines for Children and Youth: an integration of physical activity, sedentary Behaviour, and Sleep. Appl Physiol Nutr Metab. 2016;41(6 Suppl 3):S311–27. https://doi.org/10.1139/apnm-2016-0151.
Jurakić D, Pedišić Ž. Croatian 24-Hour guidelines for physical activity, sedentary Behaviour, and sleep: a proposal based on a systematic review of literature. Medicus. 2019;28(2):143.
UKK Institute for Health Promotion Research. Aikuisten liikkumisen suositus [Movement recommendations for adults]. Tampere: UKK Institute for Health Promotion Research. 2019. https://www.ukkinstituutti.fi/liikkumisensuositus/aikuisten-liikkumisen-suositus.
Okely AD, Ghersi D, Hesketh KD, Santos R, Loughran SP, Cliff DP, et al. A collaborative approach to adopting/adapting guidelines - the Australian 24-Hour Movement guidelines for the early years (birth to 5 years): an integration of physical activity, sedentary behavior, and sleep. BMC Public Health. 2017;17(5):869. https://doi.org/10.1186/s12889-017-4867-6.
Ross R, Chaput J-P, Giangregorio LM, Janssen I, Saunders TJ, Kho ME, et al. Canadian 24-Hour Movement guidelines for adults aged 18–64 years and adults aged 65 years or older: an integration of physical activity, sedentary behaviour, and sleep. Appl Physiol Nutr Metab. 2020;45(10):S57–102. https://doi.org/10.1139/apnm-2020-0467.
WHO. Guidelines on physical activity, sedentary Behaviour and Sleep for children under 5 years of age. World Health Organization; 2019.
Troiano RP, Stamatakis E, Bull FC. How can global physical activity surveillance adapt to evolving physical activity guidelines? Needs, challenges and future directions. Br J Sports Med. 2020;54(24):1468. https://doi.org/10.1136/bjsports-2020-102621.
Morgan TL, Faught E, Ross-White A, Fortier MS, Duggan M, Jain R, et al. Tools to guide clinical discussions on physical activity, sedentary behaviour, and/or sleep for health promotion between primary care providers and adults accessing care: a scoping review. BMC Prim Care. 2023;24(1):140. https://doi.org/10.1186/s12875-023-02091-9.
van Hees VT, Sabia S, Anderson KN, Denton SJ, Oliver J, Catt M, et al. A Novel, Open Access Method to Assess Sleep Duration using a wrist-worn accelerometer. PLoS ONE. 2015;10(11):e0142533. https://doi.org/10.1371/journal.pone.0142533.
Chastin SFM, Dontje ML, Skelton DA, Cukic I, Shaw RJ, Gill JMR, et al. Systematic comparative validation of self-report measures of sedentary time against an objective measure of postural sitting (activPAL). Int J Behav Nutr Phys Act. 2018;15(1):21. https://doi.org/10.1186/s12966-018-0652-x.
Dontje ML, Dall PM, Skelton DA, Gill JMR, Chastin SFM, on behalf of the Seniors USPT. Reliability, minimal detectable change and responsiveness to change: indicators to select the best method to measure sedentary behaviour in older adults in different study designs. PLoS ONE. 2018;13(4):e0195424. https://doi.org/10.1371/journal.pone.0195424.
Dowd KP, Szeklicki R, Minetto MA, Murphy MH, Polito A, Ghigo E, et al. A systematic literature review of reviews on techniques for physical activity measurement in adults: a DEDIPAC study. Int J Behav Nutr Phys Act. 2018;15(1):15. https://doi.org/10.1186/s12966-017-0636-2.
Pedišić Ž, Bauman A. Accelerometer-based measures in physical activity surveillance: current practices and issues. Br J Sports Med. 2015;49(4):219–23. https://doi.org/10.1136/bjsports-2013-093407.
Strath SJ, Kaminsky LA, Ainsworth BE, Ekelund U, Freedson PS, Gary RA, et al. Guide to the assessment of physical activity: clinical and research applications: a scientific statement from the American Heart Association. Circulation. 2013;128(20):2259–79. https://doi.org/10.1161/01.cir.0000435708.67487.da.
Shephard RJ, Aoyagi Y. Measurement of human energy expenditure, with particular reference to field studies: an historical perspective. Eur J Appl Physiol. 2012;112(8):2785–815. https://doi.org/10.1007/s00421-011-2268-6.
Bakker EA, Hartman YAW, Hopman MTE, Hopkins ND, Graves LEF, Dunstan DW, et al. Validity and reliability of subjective methods to assess sedentary behaviour in adults: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. 2020;17(1):75. https://doi.org/10.1186/s12966-020-00972-1.
Cespedes EM, Hu FB, Redline S, Rosner B, Alcantara C, Cai J, et al. Comparison of self-reported sleep duration with actigraphy: results from the Hispanic Community Health Study/Study of latinos Sueño Ancillary Study. Am J Epidemiol. 2016;183(6):561–73. https://doi.org/10.1093/aje/kwv251.
Chinapaw MJ, Mokkink LB, van Poppel MN, van Mechelen W, Terwee CB. Physical activity questionnaires for youth: a systematic review of measurement properties. Sports Med. 2010;40(7):539–63. https://doi.org/10.2165/11530770-000000000-00000.
Helmerhorst HHJF, Brage S, Warren J, Besson H, Ekelund U. A systematic review of reliability and objective criterion-related validity of physical activity questionnaires. Int J Behav Nutr Phys Act. 2012;9(1):103. https://doi.org/10.1186/1479-5868-9-103.
Lauderdale DS, Knutson KL, Yan LL, Liu K, Rathouz PJ. Self-reported and measured sleep duration: how similar are they? Epidemiology. 2008;19(6):838–45.
Prince SA, Cardilli L, Reed JL, Saunders TJ, Kite C, Douillette K, et al. A comparison of self-reported and device measured sedentary behaviour in adults: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. 2020;17(1):31. https://doi.org/10.1186/s12966-020-00938-3.
Silsbury Z, Goldsmith R, Rushton A. Systematic review of the measurement properties of self-report physical activity questionnaires in healthy adult populations. BMJ Open. 2015;5(9):e008430. https://doi.org/10.1136/bmjopen-2015-008430.
Tanaka R, Yakushiji K, Tanaka S, Tsubaki M, Fujita K. Reliability and validity of light-intensity physical activity scales in adults: a systematic review. MPEES. 2023;27(2):136–50. https://doi.org/10.1080/1091367X.2022.2120356.
van Poppel MN, Chinapaw MJ, Mokkink LB, van Mechelen W, Terwee CB. Physical activity questionnaires for adults: a systematic review of measurement properties. Sports Med. 2010;40(7):565–600. https://doi.org/10.2165/11531930-000000000-00000.
Rodrigues B, Encantado J, Carraça E, Sousa-Sá E, Lopes L, Cliff D, et al. Questionnaires measuring movement behaviours in adults and older adults: content description and measurement properties. A systematic review. PLoS ONE. 2022;17(3 March). https://doi.org/10.1371/journal.pone.0265100.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71.
Terwee CB, Mokkink LB, van Poppel MN, Chinapaw MJ, van Mechelen W, de Vet HC. Qualitative attributes and measurement properties of physical activity questionnaires: a checklist. Sports Med. 2010;40(7):525–37. https://doi.org/10.2165/11531370-000000000-00000.
Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, et al. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: an international Delphi study. Qual Life Res. 2010;19(4):539–49. https://doi.org/10.1007/s11136-010-9606-8.
Terwee CB, Mokkink LB, Knol DL, Ostelo RW, Bouter LM, de Vet HC. Rating the methodological quality in systematic reviews of studies on measurement properties: a scoring system for the COSMIN checklist. Qual Life Res. 2012;21(4):651–7. https://doi.org/10.1007/s11136-011-9960-1.
Bull FC, Maslin TS, Armstrong T. Global physical activity questionnaire (GPAQ): nine country reliability and validity study. J Phys Act Health. 2009;6(6):790–804. https://doi.org/10.1123/jpah.6.6.790.
Koo TK, Li MY. A Guideline of selecting and reporting Intraclass correlation coefficients for Reliability Research. J Chiropr Med. 2016;15(2):155–63. https://doi.org/10.1016/j.jcm.2016.02.012.
Armbrust W, Joyce Bos GJF, Geertzen JHB, Sauer PJJ, Dijkstra PU, Lelieveld OTHM. Measuring physical activity in juvenile idiopathic arthritis: activity diary versus accelerometer. J Rheumatol. 2017;44(8):1249–56. https://doi.org/10.3899/jrheum.160671.
Rodriguez G, Béghin L, Michaud L, Moreno LA, Turck D, Gottrand F. Comparison of the TriTrac-R3D accelerometer and a self-report activity diary with heart-rate monitoring for the assessment of energy expenditure in children. Br J Nutr. 2002;87(6):623–31. https://doi.org/10.1079/BJNBJN2002571.
Aggio D, Fairclough S, Knowles Z, Graves L. Validity and reliability of a modified English version of the physical activity questionnaire for adolescents. Archives Public Health. 2016;74(1). https://doi.org/10.1186/s13690-016-0115-2.
Alkhraiji MH, Barker AR, Williams CA. Reliability and validity of using the global school-based student health survey to assess 24 hour movement behaviours in adolescents from Saudi Arabia. J Sports Sci. 2022;40(14):1578–86. https://doi.org/10.1080/02640414.2022.2092982.
Anastasiou CA, Fappa E, Zachari K, Mavrogianni C, Van Stappen V, Kivelä J, et al. Development and reliability of questionnaires for the assessment of diet and physical activity behaviors in a multi-country sample in Europe the Feel4Diabetes study. BMC Endocr Disord. 2020;20(Suppl 1):135. https://doi.org/10.1186/s12902-019-0469-x.
Chasan-Taber L, Schmidt MD, Roberts DE, Hosmer D, Markenson G, Freedson P. Development and validation of a pregnancy physical activity questionnaire. Med Sci Sports Exerc. 2004;36(10):1750–60.
Gabriel KP, Sidney S, Jacobs DR Jr, Quesenberry CP Jr, Reis JP, Sheng-Fang J, et al. Convergent validity of a brief self-reported physical activity questionnaire. Med Sci Sports Exerc. 2014;46(8):1570–7.
Hillier FC, Batterham AM, Crooks S, Moore HJ, Summerbell CD. The development and evaluation of a novel internet-based computer program to assess previous-day dietary and physical activity behaviours in adults: the Synchronised Nutrition and Activity Program for adults (SNAPA™). Br J Nutr. 2012;107(8):1221–31. https://doi.org/10.1017/s0007114511004090.
Innerd P, Catt M, Collerton J, Davies K, Trenell M, Kirkwood TBL, et al. A comparison of subjective and objective measures of physical activity from the Newcastle 85 + study. Age Ageing. 2015;44(4):691–4. https://doi.org/10.1093/ageing/afv062.
Liu Y, Wang M, Tynjälä J, Lv Y, Villberg J, Zhang Z, et al. Test-retest reliability of selected items of health behaviour in school-aged children (HBSC) survey questionnaire in Beijing, China. BMC Med Res Methodol. 2010;10. https://doi.org/10.1186/1471-2288-10-73.
Mackay LM, Schofield GM, Schluter PJ. Validation of self-report measures of physical activity: a case study using the New Zealand physical activity questionnaire. Res Q Exerc Sport. 2007;78(3):189–96. https://doi.org/10.1080/02701367.2007.10599416.
Moore HJ, Ells LJ, McLure SA, Crooks S, Cumbor D, Summerbell CD, et al. The development and evaluation of a novel computer program to assess previous-day dietary and physical activity behaviours in school children: the Synchronised Nutrition and Activity Program (SNAP). Br J Nutr. 2008;99(6):1266–74. https://doi.org/10.1017/s0007114507862428.
Norman A, Bellocco R, Bergström A, Wolk A. Validity and reproducibility of self-reported total physical activity–differences by relative weight. Int J Obes Relat Metab Disord. 2001;25(5):682–8. https://doi.org/10.1038/sj.ijo.0801597.
Potchana K, Saengsuwan J, Kittipanya-ngam P. Validity and test-retest reliability of a Thai Stroke Physical Activity Questionnaire. J Stroke Cerebrovasc Dis. 2021;30(8). https://doi.org/10.1016/j.jstrokecerebrovasdis.2021.105907.
Rimmer JH, Riley BB, Rubin SS. A new measure for assessing the physical activity behaviors of persons with disabilities and chronic health conditions: the physical activity and disability survey. Am J Health Promot. 2001;16(1):34–42. https://doi.org/10.4278/0890-1171-16.1.34.
Saint-Maurice PF, Welk GJ. Web-based assessments of physical activity in youth: considerations for design and scale calibration. J Med Internet Res. 2014;16(12). https://doi.org/10.2196/jmir.3626.
Scheers T, Philippaerts R, Lefevre J. Assessment of physical activity and inactivity in multiple domains of daily life: a comparison between a computerized questionnaire and the SenseWear Armband complemented with an electronic diary. Int J Behav Nutr Phys Activity. 2012;9. https://doi.org/10.1186/1479-5868-9-71.
Song Y, Yoon YJ, Lee HJ, Kim YS, Spence JC, Jeon JY. Development of a 24-Hour Movement Behavior Questionnaire for Youth: process and reliability testing. J Nutr Educ Behav. 2021;53(12):1081–9. https://doi.org/10.1016/j.jneb.2021.08.012.
Treuth MS, Sherwood NE, Butte NF, McClanahan B, Obarzanek E, Zhou A, et al. Validity and reliability of activity measures in African-American girls for GEMS. Med Sci Sports Exerc. 2003;35(3):532–9. https://doi.org/10.1249/01.MSS.0000053702.03884.3F.
Aadahl M, Jorgensen T. Validation of a new self-report instrument for measuring physical activity. Med Sci Sports Exerc. 2003;35(7):1196–202.
Bruening M, Van Woerden I, Todd M, Brennhofer S, Laska MN, Dunton G. A mobile ecological momentary assessment tool (devilSPARC) for nutrition and physical activity behaviors in college students: a validation study. J Med Internet Res. 2016;18(7). https://doi.org/10.2196/jmir.5969.
Calabro MA, Welk GJ, Carriquiry AL, Nusser SM, Beyler NK, Matthews CE. Validation of a computerized 24-hour physical activity recall (24PAR) instrument with pattern-recognition activity monitors. J Phys Activity Health. 2009;6(2):211–20. https://doi.org/10.1123/jpah.6.2.211.
Gilbert AL, Lee J, Ma M, Semanik PA, DiPietro L, Dunlop DD, et al. Comparison of subjective and objective measures of sedentary behavior using the Yale Physical Activity Survey and Accelerometry in patients with rheumatoid arthritis. J Phys Act Health. 2016;13(4):371–6. https://doi.org/10.1123/jpah.2015-0176.
Inácio Osti RF, Totaro Garcia LM, Florindo AA. Validation of the 24-hour physical activity recall in elderly adults. / Validação do recordatório de 24 horas para avaliação da atividade física em idosos. Brazilian J Kineanthropometry Hum Perform. 2014;16(1):15–26.
Keadle SK, Patel S, Berrigan D, Christopher CN, Huang J, Saint-Maurice PF, et al. Validation of ACT24 Version 2.0 for estimating behavioral domains, active and sedentary time. Med Sci Sports Exerc. 2023;55(6):1054–62. https://doi.org/10.1249/MSS.0000000000003135.
Kim Y, Welk GJ. The accuracy of the 24-h activity recall method for assessing sedentary behaviour: the physical activity measurement survey (PAMS) project. J Sports Sci. 2017;35(3):255–61. https://doi.org/10.1080/02640414.2016.1161218.
Mace CJ, Maddison R, Olds T, Kerse N. Validation of a computerized use of time recall for activity measurement in advanced-aged adults. J Aging Phys Act. 2014;22(2):245–54. https://doi.org/10.1123/japa.2012-0280.
Matthews CE, Ainsworth BE, Hanby C, Pate RR, Addy C, Freedson PS, et al. Development and testing of a short physical activity recall questionnaire. Med Sci Sports Exerc. 2005;37(6):986–94. https://doi.org/10.1249/01.mss.0000171615.76521.69.
Ridley K, Olds TS, Hill A. The Multimedia activity recall for children and adolescents (MARCA): development and evaluation. Int J Behav Nutr Phys Activity. 2006;3. https://doi.org/10.1186/1479-5868-3-10.
Trost SG, Marshall AL, Miller R, Hurley JT, Hunt JA. Validation of a 24-h physical activity recall in indigenous and non-indigenous Australian adolescents. J Sci Med Sport. 2007;10(6):428–35. https://doi.org/10.1016/j.jsams.2006.07.018.
Welk GJ, Youngwon KIM, Stanfill B, Osthus DA, Calabro MA, Nusser SM, et al. Validity of 24-h Physical Activity Recall: physical activity measurement survey. Med Sci Sports Exerc. 2014;46(10):2014–24.
Andersen LG, Groenvold M, Jørgensen T, Aadahl M. Construct validity of a revised physical activity scale and testing by cognitive interviewing. Scand J Public Health. 2010;38(7):707–14. https://doi.org/10.1177/1403494810380099.
Bharathi AV, Kuriyan R, Kurpad AV, Thomas T, Ebrahim S, Kinra S, et al. Assessment of physical activity using accelerometry, an activity diary, the heart rate method and the Indian migration study questionnaire in south Indian adults. Public Health Nutr. 2010;13(1):47–53. https://doi.org/10.1017/s1368980009005850.
Elliott SA, Baxter KA, Davies PSW, Truby H. Accuracy of self-reported physical activity levels in obese adolescents. J Nutr Metab. 2014;2014. https://doi.org/10.1155/2014/808659.
Leicht A. Validation of a one-day self-report questionnaire for physical activity assessment in healthy adults. Eur J Sport Sci. 2008;8(6):389–96. https://doi.org/10.1080/17461390802368994.
Matthews CE, Freedson PS. Field trial of a three-dimensional activity monitor: comparison with self report. Med Sci Sports Exerc. 1995;27(7):1071–8. https://doi.org/10.1249/00005768-199507000-00017.
Namba H, Yamaguchi Y, Yamada Y, Tokushima S, Hatamoto Y, Sagayama H, et al. Validation of web-based physical activity measurement systems using doubly labeled water. J Med Internet Res. 2012;14(5):e123. https://doi.org/10.2196/jmir.2253.
Saraiva Leão Borges LP, Ries DC, Sousa AG, da Costa THM. Comparison and calibration of 24-hour physical activity recall in adult population. Eur J Sport Sci. 2022;22(2):289–96. https://doi.org/10.1080/17461391.2020.1866077.
Keadle SK, Kravitz ES, Matthews CE, Tseng M, Carroll RJ. Development and testing of an Integrated score for physical behaviors. Med Sci Sports Exerc. 2019;51(8):1759–66. https://doi.org/10.1249/mss.0000000000001955.
Gershuny J, Harms T, Doherty A, Thomas E, Milton K, Kelly P, et al. Testing Self-Report Time-Use diaries against Objective instruments in Real Time. Sociol Methodol. 2020;50(1):318–49. https://doi.org/10.1177/0081175019884591.
Falck RS, Davis JC, Khan KM, Handy TC, Liu-Ambrose T. A wrinkle in Measuring Time Use for Cognitive Health: how should we measure physical activity, sedentary Behaviour and Sleep? Am J Lifestyle Med. 2023;17(2):258–75. https://doi.org/10.1177/15598276211031495.
Foley L, Maddison R, Olds T, Ridley K. Self-report use-of-time tools for the assessment of physical activity and sedentary behaviour in young people: systematic review. Obes Rev. 2012;13(8):711–22. https://doi.org/10.1111/j.1467-789X.2012.00993.x.
Hunt T, Madigan S, Williams MT, Olds TS. Use of time in people with chronic obstructive pulmonary disease–a systematic review. Int J Chron Obstruct Pulmon Dis. 2014;9:1377–88. https://doi.org/10.2147/copd.S74298.
Rodrigues B, Encantado J, Carraça E, Martins J, Marques A, Lopes L, et al. Questionnaires measuring 24-Hour Movement behaviors in Childhood and Adolescence: content description and Measurement Properties—A systematic review. J Phys Activity Health. 2023;20(1):50–76. https://doi.org/10.1123/jpah.2022-0399.
White L, Volfson Z, Faulkner G, Arbour-Nicitopoulos K. Reliability and validity of physical activity instruments used in children and youth with physical disabilities: a systematic review. Pediatr Exerc Sci. 2016;28(2):240–63. https://doi.org/10.1123/pes.2015-0123.
Buchowski MS, Matthews CE, Cohen SS, Signorello LB, Fowke JH, Hargreaves MK, et al. Evaluation of a questionnaire to assess sedentary and active behaviors in the Southern Community Cohort Study. J Phys Act Health. 2012;9(6):765–75. https://doi.org/10.1123/jpah.9.6.765.
Csizmadi I, Neilson HK, Kopciuk KA, Khandwala F, Liu A, Friedenreich CM, et al. The sedentary time and activity reporting questionnaire (STAR-Q): reliability and validity against doubly labeled water and 7-day activity diaries. Am J Epidemiol. 2014;180(4):424–35. https://doi.org/10.1093/aje/kwu150.
Harms T, Gershuny J, Doherty A, Thomas E, Milton K, Foster C. A validation study of the Eurostat harmonised European time use study (HETUS) diary using wearable technology. BMC Public Health. 2019;19. https://doi.org/10.1186/s12889-019-6761-x.
Kastelic K, Löfler S, Matko Š, Šarabon N. Validity of the German version of Daily Activity Behaviours Questionnaire among older adults. J Aging Phys Act 2023:1–7. https://doi.org/10.1123/japa.2022-0417.
Kastelic K, Šarabon N, Burnard MD, Pedišić Ž. Validity and reliability of the Daily Activity Behaviours Questionnaire (DABQ) for Assessment of Time Spent in Sleep, sedentary Behaviour, and physical activity. Int J Environ Res Public Health. 2022;19(9). https://doi.org/10.3390/ijerph19095362.
Kikuchi H, Inoue S, Odagiri Y, Ihira H, Inoue M, Sawada N, et al. Intensity-specific validity and reliability of the Japan Public Health Center-based prospective study-physical activity questionnaire. Prev Med Rep. 2020;20. https://doi.org/10.1016/j.pmedr.2020.101169.
Kohler S, Behrens G, Olden M, Baumeister SE, Horsch A, Fischer B, et al. Design and evaluation of a computer-based 24-Hour Physical Activity Recall (cpar24) instrument. J Med Internet Res. 2017;19(5):e186. https://doi.org/10.2196/jmir.7620.
Welk GJ, Thompson RW, Galper DI. A temporal validation of Scoring algorithms for the 7-Day Physical Activity Recall. MPEES. 2001;5(3):123–38.
Zheng J, Tan TC, Zheng K, Huang T. Development of a 24-hour movement behaviors questionnaire (24HMBQ) for Chinese college students: validity and reliability testing. BMC Public Health. 2023;23(1):752. https://doi.org/10.1186/s12889-023-15393-5.
Bharathi AV, Sandhya N, Vaz M. The development & characteristics of a physical activity questionnaire for epidemiological studies in urban middle class indians. Indian J Med Res. 2000;111:95–102.
Hunt T, Williams MT, Olds TS. Reliability and validity of the Multimedia Activity recall in children and adults (MARCA) in people with chronic obstructive Pulmonary Disease. PLoS ONE. 2013;8(11):e81274. https://doi.org/10.1371/journal.pone.0081274.
Pedersen ESL, Mortensen LH, Brage S, Bjerregaard AL, Aadahl M. Criterion validity of the physical activity scale (PAS2) in Danish adults. Scand J Public Health. 2018;46(7):726–34. https://doi.org/10.1177/1403494817738470.
Rosenbaum S, Morell R, Abdel-Baki A, Ahmadpanah M, Baie L, Bauman A, et al. Assessing physical activity in people with mental illness: 23-country reliability and validity of the simple physical activity questionnaire (SIMPAQ). BMC Psychiatry. 2020. https://doi.org/10.21203/rs.2.12937/v2.
Schilling R, Schärli E, Fischer X, Donath L, Faude O, Brand S, et al. The utility of two interview-based physical activity questionnaires in healthy young adults: comparison with accelerometer data. PLoS ONE. 2018;13(9):e0203525. https://doi.org/10.1371/journal.pone.0203525.
Valles-Medina AM, Castillo-Anaya SI, Sevilla-Mena TL, Aadahl M. Validity of the Danish physical activity scale, adapted to Spanish speaking population. Aten Primaria. 2021;53(5):101949. https://doi.org/10.1016/j.aprim.2020.09.008.
Vancampfort D, Basangwa D, Rosenbaum S, Ward PB, Mugisha J. Test-retest reliability and correlates of the simple physical activity questionnaire in Ugandan out-patients with psychosis. Afr Health Sci. 2020;20(3):1438–45. https://doi.org/10.4314/ahs.v20i3.49.
van der Ploeg HP, Merom D, Chau JY, Bittman M, Trost SG, Bauman AE. Advances in Population Surveillance for physical activity and sedentary behavior: reliability and validity of time use surveys. Am J Epidemiol. 2010;172(10):1199–206. https://doi.org/10.1093/aje/kwq265.
Sattler MC, Jaunig J, Tösch C, Watson ED, Mokkink LB, Dietz P, et al. Current evidence of Measurement Properties of Physical Activity questionnaires for older adults: an updated systematic review. Sports Med. 2020;50(7):1271–315. https://doi.org/10.1007/s40279-020-01268-x.
Clevenger KA, Montoye AHK. Systematic review of Accelerometer Responsiveness to change for measuring physical activity, sedentary behavior, or Sleep. J Meas Phys Behav 2023:1–14. https://doi.org/10.1123/jmpb.2023-0025.
Giurgiu M, Ketelhut S, Kubica C, Nissen R, Doster A-K, Thron M, et al. Assessment of 24-hour physical behaviour in adults via wearables: a systematic review of validation studies under laboratory conditions. Int J Behav Nutr Phys Act. 2023;20(1):68. https://doi.org/10.1186/s12966-023-01473-7.
Hartson KR, Huntington-Moskos L, Sears CG, Genova G, Mathis C, Ford W, et al. Use of Electronic Ecological Momentary Assessment methodologies in physical activity, sedentary behavior, and Sleep Research in Young adults: systematic review. J Med Internet Res. 2023;25:e46783. https://doi.org/10.2196/46783.
Rosenberger ME, Buman MP, Haskell WL, McConnell MV, Carstensen LL. Twenty-four hours of Sleep, Sedentary Behavior, and physical activity with nine Wearable devices. Med Sci Sports Exerc. 2016;48(3):457–65. https://doi.org/10.1249/mss.0000000000000778.
Migueles JH, Cadenas-Sanchez C, Ekelund U, Delisle Nyström C, Mora-Gonzalez J, Löf M, et al. Accelerometer Data Collection and Processing Criteria to assess physical activity and other outcomes: a systematic review and practical considerations. Sports Med. 2017;47(9):1821–45. https://doi.org/10.1007/s40279-017-0716-0.
Kang M, Rowe DA. Issues and Challenges in Sedentary Behavior Measurement. MPEES 2015;19(3):105 – 15. https://doi.org/10.1080/1091367X.2015.1055566.
Sadeh A. The role and validity of actigraphy in sleep medicine: an update. Sleep Med Rev. 2011;15(4):259–67. https://doi.org/10.1016/j.smrv.2010.10.001.
Husu P, Tokola K, Vähä-Ypyä H, Sievänen H, Suni J, Heinonen OJ, et al. Physical activity, sedentary behavior, and Time in Bed among Finnish adults measured 24/7 by Triaxial Accelerometry. J Meas Phys Behav. 2021;4(2):163–73. https://doi.org/10.1123/jmpb.2020-0056.
Stevens ML, Gupta N, Inan Eroglu E, Crowley PJ, Eroglu B, Bauman A, et al. Thigh-worn accelerometry for measuring movement and posture across the 24-hour cycle: a scoping review and expert statement. BMJ Open Sport Exerc Med. 2020;6(1):e000874. https://doi.org/10.1136/bmjsem-2020-000874.
Gupta N, Mathiassen SE, Mateu-Figueras G, Heiden M, Hallman DM, Jorgensen MB, et al. A comparison of standard and compositional data analysis in studies addressing group differences in sedentary behavior and physical activity. Int J Behav Nutr Phys Act. 2018;15(1):53. https://doi.org/10.1186/s12966-018-0685-1.
Kelly P, Fitzsimons C, Baker G. Should we reframe how we think about physical activity and sedentary behaviour measurement? Validity and reliability reconsidered. Int J Behav Nutr Phys Activity. 2016;13(1):32. https://doi.org/10.1186/s12966-016-0351-4.
Terwee CB, Peipert JD, Chapman R, Lai J-S, Terluin B, Cella D, et al. Minimal important change (MIC): a conceptual clarification and systematic review of MIC estimates of PROMIS measures. Qual Life Res. 2021;30(10):2729–54. https://doi.org/10.1007/s11136-021-02925-y.
Centre for Time Use Research. Multinational Time Use Study, Social Research Institute at the University College London (UCL): Centre for Time Use Research. 2024 [ https://www.timeuse.org/mtus.]
Acknowledgements
The authors gratefully acknowledge the Slovenian Research and Innovation Agency and Ministry of Health from Republic of Slovenia for funding the project Implementing the concept of 24-hour movement behaviours as a determinant of health into the Slovenian environment (GIB24) (Project Number V3-2305). The authors also acknowledge the Slovenian Research Agency for funding the infrastructure group at the University of Primorska (research core funding No. IO-0035). NŠ research activities on this project was partially financially supported by the Slovenian Research and Innovation Agency through the research program KINSPO - Kinesiology for the effectiveness and prevention of musculoskeletal injuries in sports (P5-0443).
Funding
This study was partly funded by Slovenian Research and Innovation Agency and Ministry of Health from Republic of Slovenia. The funders had no influence on study protocol, analysis, and interpretation of data, and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
KK conceptualized the study and developed a search query. AŠ, LE, and KK screened hits for eligibility, reviewed full texts, extracted data, and conducted quality assessment. NŠ contributed as a consultant in systematic review process. AŠ and KK prepared figures and tables. AŠ drafted the manuscript. KK redrafted parts of the manuscript and contributed to the interpretation of findings. All authors reviewed all versions of the manuscript and contributed intellectually to its content.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
No ethics approval was needed for this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Šuc, A., Einfalt, L., Šarabon, N. et al. Validity and reliability of self-reported methods for assessment of 24-h movement behaviours: a systematic review. Int J Behav Nutr Phys Act 21, 83 (2024). https://doi.org/10.1186/s12966-024-01632-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-024-01632-4