
Abstract
Background
Physical activity is widely promoted to maintain and improve health across all ages. Investigating how physical activity affects subsequent food intake provides insight into the factors that contribute to maintaining energy balance and effective weight management.
Objective
This systematic review and meta-analysis summarizes the evidence on the effect of acute physical activity on subsequent food intake in children and adolescents.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA) were applied. Randomized controlled trials (RCTs) objectively measuring post-exercise energy intake in children and adolescents aged 5 to 18 years were included. Studies with self-reported food intake were excluded. The databases PubMed, Web of Science and Cochrane Library were searched for RCTs, and the data were summarized at a qualitative and quantitative level. Version 2 of the Cochrane risk-of-bias tool for randomized trials was used to assess risk of bias. Changes in energy intake were examined with random effects meta-analysis. (PROSPERO: CRD42022324259).
Results
Out of 9582 studies, 22 RCTs with cross-over design remained eligible for meta-analysis. The primary outcome was post-intervention energy intake up to the next 24 h. Heterogeneity of studies was moderate, with an I2 of 57%. The median (interquartile range, IQR) energy expended while exercising was 240 (158) kcal. Meta-analysis of 41 study arms (exercise n = 780 and control n = 478) showed no differences in total energy intake between the exercise and control group with a mean difference MD = 23.31 [-27.54, 74.15] kcal. No subgroup differences were found. Macronutrient intake and appetite sensations where not substantially affected.
Conclusion
Engaging in exercise is a suitable means of raising activity-induced energy expenditure, without causing any noticeable changes in food intake or hunger within a single day.
Similar content being viewed by others


Introduction
Energy balance is regulated by a complex interplay between energy intake and energy expenditure [1, 2]. When the balance tilts in favor of energy intake, it leads to obesity, a significant public health concern from both personal and socio-economic perspectives [3]. Although rising trends in child and adolescent body mass index (BMI) have plateaued at high levels in many high-income countries, they have accelerated in parts of Asia [4]. This trend is attributed to a combination of factors such as decreased physical activity, increased sedentary behavior [5] and the overconsumption of high-energy-dense foods and large food portions [6, 7]. Decades of research have provided a comprehensive understanding of the factors influencing energy balance [8,9,10,11], resulting in similar recommendations for daily physical activity and a healthy diet globally [12,13,14]. However, adherence to these recommendations is challenging, as evidenced by alarming obesity rates [15]. Many research questions remain, particularly concerning body weight maintenance [16, 17]. Hence, ongoing research aims to comprehend the complex interplay of factors contributing to energy balance to offer holistic recommendations to society and patients while identifying targets for medication and interventions.
Food intake is influenced by environmental, psychological, and physiological factors [18]. The primary physiological driver of food intake is the resting metabolic rate (RMR), with fat-free mass being its largest contributor [19, 20]. RMR constitutes the largest component of daily energy expenditure and remains relatively stable throughout the day, generating a constant energetic demand [21, 22]. In contrast, acute exercise creates a short-term high energy requirement and induces various physiological effects as a result of increased sympathetic activity [23, 24].
Due to the distinct nature of these predictors of food intake, they are expected to have different mechanistic effects on appetite control, as summarized by Blundell et al. [25]. While RMR is relatively stable and cannot be acutely altered, physical activity can significantly increase energy expenditure through muscle activity [26, 27]. Activity energy expenditure is a crucial determinant of energy intake [28, 29]. Thus, exercise can facilitate weight loss by boosting energy expenditure, although this effect can be counteracted by subsequent sedentary behavior and increased food intake [30].
Structured exercise programs for adults with obesity have shown varying outcomes regarding body weight changes, ranging from weight loss to weight gain [31, 32]. This variability indicates that the determinants of sedentary behavior and post-exercise food intake are not yet fully understood. Physical activity may stimulate appetite to compensate for burned energy, but it can also lead to decreased appetite and increased sensitivity to satiety signals [33,34,35].
While the acute (up to 24 h) and short-term (up to 14 days) effects of physical activity on food intake in adults have been extensively studied [36,37,38,39,40,41,42], data for children and adolescents are limited [43]. The most recent systematic review on this topic was conducted in 2016 by Thivel et al. [44], concluding that acute exercise did not affect energy intake in lean individuals but appeared to reduce food intake in youth with obesity when exercise intensity was high. Since then, further high-quality trials have been published, allowing for a more robust analysis of data with stricter inclusion criteria, which is the focus of this review.
The aim of this review was to analyze the effects of acute exercise on energy intake under controlled conditions in children and adolescents. The main research questions were: i) whether acute exercise leads to increased food intake under controlled conditions; ii) whether these findings depend on the intensity, duration, and type of exercise; and iii) whether these findings are independent of body weight status. Understanding these fundamental aspects under controlled conditions is crucial for advancing basic knowledge within the broader context of energy balance regulation, contributing to the development of tailored public health strategies.
Materials and Methods
Literature information sources and search strategy
This review was developed and executed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [45]. To identify all relevant studies examining the effect of physical activity on caloric and macronutrient intake in children and adolescents across all weight categories, the databases PubMed, Web of Science and Cochrane Library were searched on November 16th and November 20th, 2021. The protocol of this systematic review is registered at the PROSPERO platform with the registration number CRD42022324259. The full search strategy is documented in the Supporting Information Text S1 and consisted of four modules in the search term: children and adolescents, physical activity, energy intake and macronutrient intake.
Eligibility Criteria
Eligibility criteria were based on the five PICOS dimensions, i.e., participants (P), interventions (I), comparators (C), outcome (O) and study design (S) [46]. Only peer-reviewed original studies written in English or German were included.
Participants: Participants included healthy, non-smoking children and adolescents aged on average ≥ 5 year to ≤ 18 years old, without any restrictions on sex, ethnicity, and weight status.
Interventions: Physical exercise intervention had to be conducted under guidance and supervised conditions without restrictions regarding intensity, duration, and modality. Recording of vital signs was not a prerequisite. The exercise intervention had to be followed by at least one post-exercise ad libitum meal under controlled conditions, such as a laboratory or researcher-controlled setting without restrictions regarding the characteristics of the meal conditions (e.g., ad libitum buffets, ad libitum single or multiple meals). Trials that additionally implemented dietary interventions or nutritional education were excluded.
Comparators: A comparison to controls was required, either between or within subjects.
Outcomes: The primary outcome was energy intake in kcal resulting from the corresponding food intake after the exercise intervention. Therefore, food intake in grams had to be measured by a calibrated scale and the foods’ caloric value had to be derived from validated sources, either bomb calorimetry or internationally known food databases. Data from food frequency questionnaires, 24-h recalls, or similar sources were excluded. Secondary outcomes were food intake (in grams) and macronutrient intake (in grams and as % energy intake) along with the appetite sensations hunger, satiety, and prospective food consumption (i.e. how much food participants thought they could eat).
Study designs: The systematic data analysis referred exclusively to randomized controlled trials as parallel and crossover designs.
Study selection, data collection and organisation
To identify eligible studies, the search results of the databases were combined, and the duplicates removed. Next, the titles and abstracts were screened. Full-text articles were evaluated regarding their eligibility (HH and IM), with uncertainties being discussed between the authors (< 15%). In the case of discrepancies, a third author was involved (MF).
Data items and statistics
The following information was extracted from each included article: year of publication, country of origin, study type, type of intervention, method for data collection, study outcomes including caloric intake, macronutrient intake and appetite sensations, and sample characteristics (including sample size, BMI, sex, and age).
Characteristics across studies are presented as absolute values for sample size, sex and exercise duration, as mean and standard deviation (SD) or per cent (%) for macronutrient intake and exercise intensity and as mean and SD or standard error (SE) for sample size, age, BMI, energy expenditure and energy intake. All energy intake and energy expenditure values were converted to kilocalories (kcal).
Exercise intensity was determined to be either low, moderate, or high, based on percentages of maximum oxygen consumption (VO2max) or maximum heart rate (HRmax) [47, 48]. Intensity was low if average heart rate was < 64% of HRmax or if VO2max was < 50%. Intensity was moderate if average heart rate was ≥ 64%—≤ 76% of HRmax, or if VO2max was ≥ 50%—< 70%, or if exercise was performed at ventilation threshold. Intensity was high if average heart rate was ≥ 77% of HRmax or if VO2max was ≥ 70%. In studies in which neither heart rate nor VO2 max was measured, the classification into low, moderate, and high was adopted according to the classification given in the trials.
For the energy intake (kcal), the results of all 22 trials were evaluated quantitatively (meta-analysis) and qualitatively. Qualitative analysis was also carried out to describe the direction of change in energy intake (whether participants ate more, the same or less) between exercise and control groups. In the case of missing data, the provided graphs were measured with the help of a software tool (Digitizeit [49] and WebPlotDigitizer [50]) to obtain the values needed. For the meta-analysis of cross-over trials, the mean difference (MD) and standard error (SE) were calculated according to the Cochrane Handbook for Systematic Reviews of Interventions [51]. If the studies did not provide sufficient data from a paired analysis, a correlation coefficient of 0.5 was set. This approach is consistent with that of another meta-analysis of exercise interventions [52], and is described in detail by Elbourne et al. [53]. Sensitivity analyses were performed for correlation coefficients of 0.3 and 0.7. The results were then entered into a generic inverse variance approach with the random-effects model using the software package Review Manager, version 5.4 [54]. In studies with multiple intervention arms the sample size of the shared group was split according to the Cochrane Handbook [51] and Rücker et al. [55] to avoid “double-counting” of participants (unit-of-analysis error). For the meta-analysis, 41 study arms were eligible. The difference in energy intake in kcal is presented as mean difference (MD), 95% confidence interval (CI) and standard error (SE) and is displayed in forest plots.
Statistical heterogeneity was examined by visual inspection of forest plots and using the I2 statistics to quantify inconsistency between the studies. Values < 25% were interpreted as low, 25%—75% as moderate and values > 75% were interpreted as high [56]. To reduce heterogeneity, subgroup analyses were performed for intensity of physical activity, age, risk of bias and weight status.
Data on the appetite sensations hunger, satiety, and prospective food consumption was evaluated qualitatively because different assessment tools were used, and many studies did not report data but only stated that either differences or no differences were found between the groups. Authors were contacted in case of missing data up to three times and 33% (2 out of 6) responded to the inquiry.
Risk of Bias
For all eligible studies, a risk of bias assessment was conducted using the Cochrane Risk-of-Bias tool for randomized crossover trials (RoB 2) [57]. The tool consists of 5 domains addressing different types of bias: randomization process, deviations from the intended interventions, missing outcome data, measurement of the outcome and selection of the reported result. In each domain, appropriate questions must be answered for each single study. Next, the RoB 2 algorithm is applied which evaluates the risks of the individual domains. Finally, an overall risk is calculated and expressed as “low” or “high” risk of bias, or the judgment can be expressed with “some concerns”.
Results
Study selection and categorization
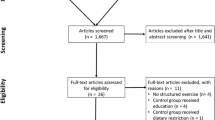
The literature search process used to identify eligible studies is shown in Fig. 1. Out of 9582 identified studies, 22 studies remained for analysis.

PRISMA flow chart for study inclusion
Summary of study characteristics
A detailed overview of the characteristics of the individual trials is presented in Table 1. The characteristics across the studies are given below.
The studies were published between 2009 and 2020. Most studies were conducted in Europe (n = 17; 67%) [60, 62,63,64,65,66,67,68, 71,72,73,74,75,76,77,78,79] followed by Canada and USA (both n = 2; 13%) [58, 59, 61, 70]. In general, a frequently implemented design in the included trials was the following: after a preliminary visit where baseline characteristics where collected, participants then visited a controlled environment for one to five intervention days, where data for primary and secondary outcomes where measured.
The studies differed in the number of post-exercise test meals. Thirteen studies examined two post-intervention meals, usually lunch and dinner [61, 63,64,65, 67, 70,71,72, 75,76,77,78, 80]. Eight studies had one post-intervention meal [58,59,60, 62, 66, 68, 69, 79]. One study had three test meals [73].
All studies used a cross-over design and compared energy intake in a timeframe of up to 24 h. In all trials, absolute short-term energy intake was the primary or secondary outcome. For the meta-analysis, all 22 trials were eligible.
Population characteristics
In total, the 22 trials included 447 participants. The median (Interquartile range, IQR) age was 13.2 (1.1) years, with a range of 9 to 16 years (one trial did not report data on mean age [58]). Twenty-one trials except for one study [58] reported data on sex and 44% of the participants were female. The median (IQR) sample size of the selected studies was 15 (6), the sample size ranged from 9 to 38. Sample size was found to be small in eight studies [64, 65, 68, 69, 71, 73, 74, 78].
Four studies included participants with normal weight [59, 61, 68, 79], 13 studies included participants with overweight or obesity [60, 63,64,65,66,67, 71,72,73,74, 76,77,78], and five studies included both, participants with normal-weight, overweight and/or obesity [58, 62, 69, 70, 75].
Exercise characteristics
The 22 trials used eleven different exercise modalities and compared them with control interventions, where participants remained sedentary. Having groups with normal weight and overweight exercising at varying intensities resulted in a total number of 43 exercise conditions, which were compared to a control group in cross-over design. Most of the trials used cycling on an ergometer as the exercise intervention (80%), the second most exercise intervention was walking or running on ground or on a treadmill (12%). Exercise duration ranged from 15 min [59, 67] to 60 min [76], with a median (IQR) duration of 40 (15) minutes. Twenty studies reported the energy expended during the exercise intervention, and two did not [58, 68].
Of the 43 exercise conditions, four (9%) were low in exercise intensity, 26 (60%) used a moderate intensity, and 13 (30%) implemented a high exercise intensity. In most studies (68%), desired exercise intensity was controlled by the previously determined VO2max [60,61,62,63,64,65, 70,71,72,73,74,75,76,77,78]. Two studies (9%) determined desired exercise intensity with the use of previously measured ventilation threshold [59, 66] one study determined desired intensity with a percentage of the heart rate reserve [58]. Some studies solely differentiated between high intensity activities (e.g. bouts of 30 s sprints) [68] and low or medium intensity activities (e.g. swimming) [69].
Summary of study outcomes
Total energy intake
At qualitative level, of the exercise conditions compared, three study arms (7%) found a significantly higher energy intake (EI) after exercise [69, 77], ten (23%) found a significant reduction in EI [62, 63, 67, 69, 71,72,73,74,75, 77] and 30 (70%) exercise interventions resulted in no significant change in EI [61,62,63,64,65,66, 68,69,70, 73, 75, 76, 78, 79].
In line, the meta-analysis of 41 study arms (exercise n = 780 and control n = 478) showed no differences in total energy intake between the exercise and control group with a mean difference MD = 23.31 [-27.54, 74.15] kcal (Fig. 2). Sensitivity analyses showed that the results were robust to different correlation coefficients.

Quantitative analysis for energy intake of randomized controlled trials. In multi-arm trials, the sample size of the shared control group was divided to prevent double counting
Overall, the heterogeneity of studies was moderate, with an I2 of 57%. After excluding studies with a high risk of bias, I2 increased to 69% (Fig. 3).

Quantitative analysis for energy intake of randomized controlled trials with low or moderate risk of bias. In multi-arm trials, the sample size of the shared control group was divided to prevent double counting
To account for differences regarding the exercise condition, age and weight status, subgroup analyses were performed for i) low to moderate exercise vs. high intensity exercise (Fig. 4), ii) normal weight vs. overweight/obese (OW/OB; Fig. 5), iii) high intensity exercise in relation to normal weight vs. OW/OB (Fig. 6) and iv) participants with age < 13 years vs. age ≥ 13 years (Fig. 7). The heterogeneity decreased to I2 = 0% when only participants with normal weight were compared, as well as in the group with normal weight exercising at high intensity. No subgroup differences were observed. In particular, there was no influence of intensity of exercise on subsequent energy intake. Sensitivity analyses revealed that the results were robust to different imputed correlation coefficients (corr = 0.3, 0.5, 0.7) (Supporting Information S2).

Quantitative analysis for energy intake of randomized controlled trials categorized by low or moderate vs. high intensity exercise. In multi-arm trials, the sample size of the shared control group was divided to prevent double counting

Quantitative analysis for energy intake of randomized controlled trials categorized by subgroups with normal weight vs. overweight or obesity. In multi-arm trials, the sample size of the shared control group was divided to prevent double counting

Quantitative analysis for energy intake of randomized controlled trials with high intensity exercise categorized by subgroups with overweight or obesity vs. normal weight. In multi-arm trials, the sample size of the shared control group was divided to prevent double counting

Quantitative analysis for energy intake of randomized controlled trials for subgroups aged < 13 years vs. age ≥ 13 years. In multi-arm trials, the sample size of the shared control group was divided to prevent double counting
Energy expenditure
Nineteen studies reported the exercise-induced energy expenditure in 33 different exercise conditions, whereas three did not [58, 68, 75]. The energy expended while exercising ranged from 63 ± 7 kcal (in 15 min) [59] to 549 ± 3 kcal (in 60 min) [76], with a median (IQR) energy expenditure of 240 (158) kcal.
Macronutrients
Seventeen studies investigated macronutrient intake (Fig. 8), while five did not [58, 59, 69, 72, 79]. Of them, fifteen studies reported data on macronutrient intake either in grams or percentage of total food intake, and two studies solely stated whether macronutrient intake differed between intervention groups [64, 78]. Regarding protein, three studies found a significant increase in protein-intake after exercise [61, 65, 74], whereas the remaining 14 reported no significant changes. With regard to fat, three studies observed a significant increase in fat-intake after exercise [61, 74, 76], the remaining 14 found no such relationship. Finally, two studies reported a decrease in carbohydrate intake after exercise [74, 75] which was not the case in the other 15 studies. Overall, physical activity had no substantial effect on macronutrient intake.

Changes in macronutrient intake (protein, carbohydrates, fat) after exercise intervention compared to sedentary control. ↑: intake was higher after exercise; ↓: intake was lower after exercise; ↔ : no significant differences; NR: not reported
Appetite Sensations
All but three studies [61, 69, 71] examined hunger, satiety and prospective food consumption, one did report only hunger and prospective food consumption [71] (Fig. 9). Six studies also investigated the desire to eat [59, 63,64,65, 67, 78] and two studies used the Leeds food preference score [64, 65]. Summarized across studies, there was no significant effect on hunger, satiety, and prospective food consumption, with the exception of two studies: Bozinovski et al. [59] found hunger significantly attenuated after short duration exercise compared to long duration exercise and control and Fillon et al. [63] reported significantly reduced hunger in both exercise groups compared to control. Overall, physical activity had no substantial effect on appetite sensations.

Changes in hunger, satiety, prospective food consumption after exercise intervention compared to sedentary control. ↑: higher after exercise; ↓: lower after exercise; ↔ : no significant differences; NR: not reported
Risk of bias
The risk of bias assessment is presented in Table 2. The overall risk of bias was low in seven studies (31%), with some concerns in eleven studies (50%) and high in four studies (18%). One of the major methodological problems of the studies was that the data used to determine the outcome were not analysed according to a pre-specified analysis plan (which was completed before the outcome data were available for analysis), as required in domain 5 (D5) [57]. Another common issue relates to the duration that elapsed between interventions. Due to the within-subject design of the trials, studies were only classified as low-risk if no more than 28 days elapsed between interventions to rule out a significant alteration in metabolism during this time. However, several trials did not report any time between interventions, so they were classified as “some-concerns”, as required in domain 4 (D4) [57]. Most studies did not do a power calculation, two reported to be underpowered [59, 61].
Discussion
The aim of this study was to analyze the effects of acute exercise on energy intake under controlled conditions in children and adolescents to contribute to our understanding of energy balance regulation. The first research question analyzed whether acute exercising is followed by increased food intake. We found that children and adolescents did not alter their caloric and macronutrient intake after exercise tasks compared to their sedentary controls. These findings are in line with the previous study conducted in children and adolescents by Thivel et al. [44]. They are also largely consistent with meta-analyses conducted in adults on the acute (24 h) and short-term (up to 14 days) impact of exercise on food intake [37, 38].
The second question addressed whether training intensity, duration, and type of exercise affected subsequent energy intake, and the third question examined the influence of body weight status on the findings. Our data are partly in line with those of the earlier study by Thivel et al. [44]. In accordance with their findings, the group with normal weight did not alter their energy intake following exercise. However, they found a reducing effect of high-intensity exercise on energy intake only in the subgroup with obesity. The authors concluded that performing exercise at high intensity may have a transient anorexigenic effect in adolescents with obesity. These findings could not be confirmed in the present meta-analysis. This is most likely because stricter inclusion criteria were applied, and new high-quality randomized controlled trials were included in the analysis.
As shown in this meta-analysis, children and adolescents did not acutely compensate for an exercise intervention with increased food intake, regardless of age group, body weight status or exercise intensity. This results, on average, in a short-term negative energy balance, assuming an otherwise neutral energy balance. In the trials examined, a median of 240 kcal was expended during exercise. This corresponds to more than 10% of the daily caloric needs of a moderately active 10- to 13-year-old child [81]. A long-term caloric deficit of this magnitude resulting from exercise would lead to loss of adipose tissue or, if compensated for, contribute to a stable bodyweight, improved body composition and aid in healthy weight management [82,83,84]. This weight-reducing effect indicated by the results reported here was also demonstrated for adults with overweight in an umbrella review [85]. Since the actual weight loss is often less than expected, compensatory mechanisms such as increased sedentary behavior or a reduction in metabolic activity to keep energy balance stable have been suggested [86, 87]. This assumption is referred to as the “constrained total energy expenditure model” [88], but its validity is the subject of current debate [89]. Data on whether and under what circumstances exercise leads to a subsequent reduction in non-exercise physical activity are mixed [30, 32, 86, 90, 91].
Data on food intake in relation to longer periods of physical activity training are based on self-reported data. Thus, results from such longer studies cannot be directly compared with short-term, highly controlled conditions such as those reviewed here. However, the effect of at least 10 weeks of regular physical activity was systematically reviewed by Schwartz et al. [92]. Adolescents with obesity were found to reduce their self-reported food intake in response to several weeks of sports intervention. Similarly, the longer-term effects of an exercise intervention on energy intake have been studied in adults. In their meta-analysis, Beaulieu et al. [36] investigated the impact of exercise training interventions (median duration 12 weeks) on energy intake and appetite in adults with overweight/obesity. They found that no significant changes in food intake or appetite over the course of an exercise intervention occurred. In summary, the above results all point in the direction that, on average, exercise does not lead to an increase in food intake.
We demonstrated that not only caloric intake, but also macronutrient consumption remained unaffected by the intervention. This is in line with the findings by Thivel et al. [44] and is still the case when long-term interventions (at least 10 weeks) are examined under less controlled conditions, as reported by Schwartz et al. [92]. Similarly, adults also do not alter their macronutrient intake in response to exercise as presented by Donnelly et al. [37] and Beaulieu et al. [36]. Contrary to popular belief, this meta-analysis showed no increase of appetite after acute exercise. This is in accordance with the literature on adults [36, 37], and youth alike [44]. The influence of exercise on appetite-related hormones in children and adolescents has been sparsely studied to date [93]. In contrast to most studies in adults, Rumbold et al. [94] found increased levels of the hunger-inducing hormone Ghrelin after acute exercise in adolescent females. Consistent with the findings in adults, Prado et al. [95] demonstrated a significant increase in the hunger-reducing hormone Peptide Y in adolescent girls with obesity following 30 min of exercise.
This study has strengths and limitations. Strengths include adherence to PRISMA guidelines and exclusive examination of randomized controlled trials. The risk of bias in the studies was assessed using the Cochrane RoB-2-tool. Additionally, studies utilizing self-reported dietary intake, food frequency questionnaires, and similar potentially biased data acquisition methods were excluded [96,97,98]. All studies employed a crossover design, where subjects acted as their own controls, ensuring high comparability. The heterogeneous study population, comprising both sexes, all levels of fitness, and a broad body weight range, was chosen to closely reflect real-life conditions, enhancing generalizability. However, there are limitations. Sample sizes were often small, and studies predominantly focused on older children and adolescents. Moreover, the short-term duration of the studies prevents determination of whether compensatory food intake occurred in subsequent hours (e.g., at night or the next morning). When studies did not provide sufficient data from a paired analysis, a correlation coefficient of 0.5 was applied. Sensitivity analysis revealed stable results when using 0.3 and 0.7 as correlation coefficient. Nevertheless, a degree of uncertainty for data interpretation remains. Additionally, the applicability of results from randomized controlled trials in laboratory settings to the everyday lives of children and adolescents remains uncertain. Environmental factors could lead to overconsumption of palatable, high-energy-dense foods and large portions [6], even after exercising. In many study designs, accurately determining whether caloric intake met or exceeded energy needs was challenging. Solely Thivel et al. [43] utilized a calorimetric chamber, to precisely measure energy balance. Only two of the included studies accounted for fluid intake through beverages, standardizing post-intervention intake across participants [59, 79]. It is conceivable that increased drinking, due to thirst after exercise, led to a feeling of fullness and reduced food intake, as distension of the gastric wall is a key signal generator for satiety [99,100,101].
Conclusions
Engaging in physical activity has no significant effect on the subsequent energy or macronutrient intake of children and adolescents, nor on their appetite sensations, compared with a sedentary control group within a single day. However, exercise acutely raises energy expenditure and thus may help to control energy balance. The findings of this meta-analysis and other reviews related to this field support the importance of physical activity in promoting weight loss and improving body composition along with a balanced diet, as children and adolescents are not expected to eat more as a result of exercise. Additionally, there was no increase in appetite, which would be detrimental to weight reduction efforts. These findings were derived from controlled conditions. Considering other literature from the field, environmental factors could lead to overconsumption of palatable, high-energy-dense foods and large portions and/or increased sedentary behavior after exercising, compensating for the increased energy expenditure. Therefore, monitoring and reflecting on individual behavior after exercising appears to be useful for individual recommendations and countermeasures.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- IQR:
-
Interquartile range
- kcal:
-
Kilocalories
- MD:
-
Mean difference
- SE:
-
Standard error
- BMI:
-
Body mass index
- RMR:
-
Resting metabolic rate
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PICOS:
-
Participants, interventions, comparators, outcome, study design
- VO2max:
-
Maximum oxygen consumption
- HRmax:
-
Maximum heart rate
- SD:
-
Standard deviation
- CI:
-
Confidence interval
- RoB 2:
-
Risk-of-Bias tool for randomized crossover trials
- EI:
-
Energy intake
- OW:
-
Overweight
- OB:
-
Obese
References
Blundell JE, Gibbons C, Caudwell P, Finlayson G, Hopkins M. Appetite control and energy balance: impact of exercise. Obes Rev. 2015;16(Suppl 1):67–76. https://doi.org/10.1111/obr.12257.
Beaulieu K, Hopkins M, Blundell J, Finlayson G. Homeostatic and non-homeostatic appetite control along the spectrum of physical activity levels: An updated perspective. Physiol Behav. 2018;192:23–9. https://doi.org/10.1016/j.physbeh.2017.12.032.
Reges O, Leibowitz M, Hirsch A, Dicker D, Finer N, Haase CL, et al. A comprehensive descriptive assessment of obesity related chronic morbidity and estimated annual cost burden from a population-based electronic health record database. Isr J Health Policy Res. 2020;9:32. https://doi.org/10.1186/s13584-020-00378-1.
NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. 2017;390:2627–42. https://doi.org/10.1016/S0140-6736(17)32129-3.
Steene-Johannessen J, Hansen BH, Dalene KE, Kolle E, Northstone K, Møller NC, et al. Variations in accelerometry measured physical activity and sedentary time across Europe - harmonized analyses of 47,497 children and adolescents. Int J Behav Nutr Phys Act. 2020;17:38. https://doi.org/10.1186/s12966-020-00930-x.
Baker P, Machado P, Santos T, Sievert K, Backholer K, Hadjikakou M, et al. Ultra-processed foods and the nutrition transition: Global, regional and national trends, food systems transformations and political economy drivers. Obes Rev. 2020;21:e13126.
Pérez-Escamilla R, Obbagy JE, Altman JM, Essery EV, McGrane MM, Wong YP, et al. Dietary energy density and body weight in adults and children: a systematic review. J Acad Nutr Diet. 2012;112:671–84. https://doi.org/10.1016/j.jand.2012.01.020.
Hill JO, Wyatt HR, Peters JC. Energy balance and obesity. Circulation. 2012;126:126–32. https://doi.org/10.1161/CIRCULATIONAHA.111.087213.
Edholm OG, Fletcher JG, Widdowson EM, Mccance RA. The energy expenditure and food intake of individual men. Br J Nutr. 1955;9:286–300. https://doi.org/10.1079/BJN19550040.
Watts AG, Kanoski SE, Sanchez-Watts G, Langhans W. The physiological control of eating: signals, neurons, and networks. Physiol Rev. 2022;102:689–813. https://doi.org/10.1152/physrev.00028.2020.
Schwartz MW, Seeley RJ, Zeltser LM, Drewnowski A, Ravussin E, Redman LM, Leibel RL. Obesity pathogenesis: an endocrine society scientific statement. Endocr Rev. 2017;38:267–96. https://doi.org/10.1210/er.2017-00111.
Herforth A, Arimond M, Álvarez-Sánchez C, Coates J, Christianson K, Muehlhoff E. A global review of food-based dietary guidelines. Adv Nutr. 2019;10:590–605. https://doi.org/10.1093/advances/nmy130.
Organization WH. Global action plan on physical activity 2018–2030: more active people for a healthier world. Geneva: World Health Organization; 2019.
Piercy KL, Troiano RP, Ballard RM, Carlson SA, Fulton JE, Galuska DA, et al. The physical activity guidelines for Americans. JAMA. 2018;320:2020–8. https://doi.org/10.1001/jama.2018.14854.
Spinelli A, Buoncristiano M, Nardone P, Starc G, Hejgaard T, Júlíusson PB, et al. Thinness, overweight, and obesity in 6- to 9-year-old children from 36 countries: the World Health Organization European Childhood Obesity Surveillance Initiative-COSI 2015–2017. Obes Rev. 2021;22(Suppl 6):e13214.
Weiland A, Nannette LK, Zipfel S, Ehehalt S, Ziser K, Junne F, Mack I. Predictors of weight loss and weight loss maintenance in children and adolescents with obesity after behavioral weight loss intervention. Front Public Health. 2022;10:813822.
Varkevisser RDM, van Stralen MM, Kroeze W, Ket JCF, Steenhuis IHM. Determinants of weight loss maintenance: a systematic review. Obes Rev. 2019;20:171–211. https://doi.org/10.1111/obr.12772.
Tremblay A, Bellisle F. Nutrients, satiety, and control of energy intake. Appl Physiol Nutr Metab. 2015;40:971–9. https://doi.org/10.1139/apnm-2014-0549.
Blundell JE, Caudwell P, Gibbons C, Hopkins M, Näslund E, King NA, Finlayson G. Body composition and appetite: fat-free mass (but not fat mass or BMI) is positively associated with self-determined meal size and daily energy intake in humans. Br J Nutr. 2012;107:445–9. https://doi.org/10.1017/S0007114511003138.
Caudwell P, Finlayson G, Gibbons C, Hopkins M, King N, Näslund E, Blundell JE. Resting metabolic rate is associated with hunger, self-determined meal size, and daily energy intake and may represent a marker for appetite. Am J Clin Nutr. 2013;97:7–14. https://doi.org/10.3945/ajcn.111.029975.
Johnstone AM, Murison SD, Duncan JS, Rance KA, Speakman JR. Factors influencing variation in basal metabolic rate include fat-free mass, fat mass, age, and circulating thyroxine but not sex, circulating leptin, or triiodothyronine. Am J Clin Nutr. 2005;82:941–8. https://doi.org/10.1093/ajcn/82.5.941.
Ravussin E, Burnand B, Schutz Y, Jéquier E. Twenty-four-hour energy expenditure and resting metabolic rate in obese, moderately obese, and control subjects. Am J Clin Nutr. 1982;35:566–73. https://doi.org/10.1093/ajcn/35.3.566.
Fisher JP, Young CN, Fadel PJ. Autonomic adjustments to exercise in humans. Compr Physiol. 2015;5:475–512. https://doi.org/10.1002/cphy.c140022.
Patel PN, Zwibel H. StatPearls: Physiology, Exercise. Treasure Island: StatPearls Publishing; 2022.
Blundell JE, Caudwell P, Gibbons C, Hopkins M, Naslund E, King N, Finlayson G. Role of resting metabolic rate and energy expenditure in hunger and appetite control: a new formulation. Dis Model Mech. 2012;5:608–13. https://doi.org/10.1242/dmm.009837.
Petridou A, Siopi A, Mougios V. Exercise in the management of obesity. Metabolism. 2019;92:163–9. https://doi.org/10.1016/j.metabol.2018.10.009.
Westerterp KR. Control of energy expenditure in humans. Eur J Clin Nutr. 2017;71:340–4. https://doi.org/10.1038/ejcn.2016.237.
Weise CM, Hohenadel MG, Krakoff J, Votruba SB. Body composition and energy expenditure predict ad-libitum food and macronutrient intake in humans. Int J Obes (Lond). 2014;38:243–51. https://doi.org/10.1038/ijo.2013.85.
Hopkins M, Duarte C, Beaulieu K, Finlayson G, Gibbons C, Johnstone AM, et al. Activity energy expenditure is an independent predictor of energy intake in humans. Int J Obes (Lond). 2019;43:1466–74. https://doi.org/10.1038/s41366-018-0308-6.
Westerterp KR. Exercise, energy balance and body composition. Eur J Clin Nutr. 2018;72:1246–50. https://doi.org/10.1038/s41430-018-0180-4.
King NA, Hopkins M, Caudwell P, Stubbs RJ, Blundell JE. Individual variability following 12 weeks of supervised exercise: identification and characterization of compensation for exercise-induced weight loss. Int J Obes (Lond). 2008;32:177–84. https://doi.org/10.1038/sj.ijo.0803712.
Martin CK, Johnson WD, Myers CA, Apolzan JW, Earnest CP, Thomas DM, et al. Effect of different doses of supervised exercise on food intake, metabolism, and non-exercise physical activity: the E-MECHANIC randomized controlled trial. Am J Clin Nutr. 2019;110:583–92. https://doi.org/10.1093/ajcn/nqz054.
Beaulieu K, Hopkins M, Blundell J, Finlayson G. Does habitual physical activity increase the sensitivity of the appetite control system? A systematic review. Sports Med. 2016;46:1897–919. https://doi.org/10.1007/s40279-016-0518-9.
Martins C, Robertson MD, Morgan LM. Effects of exercise and restrained eating behaviour on appetite control. Proc Nutr Soc. 2008;67:28–41. https://doi.org/10.1017/S0029665108005995.
Deighton K, Batterham RL, Stensel DJ. Appetite and gut peptide responses to exercise and calorie restriction. The effect of modest energy deficits. Appetite. 2014;81:52–9. https://doi.org/10.1016/j.appet.2014.06.003.
Beaulieu K, Blundell JE, van Baak MA, Battista F, Busetto L, Carraça EV, et al. Effect of exercise training interventions on energy intake and appetite control in adults with overweight or obesity: a systematic review and meta-analysis. Obes Rev. 2021;22(Suppl 4):e13251. https://doi.org/10.1111/obr.13251.
Donnelly JE, Herrmann SD, Lambourne K, Szabo AN, Honas JJ, Washburn RA. Does increased exercise or physical activity alter ad-libitum daily energy intake or macronutrient composition in healthy adults? A systematic review. PLoS One. 2014;9:e83498. https://doi.org/10.1371/journal.pone.0083498.
Schubert MM, Desbrow B, Sabapathy S, Leveritt M. Acute exercise and subsequent energy intake. A meta-analysis. Appetite. 2013;63:92–104. https://doi.org/10.1016/j.appet.2012.12.010.
Melzer K, Kayser B, Saris WHM, Pichard C. Effects of physical activity on food intake. Clin Nutr. 2005;24:885–95. https://doi.org/10.1016/j.clnu.2005.06.003.
Blundell JE, Stubbs RJ, Hughes DA, Whybrow S, King NA. Cross talk between physical activity and appetite control: does physical activity stimulate appetite?. Proc Nutr Soc. 2003;62:651–61. https://doi.org/10.1079/PNS2003286.
Balaguera-Cortes L, Wallman KE, Fairchild TJ, Guelfi KJ. Energy intake and appetite-related hormones following acute aerobic and resistance exercise. Appl Physiol Nutr Metab. 2011;36:958–66. https://doi.org/10.1139/h11-121.
Liu X-M, Wang K, Zhu Z, Cao Z-B. Compensatory effects of different exercise durations on non-exercise physical activity, appetite, and energy intake in normal weight and overweight adults. Front Physiol. 2022;13:932846. https://doi.org/10.3389/fphys.2022.932846.
Thivel D, Blundell JE, Duché P, Morio B. Acute exercise and subsequent nutritional adaptations: what about obese youths?. Sports Med. 2012;42:607–13. https://doi.org/10.2165/11632460-000000000-00000.
Thivel D, Rumbold PL, King NA, Pereira B, Blundell JE, Mathieu M-E. Acute post-exercise energy and macronutrient intake in lean and obese youth: a systematic review and meta-analysis. Int J Obes (Lond). 2016;40:1469–79. https://doi.org/10.1038/ijo.2016.122.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71.
Schardt C, Adams MB, Owens T, Keitz S, Fontelo P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inform Decis Mak. 2007;7: 16. https://doi.org/10.1186/1472-6947-7-16.
American College of Sports Medicine. ACSM's guidelines for exercise testing and prescription. Philadelphia: Lippincott Williams & Wilkins; 2013.
Physical Activity Guidelines Advisory Committee. Physical activity guidelines advisory committee report. Washington, DC: U.S. Departement of Health and Human Services; 2008.
I. Bormann. DigitizeIt. 2022. https://www.digitizeit.xyz/de/. Accessed 5 Oct 2022.
Ankit Rohatgi. WebPlotDigitizer. 2022. https://automeris.io/WebPlotDigitizer. Accessed 5 Oct 2022.
Higgins J, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. Cochrane handbook for systematic reviews of interventions. Wiley Blackwell: Hoboken, NJ, Chichester; 2019.
Miller JR, van Hooren B, Bishop C, Buckley JD, Willy RW, Fuller JT. A systematic review and meta-analysis of crossover studies comparing physiological, perceptual and performance measures between treadmill and overground running. Sports Med. 2019;49:763–82. https://doi.org/10.1007/s40279-019-01087-9.
Elbourne DR, Altman DG, Higgins JPT, Curtin F, Worthington HV, Vail A. Meta-analyses involving cross-over trials: methodological issues. Int J Epidemiol. 2002;31:140–9. https://doi.org/10.1093/ije/31.1.140.
Cochrane. Review Manager (RevMan) [Computer programme]. Version 5.4. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration; 2020.
Rücker G, Cates CJ, Schwarzer G. Methods for including information from multi-arm trials in pairwise meta-analysis. Res Synth Methods. 2017;8:392–403. https://doi.org/10.1002/jrsm.1259.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60. https://doi.org/10.1136/bmj.327.7414.557.
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. https://doi.org/10.1136/bmj.l4898.
Ajibewa TA, O’Sullivan MP, Nagy MR, Block SS, Robinson LE, Colabianchi N, Hasson RE. The effects of interrupting prolonged sitting with intermittent activity on appetite sensations and subsequent food intake in preadolescent children. PLoS ONE. 2017;12:e0188986. https://doi.org/10.1371/journal.pone.0188986.
Bozinovski NC, Bellissimo N, Thomas SG, Pencharz PB, Goode RC, Anderson GH. The effect of duration of exercise at the ventilation threshold on subjective appetite and short-term food intake in 9 to 14 year old boys and girls. Int J Behav Nutr Phys Act. 2009;6:66. https://doi.org/10.1186/1479-5868-6-66.
Fearnbach SN, Silvert L, Keller KL, Genin PM, Morio B, Pereira B, et al. Reduced neural response to food cues following exercise is accompanied by decreased energy intake in obese adolescents. Int J Obes (Lond). 2016;40:77–83. https://doi.org/10.1038/ijo.2015.215.
Fearnbach SN, Masterson TD, Schlechter HA, Ross AJ, Rykaczewski MJ, Loken E, et al. Impact of imposed exercise on energy intake in children at risk for overweight. Nutr J. 2016;15:92. https://doi.org/10.1186/s12937-016-0206-5.
Fearnbach SN, Silvert L, Pereira B, Boirie Y, Duclos M, Keller KL, Thivel D. Reduced neural responses to food cues might contribute to the anorexigenic effect of acute exercise observed in obese but not lean adolescents. Nutr Res. 2017;44:76–84. https://doi.org/10.1016/j.nutres.2017.06.006.
Fillon A, Beaulieu K, Miguet M, Bailly M, Finlayson G, Julian V, et al. Delayed meal timing after exercise is associated with reduced appetite and energy intake in adolescents with obesity. Pediatr Obes. 2020;15:e12651. https://doi.org/10.1111/ijpo.1265.
Fillon A, Beaulieu K, Miguet M, Bailly M, Finlayson G, Julian V, et al. Does exercising before or after a meal affect energy balance in adolescents with obesity? Nutr Metab Cardiovasc Dis. 2020;30:1196–200. https://doi.org/10.1016/j.numecd.2020.04.015.
Fillon A, Mathieu ME, Masurier J, Roche J, Miguet M, Khammassi M, et al. Effect of exercise-meal timing on energy intake, appetite and food reward in adolescents with obesity: The TIMEX study. Appetite. 2020;146:104506. https://doi.org/10.1016/j.appet.2019.104506.
Masurier J, Mathieu M-E, Fearnbach SN, Cardenoux C, Julian V, Lambert C, et al. Effect of exercise duration on subsequent appetite and energy intake in obese adolescent girls. Int J Sport Nutr Exerc Metab. 2018;28:593–601. https://doi.org/10.1123/ijsnem.2017-0352.
Miguet M, Fillon A, Khammassi M, Masurier J, Julian V, Pereira B, et al. Appetite, energy intake and food reward responses to an acute high intensity interval exercise in adolescents with obesity. Physiol Behav. 2018;195:90–7. https://doi.org/10.1016/j.physbeh.2018.07.018.
Morris A, Cramb R, Dodd-Reynolds CJ. Food intake and appetite following school-based high-intensity interval training in 9–11-year-old children. J Sports Sci. 2018;36:286–92. https://doi.org/10.1080/02640414.2017.1302599.
Nemet D, Arieli R, Meckel Y, Eliakim A. Immediate post-exercise energy intake and macronutrient preferences in normal weight and overweight pre-pubertal children. Int J Pediatr Obes. 2010;5:221–9. https://doi.org/10.3109/17477160903311538.
Saunders TJ, Chaput J-P, Goldfield GS, Colley RC, Kenny GP, Doucet E, Tremblay MS. Children and youth do not compensate for an imposed bout of prolonged sitting by reducing subsequent food intake or increasing physical activity levels: a randomised cross-over study. Br J Nutr. 2014;111:747–54. https://doi.org/10.1017/S000711451300295X.
Thivel D, Isacco L, Rousset S, Boirie Y, Morio B, Duché P. Intensive exercise: a remedy for childhood obesity?. Physiol Behav. 2011;102:132–6. https://doi.org/10.1016/j.physbeh.2010.10.011.
Thivel D, Isacco L, Taillardat M, Rousset S, Boirie Y, Morio B, Duché P. Gender effect on exercise-induced energy intake modification among obese adolescents. Appetite. 2011;56:658–61. https://doi.org/10.1016/j.appet.2011.02.020.
Thivel D, Isacco L, Montaurier C, Boirie Y, Duché P, Morio B. The 24-h energy intake of obese adolescents is spontaneously reduced after intensive exercise: a randomized controlled trial in calorimetric chambers. PLoS ONE. 2012;7:e29840. https://doi.org/10.1371/journal.pone.0029840.
Thivel D, Metz L, Aucouturier J, Brakoniecki K, Duche P, Morio B. The effects of imposed sedentary behavior and exercise on energy intake in adolescents with obesity. J Dev Behav Pediatr. 2013;34:616–22. https://doi.org/10.1097/DBP.0000000000000010.
Thivel D, Metz L, Julien A, Morio B, Duché P. Obese but not lean adolescents spontaneously decrease energy intake after intensive exercise. Physiol Behav. 2014;123:41–6. https://doi.org/10.1016/j.physbeh.2013.09.018.
Thivel D, Maso F, Aouiche S, Coignet B, Doré E, Duché P. Nutritional responses to acute training sessions in young elite rugby players. Appetite. 2015;84:316–21. https://doi.org/10.1016/j.appet.2014.10.030.
Thivel D, Doucet E, Julian V, Cardenoux C, Boirie Y, Duclos M. Nutritional compensation to exercise- vs. diet-induced acute energy deficit in adolescents with obesity. Physiol Behav. 2017;176:159–64. https://doi.org/10.1016/j.physbeh.2016.10.022.
Thivel D, Roche J, Miguet M, Fillon A, Khammassi M, Beaulieu K, et al. Post-moderate-intensity exercise energy replacement does not reduce subsequent appetite and energy intake in adolescents with obesity. Br J Nutr. 2020;123:592–600. https://doi.org/10.1017/s0007114519003106.
Varley-Campbell JL, Moore MS, Williams CA. The effects of a mid-morning snack and moderate-intensity exercise on acute appetite and energy intake in 12–14-year-old adolescents. Br J Nutr. 2017;117:602–10. https://doi.org/10.1017/S0007114515004201.
Thivel D, Aucouturier J, Doucet É, Saunders TJ, Chaput J-P. Daily energy balance in children and adolescents. Does energy expenditure predict subsequent energy intake?. Appetite. 2013;60:58–64. https://doi.org/10.1016/j.appet.2012.09.022.
New Reference Values for Energy Intake. Ann Nutr Metab. 2015;66:219–23. https://doi.org/10.1159/000430959.
Hill JO, Peters JC, Wyatt HR. Using the energy gap to address obesity: a commentary. J Am Diet Assoc. 2009;109:1848–53. https://doi.org/10.1016/j.jada.2009.08.007.
Wewege M, van den Berg R, Ward RE, Keech A. The effects of high-intensity interval training vs. moderate-intensity continuous training on body composition in overweight and obese adults: a systematic review and meta-analysis. Obes Rev. 2017;18:635–46. https://doi.org/10.1111/obr.12532.
Soares R, Brasil I, Monteiro W, Farinatti P. Effects of physical activity on body mass and composition of school-age children and adolescents with overweight or obesity: systematic review focusing on intervention characteristics. J Bodyw Mov Ther. 2023;33:154–63. https://doi.org/10.1016/j.jbmt.2022.09.004.
Bellicha A, van Baak MA, Battista F, Beaulieu K, Blundell JE, Busetto L, et al. Effect of exercise training on weight loss, body composition changes, and weight maintenance in adults with overweight or obesity: An overview of 12 systematic reviews and 149 studies. Obes Rev. 2021;22(Suppl 4):e13256. https://doi.org/10.1111/obr.13256.
Mansfeldt JM, Magkos F. Compensatory responses to exercise training as barriers to weight loss: changes in energy intake and non-exercise physical activity. Curr Nutr Rep. 2023. https://doi.org/10.1007/s13668-023-00467-y.
Dhurandhar EJ, Kaiser KA, Dawson JA, Alcorn AS, Keating KD, Allison DB. Predicting adult weight change in the real world: a systematic review and meta-analysis accounting for compensatory changes in energy intake or expenditure. Int J Obes (Lond). 2015;39:1181–7. https://doi.org/10.1038/ijo.2014.184.
Pontzer H, Durazo-Arvizu R, Dugas LR, Plange-Rhule J, Bovet P, Forrester TE, et al. Constrained total energy expenditure and metabolic adaptation to physical activity in adult humans. Curr Biol. 2016;26:410–7. https://doi.org/10.1016/j.cub.2015.12.046.
Gonzalez JT, Batterham AM, Atkinson G, Thompson D. Perspective: Is the response of human energy expenditure to increased physical activity additive or constrained?. Adv Nutr. 2023;14:406–19. https://doi.org/10.1016/j.advnut.2023.02.003.
Washburn RA, Lambourne K, Szabo AN, Herrmann SD, Honas JJ, Donnelly JE. Does increased prescribed exercise alter non-exercise physical activity/energy expenditure in healthy adults? A systematic review. Clin Obes. 2014;4:1–20. https://doi.org/10.1111/cob.12040.
Silva AM, Júdice PB, Carraça EV, King N, Teixeira PJ, Sardinha LB. What is the effect of diet and/or exercise interventions on behavioural compensation in non-exercise physical activity and related energy expenditure of free-living adults? A systematic review. Br J Nutr. 2018;119:1327–45. https://doi.org/10.1017/S000711451800096X.
Schwartz C, King NA, Perreira B, Blundell JE, Thivel D. A systematic review and meta-analysis of energy and macronutrient intake responses to physical activity interventions in children and adolescents with obesity. Pediatr Obes. 2017;12:179–94. https://doi.org/10.1111/ijpo.12124.
Thivel D, Finlayson G, Blundell JE. Homeostatic and neurocognitive control of energy intake in response to exercise in pediatric obesity: a psychobiological framework. Obes Rev. 2019;20:316–24. https://doi.org/10.1111/obr.12782.
Rumbold PLS, St Clair Gibson A, Stevenson EJ, King JA, Stensel DJ, Dodd-Reynolds CJ. Influence of netball-based exercise on energy intake, subjective appetite and plasma acylated ghrelin in adolescent girls. Appl Physiol Nutr Metab. 2013;38:854–61. https://doi.org/10.1139/apnm-2012-0466.
Prado WL, Balagopal PB, Lofrano-Prado MC, Oyama LM, Tenório TR, Botero JP, Hill JO. Effect of aerobic exercise on hunger feelings and satiety regulating hormones in obese teenage girls. Pediatr Exerc Sci. 2014;26:463–9. https://doi.org/10.1123/pes.2013-0200.
Burrows TL, Ho YY, Rollo ME, Collins CE. Validity of dietary assessment methods when compared to the method of doubly labeled water: a systematic review in adults. Front Endocrinol (Lausanne). 2019;10:850. https://doi.org/10.3389/fendo.2019.00850.
Burrows TL, Martin RJ, Collins CE. A systematic review of the validity of dietary assessment methods in children when compared with the method of doubly labeled water. J Am Diet Assoc. 2010;110:1501–10. https://doi.org/10.1016/j.jada.2010.07.008.
Westerterp KR, Goris AHC. Validity of the assessment of dietary intake: problems of misreporting. Curr Opin Clin Nutr Metab Care. 2002;5:489–93. https://doi.org/10.1097/00075197-200209000-00006.
Klos B, Cook J, Crepaz L, Weiland A, Zipfel S, Mack I. Impact of energy density on energy intake in children and adults: a systematic review and meta-analysis of randomized controlled trials. Eur J Nutr. 2022. https://doi.org/10.1007/s00394-022-03054-z.
Rolls BJ. The relationship between dietary energy density and energy intake. Physiol Behav. 2009;97:609–15. https://doi.org/10.1016/j.physbeh.2009.03.011.
Mack I, Sauer H, Weimer K, Dammann D, Zipfel S, Enck P, Teufel M. Obese children and adolescents need increased gastric volumes in order to perceive satiety. Obesity (Silver Spring). 2014;22:2123–5. https://doi.org/10.1002/oby.20850.
Acknowledgements
We would like to thank Dr. rer. nat. Gerta Rücker from the Institute of Medical Biometry and Statistics at the University of Freiburg for her expertise on the methodology of the meta-analysis. We acknowledge support from the Open Access Publication Fund of the University of Tübingen.
Funding
Open Access funding enabled and organized by Projekt DEAL. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Study conception and design: IM and HH; data collection: HH; risk of bias assessment: MF in consultation with HH; analysis and interpretation of data and results: HH and IM; creation of figures and tables: HH; writing of the manuscript: HH in consultation with IM and CN; adding and commenting on the manuscript: IM and CN; overall direction and supervision: IM and SZ; all authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to practice
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hahn, H., Friedel, M., Niessner, C. et al. Impact of physical activity on caloric and macronutrient intake in children and adolescents: a systematic review and meta-analysis of randomized controlled trials. Int J Behav Nutr Phys Act 21, 76 (2024). https://doi.org/10.1186/s12966-024-01620-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-024-01620-8