
Abstract
Background
Active outdoor play is important for children’s health and development, and playgrounds provide good places for play. However, the importance of playground use for health and well-being is unclear. Our scoping review aims to create an overview of all research on playground use and health benefits for children.
Methods
Scopus, Web of Science, SportDiscus, and PsycInfo were searched using two search blocks, focusing on 'playground' and 'children' respectively, for publications from 2000 to November 2023. The primary inclusion criterion was examining the relationship between playground use and positive physical, mental, or social health outcomes. Only papers published in English were reviewed. For each publication, we synthesized and condensed the results, categorizing them by playground setting, reported health outcome, participant age group, study design, methodologies, publication's country, year, and ‘stage of evidence’.
Results
Data from 247 studies were extracted and nearly 80% of these publications were descriptive or exploratory studies. Fifty-two were intervention studies. Adding playground markings to schoolyards led to increased physical activity. Greening schoolyards had mainly positive effects on social and mental health. In Early Childhood Education and Care, renewing play structures had a positive effect on physical activity in three publications. All Public Open Space interventions we found were different, with mixed effects on health outcomes.
Conclusions
The existing evidence provides good arguments for policy makers, city planners and school-leaders to invest in adding playground markings in schoolyards as this will likely result in more physical activity. The evidence for the health benefits of investing in new play structures indicated that tailoring the playground to local needs is important as ‘one size does not fit all’ and playgrounds need to be designed as engaging and interesting places for children’s play if they are to generate health benefits. Investing in ‘greening’ playgrounds is likely to result in social and mental health benefits for children, but does not always result in more physical activity.
The research field needs more efficacy and effectiveness studies, and in particular replication and scale-up studies to demonstrate which type of playground interventions are successful.
Protocol
The review protocol was registered at Open Science Framework (https://doi.org/10.17605/OSF.IO/UYN2V).
Similar content being viewed by others


Background
Every child has the right to rest, relax, play and to take part in cultural and creative activities’, as stated in article 31 of the United Nations Convention on the Rights of the Child [1]. The Convention recognizes that play is not an optional extra for children, it is fundamental to their physical, social and mental development and intrinsic to their health and happiness in the present moment. Play is considered fundamental for child development as play helps children develop social, academic, and personal competences [2]. The Millennium Cohort Study in the United Kingdom demonstrates that independent outdoor play is associated with increased moderate-to-vigorous physical activity (MVPA) and reduced sedentary time [3]. With global concerns about inadequate children's physical activity levels, only 27%–33% of children meet physical activity recommendations [4], the World Health Organization recommends children to sit less and play more to grow up healthy [5]. Following the World Health Organization definition of health [5], this means that children should thrive mentally, socially as well as physically to be healthy.
Recent decades have witnessed a decline in children's outdoor play, likely due to safety concerns, both from increased car traffic on residential streets, as well as lower levels of contact between neighbours, leading to delayed initiation of independent outdoor play [6].
A large review [7] showed that parental attitude, behaviour, support and practice are main factors influencing children’s outdoor play. Furthermore, the same review emphasised that it is important to focus on increasing outdoor play time where children can be spontaneous and creative, stimulating freely chosen and self-directed play, while focusing less on adult-led activities. Playgrounds are likely perceived as safe places for children’s play, and on average children spent more time playing at playgrounds than in any other place [6]. However, play is not only happening in children’s free time. Among the 38 OECD (Organisation for Economic Co-operation and Development) countries, on average 87% of children aged 3–5 are enrolled in Early Childhood Education and Care (ECEC) [8] and therefore ECEC centres are important settings for play. For school-aged-children, schoolyards are crucial locations for active play, contributing with up to 40% of children’s daily physical activity [9].
Numerous reviews, focusing on specific playground settings, age groups, and health parameters, have explored playground-related health outcomes. Most reviews focused on physical activity in schoolyards (e.g. Clevenger and colleagues [10]) or ECEC (e.g. Martin and colleagues [11]). A recent review and meta-analysis showed that physical activity interventions in schoolyards had a positive effect on increasing accelerometer-assessed MVPA in school-aged children [12]. Reviews have also been published on playground benefits for other physical health outcomes such as motor skills (e.g. Pawlowski and colleagues [13]), weight status (e.g. Williams and colleagues [14]) or social (e.g. Moore and colleagues [15]) and mental (e.g. Vella-Brodrick and colleagues [16]) health outcomes. Finally, some reviews looked at health benefits of using playgrounds in public open spaces (e.g. Audrey and colleagues [17]).
Because children’s play behaviour is likely to have many similarities across different playground settings, lessons learnt in one setting could potentially be applicable in other settings. Furthermore, playground interventions often have the potential to influence more than one health outcome. Having a comprehensive understanding of the overall health benefits of children’s use of playgrounds in different settings can help policy makers and city planners determine if they should prioritise investing in playgrounds. It can also help health authorities, general practitioners and paediatricians decide if they should recommend parents to take their children to playgrounds regularly.
The objective of this scoping review is to identify and assess the available evidence on the health benefits of children’s use of playgrounds. More specifically, we will: 1) identify all research on playground use and health benefits, 2) assess the stage of evidence of all included publications, and 3) summarise the health effects of intervention studies of playground use.
Methods
The scoping review was conducted in accordance with the JBI methodology for scoping reviews [18]. The review protocol was registered at Open Science Framework (https://doi.org/10.17605/OSF.IO/UYN2V) in May 2022 and the PRISMA guidelines for scoping reviews were followed in designing, conducting, and reporting the results. The search was updated in November 2023.
Information sources and search strategy
In May 2022, we initiated a systematic search in four electronic databases: Scopus, Web of Science, SportDiscus, and PsycInfo. Collaborating with a research librarian, authors tested and refined search terms. To ensure comprehensive coverage, a sensitive search strategy was devised with two blocks—one containing synonyms for 'playground' and the other for 'children'. The search terms for Scopus are outlined in Table 1. Slight adaptations were made for each database's specific requirements. The updated search looked at the same four databases to include articles from 2022 and 2023. Prior to full-text screening of new articles, 2022 publications assessed in the original search were excluded as "Already included or excluded".
Eligibility criteria
Playgrounds were defined as places designed or designated to facilitate play. We included both indoor and outdoor playgrounds, public playgrounds, school playgrounds, ECEC playgrounds, as well as private playgrounds, and playgrounds requiring payment. Publications that exclusively focused on unfixed equipment or sports facilities, were excluded, as were studies exclusively focusing on organising play activities, and studies on temporary playstreets.
The primary inclusion criterion was examining the relationship between playground usage and positive physical, mental, or social health outcomes. Studies focusing on negative health outcomes (like injuries and bullying), environmental exposures (such as pollution, pesticides, sun exposure), playground availability, quality, safety, or security were excluded.
All children and adolescent populations (aged 0–17 years) were considered, irrespective of gender, health status, or physical abilities. Peer-reviewed articles published in English from January 2000 to November 2023 were included, while guidelines, conference abstracts, protocols, book chapters, PhD dissertations, reviews, and methodological papers were excluded. The year 2000 was chosen as a start year to balance being comprehensive with the relevance of publications to inform future research. An initial pilot screening in June 2022 ensured a consistent understanding and application of the inclusion criteria among authors.
Selection process
All publications were imported into Endnote 20.0.1, and duplicates were removed, before transferring all data to Covidence for screening of titles and abstracts. The full texts of the included publications were independently assessed by two authors between August and October 2022. Any discrepancies arising from decisions about inclusion or exclusion of a publication were addressed through discussions moderated by authors JS or CSP. The process was repeated in November 2023 for the updated search.
To assess the sensitivity of our search strategy, one author (CDM) examined if we had overlooked potentially relevant publications by screening the reference lists of ten randomly selected included full-text publications for any potentially relevant additional publications. This process took place in January 2023 and did not result in additional publications being identified.
Data extraction process and data items
Data were extracted from all included publications by two student assistants and one of the authors (CDM), and cross-checked by JS, CSP, and MT to ensure accuracy and consistency. We extracted data on authorship, country of origin, World Bank country income level [19], year of publication, research aim, number of participants involved, setting, health outcomes examined, study design, methodologies employed, and key findings.
Synthesis of extracted results
We encountered multiple publications from the same study and therefore our reporting is structured per publication rather than per study. For each publication, we synthesized and condensed the results, categorizing them by playground setting, reported health outcome, participant age group, study design, methodologies, publication's country, year, and ‘stage of evidence’.
Health outcomes were categorised as: physical health (subdivided in physical activity, motor skills, and weight status), social health (e.g. interactions with peers, social network), or mental health (e.g. well-being, self-esteem, and cognitive health outcomes).
The playground settings were categorised into four main contexts: 1) ECEC (i.e. day-care, kindergarten, and pre-school), 2) School (i.e. primary, elementary, middle, and/or secondary school), 3) Public open spaces (e.g. parks, squares with public playgrounds), and 4) Healthcare (e.g. hospitals, rehabilitation centre, or facilities for children with special needs).
The broad target population of children and adolescents (aged 0–17) was divided into the following age groups: 0-2yrs (toddlers), 3-5yrs (early childhood), 6-12yrs (middle childhood), and 13-17yrs (adolescents).
Following Bauman and Nutbeam [20], we assume that there are multiple stages of evidence in relation to the evaluation of health promotion programs. Various types of descriptive and exploratory studies are primarily used to define the problem (stage 1), before developing possible solutions that are tested in feasibility and pilot studies (stage 2), followed by efficacy and effectiveness studies (stage 3), and replication studies studying the implementation and effectiveness of interventions in a different context (stage 4), before scale-up studies (stage 5), and eventually monitoring studies of fully implemented health promotion programs can take place (stage 6). For each included publication the ‘stage of evidence’ was assigned independently by authors JS and CSP, and initial inconstancies were discussed and resolved.
For publications reporting results from intervention studies, we described and categorised the main intervention components, and summarised the findings by classifying the effect of playground use on health outcomes as: positive, negative, or showed no effect. If a publication reported on the same outcome measured with multiple methods or for multiple sub-groups, with a conflicting direction of the effect, the outcome was labelled as 'inconclusive'.
Results
Publication selection
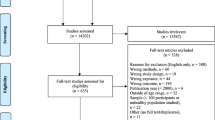
The initial search across the four databases yielded a total of 66,279 potentially relevant publications. After removing duplicates, the titles, and abstracts of 42,110 publications were screened, and 2,389 publications were selected for full-text screening. Following the full-text screening process, 215 publications met the inclusion criteria and were included in this scoping review. The search update resulted in 8,831 potentially relevant publications. After duplicates were removed 5,490 publications remained for title/abstract screening of which 5,330 were excluded, leaving 160 for full-text screening, resulting in 32 additional publications that met the inclusion criteria. In total, data extracted from 247 publications formed the basis of this scoping review. A full reference list of all 247 publications can be found in Additional file 1, and data extracted from all 247 publications can be found in Additional file 2. See Fig. 1 for the PRISMA flowchart of our selection process.

PRISMA flowchart
Publication characteristics
Three-out-of-four (75.7%) of the 247 included publications were published after 2012. Almost all publications reported on studies in high-income countries (92.7%), 117 were from Europe (47.4%), 81 were from North America (32.8%), and 33 were from Oceania (13.4%). Eighteen publications were from low- and middle-income countries (LMIC), whereof three were from Africa, five from Central and South America, and eight from Asia. Out of the 247 publications, 22 included 0–2-year-old children (8.9%), 107 included 3–5-year-old children (43.3%), 169 included 6–12-year-old children (68.4%), and 42 included 13–17-year-old children (17.0%). Only 11 of the 247 publications (also) included children and adolescents living with disability.
Most publications (n = 195, 78.9%) reported results from descriptive or exploratory studies, 31 (12.6%) presented results from feasibility or pilot studies, 20 (8.1%) were based on efficacy and effectiveness studies, and one was based on a replication study. More than half of the publications (n = 130, 52.6%) reported on studies that took place in a schoolyard playground, 63 were in an ECEC playground (25.5%), 54 (21.9%) in a public open space, and three studies took place on a playground in connection with a healthcare centre (1.2%). See characteristics of included publications in Table 2.
Results reported in the included publications
Physical activity was the primary outcome in 192 publications, followed by social health (n = 54), mental health (n = 30), motor skills (n = 15), and weight status (n = 12), see Table 3. A full overview of the results reported in all included publications can be found in Additional file 2.
Effects of using playgrounds – results from intervention studies
Presenting and summarizing all results from 247 publications in one review paper is not feasible, so we have chosen to focus on the stronger (stage 2 and higher) evidence presented in 52 intervention studies. Five focused on the health effects of free outdoor play, while 24 explored the impact of new playground structures—sometimes with additional elements like markings, loose equipment (e.g. balls, rackets, bats, skipping ropes), activities (e.g. sports or games), or staff training (e.g. on how to encourage children to be physically active during recess). The added play structures varied widely in type and budget. Playground markings were studied in 16 publications, and eight examined the effect of (access to) nature, often through greening school playgrounds. Additionally, six publications explored unique interventions, such as removing benches, lowering schoolyard density, opening the schoolyard after school hours, or comparing sports fields with playgrounds.
School
Most intervention studies were conducted in the school setting (one repetition, 17 efficacy and effectiveness, and 14 feasibility and pilot studies). The primary intervention components studied were play structures (16 publications) and playground markings (14 publications), often combined with each other, or integrated with organised activities or loose equipment.
Play structures in the schoolyard
Numerous school-based studies investigated the impact of renovating schoolyards with new play structures, greatly varying in type and size. The Danish SPACE study [21] and 'Activating Schoolyards' project [22] both included several new innovative play structures and landscaping developed after consulting school children, but results varied. Positive associations between the perceived schoolyard and physical activity were found in the SPACE study [21] while the Activating Schoolyards study reported increased activity for the least active children [22] but mixed effects in a sub-sample of all children [23]. In a Swedish study, adding play structures and landscaping during the renovations primarily attracted already active children, with less active ones being spectators [24]. The 'Camden active spaces' project in London showed insignificant effects on physical activity levels after renovating schoolyards in a deprived area where each school received a unique playground design, e.g., including new AstroTurf games pitches, climbing frames, trampolines, monkey bars, and outdoor gyms, which were designed based on themes emerging from consultations with children [25]. A study with a small (2000 Euro) intervention budget in the Netherlands [26] and a large natural experiment in Cleveland, USA [27], did not demonstrate significant effects on accelerometer-measured physical activity, but the Cleveland study did show a significant increase in schoolyard use. Conversely, a study in Denver, USA, showed increased physical activity levels after renovating schoolyards as part of the ‘Learning Landscapes’ program. Each schoolyard had unique attributes, but also common elements including areas with age-appropriate play equipment, asphalt areas for structured games such as basketball and tetherball and a grassed multipurpose playfield, typically with a track. All of the schoolyards had a central gathering space with a shade structure. Trees were planted in hard surface and grassed areas to increase shade [28]. In a small study at a school in Leadville, Colorado showed a positive effect after a renewal process added six swings, a mesh climbing structure, slides, and a spinning carousel. A new outdoor basketball court, walkways, boulder retaining walls, and grass-covered open play area were also constructed. Additional loose equipment was provided during post-observations, including balls, hula hoops, and cones for creating a course [29].
In a study focusing on eight boys with autism spectrum disorder, moving to a new playground designed for enhanced social interactions significantly increased group play and social interactions [30].
Playground markings in schoolyards
Feasibility and pilot studies examining the impact of adding playground markings in schoolyards were conducted in the UK [31, 32] the USA [33] and Spain [34] all demonstrating positive effects on physical activity. Typically, the markings consisted of a combination of game-related marking (e.g. hopscotch or 4-square), fantasy element (e.g. castles, dragons, snakes or animals), educational markings (e.g. clock faces or letter squares), or mazes and trails. In an efficacy and effectiveness study in the Northwest of England, Ridgers and colleagues reported a positive effect on recess physical activity after 6 weeks, a significant effect after 6 months, and no significant effect after 12 months [35, 36]. A study in Mexico City [37] found a positive effect on physical activity with basic and comprehensive interventions involving markings, loose equipment, and organised activities. The Australian Transform-Us! intervention showed a significant mid-intervention effect on recess physical activity [38]. A French study by Baquet et al. [39] reported a positive effect of playground markings on physical activity after 6 and 12 months. Crust and colleagues [40] found no influence on children’s physical self-perception but observed positive effects on physical activity and pro-social behaviour with added markings. Benthroldo et al. [41] in Brazil did not find a significant effect on self-reported physical activity after adding markings and loose equipment to public schools. Finally, a repetition study in France [42] reported a significant positive effect on accelerometer-measured physical activity using the same markings intervention as Ridgers and colleagues [35, 36] in the UK.
Natural elements (greening) in the schoolyard
Adding more natural elements (greening) in schoolyards was investigated in five feasibility and pilot studies. Barton et al. [43] compared loose equipment provision with a nature-based orienteering intervention, showing greater physical activity increase in the schoolyard than the orienteering area. Amicone et al. [44] found improved attention and perceived restorativeness in a green schoolyard compared to a paved surface schoolyard. Wood et al. [45] compared physical activity levels in the schoolyard versus the school field, finding children were less active (accelerometer measured) in the schoolyard than the school sports field.
A Los Angeles County pilot study [46] reported increased physical activity after replacing asphalt with green space at three time points. Similar schoolyard renovations in Chicago [47] led to heightened physical activity and prosocial interactions. A Dutch study [48] replacing pavement with greenery on schoolyards showed positive effects on attentional restoration, social well-being, and increased accelerometer-measured physical activity for girls.
Early Childhood Education and Care (ECEC)
In ECEC settings, nine publications reported on feasibility and pilot intervention studies, while two reported on efficacy and effectiveness studies. Three studies examined the feasibility of free outdoor play. MacArthur et al. [49] compared 15-min of unstructured outdoor play with 15-min of active video games using an Xbox 360 Kinect, showing inconclusive results on accelerometer measured physical activity. Tandon et al. [50] found no significant impact when comparing free outdoor play to teacher-led play. Lundy and Trawick-Smith [51] found a positive association between naturalistic playground play (i.e. free play, as opposed to adult-directed play) and on-task behaviour for boys, as well as children of low socio-economic status.
Canadian research [52] on increasing nature and risky play opportunities (play classified as: rough and tumble, height, mastery, unstable, speed, risk of getting lost) in ECEC settings showed significant decreases in accelerometer-measured physical activity and inconclusive results for social behaviours. A San Diego study observed increased activity levels after renovating a university ECEC outdoor playground, but no change in accelerometer-measured activity levels [53]. A large Belgian study [54] showed no increase in accelerometer-measured recess physical activity with added markings or loose equipment. Conversely, a Belgian pilot study [55] that varied recess times so that the number of children in the playground during recess was smaller, showed increased accelerometer-measured physical activity. A Japanese pilot study [56] reported a significant increase in accelerometer-measured physical activity by changing the layout of an ECEC playground to separate playground elements more, and make sure that play in one area did not disturb play in another area. Lastly, a natural experiment in Perth, Australia [57] showed significant increases in accelerometer-measured physical activity after renovating six ECEC outdoor playgrounds compared to unchanged ones.
Webster et al. [58] found no effect of adding playground markings and staff training on fundamental motor skills or physical activity in a US pilot study. And a small Norwegian study [59] on nature's impact on motor skills yielded mixed results.
Public open space
Our search yielded eight feasibility and pilot studies on playgrounds in public open spaces and one publication reporting on efficacy and effectiveness. The REVAMP natural experiment in Melbourne, Australia, found a positive impact on observed physical activity with the construction of a large playscape with many different play structures and landscaping [60]. A study in Sydney, Australia, showed increased physical activity for boys, but not girls, in a renovated park playground with added play structures [61]. Farley et al. [62] observed enhanced neighbourhood physical activity after opening a schoolyard for use after school hours in a low-income neighbourhood in New Orleans, USA. Roemmich et al. [63] found increased physical activity for both children and parents after removing park benches around a playground in another US study. A Danish study by Pawlowski et al. [64] evaluated the effect of co-creating a new neighbourhood playground with local 10–11-year-olds but did not observe an increase in playground use and activity levels. Molenberg et al. [65] evaluated adding 13 new activity and play spaces to low-income neighbourhoods in the Netherlands but did not show a significant effect on physical activity.
Tortella et al. [66] reported significant improvement in four out of six gross motor skills in a study of a new playground in Northern Italy designed to enhance fundamental motor skills. However, in a subsequent study [67], comparing free play and partly structured activity at the new playground showed no difference in motor skills between the two groups. Yang et al. [68] observed increased peer interactions after adding a play structure in a large park in Taipei, Taiwan.
Discussion
We set out to review and synthesise evidence on the health benefits of children's playground use. After assessing over 47,000 titles and abstracts, we extracted data from 247 included publications. Nearly 80% of these publications were descriptive or exploratory studies (evidence stage 1). Fifty-two were intervention studies, with 31 reporting on feasibility or pilot studies (stage 2), 20 reporting on efficacy and effectiveness studies (stage 3), and one reporting on a replication study (stage 4). Physical activity was the predominant health outcome studied, followed by social and mental health. Most intervention studies were conducted at schools, followed by ECEC, and Public Open Spaces. Three studies, all descriptive or exploratory (stage 1), were conducted in healthcare settings. Over 90% of all publications included were conducted in high-income countries, which limits the generalisability of currently available evidence.
The longitudinal analysis of data from the Gateshead Millennium Cohort Study revealed that the total volume of physical activity already starts declining by age 7 in the UK for both boys and girls, and, unlike many other studies, that this decline did not intensify during adolescence [69]. This emphasises the importance of implementing physical activity promotion interventions during primary-school age. One successful intervention, tested in various countries, is the addition of playground markings [31,32,33,34,35,36,37,38,39,40,41,42]. Renovating schoolyards with new play structures, though varied in budget, and yielding mixed results, also showed several positive effects [21, 22, 24, 28,29,30]. Greening schoolyards had positive effects on physical activity [46,47,48], as well as social and mental health [44, 47, 48].
In ECEC, providing more space per child had a positive impact on physical activity in a pilot study [55]. However, greening an ECEC playground had a negative effect on physical activity but a positive effect on social health [52]. In contrast to schools, adding playground markings in ECEC did not increase physical activity [58]. Renewing play structures in ECEC had a positive effect on physical activity in three publications [55,56,57].
All Public Open Space interventions we found were different, and even though many added play structures, they were not directly comparable, and results were mixed. Opening schoolyards for use by neighbourhood children outside of school hours increased activity levels [62], as did the construction of a large playscape in a park [60].
Our scoping review underscores the evidence supporting health benefits from playground use, but the effectiveness of interventions varies by setting, health outcome, and intervention component. Schoolyard markings, a cost-effective intervention, exhibit predominantly positive effects on children’s physical activity, warranting a logical next step—a scale-up study (evidence stage 5) like the one planned for the Australian 'Transform-Us!' program [70]. However, evidence for mental and social health outcomes is less abundant, highlighting the need for more comprehensive schoolyard studies. The diverse interventions adding play structures to schoolyards resulted in unclear health effects, necessitating studies that describe the interventions, and the program theory behind them, in (much) more detail, and include robust implementation measures so that the mechanisms can be better understood.
Motor skills in preschool-aged children from high-income countries are insufficient [71], impacting physical activity and weight status negatively across the lifespan [72]. Only three feasibility and pilot studies (stage 2) have explored how ECEC playgrounds influence motor skills. Larger scale (stage 3) studies are needed to provide evidence towards recommendations for motor skill development in ECEC. The planned scale-up of the Play Active intervention [73] in Australia will hopefully be able to provide stage 5 evidence of the health effects of a multi-component ECEC intervention.
The evidence for health benefits related to playgrounds in public open space playgrounds is less convincing with 47 out of the 55 included publications being based on descriptive and exploratory (stage 1) studies. Stage 2 and 3 intervention studies with a robust design, encompassing multiple health outcomes, are needed before evidence-based recommendations can be established.
Based on the playground descriptions and illustrations included in the publications we assessed, there is a very large variation in playground design Various publications mentioned that interventions need to be tailored to local needs and possibilities, ‘one size does not fit all’ when designing playground interventions, and evaluation studies need to take this tailoring process into account. A good playground renovation most likely needs to start with a thorough assessment of the current situation, to make sure that the additional play structures add variation and provide new opportunities for children that were not already catered for. Most studies mentioned consulting children before redesigning, and some studies actively involved children in the co-design of places to play. In general, involvement and co-design was mentioned as something positive but a Danish study [64] that specifically focused on evaluating the co-design process showed a negative effect on the use and activity after renewal. Furthermore, the fact that playgrounds can be designed in many ways, needs to be studied in more detail. For example, a pilot study found that the spatial layout of playground affects the pattern of play activity and the physical activity levels of young children [56].
Strengths and limitations
A scoping review is useful to map the literature on evolving or emerging topics and to identify gaps [74]. We followed the JBI methodology and PRISMA guidelines for scoping reviews for a robust, rigorous, and transparent review protocol [75], thus the risk of bias in our review methodology is low. However, despite an extensive assessment alignment process, reviewing 47,600 titles and abstracts as a team may have caused some inconsistencies in the selection process. A strength is that the search procedure was developed by a research team of experts in the research field of playground usage in collaboration with a librarian with extensive expertise in search strategies for scoping reviews. To capture as much relevant research as possible, four different databases were searched. However, given the large number of publications retrieved, we questioned if we should have created a third block containing health outcomes to narrow-down our search, but a search that is too narrow may compromise the breadth and depth of the review and is not suggested in the literature around scoping reviews [74]. Also, in accordance with doing scoping reviews, no strict quality assessment of included publications was performed since we wanted to cover all knowledge on the subject regardless of the design and quality of the study to create an overview of the research field. We did, however, assess the ‘stage of evidence’ for all publications, which, in our opinion, gives a good indication of how strong the evidence presented is. We did not include studies’only’ focusing on playground use or factors influencing playground use without measuring a health outcome. In future, these studies are also important to review to understand the mechanisms behind increasing playground use. Furthermore, while we used an inclusive definition of health, we did not include studies with relevant non-health outcomes, e.g. learning outcomes.
Finally, we only included positive physical, mental, or social health outcomes, assuming that almost all new or renovated playgrounds are safe, while challenging and fun for children. For a full overview of all health effects of using playgrounds, also negative health outcomes (like injuries and bullying), and environmental exposures (such as pollution, pesticides, sun exposure), should be assessed.
Conclusions
This scoping review builds on data extracted from 247 publications, demonstrating that there is a lot of research on the health benefits of playgrounds. However, most publications (nearly 80%) were based on descriptive or exploratory studies. We did include 52 intervention studies, but the majority were feasibility or pilot intervention studies, indicating that the research field needs more efficacy and effectiveness studies, and in particular replication and scale-up studies. However, the existing evidence already provides good arguments for policy makers, city planners and school-leaders to invest in adding playground markings in schoolyards as this will likely result in more physical activity. The evidence for the health benefits of investing in new play structures indicated that tailoring the playground to local needs is important as ‘one size does not fit all’ and playgrounds need to be designed as engaging and interesting places for children’s play if they are to generate health benefits. Investing in ‘greening’ playgrounds is likely to result in social and mental health benefits for children.
Providing available playgrounds are safe, health authorities, general practitioners and paediatricians can recommend parents to take their children to playgrounds regularly as using playgrounds will increase physical activity levels and stimulate social interaction with other children.
Availability of data and materials
All data extracted from the 247 included publications can be found in Additional file 2. Furthermore, all publications included in this scoping review can be found in a searchable database on the website of the World Playground Research Institute. See https://playgroundresearch.org/article-database/ For selected publications and topics, short summaries were created as ‘briefs’, which are also available on the website, see https://playgroundresearch.org/research-briefs/
Abbreviations
- ECEC:
-
Early Childhood Education and Care
- MVPA:
-
Moderate-to-Vigorous Physical Activity
References
Unicef. Convention on the Rights of the Child: UNICEF; 1989. Available from: https://www.unicef.org/child-rights-convention/convention-text [last accessed June 3, 2024].
Lightfood C, Cole M, Cole S. The Development of Children. Eighth Edition. New York: MacMillan Education; 2018.
Aggio D, Gardner B, Roberts J, et al. Correlates of children’s independent outdoor play: Cross-sectional analyses from the Millennium Cohort Study. Preventive Medicine Reports. 2017;8:10. https://doi.org/10.1016/j.pmedr.2017.07.007.
Aubert S, Barnes JD, Demchenko I, et al. Global matrix 4.0 Physical activity report card grades for children and adolescents: results and analyses from 57 countries. J Phys Act Health. 2022;19:700–28. https://doi.org/10.1123/jpah.2022-0456.
WHO. Guidelines on physical activity and sedentary behaviour: World Health Organization; 2019 Available from: https://www.who.int/publications/i/item/9789240015128 [Last accessed, June 3, 2024].
Dodd HF, FitzGibbon L, Watson BE, Nesbit RJ. Children’s play and independent mobility in 2020: results from the British children’s play survey. Int J Environ Res Public Health. 2021;18:4334. https://doi.org/10.3390/ijerph18084334.
Lee EY, Bains A, Hunter S, Ament A, Brazo-Sayavera J, Carson V, Hakimi S, Huang WY, Janssen I, Lee M, Lim H, Santos Silva DA, Tremblay MS. Systematic review of the correlates of outdoor play and time among children aged 3–12 years. Int J Behav Nutr Phys Act. 2021;18:41. https://doi.org/10.1186/s12966-021-01097-9.
OECD (Organisation for Economic Co-operation and Development) Family Database, Available from https://www.oecd.org/els/soc/pf3_2_enrolment_childcare_preschool.pdf [Last accessed, June 3, 2024].
Ridgers ND, Stratton G, Fairclough SJ. Physical Activity Levels of Children during School Playtime. Sports Med. 2006;36:359–71. https://doi.org/10.2165/00007256-200636040-00005.
Clevenger KA, Wierenga MJ, Howe CA, Pfeiffer KA. A Systematic Review of Child and Adolescent Physical Activity by Schoolyard Location. Kinesiology Review. 2020;9(2):147–58. https://doi.org/10.1123/kr.2019-0009.
Martin A, Brophy R, Clarke J, et al. Environmental and practice factors associated with children’s device-measured physical activity and sedentary time in early childhood education and care centres: a systematic review. Int J Behav Nutr Phys Act. 2022;19:84. https://doi.org/10.1186/s12966-022-01303-2.
Pfledderer CD, Kwon S, Strehli I, Byun W, Burns RD. The effects of playground interventions on accelerometer-assessed physical activity in pediatric populations: a meta-analysis. Int J Environ Res Public Health. 2022;19(6):3445. https://doi.org/10.3390/ijerph19063445.
Pawlowski CS, Madsen CD, Toftager M, Amholt TT, Schipperijn J. The role of playgrounds in the development of children’s fundamental movement skills: A scoping review. Plos One. 2023;18:e0294296.https://doi.org/10.1371/journal.pone.0294296
Williams AJ, Wyatt KM, Hurst AJ, Williams CA. A systematic review of associations between the primary school built environment and childhood overweight and obesity. Health Place. 2012;18:504–14. https://doi.org/10.1016/j.healthplace.2012.02.004.
Moore A, Lynch H, Boyle B. Can universal design support outdoor play, social participation, and inclusion in public playgrounds? A scoping review Dissability and Rehabilitation. 2020;44(13):3304–25. https://doi.org/10.1080/09638288.2020.1858353.
Vella-Brodrick DA, Gilowska K. Effects of Nature (Greenspace) on Cognitive Functioning in School Children and Adolescents: a Systematic Review. Educ Psychol Rev. 2022;34:1217–54. https://doi.org/10.1007/s10648-022-09658-5.
Audrey S, Batista-Ferrer H. Healthy urban environments for children and young people: A systematic review of intervention studies. Health Place. 2015;36:97–117. https://doi.org/10.1016/j.healthplace.2015.09.004.
Peters M, Marnie C, Tricco AC, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Synthesis. 2020;18(10):2119–26. https://doi.org/10.11124/JBIES-20-00167.
The-World-Bank. The World by Income and Region: The World Bank; 2022. Available from: https://datatopics.worldbank.org/world-development-indicators/the-world-by-income-and-region.html [Last accessed, June 3, 2024]. [Cited 2024 17th January]
Bauman A, Nutbeam D. Evaluation in a nutshell: a practical guide to the evaluation of health promotion programs. 3rd ed. Australia: McGraw-Hill; 2022.
Christiansen LB, Toftager M, Pawlowski CS, Andersen HB, Ersboll AK, Troelsen J. Schoolyard upgrade in a randomized controlled study design-How are school interventions associated with adolescents’ perception of opportunities and recess physical activity. Health Educ Res. 2017;32(1):58–68. https://doi.org/10.1093/her/cyw058.
Pawlowski CS, Bondo Andersen H, Schipperijn J. Difference in outdoor time and physical activity during recess after schoolyard renewal for the least-active children. J Phys ActHealth. 2020;17:968.
Andersen HB, Christiansen LB, Pawlowski CS, Schipperijn J. What we build makes a difference – Mapping activating schoolyard features after renewal using GIS, GPS and accelerometers. Landsc Urban Plan. 2019;191: 103617. https://doi.org/10.1016/j.landurbplan.2019.103617.
Fahlén J. Urgent expectations and silenced knowledge On spontaneous sport space as public health promoter and sport stimulator. European Journal for Sport and Society. 2011;8(3):167–91. https://doi.org/10.1080/16138171.2011.11687877.
Hamer M, Aggio D, Knock G, Kipps C, Shankar A, Smith L. Effect of major school playground reconstruction on physical activity and sedentary behaviour: Camden active spaces. BMC Public Health. 2017;17(1):552. https://doi.org/10.1186/s12889-017-4483-5.
Van Kann DHH, de Vries SI, Schipperijn J, de Vries NK, Jansen MWJ, Kremers SPJ. A Multicomponent Schoolyard Intervention Targeting Children’s Recess Physical Activity and Sedentary Behavior: Effects After 1 Year. J Phys Act Health. 2017;14(11):866–75. https://doi.org/10.1123/jpah.2016-0656.
Colabianchi N, Kinsella AE, Coulton CJ, Moore SM. Utilization and physical activity levels at renovated and unrenovated school playgrounds. Prev Med. 2009;48(2):140–3. https://doi.org/10.1016/j.ypmed.2008.11.005.
Brink LA, Nigg CR, Lampe SM, Kingston BA, Mootz AL, van Vliet W. Influence of schoolyard renovations on children’s physical activity: the Learning Landscapes Program. Am J Public Health. 2010;100(9):1672–8. https://doi.org/10.2105/ajph.2009.178939.
Frost MC, Kuo ES, Harner LT, Landau KR, Baldassar K. Increase in physical activity sustained 1 year after playground intervention. Am J Prev Med. 2018;54(5 Suppl 2):S124–9. https://doi.org/10.1016/j.amepre.2018.01.006.
Yuill N, Strieth S, Roake C, Aspden R, Todd B. Brief report: Designing a playground for children with autistic spectrum disorders - Effects on playful peer interactions. J Autism Dev Disord. 2007;37(6):1192–6. https://doi.org/10.1007/s10803-006-0241-8.
Stratton G, Leonard J. The effects of playground markings on the energy expenditure of 5–7-year-old school children. Pediatr Exerc Sci. 2002;14(2):170–80. https://doi.org/10.1123/pes.14.2.170.
Stratton G, Mullan E. The effect of multicolor playground markings on children’s physical activity level during recess. Preventive Medicine: An International Journal Devoted to Practice and Theory. 2005;41(5–6):828–33. https://doi.org/10.1016/j.ypmed.2005.07.009.
Huberty JL, Siahpush M, Beighle A, Fuhrmeister E, Silva P, Welk G. Ready for Recess: A Pilot Study to Increase Physical Activity in Elementary School Children. J Sch Health. 2011;81(5):251–7. https://doi.org/10.1111/j.1746-1561.2011.00591.x.
López-Fernández I, Molina-Jodar M, Garrido-González FJ, Pascual-Martos CA, Chinchilla JL, Carnero EA. Promoting physical activity at the school playground: a quasi-experimental intervention study. J Hum Sport Exerc. 2016;11(2):319–28.https://doi.org/10.14198/jhse.2016.112.05
Ridgers ND, Stratton G, Fairclough SJ. Twelve-Month Effects of a Playground Intervention on Children’s Morning and Lunchtime Recess Physical Activity Levels. J Phys Act Health. 2010;7:167–75. https://doi.org/10.1123/jpah.7.2.167.
Ridgers ND, Stratton G, Fairclough SJ, Twisk JWR. Children’s physical activity levels during school recess: a quasi-experimental intervention study. Int J Behav Nutr Phys Act. 2007;4:19. https://doi.org/10.1186/1479-5868-4-19.
Aburto NJ, Fulton JE, Safdie M, Duque T, Bonvecchio A, Rivera JA. Effect of a school-based intervention on physical activity: Cluster-randomized trial. Med Sci Sports Exerc. 2011;43(10):1898–906. https://doi.org/10.1249/MSS.0b013e318217ebec.
Yildirim M, Arundell L, Cerin E, et al. What helps children to move more at school recess and lunchtime? Mid-intervention results from Transform-Us! cluster-randomised controlled trial. Br J Sports Med. 2014;48(3):271–7. https://doi.org/10.1136/bjsports-2013-092466.
Baquet G, Aucouturier J, Gamelin FX, Berthoin S. Longitudinal follow-up of physical activity during school recess: impact of playground markings. Front Public Health. 2018;6:283. https://doi.org/10.3389/fpubh.2018.00283.
Crust L, McKenna J, Spence J, Thomas C, Evans D, Bishop D. The effects of playground markings on the physical self-perceptions of 10–11-year-old school children. Phys Educ Sport Pedagog. 2014;19(2):179–90. https://doi.org/10.1080/17408989.2012.732565.
Benthroldo RS, Paravidino VB, Cunha DB, Mediano MFF, Sichieri R, Marques ES. Environment modification at school to promote physical activity among adolescents: a cluster randomized controlled trial. Revista Brasileira de Epidemiologia. 2022;25:e220019.https://doi.org/10.1590/1980-549720220019.
Blaes A, Ridgers ND, Aucouturier J, Van Praagh E, Berthoin S, Baquet G. Effects of a playwound marking intervention on school recess physical activity in French children. Prev Med. 2013;57(5):580–4. https://doi.org/10.1016/j.ypmed.2013.07.019.
Barton J, Sandercock G, Pretty J, Wood C. The effect of playground-and nature-based playtime interventions on physical activity and self-esteem in UK school children. Int J Environ Health Res. 2015;25(2):196–206. https://doi.org/10.1080/09603123.2014.915020.
Amicone G, Petruccelli I, De Dominicis S, et al. Green Breaks: The restorative effect of the school environment’s green areas on children’s cognitive performance. Front Psychol. 2018;9:1579. https://doi.org/10.3389/fpsyg.2018.01579.
Wood C, Gladwell V, Barton J. A repeated measures experiment of school playing environment to increase physical activity and enhance self-esteem in UK school children. Plos One. 2014;9(9):e108701.https://doi.org/10.1371/journal.pone.0108701.
Raney MA, Bowers AL, Rissberger AL. Recess Behaviors of Urban Children 16 Months After a Green Schoolyard Renovation. J Phys Act Health. 2021;18(5):563–70. https://doi.org/10.1123/jpah.2020-0280.
Bohnert AM, Nicholson LM, Mertz L, Bates CR, Gerstein DE. Green schoolyard renovations in low-income urban neighborhoods: Benefits to students, schools, and the surrounding community. Am J Community Psychol. 2022. https://doi.org/10.1002/ajcp.12559.
van Dijk-Wesselius JE, Maas J, Hovinga D, van Vugt M, van den Berg AE. The impact of greening schoolyards on the appreciation, and physical, cognitive and social-emotional well-being of schoolchildren: A prospective intervention study. Landsc Urban Plan. 2018;180:15–26. https://doi.org/10.1016/j.landurbplan.2018.08.003.
MacArthur B, Coe D, Sweet A, Raynor H. Active videogaming compared to unstructured, outdoor play in young children: Percent time in moderate- to vigorous-intensity physical activity and estimated energy expenditure. Games for Health. 2014;3(6):388–94. https://doi.org/10.1089/g4h.2014.0017.
Tandon PS, Downing KL, Saelens BE, Christakis DA. Two approaches to increase physical activity for preschool children in child care centers: a matched-pair cluster-randomized trial. Int J Environ Res Public Health. 2019;16(20):4020. https://doi.org/10.3390/ijerph16204020.
Lundy A, Trawick-Smith J. Effects of active outdoor play on preschool children’s on-task classroom behavior. Early Childhood Educ J. 2021;49(3):463–71. https://doi.org/10.1007/s10643-020-01086-w.
Brussoni M, Ishikawa T, Brunelle S, Herrington S. Landscapes for play: Effects of an intervention to promote nature-based risky play in early childhood centres. J Environ Psychol. 2017;54:139–50. https://doi.org/10.1016/j.jenvp.2017.11.001.
Nicaise V, Kahan D, Reuben K, Sallis JF. Evaluation of a Redesigned Outdoor Space on Preschool Children’s Physical Activity During Recess. Pediatr Exerc Sci. 2012;24(4):507–18. https://doi.org/10.1123/pes.24.4.507.
Cardon G, Labarque V, Smits D, Bourdeaudhuij ID. Promoting physical activity at the pre-school playground: The effects of providing markings and play equipment. Prev Med. 2009;48(4):335–40. https://doi.org/10.1016/j.ypmed.2009.02.013.
Van Cauwenberghe E, De Bourdeaudhuij I, Maes L, Cardon G. Efficacy and feasibility of lowering playground density to promote physical activity and to discourage sedentary time during recess at preschool: A pilot study. Preventive Medicine: An International Journal Devoted to Practice and Theory. 2012;55(4):319–21. https://doi.org/10.1016/j.ypmed.2012.07.014.
Sumiya M, Nonaka T. Does the spatial layout of a playground affect the play activities in young children? A pilot study. Front Psychol. 2021;12:627052.https://doi.org/10.3389/fpsyg.2021.627052.
Ng M, Rosenberg M, Thornton A, et al. The effect of upgrades to childcare outdoor spaces on preschoolers’ physical activity: Findings from a natural experiment. Int J Environ Res Public Health. 2020;17(2):468. https://doi.org/10.3390/ijerph17020468.
Webster EK, Kepper MM, Saha S, et al. Painted playgrounds for preschoolers’ physical activity and fundamental motor skill improvement: a randomized controlled pilot trial of effectiveness. BMC Pediatr. 2023;23(1):455. https://doi.org/10.1186/s12887-023-04260-2.
Fjortoft I. The natural environment as a playground for children: The impact of outdoor play activities in pre-primary school children. Early Childhood Educ J. 2001;29(2):111–7. https://doi.org/10.1023/A:1012576913074.
Veitch J, Salmon J, Crawford D, et al. The REVAMP natural experiment study: the impact of a play-scape installation on park visitation and park-based physical activity. Int J Behav Nutr Phys Act. 2018;15:10. https://doi.org/10.1186/s12966-017-0625-5.
Bohn-Goldbaum EE, Phongsavan P, Merom D, Rogers K, Kamalesh V, Bauman AE. Does playground improvement increase physical activity among children? A quasi-experimental study of a natural experiment. J Environ Public Health. 2013. https://doi.org/10.1155/2013/109841.
Farley TA, Meriwether RA, Baker ET, Watkins LT, Johnson CC, Webber LS. Safe play spaces to promote physical activity in inner-city children: Results from a pilot study of an environmental intervention. Am J Public Health. 2007;97(9):1625–31. https://doi.org/10.2105/AJPH.2006.092692.
Roemmich JN, Beeler JE, Johnson L. A microenvironment approach to reducing sedentary time and increasing physical activity of children and adults at a playground. Preventive Medicine: An International Journal Devoted to Practice and Theory. 2014;62:108–12. https://doi.org/10.1016/j.ypmed.2014.01.018.
Pawlowski CS, Schmidt T, Nielsen JV, Troelsen J, Schipperijn J. Will the children use it?—A RE-AIM evaluation of a local public open space intervention involving children from a deprived neighbourhood. Eval Progr Plann. 2019;77;101706.https://doi.org/10.1016/j.evalprogplan.2019.101706.
Molenberg FJM, Noordzij JM, Burdorf A, van Lenthe FJ. New physical activity spaces in deprived neighborhoods: Does it change outdoor play and sedentary behavior? A natural experiment. Health Place. 2019;58:102151.https://doi.org/10.1016/j.healthplace.2019.102151.
Tortella P, Haga M, Loras H, Sigmundsson H, Fumagalli G. Motor skill development in Italian pre-school children induced by structured activities in a specific playground. Plos One. 2016;11(7):e0160244. https://doi.org/10.1371/journal.pone.0160244.
Tortella P, Haga M, Lorås H, Fumagalli GF, Sigmundsson H. Effects of free play and partly structured playground activity on motor competence in preschool children: a pragmatic comparison trial. Int J Environ Res Public Health. 2022;19(13):7652. https://doi.org/10.3390/ijerph19137652.
Yang JT, Chen CI, Zheng MC. Elevating children’s play experience: a design intervention to enhance children’s social interaction in park playgrounds. Sustainability (Switzerland). 2023;15(8):6971. https://doi.org/10.3390/su15086971.
Farooq MA, Parkinson KN, Adamson AJ, et al. Timing of the decline in physical activity in childhood and adolescence: Gateshead Millennium Cohort Study. Br J Sports Med. 2018;52:1002–6. https://doi.org/10.1136/bjsports-2016-096933.
Koorts H, Timperio A, Lonsdale C, et al. Scaling up a school-based intervention to increase physical activity and reduce sedentary behaviour in children: protocol for the TransformUs hybrid effectiveness–implementation trial. BMJ Open. 2023;13(10):e078410.https://doi.org/10.1136/bmjopen-2023-078410
Duncan MJ, Foweather L, Bardid F, et al. Motor Competence Among Children in the United Kingdom and Ireland: An Expert Statement on Behalf of the International Motor Development Research Consortium. Journal of Motor Learning and Development. 2022;10(1):7–26. https://doi.org/10.1123/jmld.2021-0047.
Hulteen R, Morgan P, Barnett L, Stodden D, Lubans D. Development of foundational movement skills: a conceptual model for physical activity across the lifespan. Sports Med. 2018;48:1533. https://doi.org/10.1007/s40279-018-0892-6.
McLaughlin M, Nathan A, Thornton A, Schipperijn J, Trost SG, Christian H. Adaptations to scale-up an early childhood education and care physical activity intervention for real-world availability — Play Active. Int J Behav Nutr Phys Act. 2023;20(1):65. https://doi.org/10.1186/s12966-023-01457-7.
Mak S, Thomas A. Steps for Conducting a Scoping Review. J Grad Med Educ. 2022;14(5):565–7. https://doi.org/10.4300/jgme-d-22-00621.1.
Peters MDJ, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil, H. Scoping Reviews (2020). In: Aromataris E, Lockwood C, Porritt K, Pilla B, Jordan Z, editors. JBI Manual for Evidence Synthesis. JBI; 2024. Available from: https://synthesismanual.jbi.global, https://doi.org/10.46658/JBIMES-24-09.
Acknowledgements
We would like to acknowledge student assistants Jonatan Villebro and Kasper Nørgaard Christensen and research librarian Lasse Østengaard for their contributions to this scoping review.
Funding
Open access funding provided by University of Southern Denmark This study was funded by KOMPAN, a large international playground equipment company. KOMPAN had no influence on the methods, results, or conclusions of this scoping review.
Author information
Authors and Affiliations
Contributions
JS, Conceptualization, Methodology, Writing—Original Draft, Formal analysis, Validation, Supervision, Funding acquisition. CDM, Methodology, Software, Investigation, Formal analysis, Data Curation, Visualization, Writing—Original Draft, MT, Conceptualization, Methodology, Investigation, Formal analysis, Validation, Writing—Review & Editing. DNJ, Investigation, Writing—Review & Editing. IL, Writing—Review & Editing. TTA, Conceptualization, Methodology, Investigation, Writing—Review & Editing. CSP, Conceptualization, Methodology, Investigation, Formal analysis, Validation, Writing—Review & Editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
Author JS is a member of the Editorial Board of International Journal of Behavioral Nutrition and Physical Activity. JS was not involved in the journal’s peer review process of, or decisions related to, this manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Schipperijn, J., Madsen, C.D., Toftager, M. et al. The role of playgrounds in promoting children’s health – a scoping review. Int J Behav Nutr Phys Act 21, 72 (2024). https://doi.org/10.1186/s12966-024-01618-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-024-01618-2