
Abstract
Background
Healthy lifestyle behaviors (LBs) have been widely recommended for the prevention and management of cardiovascular disease (CVD). Despite a large number of studies exploring the association between combined LBs and CVD, a notable gap exists in integration of relevant literatures. We conducted a systematic review and meta-analysis of prospective cohort studies to analyze the correlation between combined LBs and the occurrence of CVD, as well as to estimate the risk of various health complications in individuals already diagnosed with CVD.
Methods
Articles published up to February 10, 2023 were sourced through PubMed, EMBASE and Web of Science. Eligible prospective cohort studies that reported the relations of combined LBs with pre-determined outcomes were included. Summary relative risks (RRs) and 95% confidence intervals (CIs) were estimated using either a fixed or random-effects model. Subgroup analysis, meta-regression, publication bias, and sensitivity analysis were as well performed.
Results
In the general population, individuals with the healthiest combination of LBs exhibited a significant risk reduction of 58% for CVD and 55% for CVD mortality. For individuals diagnosed with CVD, adherence to the healthiest combination of LBs corresponded to a significant risk reduction of 62% for CVD recurrence and 67% for all-cause mortality, when compared to those with the least-healthy combination of LBs. In the analysis of dose-response relationship, for each increment of 1 healthy LB, there was a corresponding decrease in risk of 17% for CVD and 19% for CVD mortality within the general population. Similarly, among individuals diagnosed with CVD, each additional healthy LB was associated with a risk reduction of 27% for CVD recurrence and 27% for all-cause mortality.
Conclusions
Adopting healthy LBs is associated with substantial risk reduction in CVD, CVD mortality, and adverse outcomes among individuals diagnosed with CVD. Rather than focusing solely on individual healthy LB, it is advisable to advocate for the adoption of multiple LBs for the prevention and management of CVD.
Trial registration
PROSPERO: CRD42023431731.
Significance
The meta-analysis examined the quantitative correlation between lifestyle behaviors (LBs) and the incidence of cardiovascular disease (CVD) and CVD mortality in the general population, as well as adverse outcomes in CVD patients. The results suggest that healthy LBs are associated with substantial risk reduction in these 3 outcomes. Multiple LBs, instead of tackling one certain LB, should be recommended for the prevention and management of CVD.
Similar content being viewed by others


Background
Cardiovascular disease (CVD) has been one of the major global health concerns for decades [1, 2]. In 2017, it was estimated that approximately 1.76 billion people worldwide were affected by CVD [3]. Currently, both high-income and low-and middle-income countries are witnessing an increase in disease burden associated with CVD morbidity and mortality [4]. The World Health Organization (WHO) reported that the global annual deaths caused by CVD are approximately 17.9 million, accounting for 32% of all deaths [1]. The treatment and management of CVD may be costly, limiting the health and sustainable development of every country in the world [5]. CVD causes annual global economic losses of at least one trillion dollars [6]. To date, cost-effective interventions and health policies are imperative to reduce premature mortality and treatment costs caused by CVD.
CVD is largely recognized as a preventable disease, due to the facts that modifiable risk factors have been shown to account for more than 90% of the risk of CVD [7]. Globally, an increasing number of healthy lifestyle behaviors (LBs) have been proven to be effective in preventing and even treating CVD. Cohort studies have shown that LBs such as maintaining a healthy diet, engaging in regular physical activity, maintaining a healthy body weight, avoiding tobacco use, getting quality sleep, and fostering social interactions, are cost-effective strategies for modifying risk factors of CVD including dyslipidemia, high blood pressure, and elevated glucose levels [8,9,10,11,12]. The significant effects of healthy LBs in managing CVD are being increasingly confirmed and reiterated in numerous literature sources. The symptoms of CVD have been reported to improve and lessen following regular interventions comprising dietary adjustments and physical exercise [13, 14]. Moreover, some prospective cohort studies are uncovering the benefits of the number of LBs in lowering the incidence, mortality, and long-term adverse outcomes of CVD [12, 15,16,17,18,19].
However, to the best of our knowledge, there is currently no comprehensive meta-analysis quantifying the dose-response relationships between LBs and incident CVD and risk of health outcomes among individuals with CVD. In this study, we gathered the prospective cohort studies of healthy LBs for prevention and treatment of CVD published worldwide since 1998. We hence conducted a meta-analysis to evaluate the quantitative correlation between LBs and the incidence of CVD and CVD mortality in the general population, as well as adverse outcomes in individuals with CVD. The current study is expected to provide higher-level evidence supporting the positive role of healthy LBs in reducing the risk of CVD and promoting favorable clinical treatment outcomes for individuals with CVD.
Methods
The current systematic review and meta-analysis was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (See Additional file 1) [20]. In drafting the abstract, we adhered to the 12-item PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) extension guidelines [21]. This meta-analysis was registered with the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD42023431731.
Data source and search strategy
A comprehensive search was conducted on PubMed, EMBASE, and Web of Science databases up until February 10, 2023, to identify relevant studies reporting on the association between LBs and the incidence of total or subtypes of CVD. The search also aimed to explore the risk of total or subtypes of CVD mortality, total or subtypes of CVD recurrence, CVD mortality, or all-cause mortality among individuals with CVD. The search was limited to studies published in the English language, using a combination of MeSH terms and free-text terms (See Supplemental Table 1 in Additional file 2). We manually combed through the reference lists of the included articles to identify additional pertinent research. Published systematic reviews and meta-analyses were also used as a data source. Two investigators (JW and YF) independently conducted systematic searches, screened the articles, and reviewed the full text of the selected articles. In case of any disagreement, they discussed the discrepancies with the senior investigator to reach a consensus (YM).
Study selection
Studies were included in this meta-analysis if they met the following inclusion criteria: (1) prospective cohort study design; (2) adult population including the general population or individuals with CVD; (3) studies with a minimum follow-up duration of more than 1 year; (4) studies focusing on healthy lifestyle with three or more LBs, including those derived from the American Heart Association’s Life’s Essential 8 framework [22], excluding metabolic factors, such as blood lipid and glucose; (5) each LB in the studies was the categorical variable and different categories was assigned unequal value; (6) the studies reporting pre-determined outcomes, including incident of total CVD or CVD subtypes (including coronary heart disease [CHD], stroke, heart failure [HF], ischemic heart disease [IHD] or myocardial infarction [MI]), total or subtypes of CVD mortality in general population, CVD recurrence, CVD mortality, or all-cause mortality among individuals with CVD; (7) the studies reported quantitative estimates (odds ratio [OR], risk ratio [RR], or hazard ratio [HR]) and their 95% confidence intervals (CIs), or provided sufficient data to calculate these estimates. In cases where multiple publications were based on the same dataset, those with more complete information were selected. Otherwise, publications that included the largest number of participants were selected. Moreover, reviews, comments, letters, and editorials were excluded from the analysis. Additionally, we excluded reviews, comments, letters, and editorials.
Data extraction and quality assessment
Data were extracted from published articles with the use of a predefined protocol. Two investigators (JW and YF) independently extracted the following information from the included studies: first author, publication year, country, cohort name, sex, mean age, duration of follow-up, sample size, the definitions of combination of LBs, number of cases, outcome attainment, health status, number of cases and person-years/number of participants per LB category, most adjusted risk estimates (ORs, RRs, or HRs) with their corresponding 95% CIs for each category and adjustment variables. Any disagreement was resolved by consensus involving a third author. For articles with insufficient data or unclear information, the corresponding authors were contacted (at least two attempts were made).
The study quality of eligible prospective cohort acticles was evaluated using the Newcastle-Ottawa Scale [23], with a total score of 9 points (highest quality) for eight aspects, which focused on the selection of the study groups (4 points), the comparability of the groups (2 points) and the ascertainment of outcome (3 points).
Definitions of LB
LB refers to health-related lifestyle behaviors [24]. Our study defines combined LBs as consisting of three or more LBs, such as smoking, drinking alcohol or drinking moderately, sleep, physical exercise, diet, body weight, etc. Importantly, all LBs are regarded as equally significant in their contribution to overall health outcomes. A comprehensive LB score was obtained by assigning values to each LB. Due to the varying number of categorical divisions within each LB across the eligible studies, there are two main scoring methodologies in our meta-analysis: (1) studies simply classify individuals either exhibiting or not exhibiting a certain behavior as “1” or “0”. This method exists in the studies of dividing each LB into two categories. (2) studies assign unequal value to a certain behavior with different categories, in cases where featured LB into multiple categories. An example of this methodology is evident in the segmentation of physical activity into five categories, ranging from “rarely or never” to “4 or more times per week”, with corresponding scores ranging from 0 to 4 assigned for each category. Due to we were unable to access the original data contained within the articles, we could not differentiate the varying degree of effect of different LBs on the outcome, treating all LBs as having equal significance in their contribution. Similarly, we did not prespecify cutoffs for each LB, instead relying on the definitions provided by the respective study authors. We considered the largest number of healthy LBs in the original study as “the healthiest combination of LBs”, and similarly considered the least number of healthy LBs as “the least-healthy combination of LBs”.
Data synthesis and analysis
Relative risks (RRs) were used as the unified effect measure to assess the association between the LBs and the pre-determined outcomes. In some studies, hazard ratios (HRs) were reported and were considered approximately equal to RRs in terms of measuring the association [25, 26]. Due to the high incidence of CVD, the ORs may present an overestimation of the true RRs; therefore, we converted the ORs reported by included studies into RRs using a previously published correction method [27]. Articles reporting data separately from different cohorts, or from different regions, or reporting different types of outcomes within an article, were treated as separate studies. For articles reported data separately for different subgroups such as different sex or sub-types of outcomes, the fixed-effect model was used to re-calculate risk estimates. In cases where the number of cases or participants in each category was not explicitly provided, we calculated it using the available data [28]. When the category with the least-healthy combination of LBs was not the reference category, the method of Hamling and colleagues was used to re-calculate the risk estimates [29]. When exposures were reported as a range, we took the midpoint value for analyses. In situations where the healthiest combination of LBs and the least-healthy combination of LBs categories were open-ended, we followed a specific approach. For the least-healthy combination of LBs category, we defined 0 as the lower bound, while for the healthiest combination of LBs category, we used the number of LBs involved in the study as the upper bound. We then estimated the midpoint value accordingly to assigned values to these categories for the purpose of analysis [30].
We first used random-effects models to estimate the pooled RRs and 95%CIs for the healthiest versus the least-healthy combination of LBs and CVD incidence, mortality in general population, and CVD recurrence, CVD mortality, or all-cause mortality among individuals with CVD. We calculated study-specific slopes (linear trends) and 95% CIs from the natural logs of the reported RRs and CIs across categories of combination of LBs by using the method of Greenland [31] and the random-effects model to pool the study-specific dose-response effect estimates [32]. Study-specific effect estimates were calculated per 1 healthy LB increament. Only studies with at least three levels of combination of LBs and one point assigned to each healthy LB of the binary categories were included in the dose-response analysis.
Heterogeneity was tested by Cochran Q and I2 statistics [33]. A p < 0.10 was considered statistically significant for the Q statistic. By using a cut-off of 0.10, the issue of the Q statistic being less effective in detecting true heterogeneity was addressed, and it also helped to reduce the risk of committing a type II error [34]. I2 values of approximately 25%, 50%, and 75% were considered to reflect low, moderate, and high heterogeneity, respectively. Prespecified subgroup analyses and meta-regression by sub-types of outcomes, continent, sex, follow-up year, average age, factors included in LB score (smoking, alcohol drinking, physical activity, diet, and body weight), adjustments for age, economic level, and educational level were performed to access potential sources of heterogeneity. We also performed the sensitivity analyses by removing one study at a time to evaluate the robustness of the summary estimate. Egger’s test and funnel plot were both used to detect any evidence of publication bias for each meta-analysis [35]. In case significant publication bias was detected, we used the trim and fill method to make the adjustments [36]. Subgroup analyses, sensitivity analyses, and publication bias assessments were not conducted if there were fewer than 8 cohort comparisons available.
All analyses were performed using Stata 14.0 (Stata Corp, College Station, TX, USA). All tests were two-sided, with P < 0.05 considered statistically significant.
Results
Literature search and study characteristics
Literature search processes are summarized in Fig. 1. We identified 35,727 potential eligible articles. After removing duplicate articles (n = 6,699) and conducting titles or abstracts screening (n = 29,028), 364 articles were retrieved for critical full-text review. Finally, an overview of 61 articles (a total of 71 studies: 29 on CVD incidence, 36 on CVD mortality in general population; 2 on CVD recurrence, 1 CVD mortality, and 3 all-cause mortality among individuals with CVD) was included in the meta-analysis, representing a total of 6,163,255 participants with the average age ranged from 26.5 to 72 years. Among these articles, 2 articles reporting data from various cohorts [37, 38], 2 reporting different regions [39, 40], and 6 reporting different outcomes [16, 18, 19, 41,42,43], were treated as independent studies. The sample size of the cohorts ranged from 388 to 903,499, and the duration of follow-up ranged from 2.4 to 37 years. Geographically, 22 studies were conducted in Asia [15, 17, 19, 40, 44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60], 25 in Europe [8, 9, 16, 38, 40, 43, 61,62,63,64,65,66,67,68,69,70,71,72,73,74,75], and 24 in the United States [11, 37, 39, 41, 76,77,78,79,80,81,82,83,84,85,86,87]. 24 studies combined 5 or more main LBs [11, 18, 19, 37, 44,45,46, 48, 54, 58, 59, 61, 63,64,65, 68, 72, 76,77,78, 82, 85, 86, 88], and 60 studies reported that combinations of LBs had at least 3 levels and each LB was assigned a score, which meet the inclusion criteria for dose–response analyses [8, 9, 11, 15,16,17,18,19, 37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52, 55,56,57,58,59,60, 62, 63, 65,66,67,68, 70, 71, 73,74,75, 78,79,80,81, 86,87,88,89]. Table 1 shows the main characteristics of the included studies and Supplemental Tables 2–4 in Additional file 2 show the definition and categories of LBs. The mean (range) quality score was 7.07, assessed using the Newcastle-Ottawa Scale for cohort studies (See Supplemental Table 5 in Additional file 2).

Flowchart of article selection for the meta-analysis
Association of LBs with incident CVD in general population
Twenty-nine studies (2,523,034 participants and 189,733 cases) reported results comparing participants with the healthiest vs. least-healthy combination of LBs. The pooled RR and 95% CI was 0.42 (0.37–0.48), with high heterogeneity found (I2 = 92.5%, Pheterogeneity < 0.001; Fig. 2). Publication bias was detected using Egger’s test (P < 0.05). The trim-and-fill method was then conducted to adjust for the asymmetry, which weakened the protection effect but left the direction unchanged (RR: 0.62; 95% CI: 0.55–0.71; See Supplemental Fig. 1A in Additional file 2). Data from twenty-three studies (2,321,706 participants and 144,067 cases) were included in the dose-response analysis of LBs and CVD. The pooled RR was 0.83 (95% CI, 0.80–0.85) with per 1 healthy LB increment, with significant heterogeneity (I2 = 96.2%, Pheterogeneity < 0.001; Fig. 3). We detected statistically significant publication bias by Egger’s test (P < 0.05), with application of the trim and fill method, the protection effect did not change (RR: 0.90; 95% CI: 0.87–0.92; See Supplemental Fig. 1B in Additional file 2).

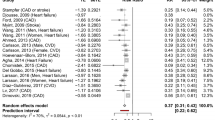
Forest plot of pooled relative risk for CVD with the healthiest versus the least-healthy combination of LBs

Forest plot for the pooled association between per 1 healthy LB increment and CVD
Considering the high heterogeneity across the included studies, we carried out meta-regression and subgroup analyses to explore the potential sources of heterogeneity. Meta-regression indicating that sex, adjustment for economic level and educational level may explain the high heterogeneity across studies in the healthiest vs. least-healthy combination of LBs (all Pregression<0.05; See Supplemental Table 6 in Additional file 2), and factors included in LB score with or without alcohol drinking (Pregression = 0.005) may the source of heterogeneity in the dose-response relationship analysis (See Supplemental Table 7 in Additional file 2). In overall, stable effects were observed in most of the subgroups except for studies conducted in MI (RR: 0.36; 95% CI: 0.10–1.27) and not included diet in LB score (RR: 0.36; 95% CI: 0.07–1.93) which showed that there were no associations in the healthiest vs. least-healthy combination of LBs analysis, and study not included diet in LB score (RR: 0.94; 95% CI: 0.84–1.05) also showed no association in the dose-response relationship analysis (See Supplemental Tables 6–7 in Additional file 2). The pooled estimates remained significant and stable when sensitivity analyses were performed after removing one study at a time (See Supplemental Figs. 2–3 in Additional file 2).
Association of LBs with CVD mortality in general population
Figure 4 shows the association between LBs and CVD mortality, with a total of 3,197,553 participants and 68,211 cases. Compared with individuals with the least-healthy combination of LBs, those with the healthiest had a 55% lower risk of CVD mortality (RR 0.45, 95%CI: 0.39–0.51; I2 = 94.4%, Pheterogeneity < 0.001). Publication bias was observed by the asymmetrical funnel plot and Egger’s test, but the result was not altered after using the trim- and- fill method to adjust for publication bias (RR: 0.45; 95% CI: 0.39–0.52; See Supplemental Fig. 4A in Additional file 2). 31 studies were included in the dose–response analysis of LBs and CVD mortality with 2,785,902 participants and 56,034 cases (Fig. 5). The pooled RR per 1 healthy LBs increment was 0.81 (95% CI: 0.78–0.84; I2 = 96.2%, Pheterogeneity < 0.001). No publication bias was detected by the funnel plot (See Supplemental Fig. 4B in Additional file 2) and Egger’s test (P = 0.375).

Forest plot of pooled relative risk for CVD mortality with the healthiest versus the least healthy combination of LBs

Forest plot for the pooled association between per 1 healthy LB increment and CVD mortality
Meta-regression and subgroup analyses were conducted to explore the potential sources of heterogeneity. Meta-regression indicating that adjustment educational level may explain the high heterogeneity across studies in the healthiest vs. least-healthy combination of LBs, and continent and factors included in combination of LBs with or without smoking may the additional source of heterogeneity in the dose-response relationship analysis (all Pregression<0.05; See Supplemental Tables 8–9 in Additional file 2). The findings from subgroup analyses generally supported the overall findings of the study. However, it is worth noting that the subgroup analysis for studies that did not include smoking in combination with LBs showed no significant association between LBs and CVD mortality in the analysis comparing the healthiest versus least-healthy combination of LBs (RR: 0.63; 95% CI: 0.38–1.05) (See Supplemental Tables 8–9 in Additional file 2). The pooled estimates remained significant and stable when sensitivity analyses were performed after removing one study at a time (See Supplemental Figs. 5–6 in Additional file 2).
Association between LBs and prognosis among individuals with CVD
Supplemental Fig. 7 in Additional file 2 shows the associations between LBs and CVD recurrence, CVD mortality, and all-cause mortality among individuals with CVD. The pooled RRs comparing participants with the healthiest versus the least-healthy combination of LBs were 0.38 (95%CI: 0.25–0.58; I2 = 0.0%, Pheterogeneity =1.000; 4,890 participants and 623 cases) for CVD recurrence and 0.33 (95%CI: 0.15–0.71; I2 = 86.4%, Pheterogeneity = 0.001; 465,609 participants and 13,551 cases) for all-cause mortality. In the dose-response analysis of LBs and prognosis among individuals with CVD, the pooled RRs with per 1 healthy LB increase were 0.73 (95%CI: 0.66–0.80; I2 = 0.0%, Pheterogeneity =0.608) for CVD recurrence and 0.73 (95%CI: 0.59–0.90; I2 = 92.1%, Pheterogeneity <0.001) for all-cause mortality among individuals with CVD (See Supplemental Fig. 8 in Additional file 2). Due to the limited number of studies on CVD recurrence and all-cause mortality, the corresponding meta-regression, subgroup analyses, sensitivity analyses, and publication bias assessments were not performed in the current meta-analysis. In addition, it is noteworthy that only one study reported the association of LBs and CVD mortality among participants diagnosed with CVD and hence the pooled RR could not be performed. In this study [18], individuals exhibiting the healthiest combination of LBs demonstrated a remarkable 92% reduction in the risk of CVD mortality compared to those with the least-healthy combination of LBs. Furthermore, each incremental increase in healthy LBs corresponded to a 47% decrease in the risk of CVD mortality.
Discussion
The current meta-analysis gathered a total of 29 prospective cohort studies to examine the association between combination of LBs and CVD, 36 studies between LBs and CVD mortality. Meanwhile, 6 prospective cohort studies were gathered to examine the association of LBs and prognosis of individuals with CVD (2 on CVD recurrence, 1 on CVD mortality, and 3 on all-cause mortality). We provided comprehensive and quantitative estimates for the associations between LBs and CVD, CVD mortality, as well as adverse outcomes in CVD individuals after adjustment for confounding factors.
This study indicated that, individuals with the healthiest combination of LBs would have a 58% and 55% lower risk of incident CVD and CVD mortality, respectively. With per 1 healthy LBs increment, the risk of CVD and CVD mortality are decreased by 17% and 19%, respectively. The associations were consistent among populations with most diverse socioeconomic backgrounds and baseline characteristics. Moreover, adopting a healthy LB was associated with a 62% and 67% lower risk of CVD recurrence and all-cause mortality among individuals diagnosed with CVD. Additionally, for each incremental increase in healthy LBs, the risk of CVD recurrence and all-cause mortality decreased by 27% and 27%, respectively.
There has not been a meta-analytical synthesis of LBs with the risk of CVD, CVD mortality, and the prognosis of individuals with CVD to date, though several meta-analyses addressed the associations between lifestyle indices and the risk of CVD and mortality. One meta-analysis comprising five LBs (physical activity, smoking, diet, alcohol consumption, and body weight) [90] reported consistent results with our study. It was found that a healthy LB was associated with a reduced risk of 66% for CVD, 60% for stroke, and 69% for HF. Another meta-analysis concluded that adopting the healthy lifestyle was associated with a 62% and 58% reduced risk for CVD and CVD mortality, and a 55–71% lower risk of multiple subtypes of CVDs [91]. Unlike to previous articles included metabolic factors such as blood lipids and blood glucose, our meta-analysis included prospective cohort studies purely on LBs. Additionally, our meta-analysis confirmed the benefits of each additional healthy LB increament in lowering the risk of CVD, CVD mortaliy, and adverse outcomes among individuals with CVD. Obviously, the current meta-analysis for the first time represented the comprehensively quantitative correlations between LBs and CVD and the prognosis of the clinical treatment of CVD.
In order to identify potential sources of heterogeneity, we conducted meta regression and various subgroup analyses on the relationships between LBs and CVD and CVD mortality. The results were consistent with the overall findings across different age groups, genders, geographic regions, and adjustment for age, ecomomic level, and educational level, which may have important public health implications, suggesting that people with different demographic characteristics can obtain health benefits by adopting LBs to achieve the purpose of preventing CVD. Evidence found here implied that primary health care service providers should prioritize the assessment of LBs in lowering the risk of CVD [92].
Educational level was found to be an important confounder in the relationship between LB and CVD morbidity and mortality. Slightly different risk relative reductions were found in studies between adjusted and unadjusted educational levels of the current meta-analysis. In general, the population with lower level of education showed worse adherence to healthy LBs. While the causes remain controversial, a significant proportion of previous studies have suggested that poor health awareness and a lack of awareness among individuals may be related to the observed correlations [51]. The inclusion of alcohol consumption as a LB in the LB score could potentially contribute to the high heterogeneity observed in the analysis. It is worth noting that the heterogeneity in subgroups that did not include alcohol consumption as a LB was lower than the overall heterogeneity in the context of CVD.
Correlations were not found between LBs and MI based on the included three prospective cohort studies, including Ford, E. S. et al. (2009) [69], Akesson, A. et al. (2014) [64], and Zuo, Y. et al. (2022) [15]. According to the included study by Cardi, M. et al. (2009) [81], a meaningful finding was concluded that LBs showed no association with CVD when diet was not included into the combinations. The possible reason is that a small number of studies are included, which may have been underpowered to detect associations with adverse outcomes [16, 93].
Our study also added important evidence to a clinical issue that patients with CVD can also benefit from LBs. The findings showed that LBs contribute more protection to individuals with CVD than general population. Participants with the healthiest combination of LBs were related to a reduced of 62% for CVD recurrence and 67% for all-cause mortality among individuals with CVD. Meanwhile, the risk of CVD and CVD mortality in the general population decreased by 58% and 55%, respectively. The risk reductions indicated that LBs modifications are still meaningful and should be recommended for individuals with CVD. As shown in the study by Jeong et al. (2019) [94], individuals with CVD may benefit more from physical activities than the group without CVD. Re-understanding and evaluation of the potential value of LBs in the clinical treatment of CVD, basing on more clinical randomized controlled trials or large-scale prospective cohort studies, has become an urgent task for the global response to the increasing incidence and disease burden of CVD.
Our findings suggest that each additional healthy LB is associated with reductions ranging from 17 to 27% in risk of CVD, CVD mortality, and prognosis. Several other studies have reported the dose-response relationship between LBs and CVD and its prognosis [16, 17, 37, 42, 95]. In a study based on two large prospective Study (Nurses’ Health Study and Health Professionals Follow-up Study; n = 121,700), there was a 20% stepwise risk reduction of CVD mortality for each additional healthy LB over 27 follow-up years [96]. Besides, our results also show that the protective effect of the healthiest combination of LBs on CVD and its prognosis is greater compared to individuals with least-healthy combination of LBs. For the individuals with the best quantified combination of LBs, CVD risk was reduced by 58%, CVD mortality was reduced by 55%, and the risk of poor prognosis was reduced by 62–67%, compared with the rest of the population. At the same time, for each additional LB, the risk of CVD decreased by 17%, CVD mortality decreased by 19%, and the risk of CVD poor prognosis decreased by around 27%, respectively. This indicates that the healthiest combination of multiple LBs has a more significant protective effect than simply strengthening a LB.
How LBs affect CVD and its poor prognosis has been partially revealed by some previously published studies. According Warburton, D. E. R. et al. (2017) [97], Lloyd-Price, J. et al. (2016) [98], and Jha, P. et al. (2014) [99], physical activity reduce the risk of chronic diseases through lowering blood pressure, blood sugar and cholesterol. Diet matters with the immune system and metabolic function by affecting the intestinal flora. While smoking increases the risk of adverse outcomes through genetic mutations has been confirmed.
Strengths and limitations
This is the first systematic review and meta-analysis to summarise the existing dose-response relationships between LBs and CVD in general population, as well as the risk of recurrence, mortality and all-cause mortality among individuals with CVD. Compared to the previous meta-analysis, this study confirmed for the first time that the combination of multiple healthy LBs has a more significant protective effect than simply strengthening a LB. Meanwhile, the constructions of lifestyle scores varied across studies, but this study only included articles containing LBs and did not involve any biochemical attributes such as blood lipids, blood glucose and so on. These LBs are closely related to the primary prevention of CVD and the management of its prognosis and are more conducive to basic public health service providers to assess the level of healthy lifestyles in the population and clinicians to develop comprehensive healthy lifestyle intervention strategies for patients.
There are several limitations in the current meta-analysis that have to be acknowledged. First, the study obtained a limited number of prospective cohort studies available specifically focusing on the prognosis of individuals with CVD. This limitation hindered our ability to perform further stratified analyses and examine the potential effects of LBs on improving the poor prognosis of CVD. Second, the LBs in all included studies were self-reported, meaning the validity of the study may be limited as it can be argued that the data represent only a collection of memories or subjective perceptions of lifestyle behaviors. Third, it should be noted that there is always the variability in the selection of confounding variables for adjustment across different studies. This variations in the choice and inclusion of confounders may have introduced residual confounding, which could not be completely ruled out. However, we conducted subgroup analysis based on whether common confounding factors were adjusted, and found that the most results were consistent with the main findings. Fourth, it is essential to acknowledge that the distinguishment of the priority of different LBs and the establishment of specific thresholds or ranges for each LB were not feasible due to the unavailability of individual-level original data. Instead, all LBs are treated to have equally significant contributions and the division of thresholds or ranges relies exclusively on the definitions provided by the respective authors of the included studies. It is noteworthy that these methodologies align with established practices observed in prior meta-analyses in the same research domain100–102. Lastly, it is important to acknowledge that there was moderate to high statistical heterogeneity observed in most of the analyses. Previous evidence has shown that there is substantial heterogeneity in the estimation of correlation in most analyses. We performed meta regression and subgroup analysis to explore the sources of heterogeneity, the findings suggest that the composition of LBs, confounding factors of adjustment and sub-types of outcomes may be the potential sources of heterogeneity.
Conclusions
LBs are associated with substantial risk reduction in CVD, CVD mortality, and adverse outcomes among individuals with CVD. Meanwhile, the combination of multiple healthy LBs has a more significant protective effect on CVD compared to merely focusing on strengthening a single LB. Multiple LBs, instead of tackling one certain LB, should be recommended for the prevention and management of CVD. With the growing incidence and burden of CVD globally, there is an urgent need to pay more attention to the role of LBs in individuals with CVD in the future, providing evidence for the prevention and clinical treatment of adverse outcomes in patients with CVD.
Data availability
Data (including the extracted contents from the searched articles) are available upon reasonable request from Dr. Yifei Feng; mail: fengyifei2019@163.com.
Abbreviations
- CVD:
-
Cardiovascular disease
- CHD:
-
Coronary heart disease
- CI:
-
Confidence interval
- HF:
-
Heart failure
- HR:
-
Hazard ratio
- IHD:
-
Ischemic heart disease
- LB:
-
Lifestyle behavior
- MI:
-
Myocardial infarction
- OR:
-
Odds ratio
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PROSPERO:
-
Prospective Register of Systematic Reviews
- RR:
-
Relative risk
References
World Health Organization. Cardiovascular diseases (CVDs). 2021. https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds).Accessed 27 May 2023.
Global. burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet (London, England). 2020;396(10258):1223-49.
Roth GA, Johnson CO, Abate KH, Abd-Allah F, Ahmed M, Alam K, et al. The Burden of Cardiovascular diseases among US States, 1990–2016. JAMA Cardiol. 2018;3(5):375–89.
Anand S, Bradshaw C, Prabhakaran D. Prevention and management of CVD in LMICs: why do ethnicity, culture, and context matter? BMC Med. 2020;18(1):7.
Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. Global Burden of Cardiovascular diseases and Risk factors, 1990–2019: Update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021.
World Heart Federation. Economic cost of cardiovascular disease. 2021. https://www.world-heart-federation.org/resources/economic-cost-of-cardiovascular-disease. Accessed 3 Jun 2023.
Kaminsky LA, German C, Imboden M, Ozemek C, Peterman JE, Brubaker PH. The importance of healthy lifestyle behaviors in the prevention of cardiovascular disease. Prog Cardiovasc Dis. 2022;70:8–15.
Khaw KT, Wareham N, Bingham S, Welch A, Luben R, Day N. Combined impact of health behaviours and mortality in men and women: the EPIC-Norfolk prospective population study. PLoS Med. 2008;5(1):e12.
Kvaavik E, Batty GD, Ursin G, Huxley R, Gale CR. Influence of individual and combined health behaviors on total and cause-specific mortality in men and women: the United Kingdom health and lifestyle survey. Arch Intern Med. 2010;170(8):711–8.
Petersen KE, Johnsen NF, Olsen A, Albieri V, Olsen LK, Dragsted LO, et al. The combined impact of adherence to five lifestyle factors on all-cause, cancer and cardiovascular mortality: a prospective cohort study among Danish men and women. Br J Nutr. 2015;113(5):849–58.
Li Y, Pan A, Wang DD, Liu X, Dhana K, Franco OH, et al. Impact of healthy lifestyle factors on life expectancies in the US Population. Circulation. 2018;138(4):345–55.
Kris-Etherton PM, Sapp PA, Riley TM, Davis KM, Hart T, Lawler O. The dynamic interplay of Healthy Lifestyle Behaviors for Cardiovascular Health. Curr Atheroscler Rep. 2022;24(12):969–80.
Eckel RH, Jakicic JM, Ard JD, de Jesus JM, Houston Miller N, Hubbard VS, et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice guidelines. J Am Coll Cardiol. 2014;63(25 Pt B):2960–84.
Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart disease and stroke statistics–2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29–322.
Zuo Y, Li H, Chen S, Tian X, Mo D, Wu S, et al. Joint association of modifiable lifestyle and metabolic health status with incidence of cardiovascular disease and all-cause mortality: a prospective cohort study. Endocrine. 2022;75(1):82–91.
Heath L, Jebb SA, Aveyard P, Piernas C. Obesity, metabolic risk and adherence to healthy lifestyle behaviours: prospective cohort study in the UK Biobank. BMC Med. 2022;20(1):65.
Yang YL, Leu HB, Yin WH, Tseng WK, Wu YW, Lin TH, et al. Adherence to healthy lifestyle improved clinical outcomes in coronary artery disease patients after coronary intervention. J Chin Med Assoc. 2021;84(6):596–605.
Towfighi A, Markovic D, Ovbiagele B. Impact of a healthy lifestyle on all-cause and cardiovascular mortality after stroke in the USA. J Neurol Neurosurg Psychiatry. 2012;83(2):146–51.
Han Y, Hu Y, Yu C, Guo Y, Pei P, Yang L, et al. Lifestyle, cardiometabolic disease, and multimorbidity in a prospective Chinese study. Eur Heart J. 2021;42(34):3374–84.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Beller EM, Glasziou PP, Altman DG, Hopewell S, Bastian H, Chalmers I et al. PRISMA for Abstracts: reporting systematic reviews in journal and conference abstracts. PLoS medicine. 2013;10(4):e1001419.
Lloyd-Jones DM, Allen NB, Anderson CAM, Black T, Brewer LC, Foraker RE, et al. Life’s essential 8: updating and enhancing the American Heart Association’s construct of Cardiovascular Health: a Presidential Advisory from the American Heart Association. Circulation. 2022;146(5):e18–43.
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–5.
Byrne DW, Rolando LA, Aliyu MH, McGown PW, Connor LR, Awalt BM, et al. Modifiable healthy lifestyle behaviors: 10-Year Health outcomes from a Health Promotion Program. Am J Prev Med. 2016;51(6):1027–37.
Orsini N, Li R, Wolk A, Khudyakov P, Spiegelman D. Meta-analysis for linear and nonlinear dose-response relations: examples, an evaluation of approximations, and software. Am J Epidemiol. 2012;175(1):66–73.
Han M, Qie R, Shi X, Yang Y, Lu J, Hu F, et al. Cardiorespiratory fitness and mortality from all causes, cardiovascular disease and cancer: dose-response meta-analysis of cohort studies. Br J Sports Med. 2022;56(13):733–9.
Zhang J, Yu KF. What’s the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. JAMA. 1998;280(19):1690–1.
Bekkering GE, Harris RJ, Thomas S, Mayer AM, Beynon R, Ness AR, et al. How much of the data published in observational studies of the association between diet and prostate or bladder cancer is usable for meta-analysis? Am J Epidemiol. 2008;167(9):1017–26.
Hamling J, Lee P, Weitkunat R, Ambühl M. Facilitating meta-analyses by deriving relative effect and precision estimates for alternative comparisons from a set of estimates presented by exposure level or disease category. Stat Med. 2008;27(7):954–70.
Hartemink N, Boshuizen HC, Nagelkerke NJ, Jacobs MA, van Houwelingen HC. Combining risk estimates from observational studies with different exposure cutpoints: a meta-analysis on body mass index and diabetes type 2. Am J Epidemiol. 2006;163(11):1042–52.
Greenland S. Dose-response and trend analysis in epidemiology: alternatives to categorical analysis. Epidemiol (Cambridge Mass). 1995;6(4):356–65.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–88.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Hardy RJ, Thompson SG. Detecting and describing heterogeneity in meta-analysis. Stat Med. 1998;17(8):841–56.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–34.
Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000;56(2):455–63.
Guasch-Ferré M, Li Y, Bhupathiraju SN, Huang T, Drouin-Chartier J-P, Manson JE, et al. Healthy lifestyle score including Sleep Duration and Cardiovascular Disease Risk. Am J Prev Med. 2022;63(1):33–42.
Larsson SC, Tektonidis TG, Gigante B, Akesson A, Wolk A. Healthy lifestyle and risk of Heart failure: results from 2 prospective cohort studies. Circ Heart Fail. 2016;9(4):e002855.
Warren Andersen S, Zheng W, Sonderman J, Shu XO, Matthews CE, Yu D, et al. Combined impact of Health behaviors on Mortality in Low-Income americans. Am J Prev Med. 2016;51(3):344–55.
Taheri S, Eriksen A, Tillin T, O’Connor L, Brage S, Hughes A et al. The impact of Health behaviours on Incident Cardiovascular Disease in europeans and South asians – a prospective analysis in the UK SABRE Study. PLoS ONE. 2015;10(3).
Lee CD, Sui X, Blair SN. Combined effects of cardiorespiratory fitness, not smoking, and normal waist girth on morbidity and mortality in men. Arch Intern Med. 2009;169(22):2096–101.
Booth JN 3rd, Levitan EB, Brown TM, Farkouh ME, Safford MM, Muntner P. Effect of sustaining lifestyle modifications (nonsmoking, weight reduction, physical activity, and mediterranean diet) after healing of myocardial infarction, percutaneous intervention, or coronary bypass (from the REasons for Geographic and racial differences in Stroke Study). Am J Cardiol. 2014;113(12):1933–40.
Hoevenaar-Blom MP, Spijkerman AM, Kromhout D, Verschuren WM. Sufficient sleep duration contributes to lower cardiovascular disease risk in addition to four traditional lifestyle factors: the MORGEN study. Eur J Prev Cardiol. 2014;21(11):1367–75.
Yang R, Lv J, Yu C, Guo Y, Bian Z, Han Y, et al. Importance of healthy lifestyle factors and ideal cardiovascular health metrics for risk of heart failure in Chinese adults. Int J Epidemiol. 2022;51(2):567–78.
Tsai M-C, Yeh T-L, Hsu H-Y, Hsu L-Y, Lee C-C, Tseng P-J et al. Comparison of four healthy lifestyle scores for predicting cardiovascular events in a national cohort study. Sci Rep. 2021;11(1).
Lv J, Yu C, Guo Y, Bian Z, Yang L, Chen Y, et al. Adherence to healthy Lifestyle and Cardiovascular diseases in the Chinese Population. J Am Coll Cardiol. 2017;69(9):1116–25.
Wang T, Ding C, Zhou W, Zhu L, Yu C, Huang X, et al. Associations of combined lifestyle behaviors with all-cause and cardiovascular mortality in adults: a population-based cohort study in Jiangxi Province of China. Front Public Health. 2022;10:942113.
Hu P, Zheng M, Huang J, Fan HY, Fan CJ, Ruan HH, et al. Effect of healthy lifestyle index and lifestyle patterns on the risk of mortality: a community-based cohort study. Front Med (Lausanne). 2022;9:920760.
Kim S, Kang H. Impact of behavioral risk factors on Mortality Risk in older Korean Women. Iran J Public Health. 2022;51(1):105–14.
Liu G, Xie Z, Pang Y, Huang T, Huang Y. Association between 4-dimension lifestyle pattern and 10-year mortality risk in Chinese individuals older than 65: a population-based cohort study. Aging. 2021;13(6):8835–48.
Zhang X, Lu J, Wu C, Cui J, Wu Y, Hu A, et al. Healthy lifestyle behaviours and all-cause and cardiovascular mortality among 0.9 million Chinese adults. Int J Behav Nutr Phys Act. 2021;18(1):162.
Lee DH, Nam JY, Kwon S, Keum N, Lee JT, Shin MJ, et al. Lifestyle risk score and mortality in Korean adults: a population-based cohort study. Sci Rep. 2020;10(1):10260.
Wu MY, Wang JB, Zhu Y, Lu JM, Li D, Yu ZB, et al. Impact of individual and combined lifestyle factors on mortality in China: a Cohort Study. Am J Prev Med. 2020;59(3):461–8.
Zhu N, Yu C, Guo Y, Bian Z, Han Y, Yang L, et al. Adherence to a healthy lifestyle and all-cause and cause-specific mortality in Chinese adults: a 10-year prospective study of 0.5 million people. Int J Behav Nutr Phys Act. 2019;16(1):98.
Han C, Liu F, Yang X, Chen J, Li J, Cao J, et al. Ideal cardiovascular health and incidence of atherosclerotic cardiovascular disease among Chinese adults: the China-PAR project. Sci China Life Sci. 2018;61(5):504–14.
Zhang QL, Zhao LG, Zhang W, Li HL, Gao J, Han LH, et al. Combined impact of known lifestyle factors on total and cause-specific mortality among Chinese men: a prospective cohort study. Sci Rep. 2017;7(1):5293.
Fazel-Tabar Malekshah A, Zaroudi M, Etemadi A, Islami F, Sepanlou S, Sharafkhah M, et al. The Combined effects of healthy lifestyle behaviors on all-cause mortality: the Golestan Cohort Study. Arch Iran Med. 2016;19(11):752–61.
Eguchi E, Iso H, Tanabe N, Wada Y, Yatsuya H, Kikuchi S, et al. Healthy lifestyle behaviours and cardiovascular mortality among Japanese men and women: the Japan collaborative cohort study. Eur Heart J. 2012;33(4):467–77.
Odegaard AO, Koh WP, Gross MD, Yuan JM, Pereira MA. Combined lifestyle factors and cardiovascular disease mortality in Chinese men and women: the Singapore Chinese health study. Circulation. 2011;124(25):2847–54.
Nechuta SJ, Shu XO, Li HL, Yang G, Xiang YB, Cai H et al. Combined impact of lifestyle-related factors on total and cause-specific mortality among Chinese women: prospective cohort study. PLoS Med. 2010;7(9).
Mo M, Moller J, Laszlo KD, Liang Y. The joint effect between fetal growth and health behaviors on the risk of cardiovascular diseases in young adulthood. Ann Epidemiol. 2023;78:54–60.
Dimovski K, Orho-Melander M, Drake I. A favorable lifestyle lowers the risk of coronary artery disease consistently across strata of non-modifiable risk factors in a population-based cohort. BMC Public Health. 2019;19(1):1575.
Diaz-Gutierrez J, Ruiz-Canela M, Gea A, Fernandez-Montero A, Martinez-Gonzalez MA. Association between a healthy lifestyle score and the risk of Cardiovascular Disease in the SUN Cohort. Rev Esp Cardiol (Engl Ed). 2018;71(12):1001–9.
Akesson A, Larsson SC, Discacciati A, Wolk A. Low-risk diet and lifestyle habits in the primary prevention of myocardial infarction in men: a population-based prospective cohort study. J Am Coll Cardiol. 2014;64(13):1299–306.
Larsson SC, Akesson A, Wolk A. Healthy diet and lifestyle and risk of stroke in a prospective cohort of women. Neurology. 2014;83(19):1699–704.
Carlsson AC, Wandell PE, Gigante B, Leander K, Hellenius ML, de Faire U. Seven modifiable lifestyle factors predict reduced risk for ischemic cardiovascular disease and all-cause mortality regardless of body mass index: a cohort study. Int J Cardiol. 2013;168(2):946–52.
Wang Y, Tuomilehto J, Jousilahti P, Antikainen R, Mahonen M, Katzmarzyk PT, et al. Lifestyle factors in relation to heart failure among Finnish men and women. Circ Heart Fail. 2011;4(5):607–12.
Zhang Y, Tuomilehto J, Jousilahti P, Wang Y, Antikainen R, Hu G. Lifestyle factors on the risks of ischemic and hemorrhagic stroke. Arch Intern Med. 2011;171(20):1811–8.
Ford ES, Bergmann MM, Kröger J, Schienkiewitz A, Weikert C, Boeing H. Healthy living is the best revenge: findings from the European prospective investigation into Cancer and Nutrition-Potsdam study. Arch Intern Med. 2009;169(15):1355–62.
Myint PK, Luben RN, Wareham NJ, Bingham SA, Khaw KT. Combined effect of health behaviours and risk of first ever stroke in 20,040 men and women over 11 years’ follow-up in Norfolk cohort of European prospective investigation of Cancer (EPIC Norfolk): prospective population study. BMJ. 2009;338:b349.
Ibsen DB, Sogaard K, Sorensen LH, Olsen A, Tjonneland A, Overvad K, et al. Modifiable lifestyle recommendations and mortality in Denmark: a Cohort Study. Am J Prev Med. 2021;60(6):792–801.
Sotos-Prieto M, Ortola R, Ruiz-Canela M, Garcia-Esquinas E, Martinez-Gomez D, Lopez-Garcia E, et al. Association between the Mediterranean lifestyle, metabolic syndrome and mortality: a whole-country cohort in Spain. Cardiovasc Diabetol. 2021;20(1):5.
Lohse T, Faeh D, Bopp M, Rohrmann S, Swiss National Cohort Study G. Adherence to the cancer prevention recommendations of the World Cancer Research Fund/American Institute for Cancer Research and mortality: a census-linked cohort. Am J Clin Nutr. 2016;104(3):678–85.
Knoops KT, de Groot LC, Kromhout D, Perrin AE, Moreiras-Varela O, Menotti A, et al. Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European men and women: the HALE project. JAMA. 2004;292(12):1433–9.
Luoto R, Prättälä R, Uutela A, Puska P. Impact of unhealthy behaviors on cardiovascular mortality in Finland, 1978–1993. Prev Med. 1998;27(1):93–100.
Mao Z, Troeschel AN, Judd SE, Shikany JM, Levitan EB, Safford MM, et al. Association of an evolutionary-concordance lifestyle pattern score with incident CVD among black and white men and women. Br J Nutr. 2022;129(8):1405–14.
Chomistek AK, Chiuve SE, Eliassen AH, Mukamal KJ, Willett WC, Rimm EB. Healthy lifestyle in the primordial prevention of cardiovascular disease among young women. J Am Coll Cardiol. 2015;65(1):43–51.
Del Gobbo LC, Kalantarian S, Imamura F, Lemaitre R, Siscovick DS, Psaty BM, et al. Contribution of major lifestyle risk factors for Incident Heart failure in older adults: the Cardiovascular Health Study. JACC Heart Fail. 2015;3(7):520–8.
Agha G, Loucks EB, Tinker LF, Waring ME, Michaud DS, Foraker RE, et al. Healthy lifestyle and decreasing risk of heart failure in women: the women’s Health Initiative observational study. J Am Coll Cardiol. 2014;64(17):1777–85.
Ahmed HM, Blaha MJ, Nasir K, Jones SR, Rivera JJ, Agatston A, et al. Low-risk lifestyle, coronary calcium, cardiovascular events, and mortality: results from MESA. Am J Epidemiol. 2013;178(1):12–21.
Cardi M, Munk N, Zanjani F, Kruger T, Schaie KW, Willis SL. Health behavior risk factors across age as predictors of cardiovascular disease diagnosis. J Aging Health. 2009;21(5):759–75.
Kurth T, Moore SC, Gaziano JM, Kase CS, Stampfer MJ, Berger K, et al. Healthy lifestyle and the risk of stroke in women. Arch Intern Med. 2006;166(13):1403–9.
Troeschel AN, Byrd DA, Judd S, Flanders WD, Bostick RM. Associations of dietary and lifestyle inflammation scores with mortality due to CVD, cancer, and all causes among black and white American men and women. Br J Nutr. 2023;129(3):523–34.
Li Z, Gao Y, Byrd DA, Gibbs DC, Prizment AE, Lazovich D, et al. Novel dietary and lifestyle inflammation scores directly Associated with All-Cause, All-Cancer, and all-Cardiovascular Disease Mortality Risks among women. J Nutr. 2021;151(4):930–9.
Troeschel AN, Hartman TJ, Flanders WD, Akinyemiju T, Judd S, Bostick RM. A novel evolutionary-concordance lifestyle score is inversely associated with all-cause, all-cancer, and all-cardiovascular disease mortality risk. Eur J Nutr. 2021;60(6):3485–97.
McCullough ML, Patel AV, Kushi LH, Patel R, Willett WC, Doyle C et al. Following cancer prevention guidelines reduces risk of cancer, cardiovascular disease, and all-cause mortality. Cancer epidemiology, biomarkers & prevention: a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology. 2011;20(6):1089–97.
Mitchell JA, Bornstein DB, Sui X, Hooker SP, Church TS, Lee CD, et al. The impact of combined health factors on cardiovascular disease mortality. Am Heart J. 2010;160(1):102–8.
Ford ES, Zhao G, Tsai J, Li C. Low-risk lifestyle behaviors and all-cause mortality: findings from the National Health and Nutrition Examination Survey III Mortality Study. Am J Public Health. 2011;101(10):1922–9.
Bonaccio M, Di Castelnuovo A, Costanzo S, De Curtis A, Persichillo M, Cerletti C, et al. Impact of combined healthy lifestyle factors on survival in an adult general population and in high-risk groups: prospective results from the Moli-Sani Study. J Intern Med. 2019;286(2):207–20.
Barbaresko J, Rienks J, Nöthlings U. Lifestyle indices and Cardiovascular Disease Risk: a Meta-analysis. Am J Prev Med. 2018;55(4):555–64.
Zhang YB, Pan XF, Chen J, Cao A, Xia L, Zhang Y, et al. Combined lifestyle factors, all-cause mortality and cardiovascular disease: a systematic review and meta-analysis of prospective cohort studies. J Epidemiol Commun Health. 2021;75(1):92–9.
Williams MA, Kaminsky LA. Healthy Lifestyle Medicine in the Traditional Healthcare Environment-Primary Care and Cardiac Rehabilitation. Prog Cardiovasc Dis. 2017;59(5):448–54.
Hamer M, Stamatakis E. Metabolically healthy obesity and risk of all-cause and cardiovascular disease mortality. J Clin Endocrinol Metab. 2012;97(7):2482–8.
Jeong SW, Kim SH, Kang SH, Kim HJ, Yoon CH, Youn TJ, et al. Mortality reduction with physical activity in patients with and without cardiovascular disease. Eur Heart J. 2019;40(43):3547–55.
Zhu Z, Li FR, Jia Y, Li Y, Guo D, Chen J, et al. Association of Lifestyle with incidence of heart failure according to metabolic and genetic risk status: a Population-based prospective study. Circ Heart Fail. 2022;15(9):e009592.
Wang K, Li Y, Liu G, Rimm E, Chan AT, Giovannucci EL, et al. Healthy Lifestyle for Prevention of Premature Death among Users and nonusers of common preventive medications: a prospective study in 2 US cohorts. J Am Heart Assoc. 2020;9(13):e016692.
Warburton DER, Bredin SSD. Health benefits of physical activity: a systematic review of current systematic reviews. Curr Opin Cardiol. 2017;32(5):541–56.
Lloyd-Price J, Abu-Ali G, Huttenhower C. The healthy human microbiome. Genome Med. 2016;8(1):51.
Jha P, Peto R. Global effects of smoking, of quitting, and of taxing tobacco. N Engl J Med. 2014;370(1):60–8.
Acknowledgements
Not applicable.
Funding
This study was supported by the National Social Science Fund of China (grant number 21BGL222), Collaborative Innovation System Research on Drug Intervention&Non-drug Intervention in Proactive Health Context (20220518 A), the 2023 Graduate Independent Innovation Project of Zhengzhou University (No. 20230440) and Platform for Dynamic Monitoring and Comprehensive Evaluation of Healthy Central Plains Action (20220134B). The funder had no role in the conceptualization, design, data collection, analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
JW and YF developed the initial idea for the study, designed the scope, planned the methodological approach, and performed the meta-analysis. JW and YF coordinated the systematic review process, wrote the systematic review protocol, completed the PROSPERO registration, and extracted the data for further analysis. ZG, QZ, RL, and XZ defined the search strings, executed the search, exported the results, and removed duplicate records. XG and QL screened the abstracts and texts for the systematic review, extracted relevant data from the systematic review articles, and performed quality assessment. WS, LZ, MM, ZS, and YZ performed the data visualization. FY, BL, JG, CST, and YM contributed to critically revising the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
There was no human participant being recruited, no animals, tissues, cells, body fluid, or any living creatures being involved, therefore, no Institutional Review Board approval is necessary and no informed consent obtained.
Consent for publication
Not applicable.
Competing interests
The authors declare there are no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wu, J., Feng, Y., Zhao, Y. et al. Lifestyle behaviors and risk of cardiovascular disease and prognosis among individuals with cardiovascular disease: a systematic review and meta-analysis of 71 prospective cohort studies. Int J Behav Nutr Phys Act 21, 42 (2024). https://doi.org/10.1186/s12966-024-01586-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-024-01586-7