
Abstract
Background
Lifestyle behaviours related to smoking, alcohol, nutrition, and physical activity are leading risk factors for the development of chronic disease. For people in rural areas, access to individualised lifestyle services targeting behaviour change may be improved by using telehealth. However, the scope of literature investigating telehealth lifestyle behaviour change interventions for rural populations is unknown, making it difficult to ascertain whether telehealth interventions require adaptation for rural context via a systematic review. This scoping review aimed to address this gap, by mapping existing literature describing telehealth lifestyle interventions delivered to rural populations to determine if there is scope for systematic review of intervention effectiveness in this research topic.
Methods
The PRISMA extension for scoping review checklist guided the processes of this scoping review. A search of eight electronic databases reported in English language until June 2023 was conducted. Eligible studies included adults (18 years and over), who lived in rural areas of high-income countries and undertook at least one synchronous (video or phone consultation) telehealth intervention that addressed either addictive (smoking or alcohol), or non-addictive lifestyle behaviours (nutrition or physical activity). Studies targeting addictive and non-addictive behaviours were separated after full text screening to account for the involvement of addictive substances in smoking and alcohol studies that may impact behaviour change interventions described. Studies targeting nutrition and/or physical activity interventions are presented here.
Results
The search strategy identified 17179 citations across eight databases, with 7440 unique citations once duplicates were removed. Full texts for 492 citations were retrieved and screened for inclusion with 85 publications reporting on 73 studies eligible for data extraction and analysis. Of this, addictive behaviours were comprised of 15 publications from 13 studies. Non-addictive behaviours included 70 publications from 58 studies and are reported here. Most interventions were delivered within the United States of America (n = 43, 74.1%). The most common study design reported was Randomised Control Trial (n = 27, 46.6%). Included studies involved synchronous telehealth interventions targeting nutrition (11, 18.9%), physical activity (5, 8.6%) or nutrition and physical activity (41, 70.7%) and were delivered predominately via videoconference (n = 17, 29.3%).
Conclusions
Despite differences in intervention characteristics, the number of randomised control trials published suggests sufficient scope for future systematic reviews to determine intervention effectiveness related to nutrition and physical activity telehealth interventions for rural populations.
Trial registration
The scoping review protocol was not pre-registered.
Similar content being viewed by others


Background
Chronic diseases including cardiovascular disease, cancer, chronic respiratory disease, and diabetes are among the leading causes of morbidity and mortality worldwide [1]. Smoking, poor nutrition, at-risk alcohol consumption, and physical inactivity (SNAP) are key behavioural risk factors in the development of these chronic diseases and their reduction is listed as the third objective on the World Health Assembly’s WHO Global action plan for the prevention and control of Noncommunicable Diseases (NCDs) 2013–2020 [1,2,3]. Health behaviour change interventions are organized sets of activities designed to change specific health behaviours, such as SNAP behaviours [4]. Effective behaviour change interventions are often complex, and can target varying populations, communities, or individuals [4,5,6,7,8,9,10]. They can also incorporate different behaviour change techniques and methods of delivery depending on the intervention context [4,5,6,7,8,9,10]. This can make them challenging to replicate or implement across different contexts, such as between urban and rural areas [4].
People living in rural areas, defined broadly as any area outside of a major city, can experience unique challenges accessing health services and professionals that provide individualised behaviour change interventions as part of their routine care [10, 11]. Geographical distance impacts rural health worker recruitment and retention, resulting in a shortage of healthcare professionals in rural areas worldwide [12,13,14,15]. This shortage can result in increased travel distances for rural people accessing health services, higher cost of private services and longer wait times for public services [11, 15]. Challenges accessing healthcare services, in combination with lower socio-economic factors, contribute to the higher prevalence of risky lifestyle behaviours and overall poorer health outcomes experienced by rural populations compared to their metropolitan counterparts [11]. It is therefore important to understand how service models such as telehealth, which may be used to connect rural populations with healthcare providers, can be utilised to improve health behaviours, and overall health outcomes, in these populations.
Telehealth is defined as ‘delivery of health services, where distance is a critical factor, by health professionals using information and communication technologies (ICT)’ [16]. The term telehealth is often used interchangeably with telemedicine [17]. However telemedicine refers to the delivery of medical, diagnostic and treatment related services, usually by doctors, whilst telehealth includes a wider variety of remote healthcare services, including behaviour change interventions often delivered by allied health workers [17]. Telehealth has been consistently shown to be effective for healthcare delivery and has additional benefits for rural communities [18,19,20,21]. These benefits include improved access to and increased quality of clinical care, reduced overall cost of service delivery, reduced demand for emergency services, reduced travel time for both rural patients and health professionals, improved management of chronic and complex conditions, and improved professional development opportunities for rural staff which may contribute to improved rural medical workforce recruitment and retention [22,23,24,25].
Despite these benefits, uptake of telehealth into mainstream rural health service delivery has been slow [23]. Proposed barriers to implementation include initial cost of set up, [25] inconsistent government rebates for telehealth, [26] lack of education and training for clinicians, [24, 27, 28] limited knowledge of the changes in provider-patient interactions as a result of altered communication patterns, [29] lack of clinician skill with technology, and concerns with insurance and liability [19]. Additionally, clinicians, clients and service providers may view telehealth as a lesser service compared to face-to-face models [19].
Research into the implementation of telehealth into rural health services has largely focused on medical interventions in acute care settings [23]. A 2016 systematic review summarising currently published telehealth studies in rural Australia found nearly 60% (n = 41) of studies were for medical interventions alone and only 13% (n = 9) investigated intervention delivery by allied health professionals [23]. The type of allied health professionals delivering the interventions was not specified in the review nor was there any description of any behaviour change interventions provided [23]. To our knowledge there is no recent review scoping the literature on telehealth delivery of SNAP lifestyle interventions in rural areas.
The aim of this current scoping review is to begin to address this evidence gap, by summarising the characteristics of studies investigating synchronous telehealth interventions targeting two SNAP lifestyle behaviours of nutrition and physical activity for adults living in rural areas. The purpose of this is to contribute to understanding of the scope of studies in this area and provide a foundation for systematic review of intervention effectiveness in the future. In this review, nutrition and physical activity interventions have been separated from smoking and alcohol interventions due to acknowledgment that lifestyle behaviour change techniques may vary if the targeted behaviour involves an addictive substance (alcohol or smoking) or not (physical activity and nutrition) [4,5,6,7,8,9,10].
Objectives
To summarise the characteristics of studies investigating synchronous telehealth interventions targeting nutrition and physical activity behaviours in adults living in rural areas. This will include addressing the following questions:
-
1.
What is the scope of research describing nutrition and physical activity interventions delivered using telehealth to rural populations, including number of citations retrieved and their included interventions, reported publication date and study design?
-
2.
What are the characteristics of included interventions, including intervention settings, methods and reported outcomes?
-
3.
What theories are referenced in current literature, including implementation or behaviour change theories?
-
4.
Does the current body of literature contain enough homogenous study design to warrant systematic review?
Methods
Protocol and registration
The methods of this scoping review were guided by the PRISMA extension for scoping review checklist (Additional file 1) [30]. The scoping review protocol was not pre-registered.
Eligibility criteria
Studies eligible for inclusion during title/abstract screening included adult participants aged 18 years and over living in rural areas and involved a synchronous (video or phone consultation) telehealth intervention that addressed smoking and/or alcohol and/or physical activity and/or nutrition. Studies involving mHealth, defined by the World Health Organisation (WHO) as ‘medical and public health practice supported by mobile devices, such as mobile phones, patient monitoring devices, Personal Digital Assistants (PDAs), and other wireless devices’, and face-to-face interventions were included if they also had a synchronous phone or video telehealth component [31].
A comparator was not necessary for inclusion and all study designs except for systematic and scoping reviews were eligible. Studies were limited to high income countries as classified by the World Bank and all outcomes were considered [32].
‘Rural’ was defined by the included study authors and may have included but was not limited to descriptions such as ‘rural’, ‘regional’, ‘remote’ or ‘non-metropolitan’. This was to account for the lack of international definition of ‘rural’.
Studies were excluded if they were duplicates; were not in English; were not set in a high-income country; did not include a lifestyle intervention or a synchronous telehealth component; were not set in a rural area or present data from rural populations separately; were systematic/scoping reviews; included populations currently undergoing acute care treatment; included paediatric populations or were published outside of the included date range. This inclusion/exclusion criteria was re-applied to studies retrieved for full-text screening. Studies addressing smoking and/or alcohol were excluded after full text screening.
Information sources
Electronic databases searched included MEDLINE, EMBASE, COCHRANE, PSYCHINFO, SCOPUS, CINAHL, Web of Science and INFORMIT. A search of the reference lists of included articles and retrieved systematic reviews was also completed. All databases were searched up to June 2023.
Search strategy
The search strategy was developed by the research team and in consultation with the medical librarian. The search consisted of Medical Subject Headings (MeSH) and focussed keywords. MeSH terms included telemedicine, remote consultation, health behaviour, diet, diet therapy, nutrition therapy, eating, exercise, exercise therapy, physical therapy modalities, sedentary behaviour, alcohol drinking, tobacco smoking, smoking cessation, smoking reduction, smoking, obesity, obesity management, weight loss, diabetes mellitus type 2, cardiovascular diseases, chronic disease, rural health services, rural health, rural population, and regional health planning. The term telehealth was included under the telemedicine MeSH. The full MEDLINE search strategy can be found in Additional file 2.
Data management
All records were exported from databases into an endnote library and deduplicated. Remaining records were uploaded to Covidence (Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org) for additional de-duplication, abstract and full text screening.
Selection process
Two independent reviewers completed abstract and full text screening of all articles. Conflicts were discussed and resolved between independent reviewers or resolved by a third reviewer.
Data collection process
Data extraction was completed by one reviewer and checked by another. Variables collected for each study included study title, author, year of publication, study design, National Health and Medical Research Council (NHMRC) Evidence Hierarchy categorisation of study design, aim, setting (country of intervention delivery), rural definition provided, participant inclusion/exclusion criteria, lifestyle risk factor targeted, methods of intervention delivery, qualification of intervention facilitator, timing of intervention including number of telehealth consults, length of consults, and duration of the intervention, theory referenced, outcomes measured and whether there were statistically significant findings reported [33].
Data synthesis
Data relating to nutrition and physical activity behaviours will be summarised using descriptive statistics. Percentages will be calculated from the number of included studies when describing study design and intervention characteristics, and from the number of included publications when describing reported outcomes and theoretical frameworks referenced.
Results
Citation retrieval
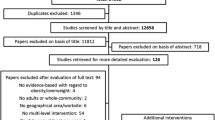
The search strategy identified 17179 citations across eight databases (Fig. 1). After duplication and title/abstract screening 500 citations were eligible for full text retrieval. Of these citations a total of 85 publications (n = 73 studies) were identified as eligible with 70 publications (n = 58 studies) identified for non-addictive behaviours (nutrition and physical activity) and 15 publications (n = 13 studies) for addictive behaviours (smoking and alcohol). The 15 publications (n = 13 studies) identified for smoking and alcohol were excluded at this stage and the characteristics of the 70 publications (n = 58 studies) for nutrition and physical activity are described here.

Map of the identification and screening of studies for review inclusion [32]. *SNAP: Smoking, Nutrition, Alcohol and Physical Activity. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. https://doi.org/10.1136/bmj.n71. For more information, visit: http://www.prisma-statement.org/
Publication dates
Included nutrition and/or physical activity records were published from 1999–2023, with 63 (90%) records published from 2010 onward and approximately a third (n = 22, 32.4%) records published since the COVID-19 pandemic from 2020 onward (see Additional files 3 and 4) [34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94].
Study design
Of the 58 included studies, Randomised Control Trial (RCT) was the most common study design (n = 27, 46.6%), [35, 37,38,39, 43,44,45, 52, 54,55,56, 58, 59, 61, 65, 69,70,71,72,73, 79,80,81, 95,96,97] followed by pre-post (n = 11, 19.0%) [50, 60, 63, 64, 66, 77, 78, 86, 98,99,100,101]. Study design of remaining studies included cohort (retrospective and prospective) (n = 7, 12.1%), [34, 36, 47, 48, 83,84,85, 88] single arm trial (n = 6, 10.3%), [40, 41, 46, 67, 82, 89, 92, 102, 103] case study (n = 3, 5.2%), [57, 104, 105] pseudo-RCT (n = 2, 3.4%), [42, 51] non-inferiority trial (n = 1, 1.7%) and qualitative (n = 1, 1.7%) [49, 76]. Study designs were categorised according to the NHMRC Evidence Hierarchy as level II (n = 27, 46.6%), level III study (n = 28, 50.9%), level IV (n = 14, 24.2%) or not at all (n = 1, 1.7%) see Additional files 3 and 5) [35, 37,38,39, 43,44,45, 49, 52, 54,55,56, 58, 59, 61, 65, 69,70,71,72,73, 79,80,81, 95,96,97].
Intervention characteristics
Intervention characteristics are summarised in Table 1, with additional information included in Additional file 3.
Settings
The majority of included studies were set in rural areas of the United States of America (USA) (n = 43, 74.1%), [34, 36, 37, 40,41,42,43,44,45,46,47,48, 51,52,53,54,55, 57,58,59, 62,63,64,65,66, 69,70,71, 73, 77,78,79,80,81,82, 86,87,88,89,90,91,92, 95,96,97, 100, 104, 105] with the remaining set in rural areas of Canada (n = 6, 11.5%), [35, 50, 60, 67, 68, 75, 76, 99] Australia (n = 6, 10.3%), [38, 39, 72, 74, 83,84,85, 93, 94] United Kingdom (UK) (n = 2, 3.4%), [49, 56] and Taiwan (n = 1, 1.7%) (see Additional files 3 and 6). [61] A definition of rurality was reported in 19 (32.8%) studies. [42,43,44, 46, 50, 52, 57,58,59,60, 67, 70, 75, 77, 78, 81, 85, 88, 92, 96, 97, 103] Nine studies (15.5%) used an official measure of rurality that was recognised by the country in which the study was conducted, and 10 studies (17.2%) reported an unofficial measure (see Additional files 6 and 7) [42,43,44, 46, 50, 52, 57, 58, 60, 67, 68, 70, 74, 75, 77, 78, 81, 85, 88, 92, 96, 97].
Intervention methods
Most study interventions (n = 41, 70.7%) targeted nutrition and physical activity simultaneously [34,35,36,37, 40,41,42,43,44, 46, 48,49,50,51,52, 54,55,56,57, 60, 62, 63, 65,66,67, 70,71,72,73,74, 76,77,78,79,80,81,82, 84,85,86,87,88,89,90,91,92,93,94,95, 99, 103]. Videoconference was the most popular method of telehealth intervention delivery. (n = 38, 65.5%) [34, 35, 40, 41, 43, 46,47,48,49,50,51,52,53,54, 57,58,59,60,61,62,63,64, 66, 67, 69, 71, 73, 75,76,77,78,79,80, 82, 86, 88, 91, 95, 99, 100, 103,104,105]. In some studies videoconference was used in conjunction with phone (n = 8, 13.7%), [35, 43, 49, 69, 73, 80, 104] face-to-face (9, 15.5%), [40, 41, 47, 50, 51, 61, 62, 66, 71, 82, 86, 95] phone plus face-to-face (n = 2, 3.3%), [52, 88] or a combination of phone and/or face to face and/or mHealth methods (n = 3, 5.2%) [84, 87, 89]. Telehealth delivery was reported as an adjunct to in-person delivery in n = 17 (29.3%) included studies [40, 41, 44, 47, 50,51,52, 61, 70, 71, 82, 84,85,86, 88, 93,94,95,96, 102, 106].
Most interventions included one-on-one delivery to individuals as the only intervention mode (n = 24, 41.4%), [36,37,38,39, 45, 47, 55,56,57,58,59, 64, 67, 72,73,74, 79,80,81, 84, 85, 87, 89, 91,92,93,94, 97, 100, 103, 104] or in combination with a group component (n = 17, 29.3%) [35, 40,41,42, 44, 48, 52, 62, 65, 66, 70, 71, 75, 95, 96, 105]. Most interventions (n = 49, 80.3%) were delivered by one or more health professionals or health/lifestyle coaches, [34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52, 55, 57,58,59, 61, 62, 64, 65, 67, 69, 70, 82, 84, 85, 87,88,89,90,91,92,93,94,95, 103,104,105] with the most utilised being dietitians (n = 26, 44.8%), [34, 35, 40,41,42,43,44,45,46,47,48,49, 52, 55, 57,58,59, 61, 64, 65, 71, 77,78,79, 82, 85, 88, 95, 104, 105] nurses (n = 16, 27.6%), [35,36,37, 47, 48, 52, 57,58,59, 61, 79, 80, 84, 85, 87, 88, 92,93,94, 96] and exercise professionals (either scientist or physiologists) (n = 11, 19%) [35, 44, 46,47,48, 51, 65, 71, 77, 85, 95].
The total number of telehealth consults delivered throughout included interventions ranged from a single session (n = 3, 4.9%), [63, 100, 106] to up to 78 sessions (n = 1, 1.7%) [40, 41]. The intervention that delivered 78 telehealth sessions included 26 weekly nutrition consultations and 52 bi-weekly telehealth exercise consultations delivered over a 26-week period [40, 41]. Twenty interventions delivered less than 10 consultations over the reported intervention period whilst 23 interventions delivered 10 consultations or more [36,37,38,39, 46, 50, 51, 56, 59,60,61, 63, 66, 72, 80, 82, 85,86,87,88,89,90,91,92, 94, 96, 100]. The frequency of delivery of 13 studies was not described, whilst three interventions were delivered at varied frequencies depending on patient preference [45, 47, 57, 59, 64, 69, 77,78,79, 83, 84, 93, 97, 101, 104, 105, 107]. Timing of telehealth consultations ranged from 15 min to 2 h with nutrition consultations generally shorter (15–60 min) and physical activity consultations generally longer (60–120 min).
Reported Outcomes
Many publications reported multiple primary outcomes (see Table 1). Primary outcomes related to participant behaviour change (n = 48, 68.6%); [36, 38,39,40,41,42, 45, 47,48,49,50,51,52,53,54,55,56,57, 59, 60, 62,63,64,65,66,67,68,69, 71, 72, 75, 77,78,79,80,81, 87,88,89,90,91,92,93, 95,96,97, 99] disease status (n = 13, 18.6%); [47, 51, 59, 61, 63, 73, 79, 87, 93, 96, 97] anthropometric markers (weight loss) (n = 40, 57.1%); [34, 36, 37, 40,41,42,43,44,45,46, 48, 51, 52, 54, 55, 58, 59, 61,62,63,64,65, 82, 87, 95] biochemistry (n = 26, 44.8%); [36, 44,45,46,47, 51, 52, 55, 58, 59, 61,62,63,64, 69, 71, 73, 74, 77,78,79, 88, 90, 93,94,95,96] intervention feasibility (n = 22, 31.4%); [35, 40, 41, 47, 50, 57, 64, 66,67,68, 83,84,85,86,87,88,89,90, 92, 99, 100] participant experience measured through qualitative methods (n = 7, 10%), [35, 49, 50, 53, 62, 76, 92], and cost-effectiveness (n = 2, 2.9%) [38, 43].
Reference to a theorical framework
Twenty-five publications (32.1%) referenced a theory, theoretical framework, or theoretical model in the description of the intervention methods (see Table 2) [37,38,39,40,41,42,43, 45, 49, 52, 55, 56, 66,67,68,69, 81, 83, 84, 86, 87, 89, 91, 92, 95]. Nine of these (12.5%) referenced more than one theory [40, 41, 45, 52, 55, 66, 81, 86, 89]. A total of ten theories were referenced with the most common theories relating to behaviour change. These included the social cognitive theory (n = 9), [37, 40,41,42,43, 55, 66, 86, 89] self-determination theory (n = 6), [37,38,39,40,41,42,43, 49, 55, 66,67,68, 86, 89] and trans-theoretical model of behaviour change (n = 5) [45, 52, 56, 69, 91].
Discussion
The aim of the current scoping review is to summarise the characteristics of studies investigating synchronous telehealth interventions targeting non-addictive, nutrition and physical activity behaviours in adults living in rural areas. The purpose of this was to increase understanding of the extent, range, and nature of studies in this area, and provide a foundation for systematic review of these studies in the future. Publications included in the current review were identified as a part of a larger database search which also included addictive behaviour interventions targeting smoking and alcohol behaviours in rural populations. However, studies reporting addictive behaviours were separated at data analysis to be reported independently, due to consideration of the varying behaviour change techniques that may be more effective in behaviours involving addictive substances [4,5,6,7,8,9,10]. Overall, this current scoping review included a substantial number of RCT’s (n = 27, 46.6%), highlighting that the current scope of research in this area warrants future systematic reviews to determine intervention effectiveness.
Of the many publications (n = 70, 58 studies) identified for inclusion in this review, the majority were published after 2010. The current review identified a proliferation of publications between 2020 and 2022. This increase coincides with the COVID-19 pandemic and demonstrates a shift toward telehealth research to meet the demands of physical distancing during the pandemic years [16]. There appears to be a drop in publications from 2022–2023, however, this may reflect the current review only including studies published before June 2023 (Additional file 4).
Only five of the 80 high-income countries were represented in the current review with the USA, Canada and Australia accounting for the highest proportion of published studies [32]. These countries are among the top 10 highest income countries in the world, and have large geographical distances between metropolitan and rural/remote areas. In particular, Canada and Australia both have very small populations per land mass (four and three people per square kilometre of land respectively) [32, 117]. As such, impetus, and availability of resources for adopting evidence-based telehealth services into healthcare delivery may drive a higher output of studies in these areas. However, this small number of represented countries highlights a limitation in the current scope of research and should be considered in future interpretations of study effectiveness and transferability across rural settings in different countries.
This review identified that a wide range of definitions of rurality were used by the included studies, which may result in varying population characteristics and rural settings [118]. In some studies, rurality was stated, but not defined, making it difficult to ascertain population characteristics or study settings. In studies that did provide a definition of rurality, only nine used an official definition of rurality recognised by the country of intervention setting. Within these nine studies, six varying official definitions of rurality are described [42,43,44, 46, 58, 59, 70, 74, 81, 97]. Such differences in definitions have been shown to result in a wide range of intervention contexts, including varying population characteristics such as education and poverty status, population density and access to health services [118]. The use of official measures of rurality in the design of future rural telehealth interventions will make identification of included population characteristics easier to understand and assist in transferability of intervention designs across contexts.
Included studies demonstrated key similarities across intervention characteristics. A large proportion of the included studies targeted nutrition and physical activity simultaneously. This is not surprising, given weight loss was a commonly reported outcomes of included studies, and improving dietary intake and physical activity are nationally recommended strategies for weight management [119,120,121,122].
Key differences identified across intervention characteristics included consultation lengths (ranging from 15 min to over 60 min), consultation frequencies (ranging from a single consultation up to 78 consultations) and combinations of delivery methods (telehealth alone or in combination with face-to-face or mHealth methods). There are currently no guidelines outlining optimum intervention intensity for nutrition and physical activity behaviour change interventions, nor is it clear whether telehealth interventions are more effective as a standalone or complimentary service to more traditional face-to-face models. A systematic review of reported outcomes stratified by intervention characteristics may identify which characteristics are more effective for nutrition and physical activity behaviour change.
While future systematic reviews are warranted, a potential limitation to consider is the inconsistent reporting of behaviour change outcomes across included studies. Despite all included studies describing the delivery of behaviour change interventions, only 40 studies (48 publications) reported behaviour change variables such as changes in diet or physical activity levels as a study outcome. This means the effectiveness of the behaviour change interventions on nutrition and physical activity levels in the remaining 18 studies (25 publications) cannot be assessed.
Approximately one third of included publications (n = 25) referenced a theoretical framework and most of these publications (n = 23) referenced theory related to behaviour change. Only two studies referenced an implementation theory, framework, or model, suggesting a lack of consideration of implementation science in current literature. This is a limitation of included studies, as implementation factors such as poor internet connectivity, cost of set-up and lack of healthcare professional telehealth training are cited as key barriers to the uptake of telehealth universally, not just in rural areas [24]. Use of implementation science can inform study design, ensuring implementation factors are considered across a diverse range of contexts [123]. This may be particularly relevant in a rural setting, where context can vary greatly, and implementation strategies need to be adaptable in order to sustain telehealth services [23].
Strengths
To our knowledge there are no other reviews summarising the scope of research investigating nutrition and physical activity interventions delivered using telehealth to adults living in rural areas. A previous systematic review published in 2016 synthesised literature on telehealth services in rural Australia and aimed to synthesise factors associated with successful and sustainable telehealth services [23]. Whilst it included a large number of articles (n = 116), only nine related to allied health and there was no distinction as to whether these services provided nutrition or physical activity interventions [23]. A more recent systematic review has described the effectiveness of telehealth individual video-conference interventions in reducing smoking, nutrition, alcohol, physical activity, and obesity risk factors in an adult population, and included RCTs from both metropolitan and rural areas [108]. However, of the included studies, only four were set in rural locations, and only two were related to physical activity and none were related to nutrition [108]. The current scoping review is the first to summarise current literature on this topic and lays a foundation for future systematic reviews on this topic in the future.
Limitations
A scoping review study design can result in the identification of a large volume of literature; however, the quality of evidence is not appraised. Furthermore, a scoping review design does not synthesise outcomes to assess intervention effectiveness. The search strategy of this scoping review was limited to studies in the English language and only included interventions that were published. It is likely that many other synchronous telehealth physical activity and nutrition services exist in practise, but have not been published [23]. Lastly, there were many studies that included a synchronous telehealth nutrition and/or physical activity intervention in areas that may have included a rural population, however, the results of these studies were not stratified by rurality. Studies that did not stratify by rurality were not included as it was impossible to ascertain whether they included the target population.
Conclusion
The current scoping review summarised literature on telehealth nutrition and/or physical activity interventions delivered to adults living in rural areas of high-income countries. A large volume of literature was identified and included a predicted spike in intervention numbers coinciding with the COVID-19 pandemic. Included studies were largely from rural areas of the USA, with definitions of rurality varying across studies. This may result in variation across what is defined as a rural context, and comparison between study outcomes in the future difficult. Whilst study designs varied, the current review identified 27 published RCTs for physical activity and nutrition, providing a strong foundation for future systematic review of study quality, outcomes, and overall intervention effectiveness. Reported outcomes stratified by intervention characteristics (e.g., length, frequency, and mode of delivery) may identify which telehealth delivery method is most effective for rural populations. Lastly, there is limited reference to implementation or behaviour change theories in the included intervention designs. This indicates an area of potential improvement in future intervention study design of telehealth interventions targeting improved nutrition and physical activity levels in rural populations.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
World Health Organisation. Noncommunicable Diseases 2023. Available from: https://www.who.int/health-topics/noncommunicable-diseases#tab=tab_1.
World Health Organisation. Global action plan for the prevention and control of noncommunicable diseases. Geneva: WHO Press; 2013.
World Health Organisation. Implementation roadmap 2023–2030 for the Global action plan for the prevention and control of NCDs 2013–2030 2023 [cited 2023 23/03/2023]. Available from: https://www.who.int/teams/noncommunicable-diseases/governance/roadmap.
Araújo-Soares V, Hankonen N, Presseau J, Rodrigues A, Sniehotta FF. Developing Behavior Change Interventions for Self-Management in Chronic Illness: An Integrative Overview. Eur Psychol. 2019;24(1):7–25.
Howlett N, García-Iglesias J, Bontoft C, Breslin G, Bartington S, Freethy I, et al. A systematic review and behaviour change technique analysis of remotely delivered alcohol and/or substance misuse interventions for adults. Drug Alcohol Depend. 2022;239: 109597.
Black N, Johnston M, Michie S, Hartmann-Boyce J, West R, Viechtbauer W, et al. Behaviour change techniques associated with smoking cessation in intervention and comparator groups of randomized controlled trials: a systematic review and meta-regression. Addiction. 2020;115(11):2008–20.
Samdal GB, Eide GE, Barth T, Williams G, Meland E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int J Behav Nutr Phys Act. 2017;14(1):42.
Michie S, Whittington C, Hamoudi Z, Zarnani F, Tober G, West R. Identification of behaviour change techniques to reduce excessive alcohol consumption. Addiction. 2012;107(8):1431–40.
Fergie L, Campbell KA, Coleman-Haynes T, Ussher M, Cooper S, Coleman T. Identifying effective behavior change techniques for alcohol and illicit substance use during pregnancy: a systematic review. Ann Behav Med. 2019;53(8):769–81.
Keyworth C, Epton T, Goldthorpe J, Calam R, Armitage CJ. Delivering opportunistic behavior change interventions: a systematic review of systematic reviews. Prev Sci. 2020;21(3):319–31.
Russell D, Mathew S, Fitts M, Liddle Z, Murakami-Gold L, Campbell N, et al. Interventions for health workforce retention in rural and remote areas: a systematic review. Hum Resour Health. 2021;19(1):103.
McCormack LA, Meendering JR, Burdette L, Prosch N, Moore L, Stluka S. Quantifying the Food and Physical Activity Environments in Rural, High Obesity Communities. Int J Environ Res Public Health. 2021;18(24):13344.
Australian Institute of Health and Welfare. Rural & remote health: Australian Government; 2019. Available from: https://www.aihw.gov.au/reports/rural-health/rural-remote-health/contents/rural-health.
Lancet T. Rural health inequities: data and decisions. Lancet. 2015;385(9980):1803.
Cosgrave C, Malatzky C, Gillespie J. Social Determinants of Rural Health Workforce Retention: A Scoping Review. Int J Environ Res Public Health. 2019;16(3):314.
Monaghesh E, Hajizadeh A. The role of telehealth during COVID-19 outbreak: a systematic review based on current evidence. BMC Public Health. 2020;20(1):1193.
Commission. FC. Telehealth, telemedicine, and telecare: What's what? 2023 [Available from: https://www.fcc.gov/general/telehealth-telemedicine-and-telecare-whats-what#:~:text=Telehealth.
Kelly JT, Reidlinger DP, Hoffmann TC, Campbell KL. Telehealth methods to deliver dietary interventions in adults with chronic disease: a systematic review and meta-analysis. Am J Clin Nutr. 2016;104(6):1693–702.
Speyer R, Denman D, Wilkes-Gillan S, Chen YW, Bogaardt H, Kim JH, et al. Effects of telehealth by allied health professionals and nurses in rural and remote areas: A systematic review and meta-analysis. J Rehabil Med. 2018;50(3):225–35.
Ekeland AG, Bowes A, Flottorp S. Effectiveness of telemedicine: a systematic review of reviews. Int J Med Inform. 2010;79(11):736–71.
World Health Organization. Telemedicine: opportunities and developments in Member States. Geneva: WHO; 2009.
Moffatt JJ, Eley DS. The reported benefits of telehealth for rural Australians. Aust Health Rev. 2010;34(3):276–81.
Bradford N, Caffery L, Smith A. Telehealth services in rural and remote Australia: a systematic review of models of care and factors influencing success and sustainability. 2016.
Almathami HKY, Win KT, Vlahu-Gjorgievska E. Barriers and facilitators that influence telemedicine-based, real-time, online consultation at patients’ homes: systematic literature review. J Med Internet Res. 2020;22(2): e16407.
Rollo ME, Burrows T, Vincze LJ, Harvey J, Collins CE, Hutchesson MJ. Cost evaluation of providing evidence-based dietetic services for weight management in adults: In-person versus eHealth delivery. Nutr Diet. 2018;75(1):35–43.
Wade V, Soar J, Gray L. Uptake of telehealth services funded by Medicare in Australia. Aust Health Rev. 2014;38(5):528–32.
Edirippulige S, Armfield NR. Education and training to support the use of clinical telehealth: A review of the literature. J Telemed Telecare. 2017;23(2):273–82.
Campbell J, Theodoros D, Hartley N, Russell T, Gillespie N. Implementation factors are neglected in research investigating telehealth delivery of allied health services to rural children: A scoping review. J Telemed Telecare. 2020;26(10):590–606.
Henry BW, Block DE, Ciesla JR, McGowan BA, Vozenilek JA. Clinician behaviors in telehealth care delivery: a systematic review. Adv Health Sci Educ Theory Pract. 2017;22(4):869–88.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018;169(7):467–73.
World Health Organisation. mHealth programmes are sponsored by government 2023 Available from: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/4774.
The World Bank Group. High Income 2023. Available from: https://data.worldbank.org/country/XD.
Merlin T, Weston A, Tooher R. Extending an evidence hierarchy to include topics other than treatment: revising the Australian’levels of evidence’. BMC Med Res Methodol. 2009;9(1):1–8.
Ahrendt AD, Kattelmann KK, Rector TS, Maddox DA. The effectiveness of telemedicine for weight management in the MOVE! Program J Rural Health. 2014;30(1):113–9.
Banner D, Kandola D, Bates J, Horvat D, Ignaszewski A, Singer J, et al. Patient experiences of undertaking a virtual cardiac rehabilitation program. Can J Cardiovasc Nurs. 2019;29(2):6–14.
Barker K, Mallow J, Theeke L, Schwertfeger R. A telehealth rural practice change for diabetes education and management. The Journal for Nurse Practitioners. 2016;12(5):e225–9.
Barnason S, Zimmerman L, Schulz P, Pullen C, Schuelke S. Weight management telehealth intervention for overweight and obese rural cardiac rehabilitation participants: A randomised trial. J Clin Nurs. 2019;28(9–10):1808–18.
Barrett S, Begg S, O’Halloran P, Kingsley M. Cost-effectiveness of telephone coaching for physically inactive ambulatory care hospital patients: economic evaluation alongside the Healthy4U randomised controlled trial. BMJ Open. 2019;9(12): e032500.
Barrett S, Begg S, O’Halloran P, Kingsley M. Integrated motivational interviewing and cognitive behaviour therapy can increase physical activity and improve health of adult ambulatory care patients in a regional hospital: the Healthy4U randomised controlled trial. BMC Public Health. 2018;18(1):1–11.
Batsis JA, McClure AC, Weintraub AB, Kotz DF, Rotenberg S, Cook SB, et al. Feasibility and acceptability of a rural, pragmatic, telemedicine-delivered healthy lifestyle programme. Obes Sci Pract. 2019;5(6):521–30.
Batsis JA, Petersen CL, Clark MM, Cook SB, Kotz D, Gooding TL, et al. Feasibility and acceptability of a technology-based, rural weight management intervention in older adults with obesity. BMC geriatr. 2021;21(1):44.
Befort CA, Donnelly JE, Sullivan DK, Ellerbeck EF, Perri MG. Group versus individual phone-based obesity treatment for rural women. Eat Behav. 2010;11(1):11–7.
Befort CA, Klemp JR, Sullivan DK, Shireman T, Diaz FJ, Schmitz K, et al. Weight loss maintenance strategies among rural breast cancer survivors: The rural women connecting for better health trial. Obesity (Silver Spring). 2016;24(10):2070–7.
Befort CA, VanWormer JJ, Desouza C, Ellerbeck EF, Gajewski B, Kimminau KS, et al. Effect of behavioral therapy with in-clinic or telephone group visits vs in-clinic individual visits on weight loss among patients with obesity in rural clinical practice: a randomized clinical trial. JAMA. 2021;325(4):363–72.
Benson GA, Sidebottom A, Hayes J, Miedema MD, Boucher J, Vacquier M, et al. Impact of ENHANCED (diEtitiaNs Helping pAtieNts CarE for Diabetes) Telemedicine Randomized Controlled Trial on Diabetes Optimal Care Outcomes in Patients with Type 2 Diabetes. J Acad Nutr Diet. 2019;119(4):585–98.
Brown JD, Hales S, Evans TE, Turner T, Sword DO, O’Neil PM, et al. Description, utilisation and results from a telehealth primary care weight management intervention for adults with obesity in South Carolina. J Telemed Telecare. 2020;26(1–2):28–35.
Ciemins E, Coon P, Peck R, Holloway B, Min SJ. Using telehealth to provide diabetes care to patients in rural Montana: findings from the promoting realistic individual self-management program. Telemed J E Health. 2011;17(8):596–602.
Ciemins EL, Coon PJ, Coombs NC, Holloway BL, Mullette EJ, Dudley WN. Intent-to-treat analysis of a simultaneous multisite telehealth diabetes prevention program. BMJ open diabetes res. 2018;6(1): e000515.
Cliffe M, Di Battista E, Bishop S. Can you see me? Participant experience of accessing a weight management programme via group videoconference to overcome barriers to engagement. Health Expect. 2021;24(1):66–76.
Dal Bello-Haas VP, O’Connell ME, Morgan DG, Crossley M. Lessons learned: feasibility and acceptability of a telehealth-delivered exercise intervention for rural-dwelling individuals with dementia and their caregivers. Rural Remote Health. 2014;14(3):2715.
Dalleck LC, Schmidt LK, Lueker R. Cardiac rehabilitation outcomes in a conventional versus telemedicine-based programme. J Telemed Telecare. 2011;17(5):217–21.
Davis RM, Hitch AD, Salaam MM, Herman WH, Zimmer-Galler IE, Mayer-Davis EJ. TeleHealth improves diabetes self-management in an underserved community: diabetes TeleCare. Diabetes Care. 2010;33(8):1712–7.
Elder AJS, Scott WS, Kluge MA, Elder CL. CyberEx internet-based group exercise for rural older adults: a pilot study. Act Adapt Aging. 2016;40(2):107–24.
Fazzino TL, Fabian C, Befort CA. Change in Physical Activity During a Weight Management Intervention for Breast Cancer Survivors: Association with Weight Outcomes. Obesity (Silver Spring). 2017;25(Suppl 2):S109–15.
Foley P, Levine E, Askew S, Puleo E, Whiteley J, Batch B, et al. Weight gain prevention among black women in the rural community health center setting: the Shape Program. BMC Public Health. 2012;12:305.
Gillham S, Endacott R. Impact of enhanced secondary prevention on health behaviour in patients following minor stroke and transient ischaemic attack: a randomized controlled trial. Clin Rehabil. 2010;24(9):822–30.
Holloway B, Coon PJ, Kersten DW, Ciemins EL. Telehealth in rural Montana: promoting realistic independent self-management of diabetes. Diabetes Spectrum. 2011;24(1):50–4.
Homenko DR, Morin PC, Eimicke JP, Teresi JA, Weinstock RS. Food insecurity and food choices in rural older adults with diabetes receiving nutrition education via telemedicine. J Nutr Educ Behav. 2010;42(6):404–9.
Izquierdo R, Lagua CT, Meyer S, Ploutz-Snyder RJ, Palmas W, Eimicke JP, et al. Telemedicine intervention effects on waist circumference and body mass index in the IDEATel project. Diabetes Technol Ther. 2010;12(3):213–20.
Jaglal SB, Haroun VA, Salbach NM, Hawker G, Voth J, Lou W, et al. Increasing access to chronic disease self-management programs in rural and remote communities using telehealth. Telemed J E Health. 2013;19(6):467–73.
Liou JK, Soon MS, Chen CH, Huang TF, Chen YP, Yeh YP, et al. Shared care combined with telecare improves glycemic control of diabetes patients in a rural, underserved community. J Diabetes Sci Technol. 2013;7(1):A82.
Schepens Niemiec SL, Vigen CLP, Martinez J, Blanchard J, Carlson M. Long-Term Follow-Up of a Lifestyle Intervention for Late-Midlife, Rural-Dwelling Latinos in Primary Care. Am J Occup Ther. 2021;75(2):7502205020 p1-p11.
Nuovo J. The impact of a diabetes self-management education program provided through a telemedicine link to rural california health care clinics. Health Serv Insights. 2013;6(6):1–7.
Olfert MD, Barr ML, Hagedorn RL, Long DM, Haggerty TS, Weimer M, et al. Feasibility of a mHealth Approach to Nutrition Counseling in an Appalachian State. J. 2019;9(4):20.
Perri MG, Shankar MN, Daniels MJ, Durning PE, Ross KM, Limacher MC, et al. Effect of telehealth extended care for maintenance of weight loss in Rural US communities: a randomized clinical trial. JAMA Netw Open. 2020;3(6): e206764.
Porter KJ, Moon KE, LeBaron VT, Zoellner JM. A novel behavioral intervention for rural appalachian cancer survivors (weSurvive): participatory development and proof-of-concept testing. JMIR Cancer. 2021;7(2): e26010.
Price J, Brunet J. Feasibility and acceptability of a telehealth behavior change intervention for promoting physical activity and fruit and vegetable consumption among rural-living young adult cancer survivors. J Psychosoc Oncol. 2021;39(6):715–33.
Price J, Brunet J. The Potential of Telehealth Interventions for Health Behaviour Change Among Rural-Living Young Adult Cancer Survivors. J SportExer Psychol. 2020;42:S101.
Prochaska JJ, Epperson A, Skan J, Oppezzo M, Barnett P, Delucchi K, et al. The Healing and Empowering Alaskan Lives Toward Healthy-Hearts (HEALTHH) Project: Study protocol for a randomized controlled trial of an intervention for tobacco use and other cardiovascular risk behaviors for Alaska Native People. Contemp Clin Trials. 2018;71:40–6.
Radcliff TA, Bobroff LB, Lutes LD, Durning PE, Daniels MJ, Limacher MC, et al. Comparing costs of telephone vs face-to-face extended-care programs for the management of obesity in rural settings. J Acad Nutr Diet. 2012;112(9):1363–73.
Rickel KA, Milsom VA, Ross KM, Hoover VJ, Peterson ND, Perri MG. Differential response of African American and Caucasian women to extended-care programs for obesity management. Ethn Dis. 2011;21(2):170–5.
Sangster J, Furber S, Allman-Farinelli M, Phongsavan P, Redfern J, Haas M, et al. Effectiveness of a pedometer-based telephone coaching program on weight and physical activity for people referred to a cardiac rehabilitation program: a randomized controlled trial. J Mol Signal. 2015;35(2):124–9.
Siminerio L, Ruppert K, Huber K, Toledo FG. Corrigendum. Diabetes Educ. 2015;41(6):778.
Ski CF, Vale MJ, Bennett GR, Chalmers VL, McFarlane K, Jelinek VM, et al. Improving access and equity in reducing cardiovascular risk: the Queensland Health model. Med J Aust. 2015;202(3):148–52.
Stickland M, Jourdain T, Wong EY, Rodgers WM, Jendzjowsky NG, Macdonald GF. Using Telehealth technology to deliver pulmonary rehabilitation in chronic obstructive pulmonary disease patients. Can Respir J. 2011;18(4):216–20.
Taylor DM, Stone SD, Huijbregts MP. Remote participants’ experiences with a group-based stroke self-management program using videoconference technology. Rural Remote Health. 2012;12:1947.
Vadheim LM, McPherson C, Kassner DR, Vanderwood KK, Hall TO, Butcher MK, et al. Adapted diabetes prevention program lifestyle intervention can be effectively delivered through telehealth. Diabetes Conference: 70th Scientific Sessions of the American Diabetes Association Orlando, FL United States Conference Publication. 2010.
Vadheim LM, Patch K, Brokaw SM, Carpenedo D, Butcher MK, Helgerson SD, et al. Telehealth delivery of the diabetes prevention program to rural communities. Transl Behav Med. 2017;7(2):286–91.
West SP, Lagua C, Trief PM, Izquierdo R, Weinstock RS. Goal setting using telemedicine in rural underserved older adults with diabetes: experiences from the informatics for diabetes education and telemedicine project. Telemed J E Health. 2010;16(4):405–16.
Young H, Miyamoto S, Ward D, Dharmar M, Tang-Feldman Y, Berglund L. Sustained effects of a nurse coaching intervention via telehealth to improve health behavior change in diabetes. Telemed J E Health. 2014;20(9):828–34.
Zoellner JM, You W, Estabrooks PA, Chen Y, Davy BM, Porter KJ, et al. Supporting maintenance of sugar-sweetened beverage reduction using automated versus live telephone support: findings from a randomized control trial. Int J Behav Nutr Phys Act. 2018;15(1):97.
Batsis JA, Shirazi D, Petersen CL, Roderka MN, Lynch D, Jimenez D, et al. Changes in body composition in older adults after a technology-based weight loss intervention. J Frality Aging. 2022;11(2):151–5.
Beleigoli A, Champion S, Tirimacco R, Nesbitt K, Tideman P, Clark RA. A co-designed telehealth-based model of care to improve attendance and completion to cardiac rehabilitation of rural and remote Australians: The Country Heart Attack Prevention (CHAP) project. J Telemed Telecare. 2021;27(10):685–90.
Beleigoli A, Nicholls SJ, Brown A, Chew DP, Beltrame J, Maeder A, et al. Implementation and prospective evaluation of the Country Heart Attack Prevention model of care to improve attendance and completion of cardiac rehabilitation for patients with cardiovascular diseases living in rural Australia: A study protocol. BMJ Open. 2022;12(2):e054558.
Champion S, Clark RA, Tirimacco R, Tideman P, Gebremichael L, Beleigoli A. The Impact of the SARS-CoV-2 Virus (COVID-19) pandemic and the rapid adoption of telehealth for cardiac rehabilitation and secondary prevention programs in rural and remote australia: a multi-method study. Heart Lung Circ. 2022;31(11):1504–12.
Dennett AM, Hirko KA, Porter KJ, Loh KP, Liao Y, Yang L, et al. Embedding lifestyle interventions into cancer care: has telehealth narrowed the equity gap? J Natl Cancer Inst Monogr. 2023;2023(61):133–9.
Johansson P, Rowland SA, Schulz PS, Struwe L, Hebert L, Brueggemann G, et al. Cardiovascular disease risk in rural adults a pilot intervention study using registered nurse/community health worker teams. J Cardiovasc Nurs. 2023;38(3):262–71.
Ladner KA, Berry SR, Hardy J. Increasing access to diabetes education in rural Alabama through telehealth. Am. 2022;122(9):39–47.
Li S, Yin Z, Lesser J, Li C, Choi BY, Parra-Medina D, et al. Community Health Worker-Led mHealth-Enabled Diabetes Self-management Education and Support Intervention in Rural Latino Adults: Single-Arm Feasibility Trial. JMIR Diabetes. 2022;7(2):e37534.
O’Neal LJ, Perri MG, Befort C, Janicke DM, Shankar MN, Bauman V, et al. Differential impact of telehealth extended-care programs for weight-loss maintenance in African American versus white adults. J Behav Med. 2022;45(4):580–8.
Oppezzo M, Knox M, Skan J, Chieng A, Crouch M, Aikens RC, et al. Traditional heart-healthy diet and medication adherence in the Norton Sound Region: an 18-month telehealth intervention. Int J Environ Res Public Health. 2022;19(16):14.
Price J, Brunet J. Understanding rural-living young adult cancer survivors’ motivation during a telehealth behavior change intervention within a single-arm feasibility trial. Health Inform J. 2022;28(1):14604582221075560.
Yiallourou SR, Carrington MJ. Improved sleep efficiency is associated with reduced cardio-metabolic risk: Findings from the MODERN trial. J Sleep Res. 2021;30(6):e13389.
Carrington MJ, Zimmet P. Nurse health and lifestyle modification versus standard care in 40 to 70 year old regional adults: study protocol of the Management to Optimise Diabetes and mEtabolic syndrome Risk reduction via Nurse-led intervention (MODERN) randomized controlled trial. BMC Health Serv Res. 2017;17(1):813.
Perri MG, Limacher MC, Durning PE, Janicke DM, Lutes LD, Bobroff LB, et al. Extended-care programs for weight management in rural communities: the treatment of obesity in underserved rural settings (TOURS) randomized trial. Arch Intern Med. 2008;168(21):2347–54.
Skelly AH, Carlson J, Leeman J, Soward A, Burns D. Controlled trial of nursing interventions to improve health outcomes of older African American women with type 2 diabetes. Nurs Res. 2009;58(6):410–8.
Tessaro I, Rye S, Parker L, Mangone C, McCrone S. Effectiveness of a nutrition intervention with rural low-income women. Am J Health Behav. 2007;31(1):35–43.
Taylor DM, Cameron JI, Walsh L, McEwen S, Kagan A, Streiner DL, et al. Exploring the feasibility of videoconference delivery of a self-management program to rural participants with stroke. Telemed J E Health. 2009;15(7):646–54.
Stiles N, Boosalis M, Thompson K, Stinnett D, Rayens MK. Nutrition telemedicine consultation for rural elders. J Nutr Elder. 1999;18(1):47–55.
Levy CE, Silverman E, Jia H, Geiss M, Omura D. Effects of physical therapy delivery via home video telerehabilitation on functional and health-related quality of life outcomes. J Rehabil Res Dev. 2015;52(3):361–70.
Niemiec SLS, Vigen CLP, Martinez J, Blanchard J, Carlson M. Long-Term Follow-Up of a Lifestyle Intervention for Late-Midlife, Rural-Dwelling Latinos in Primary Care. Am J Occup Ther. 2021;75(2):1–11.
Price J, Brunet J. Telehealth coaching for rural-living young adult cancer survivors: A protocol. Health Educ J. 2019;79(2):212–24.
Johnson A, Gorman M, Lewis C, Baker F, Coulehan N, Rader J. Interactive videoconferencing improves nutrition intervention in a rural population. J Am Diet Assoc. 2001;101(2):173–4.
McCabe BJ, Copeland NP, Shull CA, Dictson KD. Telehealth and Telenutrition. J Nutr Elder. 2001;21(2):73–84.
Wang Y, Lombard C, Hussain SM, Harrison C, Kozica S, Brady SRE, et al. Effect of a low-intensity, self-management lifestyle intervention on knee pain in community-based young to middle-aged rural women: a cluster randomised controlled trial. Arthritis Res Ther. 2018;20(1):74.
Siminerio L, Ruppert K, Huber K, Toledo FG. Telemedicine for Reach, Education, Access, and Treatment (TREAT): linking telemedicine with diabetes self-management education to improve care in rural communities. Diabetes Educ. 2014;40(6):797–805.
The World Bank Group. Population Density: The World Bank Group; 2023. Available from: https://data.worldbank.org/indicator/EN.POP.DNST.
Bandura A. Social cognitive theory of personality. Handbook of personality. 1999;2:154–96.
Deci EL, Ryan RM. Self-determination theory in health care and its relations to motivational interviewing: a few comments. Int J Behav Nutr Phys Act. 2012;9:24.
Silva P. Davis' technology acceptance model (TAM)(1989). Information seeking behavior and technology adoption: Theories and trends. 2015:205–19.
Becker MH. The health belief model and personal health behavior. Health Educ Monogr. 1974;2:324–473.
Prochaska JO, Velicer WF. The transtheoretical model of health behavior change. Am J Health Promot. 1997;12(1):38–48.
Glasgow RE, Klesges LM, Dzewaltowski DA, Estabrooks PA, Vogt TM. Evaluating the impact of health promotion programs: using the RE-AIM framework to form summary measures for decision making involving complex issues. Health Educ Res. 2006;21(5):688–94.
Kanfer FH, Goldstein AP. Helping people change: A textbook of methods: Pergamon Press; 1991.
Czajkowski SM, Powell LH, Adler N, Naar-King S, Reynolds KD, Hunter CM, et al. From ideas to efficacy: The ORBIT model for developing behavioral treatments for chronic diseases. Health Psychol. 2015;34(10):971–82.
Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211.
Long JC, Delamater PL, Holmes GM. Which definition of rurality should i use?: the relative performance of 8 federal rural definitions in identifying rural-urban disparities. Med Care. 2021;59(Suppl 5):S413–9.
Cornier MA. A review of current guidelines for the treatment of obesity. Am J Manag Care. 2022;28(15 Suppl):S288–96.
National Institute of Health and Care Excellence. Obesity: identification, assessment and management. In: Excellence NIoHaC, editor. United Kingdom: National Institute of Health and Care Excellence; 2014.
Wharton S, Lau DCW, Vallis M, Sharma AM, Biertho L, Campbell-Scherer D, et al. Obesity in adults: a clinical practice guideline. CMAJ. 2020;192(31):E875–91.
National Health and Medical Research Council. Clinical practice guidelines for the management of overweight and obesity in adults, adolescents, and children in Australia. In: Health Do, editor. Melbourne: National Health and Medical Research Council 2013.
Moullin JC, Dickson KS, Stadnick NA, Albers B, Nilsen P, Broder-Fingert S, et al. Ten recommendations for using implementation frameworks in research and practice. Implement Sci Commun. 2020;1(1):42.
Byaruhanga J, Atorkey P, McLaughlin M, Brown A, Byrnes E, Paul C, et al. Effectiveness of individual real-time video counseling on smoking, nutrition, alcohol, physical activity, and obesity health risks: systematic review. J Med Internet Res. 2020;22(9): e18621.
Acknowledgements
University of Newcastle Librarian Nicole Faull-Brown assisted in design of initial search strategy and translation of search strategy across databases. Research assistant Kee June Ooi assisted with title/abstract screen, full text retrieval and screen, and data extraction.
Funding
PhD candidate JH scholarship funded by the Medical Research Futures Fund. CEC is supported by a National Health and Medical Research Council of Australia Leadership (L3) Research Fellowship (APP2009340). Funding agencies had no role in this review.
Author information
Authors and Affiliations
Contributions
All authors contributed to inception of scoping review question. JH designed initial search in collaboration with co-authors TS, LB and CC. JH conducted initial search of databases, and was second reviewer for abstract/full text screen and data extraction. JH completed data analysis and prepared initial manuscript draft and all authors review subsequent drafts and approved final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
Clare Collins is deputy editor of the International Journal of Behavioural Nutrition and Physical Activity. There are no other conflicts to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Preferred Reporting Items for Systematic reviews and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR) Checklist.PRISMA checklist outlining page numbers of completed sections in manuscript.
Additional file 2.
Medline search strategy and initial results for current scoping review.Medline search strategy and initial results for current scoping review presented in table format.
Additional file 3.
Characteristics of included studies. Summary table describing the extracted characteristics of each included study.
Additional file 4.
Number of studies and year of publication since 1999. Visual representation of number of studies published each year since 1999.
Additional file 5.
Classification of included studies into National Health and Medical Research Council (NHMRC) categories.
Additional file 6.
Measure of rurality provided per country of intervention setting. Bar graph describing the measure of rurality provided per country, and distinguishing whether the measure was official or unofficial.
Additional file 7.
Official measure of rurality featured in included studies. Description of the official measures of rurality referenced in included studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Herbert, J., Schumacher, T., Brown, L.J. et al. Delivery of telehealth nutrition and physical activity interventions to adults living in rural areas: a scoping review. Int J Behav Nutr Phys Act 20, 110 (2023). https://doi.org/10.1186/s12966-023-01505-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-023-01505-2