
Abstract
Objectives
We investigated associations between leisure-time physical activity (LTPA) at different intensities (moderate and vigorous or moderate-to-vigorous) and prospective weight gain in non-obese people. We also examined whether these associations were independent of other lifestyle factors and changes in muscle mass and whether they were age-dependent and changed over a person’s life course.
Methods
The data were extracted from the Lifelines cohort study (N = 52,498; 43.5% men) and excluded obese individuals (BMI > 30 kg/m2). We used the validated SQUASH questionnaire to estimate moderate-to-vigorous (MVPA; MET≥4), moderate (MPA; MET between 4 and 6.5) and vigorous PA (VPA; MET≥6.5). Body weight was objectively measured, and changes were standardized to a 4-year period. Separate analyses, adjusted for age, educational level, diet, smoking, alcohol consumption and changes in creatinine excretion (a marker of muscle mass), were performed for men and women.
Results
The average weight gain was + 0.45 ± 0.03 kg in women. Relative to each reference groups (No-MVPA, No-MPA and No-VPA), MVPA (Beta (95%CI): − 0.34 kg (− 0.56;-0.13)), MPA (− 0.32 kg (− 0.54;-0.10)) and VPA (− 0.30 kg (− 0.43;-0.18)) were associated with less gain in body weight in women after adjusting for potential confounders, described above. These associations were dose-dependent when physically active individuals were divided in tertiles. Beta-coefficients (95%CI) for the lowest, middle, and highest MVPA tertiles relative to the ‘No-MVPA’ were, respectively, − 0.24 (− 0.47;-0.02), − 0.31 (− 0.53;-0.08), and − 0.38 (− 0.61;-0.16) kg. The average weight gain in men was + 0.13 ± 0.03 kg, and only VPA, not MPA was associated with less body weight gain. Beta-coefficients (95%CI) for the VPA tertiles relative to the ‘No-VPA’ group were, respectively, − 0.25 (− 0.42;-0.09), − 0.19 (− 0.38;-0.01) and − 0.20 (− 0.38;-0.02) kg. However, after adjusting for potential confounders, the association was no longer significant in men. The potential benefits of leisure-time PA were age-stratified and mainly observed in younger adults (men < 35 years) or stronger with younger age (women < 55 years).
Conclusion
Higher leisure-time MVPA, MPA, and VPA were associated with less weight gain in women < 55 years. In younger men (< 35 years), only VPA was associated with less weight gain.
Similar content being viewed by others


Introduction
Obesity contributes to the development of a number of chronic diseases, such as type 2 diabetes, cardiovascular diseases, and certain cancers [1]. Obesity rates among adults nearly trebled between 1975 and 2016 [2], and the epidemic proportions of obesity and obesity-related diseases continue to pose major health problems, globally. The global rate of type 2 diabetes among adults rose from 4.7% in 1980 to 8.5% in 2014 [1]. while one-third of all deaths worldwide are attributed to cardiovascular diseases [3]. With obesity acknowledged as the underlying cause of these health concerns, attention has shifted to the primordial prevention of obesity in non-obese people, necessitating the development and improvement of strategies for preventing weight gain [4, 5]. Genetic, socio-economic, and environmental factors generally account for body weight gain [6,7,8]. These factors influence energy balance-related behaviours that determine energy intake and expenditure. The primordial prevention of excessive calorie intake and of low levels of energy expenditure (i.e., low physical activity) constitute the main strategy for reducing the risk of weight gain [7, 9].
Previous studies have mainly focused on the benefits of increased physical activity (PA) as a strategy for promoting body weight loss and for preventing the regaining of body weight in obese individuals [10]. They have shown that individuals who become more active lose more body weight. Several large-scale studies have found that PA plays a role in the prevention of body weight gain [11,12,13]. By contrast, other studies have found no association between baseline PA and changes in body weight during follow-up assessments [14,15,16,17]. In some studies that mostly included small sample sizes, this association was only observed in subgroups, for example, in normal weight, female, or younger adults [18, 19]. Therefore, large-scale population-based studies that test the benefits of PA across groups differentiated by age and sex are required. Moreover, little is known about how the intensity and type of daily-life PA impact on its association with prospective changes in body weight. Clinical guidelines on physical activity recommended that people should do at least 150 min of moderate-intensity, or 75 min of vigorous intensity PA a week [20]. Although clinical guidelines recommend that physical activities should be conducted at moderate-to-vigorous and not at light intensity levels, most previous studies focused on total PA, including light PA [14, 15, 18, 19, 21]. Moreover, there are still unanswered questions as to whether vigorous PA is necessary for achieving a health benefit. As reported in the literature, VPA has more impact on VO2max and fitness level and induces more release of growth hormone and catecholamines, suggesting that benefits of physical activity differ according to intensity level, such that vigorous PA may affect muscle mass more, and also increase basal metabolic rate more, than moderate and light PA [22, 23]. However, not all individuals are able or willing to perform vigorous PA, and this may not even be necessary if a moderate intensity level is in fact effective.
The primary objective of our study is to determine associations between leisure-time physical activity (LTPA) at different intensities (moderate and vigorous or moderate-to-vigorous) and prospective weight gain in non-obese people. We also examined whether these associations are independent of other lifestyle factors and changes in muscle mass and whether they are age-dependent and change over a person’s life course. In case that the association of MVPA depends on its intensity, we explore how it relates to the types of activities reported by the participants for translational purposes.
Methods
Data source and study population
Lifelines is a multidisciplinary prospective population-based cohort and biobank of more than 167,000 people living in the North of the Netherlands [21]. It employs a broad range of investigative procedures in assessing the biomedical, socio-demographic, behavioral, physical, and psychological factors that contribute to the health and disease of the general population, with a special focus on multi-morbidity and complex genetics. The study is conducted according to the Helsinki Declaration, and it was approved by the medical ethical committee of the University Medical Center Groningen in the Netherlands. All participants provided their written informed consent [24].
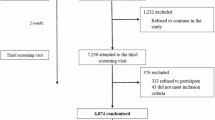
In this study, the analyses were based on the data at baseline and at 4-year follow-up. We included non-obese (BMI < 30 kg/m2) adult (> 18 years) subjects of Western European origin. The first exclusion was any missing and/or implausible data related to the main determinant and outcome: assessment of physical activity and the measurements of body weight. Further exclusions were related to minimize bias from changes in physical activity or body weight: excessive or unwanted weight loss, pregnancy, type 2 diabetes, thyroid diseases, irritable bowel syndrome, transplantation, cancer, heart failure, stroke, stent or bypass and pacemaker. In all, 52,498 participants were included in the current analyses (Fig. 1).

Flowchart of the study population
Assessment of physical activity
Physical activity was assessed using the Short QUestionnaire to ASsess Health-enhancing (SQUASH) physical activity, a validated questionnaire, which estimates habitual physical activities with reference to a normal week in the past month [25]. The SQUASH questionnaire allows for the categorization of minutes of PA according to levels of intensity, namely light, moderate, and vigorous. Furthermore, another reason for having chosen this questionnaire in this study is that the SQUASH allows to measure PA minutes through intensity level and through different types of daily-life PA at the same time. The SQUASH is pre-structured into four domains: commuting, leisure time, household, and occupational activities. Questions consisted of three main queries: days per week, average time per day, and intensity. Each activity in minutes per week was calculated by multiplying frequency (days/week) by duration (min/day). Then, the activities were assigned to a certain level of effort, or intensity, indicated by the MET value of the activity [25,26,27] MET values were assigned to activities with the help of Ainsworth’s Compendium of Physical Activities [28].
In this study, leisure-time (including commuting) moderate-to-vigorous PA (MVPA; MET ≥4.0), moderate PA (MPA; MET between 4 and 6.5) and vigorous PA (VPA; MET ≥6.5) categories were used as the main measures of physical activity. These intervals are applied according to the guidelines for Dutch physical activity [29]. Participants were divided into distinct categories based on the amount of MVPA, MPA and VPA. Individuals who performed no physical activity at MVPA, MPA and VPA, respectively were classified as ‘No-MVPA’, ‘No-MPA’ and ‘No-VPA’ (T0). The other participants (MVPA> 0 min/week, MPA > 0 min/week and VPA > 0 min/week) were divided into distinct tertiles of MVPA, MPA and VPA ranging from low (tertile 1, T1), middle (tertile 2, T2) to high (tertile 3, T3). Thus, T0, T1, T2 and T3 were considered as ‘inactive’, ‘a little bit active’, ‘active’, and ‘very active’ respectively [26].
Additionally, activity minutes per week for specific types of daily-life physical activity (walking, cycling, sports and odd jobs) at moderate or vigorous intensity were categorized into two levels: No-MPA and MPA > 0 min per week, or No-VPA and VPA > 0 min per week.
Body weight measurement
Participants’ body weights (in kg) were measured by well-trained assistants who are permanent staff members using a standardized protocol [24]. At a follow-up session conducted after 4 years, their body weights were measured to the nearest 0.1 kg using the same baseline protocol. Changes between baseline and follow-up measurements were standardized to a 4-year period.
Other baseline measurements
Body height, waist circumference and blood pressure were measured by trained assistants at baseline, and BMI (kg/m2) was calculated. Blood samples were collected in the fasting state and analyzed on the day of collection at the Department of Laboratory Medicine of the University Medical Center Groningen, the Netherlands (Supplementary method 1, Additional file 2) [24].
The supplementary methods section (Supplementary method 2, Additional file 2) provides definitions for the covariates. In brief, education levels were categorized as low, medium, and high. Current smoking status was categorized as non-smokers and smokers. Daily caloric and alcohol intakes were calculated using the Food Frequency Questionnaire and presented as kilocalories per day (kcal/day) and grammes of alcohol per day (g/day). Diet quality was assessed using the Lifelines Diet Score, which is described in greater detail elsewhere [30]. Creatinine excretion was calculated as the mean value derived from two urine samples collected over a 24-h period [31]. The method applied for analysing the urine samples is described in detail elsewhere [24].
Statistical analysis
The study characteristics were expressed as means with a standard deviation for normally distributed variables or as medians with interquartile range (25th to 75th percentile) for non-normally distributed variables and numbers with percentages in case of categorical data. The differences between groups were compared using 1-way analysis of variance tests or Kruskal-Wallis tests for continuous variables. The frequency distributions of categorical variables were analyzed using the Pearson Chi-Square test. Furthermore, estimated changes in body weight were estimated according to the level of physical activity (MVPA and VPA) using age and education adjusted ANOVA. Outcomes were presented as mean of kilogram body weight with standard error.
Linear regression analysis was performed to evaluate the association between PA and changes in body weight. First, we investigated MVPA, MPA and VPA dichotomously (No-PA and PA > 0). In the main analysis, dummy exposure variables were created to compare each tertile of MVPA, MPA and VPA (T1–3) with the reference group (No-MVPA, No-MPA and No-VPA). Outcomes were presented as unstandardized beta-coefficients with 95% confidence intervals (95%CI). In the regression analyses, the basic model was adjusted for age and education level. In model 1, we added diet (LLDS for diet quality and daily caloric intake for diet quantity), current smoking (yes/no) and alcohol consumption (g/day) as potential lifestyle confounders to the basic model. Model 2 was adjusted for changes in creatinine excretion, a marker of muscle mass, in addition to adjustments in model 1. Model 3 included an additional sensitivity analysis on non-leisure time PA (occupational MVPA). All the regression analyses were repeated stratified by age categories (18–34, 35–54, and ≥ 55 years). Furthermore, the role of specific types of daily-life physical activities was investigated by repeating the analyses with the physical activity determinant divided into its underlying components (e.g. walking, cycling, sports etc.).
All statistical analyses were performed using IBM SPSS V.22.0 (Chicago, IL) and GraphPad Prism V.4.03 (San Diego, CA). A two-sided statistical significance was set at p < 0.05 for all tests.
Results
In this study, we included 52,498 non-obese participantsof the Lifelines cohort study. Female participants were more likely to have healthy lifestyles at baseline. Fewer women were smokers or consumed alcohol, and their diet scores were healthier than those of men (Table 1). Of the participants, 13.3% of males (n = 3035) and 8.8% of females (n = 2519) did not perform any activities at a moderate-to-vigorous level (No-MVPA). Inactive participants had more often a lower educational level, lower diet score, higher cholesterol and were more often smokers. Men’s PA levels (min/week), and especially VPA were significantly higher than those of women. Table S1 shows the participants’ characteristics stratified by age. The age- and education-adjusted leisure-time MVPA mean values for men and women in min/week were, respectively, 288.0 ± 1.9 and 279.4 ± 1.7, and those for leisure-time VPA were 133.4 ± 4.2 and 88.8 ± 1.1, respectively. Figure S1 shows the levels of specific types of leisure-time MVPA.
After 4 years, the body weights of male and female participants had increased on average by 0.13 ± 0.03 kg and 0.45 ± 0.03 kg, respectively. Increases in the body weights of participants, stratified by age, were mostly observed in younger men (18–35 years) and young and middle-aged women (18–54 years, Figure S2). Changes in body weight, estimated with an age- and education-adjusted ANOVA were visualized according to PA levels in Fig. 2. All groups of the female participants gained body weight, but this increase in body weight was attenuated with increasing MVPA and VPA levels (T1–T3). This was observed in men only for the association between VPA and changes in body weight (Fig. 2).

Estimated changes in body weight (kg) adjusted for age and education level, stratified by levels of moderate-to-vigorous (a and b) and vigorous (c and d) leisure-time physical activity. Measured body weight change adjusted with ANOVA. MVPA = moderate-to-vigorous physical activity, VPA = vigorous physical activity, T = tertile. Leisure-time MVPA and VPA were used in the analysis
To test the significance of these observations, inactive participants were compared to active participants in regression analyses (Table 2, Table S3). Higher leisure-time MVPA, as well as MPA and VPA separately, were associated with less gain in body weight in women. Beta coefficients (95%CI) for the MVPA> 0, MPA > 0 and VPA > 0 relative to each reference group (No-MVPA, No-MPA and No-VPA) were, respectively − 0.34 (− 0.56; − 0.13), − 0.32 (− 0.54; − 0.10) and − 0.30 (− 0.43; − 0.18) kg. These associations were dose-dependent when PA was categorized into four groups (Table 2, Table S3). In women, the beta-coefficients attenuated by 10–20% but remained significant after adjusting for potential confounders, including muscle mass. An in-depth investigation of the roles of the confounders indicated that the diet-based confounding effect was slightly stronger than the confounding effects of smoking and alcohol consumption (Table S2). In men, higher VPA, but not higher MPA or MVPA, was associated with less body weight gain. However, after adjusting for potential confounders, the association was no longer significant (Tables 2, S2, S3).
Stratification of the participants by age revealed significant associations mainly in younger adults (Fig. 3). For men below 35 years and for women aged 35–55 years, leisure-time VPA was dose-dependently associated with less gain in body weight after fully adjusting for confounding factors (Table S4).

Association between vigorous leisure-time physical activity and changes in body weight, stratified by age in men (a) and women (b). Regression analysis. Data are expressed as unstandardized beta coefficient (presented as bar) with 95% confidence interval (95% CI, presented as arrow). Physical activity was shown as vigorous physical activity categories (T0-T3). T = tertile. Analysis was adjusted for age, education. Diet score, energy intake, smoking and alcohol use
We conducted additional analyses aimed at elucidating the role of individual daily-life activities within the physical activity domain for translational purposes (Table S5). These analyses were performed for men below 35 years and women below 55 of age years because significant associations of LTPA and changes in body weight were observed for individuals in these age groups. Our findings based on analyses with dichotomized PA (No-MPA and MPA > 0 or No-VPA and VPA > 0) indicated that higher levels of moderate (cycling) and vigorous (cycling and sports) PA were associated with less weight gain in women after fully adjusting for confounding factors. For men, only higher levels of VPA (cycling and sports) were associated with less weight gain (Table S5). In a sensitivity analysis, there was no clear association between occupational MVPA and changes in body weight among both men and women (Table 2).
Discussion
In this large-scale, population-based study, a higher leisure-time MVPA was found to be associated to less weight gain in women in a dose-dependent way. Moreover, these associations were stronger and independent of other potential confounders in women under the age of 55 years. Furthermore, the potentially favourable effects of PA for women applied to both moderate and vigorous physical activities like cycling and sports. Among male participants, strenuous physical activities, such as vigorous cycling and sports, were predominantly associated to lower weight gain but only in younger (< 35 years) men after adjusting for other lifestyle factors.
Several previous prospective studies found an inverse association between PA and changes in body weight [11,12,13, 32, 33]. However this association has not been confirmed in other studies [14,15,16,17]. Moreover, this association was found to be restricted to specific groups in some studies [18, 19]. For instance, a large-scale, multi-country EPIC study (n = 288,498) found an association between PA and 5-year changes in body weight only in younger women (< 50 years) and those of normal weight [18]. In our large-scale, population-based study, the benefits of LTPA differed among men and women relative to the PA intensity level. Moreover, the associations between PA and changes in body weight differed according age. These core findings are discussed in more detail below.
Clinical guidelines on PA levels state that physical activities at the moderate-to-vigorous level, but not at the light level, are essential for maintaining a healthy body weight [34]. However, most previous studies focused on total PA, including light PA, and did not test for or report on different PA intensity levels [14, 15, 18, 19, 21]. The few studies that tested intensity levels suggest that physical activities at higher intensity levels are more effective than those at lower intensity levels in weight management [17, 35]. Williams et al. found that weight loss from running exceeded that from walking after 6.2 years of follow-up [35]. Furthermore, there is some debate about intensity, duration and load. In theory, a longer bout of MPA would lead to the same energy expenditure as a shorter bout of VPA. However, a review study concluded that even if the PA requires the same amount of energy, so same energy expenditure but at moderate or vigorous load, there were different effects, suggesting a greater cardioprotective benefit from VPA than MPA [36]. More recent studies confirm this [37, 38]. In this observational study, we cannot provide explanatory mechanisms related to exact load or duration. Instead, we study the effects of MPA and VPA in free-living situations. The interpretation is that people who practice more VPA are less prone to weight gain. The value is in quantifying this association, describing relevant gender differences, and attributing this relation to the type of activity in a large population of participants.
A question that we aimed to address in our study was whether a vigorous level of PA better predicts future changes in body weight. This was found to be the case in men (< 35 years) for whom only vigorous activities were related to weight changes. However, in women, both moderate (cycling) and vigorous (cycling and sports) activities were related to body weight changes. Even more so, the benefits of total daily-life MVPA were mostly explained by MPA in women. The considerably lower changes in the body weights of men compared with those of women during the follow-up assessment may be indicative of a statistical power issue that could partly account for this gender difference. Another explanation could be that male participants’ reporting of VPA was more accurate than their reporting of MPA or other physical activities in the questionnaire [39]. Accordingly, more longitudinal studies are needed to establish the effects of different PA intensities for men to prevent body weight gain. For women, not only VPA but also MPA can be considered as an option for avoiding body weight gain.
In this study, the association of physical activity with changes in body weight was mainly observed in younger adults. This association may be related to the observation that life-time weight gain mostly occurred during this period (Figure S2). In line with our findings, another study found that the transition from normal weight to obesity was mostly observed around the ages of 28–33 and 31–36 years [33]. The findings of this and other studies suggest that a high level of activity during those ages can prevent overweight or obesity [11, 33]. This is plausible, as an increased energy expenditure may help to avoid a positive energy balance. Nevertheless, the usefulness of physical activity alone in body weight control has been doubted. This is based on studies showing that increasing physical activity alone is not effective for weight loss [10]. In our view, the process of weight loss is not simply the reverse of the process of weight gain, as with weight loss, there are many hormones counteracting negative energy balance [40]. In the case of prevention of weight gain, these hormones do not play a role. Indeed, a number of studies have reported that a very active lifestyle at younger adult ages may entail the benefit of obesity prevention at later ages [9, 12, 30]. Moreover, a higher BMI in early adult life is a predictor of cardiovascular diseases in later life [41]. Thus, a conclusion that merits emphasis is that increasing PA at younger ages may be an important primordial obesity prevention strategy while simultaneously preventing non-communicable diseases in later adult life.
It should be noted that our outcome measure focused on changes in overall body weight and not specifically on body fat mass. Changes in body weight, especially in younger adults, could reflect changes in muscle mass. Consequently, we adjusted for creatinine excretion in all of the analyses and found that the association between PA and changes in body weight was independent of changes in muscle mass over time. Previous studies that used direct measures of body composition indeed explained differences in weight gain by smaller changes in body fat in very active younger adults and greater gains in body fat in inactive young adults [11, 42]. Although 24-h urinary creatinine excretion may not be a precise marker for the absolute level of muscle mass, changes in creatinine excretion have been found to be a more sensitive measure for changes in body composition compared with DEXA [43]. Therefore, we concluded that increased PA can be an effective strategy for preventing body weight gain independently of muscle mass.
The main strength of our study is its large sample size obtained from the general population, which enabled us to estimate the dose-dependency of different PA intensities with changes in body weight for sex- and age-differentiated groups with sufficient statistical power. A second strength of the study relates to the objective measurements of body weight that were taken during the baseline and follow-up phases. Although we excluded many participants who are obese or with several diseases it helps to minimize cause-effect bias relating to changes in PA or body weight caused by poor health. However, it also can be a limitation in that it confers a reduction of representativeness of the population. Another limitation is that PA was reported only at the baseline stage. A few studies have concluded that a single measure of PA weakly predicts future changes in body weight [14, 44], which may be related to a bidirectional association of PA and obesity [17, 45]. The inclusion in the analyses of more individuals living with obesity could attenuate the association between baseline PA and body weight at the follow-up assessment because individuals with obesity may on the one hand may be more inclined to be y inactive while simultaneously making conscious efforts to prevent weight gain through diet. In our study, we included only non-obese individuals with the aim of reducing such information bias. Another limitation relates to our assessment of PA that was based on self-reporting and therefore subject to recall bias. However, the SQUASH questionnaire has been validated within the general population, demonstrating a Spearman correlation coefficient for reproducibility of 0.58 [25]. Furthermore, the SQUASH questionnaire was not specifically validated for the different types of leisure time activity. Although PA quantification may have been subject to reporting bias, the qualitative information about the types and domain of MVPA proved valuable.
Conclusions
A higher level of leisure-time MVPA is associated with less gain in body weight in women. The potentially favourable effects of MVPA for women applied to both moderate and vigorous physical activities. The associations were found to be dose-dependent, suggesting that more MVPA is more beneficial. Furthermore, the associations were strongest in younger and middle-aged women (< 55 years) and were independent of diet, smoking, alcohol use, and 4-year changes in creatinine excretion, considered a marker of muscle mass. For men, only vigorous LTPA was associated with less weight gain in younger adults (< 35 years).
Availability of data and materials
The Lifelines Cohort does not enable public data sharing. The cohort’s data is only available to researchers who, upon approval of a submitted research proposal, have signed a Data/Material Transfer Agreement.
References
Zhou B, Lu Y, Hajifathalian K, Bentham J, Di Cesare M, Danaei G, et al. Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4.4 million participants. Lancet. 2016;387(10027):1513–30. https://doi.org/10.1016/S0140-6736(16)00618-8.
WHO. Obesity and overweight: Fact sheet: WHO Media Cent; 2016.
Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Executive summary: heart disease and stroke statistics-2016 update: a report from the American Heart Association. Circulation. 2016;131(4):434–41.
Kelishadi R, Heidari-Beni M. Prevention and Control of Childhood Obesity: The Backbone in Prevention of Non Communicable Disease; 2019. https://doi.org/10.1007/978-3-030-10616-4_7.
Climie R, Fuster V, Empana JP. Health literacy and primordial prevention in childhood - an opportunity to reduce the burden of cardiovascular disease. JAMA Cardiol. 2020;5(12):1323–4. https://doi.org/10.1001/jamacardio.2020.2864.
Speliotes EK, Willer CJ, Berndt SI, Monda KL, Thorleifsson G, Jackson AU, et al. Association analyses of 249,796 individuals reveal 18 new loci associated with body mass index. Nat Genet. 2010;42(11):937–48. https://doi.org/10.1038/ng.686.
Omer T. The causes of obesity: an in-depth review. Adv Obesity Weight Manag Control. 2020;10(4):90–4. https://doi.org/10.15406/aowmc.2020.10.00312.
Joosen AMCP, Gielen M, Vlietinck R, Westerterp KR. Genetic analysis of physical activity in twins. Am J Clin Nutr. 2005;82(6):1253–9. https://doi.org/10.1093/ajcn/82.6.1253.
Hayman LL, Worel JN. Healthy lifestyle behaviors the importance of individual and population approaches. J Cardiovasc Nurs. 2014;29(6):477–8. https://doi.org/10.1097/JCN.0000000000000199.
Swift DL, Johannsen NM, Lavie CJ, Earnest CP, Church TS. The role of exercise and physical activity in weight loss and maintenance. Prog Cardiovasc Dis. 2014;56(4):441–7. https://doi.org/10.1016/j.pcad.2013.09.012.
Hankinson AL, Daviglus ML, Bouchard C, Carnethon M, Lewis CE, Schreiner PJ, et al. Maintaining a high physical activity level over 20 years and weight gain. JAMA - J Am Med Assoc. 2010;304(23):2603–10. https://doi.org/10.1001/jama.2010.1843.
Moholdt T, Wisløff U, Lydersen S, Nauman J. Current physical activity guidelines for health are insufficient to mitigate long-term weight gain: more data in the fitness versus fatness debate (the HUNT study, Norway). Br J Sports Med. 2014;48(20):1489–96. https://doi.org/10.1136/bjsports-2014-093416.
Hamer M, Brunner EJ, Bell J, Batty GD, Shipley M, Akbaraly T, et al. Physical activity patterns over 10 years in relation to body mass index and waist circumference: the Whitehall II cohort study. Obesity. 2013;21(12):755–61.
AM M, HB B-M, Boshuizen H, AMW S, PH P, WMM V. Effect of change in physical activity on body fatness over a 10-y period in the Doetinchem cohort study. Am J Clin Nutr. 2010;92(3):491–9.
Dugas LR, Kliethermes S, Plange-Rhule J, Tong L, Bovet P, Forrester TE, et al. Accelerometer-measured physical activity is not associated with two-year weight change in African-origin adults from five diverse populations. PeerJ. 2017;5:e2902. https://doi.org/10.7717/peerj.2902.
Barone Gibbs B, Pettee Gabriel K, Carnethon MR, Gary-Webb T, Jakicic JM, Rana JS, et al. Sedentary time, physical activity, and adiposity: cross-sectional and longitudinal associations in CARDIA. Am J Prev Med. 2017;53(6):764–71. https://doi.org/10.1016/j.amepre.2017.07.009.
Ekelund U, Kolle E, Steene-Johannessen J, Dalene KE, Nilsen AKO, Anderssen SA, et al. Objectively measured sedentary time and physical activity and associations with body weight gain: does body weight determine a decline in moderate and vigorous intensity physical activity? Int J Obes. 2017;41(12):1769–74. https://doi.org/10.1038/ijo.2017.186.
Ekelund U, Besson H, Luan J, May AM, Sharp SJ, Brage S, et al. Physical activity and gain in abdominal adiposity and body weight: prospective cohort study in 288,498 men and women. Am J Clin Nutr. 2011;93(4):826–35. https://doi.org/10.3945/ajcn.110.006593.
Lee IM, Djoussé L, Sesso HD, Wang L, Buring JE. Physical activity and weight gain prevention. JAMA - J Am Med Assoc. 2010;303(12):1173–9. https://doi.org/10.1001/jama.2010.312.
World Health Organization. Global recommendations on physical activity for health. 2010.
Van Dyck D, Cerin E, De Bourdeaudhuij I, Hinckson E, Reis RS, Davey R, et al. International study of objectively measured physical activity and sedentary time with body mass index and obesity: IPEN adult study. Int J Obes. 2015;39(2):199–207. https://doi.org/10.1038/ijo.2014.115.
Wenger HA, Bell GJ. The interactions of intensity, frequency and duration of exercise training in altering cardiorespiratory fitness. Sport Med. 1986;3(5):346–56. https://doi.org/10.2165/00007256-198603050-00004.
Felsing NE, Brasel JA, Cooper DM. Effect of low and high intensity exercise on circulating growth hormone in men. J Clin Endocrinol Metab. 1992;71(1):157–62.
Stolk RP, Rosmalen JGM, Postma DS, De Boer RA, Navis G, Slaets JPJ, et al. Universal risk factors for multifactorial diseases: LifeLines: a three-generation population-based study. Eur J Epidemiol. 2008;23(1):67–74. https://doi.org/10.1007/s10654-007-9204-4.
Wendel-Vos GCW, Schuit AJ, Saris WHM, Kromhout D. Reproducibility and relative validity of the short questionnaire to assess health-enhancing physical activity. J Clin Epidemiol. 2003;56(12):1163–9. https://doi.org/10.1016/S0895-4356(03)00220-8.
Byambasukh O, Snieder H, Corpeleijn E. The relation between leisure time, commuting and occupational physical activity with blood pressure in 125,402 adults: the Lifelines cohort. J Am Heart Assoc. 2019;8:e0814313.
Byambasukh O, Zelle D, Corpeleijn E. Physical activity, fatty liver, and glucose metabolism over the life course. Am J Gastroenterol. 2019;114(6):907–15. https://doi.org/10.14309/ajg.0000000000000168.
Ainsworth BE, Haskell WL, Herrmann SD, Meckes N, Bassett DR, Tudor-Locke C, et al. 2011 compendium of physical activities: a second update of codes and MET values. Med Sci Sports Exerc. 2011;43(8):1575–81. https://doi.org/10.1249/MSS.0b013e31821ece12.
Weggemans RM, Backx FJG, Borghouts L, Chinapaw M, Hopman MTE, Koster A, et al. The 2017 Dutch physical activity guidelines. Int J Behav Nutr Phys Act. 2018;15(1):58. https://doi.org/10.1186/s12966-018-0661-9.
Vinke PC, Corpeleijn E, Dekker LH, Jacobs DR, Navis G, Kromhout D. Development of the food-based Lifelines diet score (LLDS) and its application in 129,369 Lifelines participants. Eur J Clin Nutr. 2018;72(8):1111–9. https://doi.org/10.1038/s41430-018-0205-z.
Oterdoom LH, Gansevoort RT, Schouten JP, de Jong PE, Gans ROB, Bakker SJL. Urinary creatinine excretion, an indirect measure of muscle mass, is an independent predictor of cardiovascular disease and mortality in the general population. Atherosclerosis. 2009;207(2):534–40. https://doi.org/10.1016/j.atherosclerosis.2009.05.010.
Williamson DF, Madans J, Anda RF, Kleinman JC, Kahn HS, Byers T. Recreational physical activity and ten-year weight change in a US national cohort. IntJObesRelat Metab Disord. 1993;17:279–86.
Pavey TG, Peeters Geeske GMEE, Gomersall SR, Brown WJ. Long-term effects of physical activity level on changes in healthy body mass index over 12 years in young adult women. Mayo Clin Proc. 2016;91(6):735–44. https://doi.org/10.1016/j.mayocp.2016.03.008.
Yumuk V, Tsigos C, Fried M, Schindler K, Busetto L, Micic D, et al. European guidelines for obesity management in adults. Obes Facts. 2015;8(6):402–24. https://doi.org/10.1159/000442721.
Williams PT. Greater weight loss from running than walking during a 6.2-yr prospective follow-up. Med Sci Sports Exerc. 2013;45(4):706.
Swain DP, Franklin BA. Comparison of cardioprotective benefits of vigorous versus moderate intensity aerobic exercise. Am J Cardiol. 2006;97(1):141–7. https://doi.org/10.1016/j.amjcard.2005.07.130.
Orri J, Hughes E, Mistry D, Scala A. Is vigorous exercise training superior to moderate for CVD risk after menopause? Sport Med Int Open. 2017;1(5):E166.
Hidalgo-Santamaria M, Fernandez-Montero A, Martinez-Gonzalez MA, Moreno-Galarraga L, Sanchez-Villegas A, Barrio-Lopez MT, et al. Exercise intensity and incidence of metabolic syndrome: the SUN project. Am J Prev Med. 2017;52(4):e95–101. https://doi.org/10.1016/j.amepre.2016.11.021.
Ainsworth BE, Leon AS, Richardson MT, Jacobs DR, Paffenbarger RS. Accuracy of the college alumnus physical activity questionnaire. J Clin Epidemiol. 1993;46(12):1403–11. https://doi.org/10.1016/0895-4356(93)90140-V.
Ueda SY, Yoshikawa T, Katsura Y, Usui T, Nakao H, Fujimoto S. Changes in gut hormone levels and negative energy balance during aerobic exercise in obese young males. J Endocrinol. 2009;201(1):151–9. https://doi.org/10.1677/JOE-08-0500.
Park MH, Sovio U, Viner RM, Hardy RJ, Kinra S. Overweight in childhood, adolescence and adulthood and cardiovascular risk in later life: pooled analysis of three British birth cohorts. PLoS One. 2013;8(7):1–6.
Staiano AE, Martin CK, Champagne CM, Rood JC, Katzmarzyk PT. Sedentary time, physical activity, and adiposity in a longitudinal cohort of nonobese young adults. Am J Clin Nutr. 2018;108(5):946–52. https://doi.org/10.1093/ajcn/nqy191.
Proctor DN, O’Brien PC, Atkinson EJ, Nair KS. Comparison of techniques to estimate total body skeletal muscle mass in people of different age groups. Am J Physiol - Endocrinol Metab. 1999;277(3):E489–95. https://doi.org/10.1152/ajpendo.1999.277.3.E489.
Summerbell CD, Douthwaite W, Whittaker V, Ells LJ, Hillier F, Smith S, et al. The association between diet and physical activity and subsequent excess weight gain and obesity assessment at 5 years age or older: a systematic review of the epidemiological evidence. Int J Obes. 2009;92:491–9.
Golubic R, Wijndaele K, Sharp SJ, Simmons RK, Griffin SJ, Wareham NJ, et al. Physical activity, sedentary time and gain in overall and central body fat: 7-year follow-up of the ProActive trial cohort. Int J Obes. 2015;39(1):142–8. https://doi.org/10.1038/ijo.2014.66.
Acknowledgements
The authors wish to acknowledge the assistance of the Lifelines Cohort Study, the contributing research centers which deliver data to Lifelines and all the study participants.
Funding
None.
Author information
Authors and Affiliations
Contributions
All authors drafted the concept and design. OB performed the analysis and drafted the manuscript. PV prepared the dataset for the current study. EC edited the drafts. PV, DK and GN commented on the drafts. OB and EC produced the final manuscript. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the medical ethical review committee of the University Medical Center Groningen, the Netherlands. All participants provided their written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
STROBE Statement—checklist of items that should be included in reports of observational studies.
Additional file 2:
Anthropometry and laboratory measurements. Definition of lifestyle confounders and diseases. Table S1. General characteristics of the study population, by age. Table S2. Role of lifestyle confounders in the association between physical activity and changes in body weight. Table S3. Leisure-time MPA and 4-year changes in body weight. Table S4. Moderate-to-vigorous physical activity and changes in body weight, according to age. Table S5. Individual physical activities and 4-year changes in body weight. Fig. S1. Level of daily-life physical activity according to sex. Fig. S2. 4-year changes in body weight, according to 6 categories of age.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Byambasukh, O., Vinke, P., Kromhout, D. et al. Physical activity and 4-year changes in body weight in 52,498 non-obese people: the Lifelines cohort. Int J Behav Nutr Phys Act 18, 75 (2021). https://doi.org/10.1186/s12966-021-01141-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-021-01141-8